OralDisk: A Chair-Side Compatible Molecular Platform Using Whole Saliva for Monitoring Oral Health at the Dental Practice

 , ,
, ,  ,
,  , , , , , , ,
, , , , , , ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection and Ethics Permission
2.2. Selected Bacterial Panel
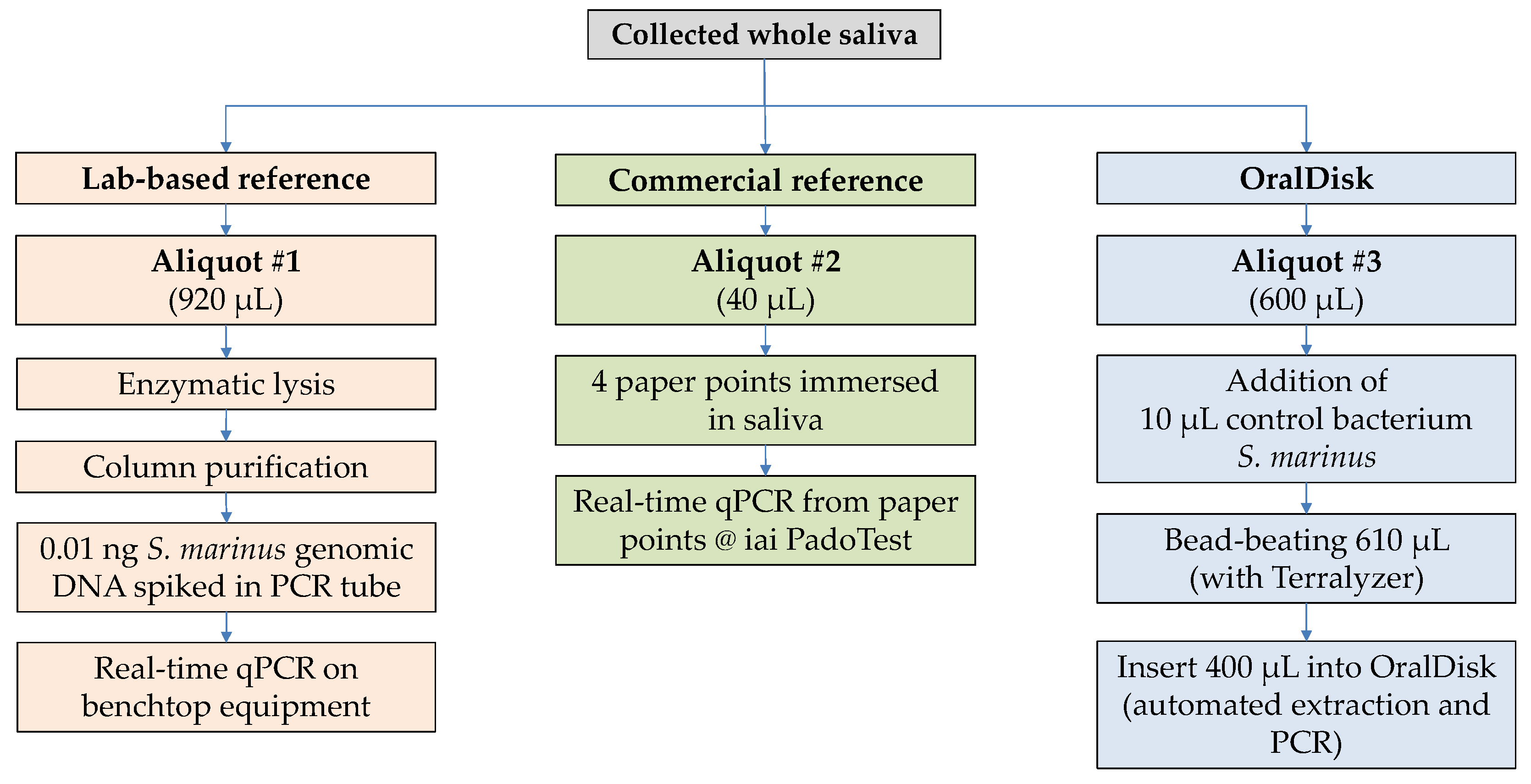
2.3. Reference Method #1: Lab-Based DNA Extraction and qPCR
2.4. Reference Method #2: Commercial iai PadoTest
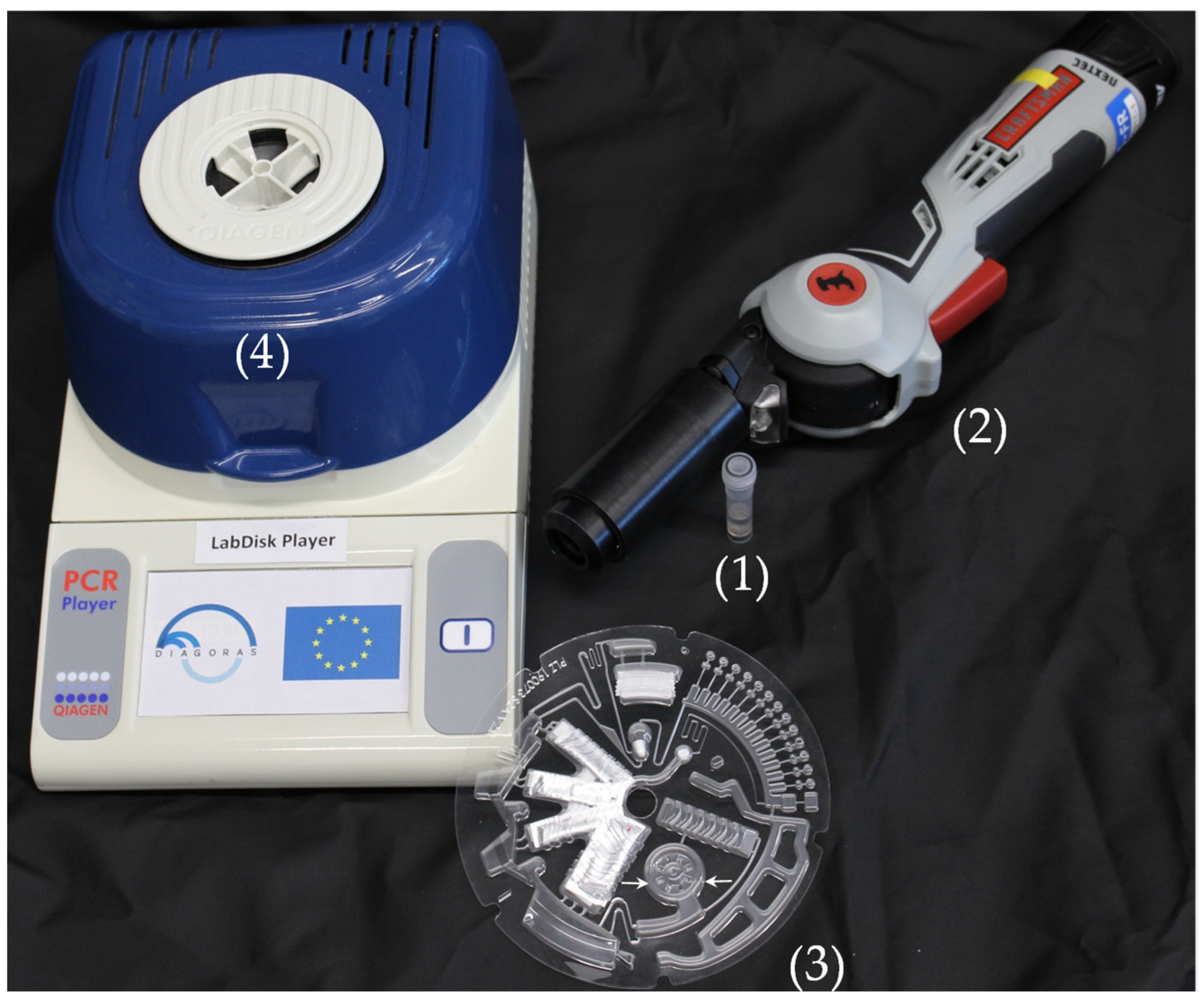
2.5. Mechanical Lysis and Homogenization of Saliva Samples Prior to Insertion into the OralDisk
2.6. OralDisk Design and Workflow for Fully Automated Real-Time PCR
2.7. OralDisk Fabrication
2.8. Statistics
3. Results and Discussion
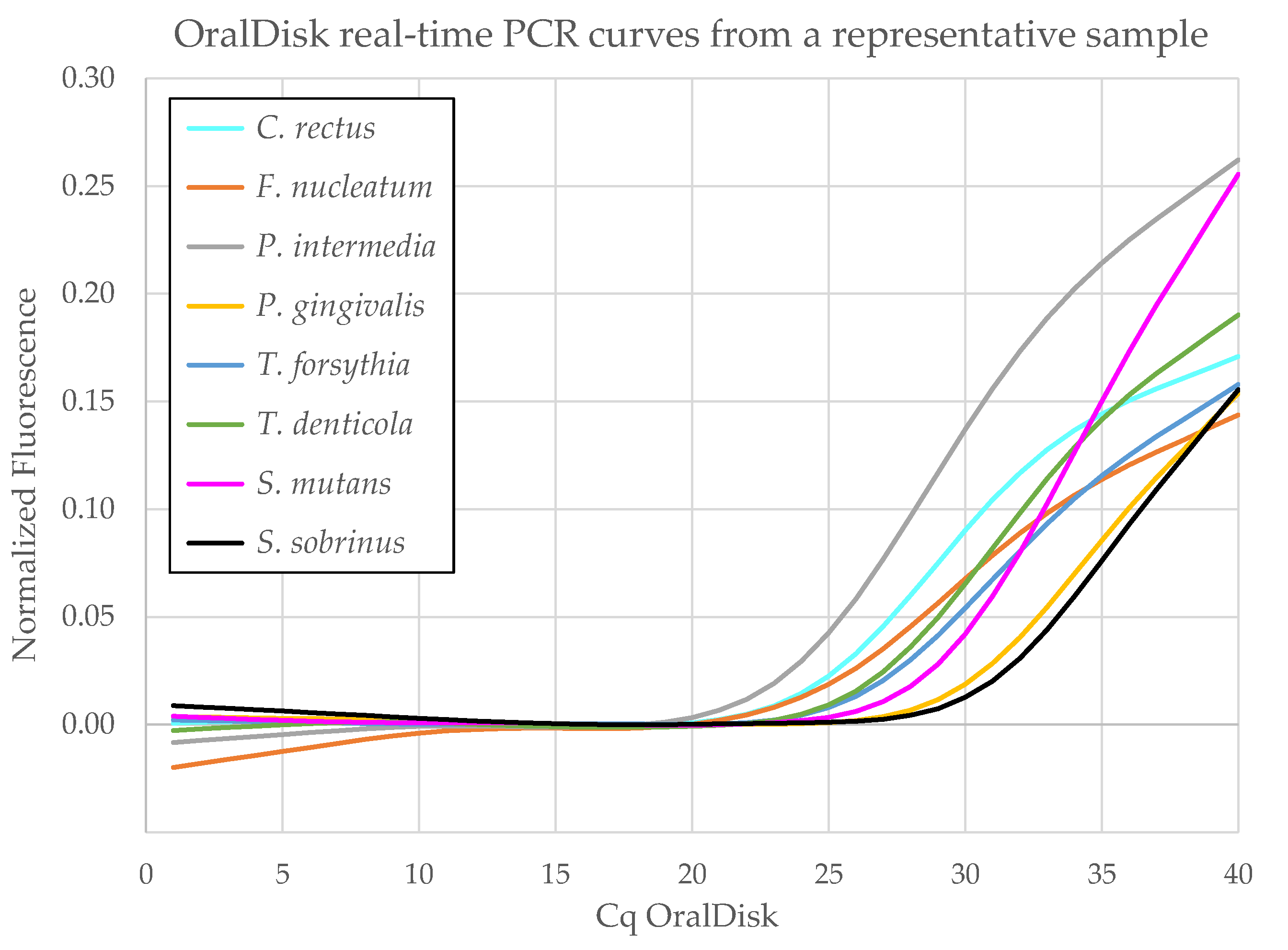
3.1. Real-Time PCR on the OralDisk
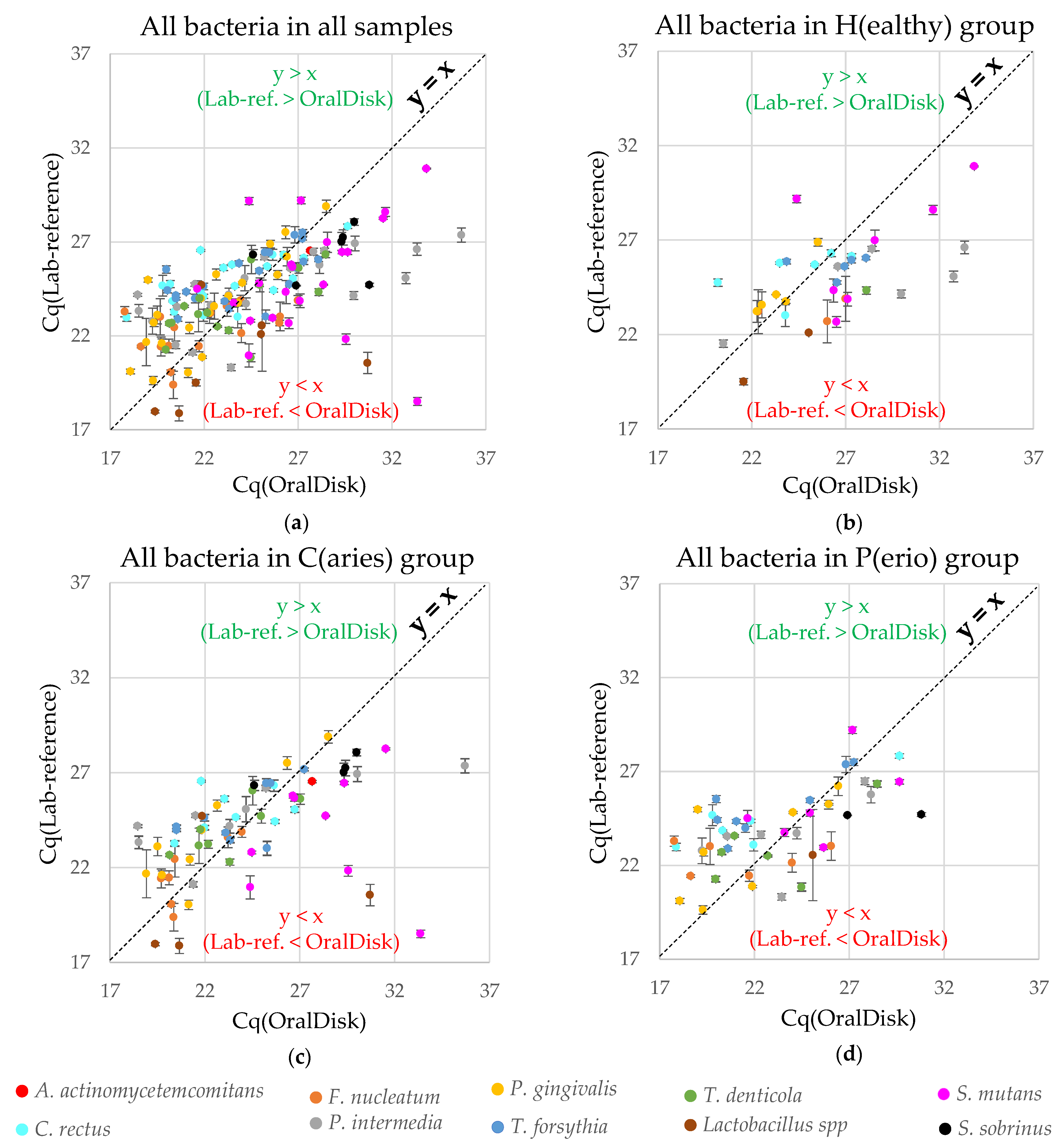
3.2. Performance Comparison between the OralDisk and the Lab-Based Reference Method
- (a)
- assay targets detected as positive by both the OralDisk and the lab-based reference (agreement in positive samples: 154/175 (88.0%) cases);
- (b)
- assay targets detected as positive by the OralDisk but negative by the lab-based reference (disagreement in 7/59 (11.9%) cases);
- (c)
- assay targets detected as negative by both the OralDisk and the lab-based reference (agreement in negative samples: 52/59 (88.1%) cases);
- (d)
- assay targets detected as negative by the OralDisk but positive by the lab-based reference (disagreement in 21/175 (12.0%) cases).
3.3. Performance Comparison between the OralDisk and the Commercial iai PadoTest
3.4. Comparison of Cq Performance
3.5. Overall Evaluation of the OralDisk
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dental Diseases and Oral Health. Available online: www.who.int/oral_health/publications/en/orh_fact_sheet.pdf (accessed on 30 September 2021).
- Listl, S.; Grytten, J.I.; Birch, S. What is health economics? Community Dent. Health 2019, 36, 262–274. [Google Scholar] [PubMed]
- Belibasakis, G.N.; Lund, B.; Krüger Weiner, C.; Johannsen, B.; Baumgartner, B.; Manoil, C.; Hultin, M.; Mitsakakis, K. Healthcare Challenges and Solutions in Dental Practice: Assessing Oral Antibiotic Resistances by Contemporary Point-of-Care Solutions. Antibiotics 2020, 9, 810. [Google Scholar] [CrossRef] [PubMed]
- Suda, K.J.; Calip, G.S.; Zhou, J.F.; Rowan, S.; Gross, A.E.; Hershow, R.C.; Perez, R.I.; McGregor, J.C.; Evans, C.T. Assessment of the appropriateness of antibiotic prescriptions for infection prophylaxis before dental procedures, 2011 to 2015. JAMA Netw. Open 2019, 2, e193909. [Google Scholar] [CrossRef] [Green Version]
- Bernabe, E.; Marcenes, W.; Hernandez, C.R.; Bailey, J.; Abreu, L.G.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; Arora, A.; et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [PubMed]
- WHO, Regional Office for Europe, Oral Health, Data and Statistics. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/oral-health/data-and-statistics (accessed on 30 September 2021).
- NIDCR, NIH, Periodontal (Hum) Disease. Available online: http://www.nidcr.nih.gov/OralHealth/Topics/GumDiseases/PeriodontalGumDisease.htm (accessed on 30 September 2021).
- Seitz, M.W.; Listl, S.; Bartols, A.; Schubert, I.; Blaschke, K.; Haux, C.; Van Der Zande, M.M. Current Knowledge on Correlations Between Highly Prevalent Dental Conditions and Chronic Diseases: An Umbrella Review. Prev. Chronic. Dis. 2019, 16, 180641. [Google Scholar] [CrossRef] [Green Version]
- D’Aiuto, F.; Gable, D.; Syed, Z.; Allen, Y.; Wanyonyi, K.L.; White, S.; Gallagher, J.E. Evidence summary: The relationship between oral diseases and diabetes. Br. Dent. J. 2017, 222, 944–948. [Google Scholar] [CrossRef] [Green Version]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Petersen, P.E. Global policy for improvement of oral health in the 21st century--implications to oral health research of World Health Assembly 2007, World Health Organization. Community Dent. Oral Epidemiol. 2009, 37, 1–8. [Google Scholar] [CrossRef]
- Listgarten, M.A. Periodontal probing: What does it mean? J. Clin. Periodontol. 1980, 7, 165–176. [Google Scholar] [CrossRef]
- Hefti, A.F. Periodontal probing. Crit. Rev. Oral. Biol. Med. 1997, 8, 336–356. [Google Scholar] [CrossRef] [Green Version]
- Olsen, I. Update on bacteraemia related to dental procedures. Transfus. Apher. Sci. 2008, 39, 173–178. [Google Scholar] [CrossRef]
- Daly, C.G.; Mitchell, D.H.; Highfield, J.E.; Grossberg, D.E.; Stewart, D. Bacteremia due to periodontal probing: A clinical and microbiological investigation. J. Periodontol. 2001, 72, 210–214. [Google Scholar] [CrossRef]
- Preshaw, P.M. Detection and diagnosis of periodontal conditions amenable to prevention. BMC Oral Health 2015, 15, S5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitsakakis, K.; Stumpf, F.; Strohmeier, O.; Klein, V.; Mark, D.; von Stetten, F.; Peham, J.R.; Herz, C.; Tawakoli, P.N.; Wegehaupt, F.; et al. Chair/bedside diagnosis of oral and respiratory tract infections, and identification of antibiotic resistances for personalised monitoring and treatment. Stud. Health Technol. Inform. 2016, 224, 61–66. [Google Scholar] [PubMed]
- Czilwik, G.; Messinger, T.; Strohmeier, O.; Wadle, S.; von Stetten, F.; Paust, N.; Roth, G.; Zengerle, R.; Saarinen, P.; Niittymaki, J.; et al. Rapid and fully automated bacterial pathogen detection on a centrifugal-microfluidic LabDisk using highly sensitive nested PCR with integrated sample preparation. Lab Chip 2015, 15, 3749–3759. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, F.; Schwemmer, F.; Hutzenlaub, T.; Baumann, D.; Strohmeier, O.; Dingemanns, G.; Simons, G.; Sager, C.; Plobner, L.; von Stetten, F.; et al. LabDisk with complete reagent prestorage for sample-to-answer nucleic acid based detection of respiratory pathogens verified with influenza A H3N2 virus. Lab Chip 2016, 16, 199–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hin, S.; Lopez-Jimena, B.; Bakheit, M.; Klein, V.; Stack, S.; Fall, C.; Sall, A.; Enan, K.; Mustafa, M.; Liz Gillies, L.; et al. Fully automated point-of-care differential diagnosis of acute febrile illness. PLoS Negl. Trop. Dis. 2021, 15, e0009177. [Google Scholar] [CrossRef]
- Rombach, M.; Hin, S.; Specht, M.; Johannsen, B.; Lüddecke, J.; Paust, N.; Zengerle, R.; Roux, L.; Sutcliffe, T.; Peham, J.R.; et al. RespiDisk: A Point-of-Care platform for fully automated detection of respiratory tract infection pathogens in clinical samples. Analyst 2020, 145, 7040–7047. [Google Scholar] [CrossRef]
- Paqué, P.N.; Herz, C.; Jenzer, J.S.; Wiedemeier, D.; Attin, T.; Bostanci, N.; Belibasakis, G.N.; Bao, K.; Körner, P.; Fritz, T.; et al. Microbial analysis of saliva to identify oral diseases using a point-of-care compatible qPCR assay. J. Clin. Med. 2020, 9, 2945. [Google Scholar] [CrossRef]
- Lamont, R.J.; Hajishengallis, G. Polymicrobial synergy and dysbiosis in inflammatory disease. Trends Mol. Med. 2015, 21, 172–183. [Google Scholar] [CrossRef] [Green Version]
- Bostanci, N.; Bao, K.; Greenwood, D.; Silbereisen, A.; Belibasakis, G.N. Periodontal disease: From the lenses of light microscopy to the specs of proteomics and next-generation sequencing. Adv. Clin. Chem. 2019, 93, 263–290. [Google Scholar] [PubMed]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent Jr, R.L. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Haffajee, A.D.; Socransky, S.S.; Patel, M.R.; Song, X. Microbial complexes in supragingival plaque. Oral Microbiol. Immunol. 2008, 23, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Website of iai PadoTest. Available online: https://www.padotest.ch/en (accessed on 30 September 2021).
- Belibasakis, G.N.; Schmidlin, P.R.; Sahrmann, P. Molecular microbiological evaluation of subgingival biofilm sampling by paper point and curette. APMIS 2014, 122, 347–352. [Google Scholar] [CrossRef] [Green Version]
- Yi, H.; Schumann, P.; Sohn, K.; Chun, J. Serinicoccus marinus gen. nov., sp. nov., a novel actinomycete with L-ornithine and L-serine in the peptidoglycan. Int. J. Syst. Evol. Microbiol. 2004, 54, 1585–1589. [Google Scholar] [CrossRef] [Green Version]
- Strohmeier, O.; Keller, M.; Schwemmer, F.; Zehnle, S.; Mark, D.; von Stetten, F.; Zengerle, R.; Paust, N. Centrifugal microfluidic platforms: Advanced unit operations and applications. Chem. Soc. Rev. 2015, 44, 6187–6229. [Google Scholar] [CrossRef] [Green Version]
- Boom, R.; Sol, M.M.; Jansen, C.L.; Wertheim-van Dillen, P.M.; van der Noordaa, J. Rapid and simple method for purification of nucleic acids. J. Clin. Microbiol. 1990, 28, 495–503. [Google Scholar] [CrossRef] [Green Version]
- Van Oordt, T.; Barb, Y.; Smetana, J.; Zengerle, R.; von Stetten, F. Miniature stick-packaging—An industrial technology for pre-storage and release of reagents in lab-on-a-chip systems. Lab Chip 2013, 13, 2888–2892. [Google Scholar] [CrossRef]
- Hin, S.; Paust, N.; Rombach, M.; Lüddecke, J.; Specht, M.; Zengerle, R.; Mitsakakis, M. Minimizing ethanol carry-over in centrifugal microfluidic nucleic acid extraction by advanced bead handling and management of diffusive mass transfer. In Proceedings of the 20th International Conference on Solid-State Sensors, Actuators and Microsystems & Eurosensors XXXIII, Berlin, Germany, 23–27 June 2019. [Google Scholar] [CrossRef]
- Keller, M.; Czilwik, G.; Schott, J.; Schwarz, I.; Dormanns, K.; von Stetten, F.; Zengerle, R.; Paust, N. Robust temperature change rate actuated valving and switching for highly integrated centrifugal microfluidics. Lab Chip 2017, 17, 864–875. [Google Scholar] [CrossRef]
- Zehnle, S.; Schwemmer, F.; Roth, G.; von Stetten, F.; Zengerle, R.; Paust, N. Centrifugo-dynamic inward pumping of liquids on a centrifugal microfluidic platform. Lab Chip 2012, 12, 5142–5145. [Google Scholar] [CrossRef] [Green Version]
- Hin, S.; Paust, N.; Keller, M.; Rombach, M.; Strohmeier, O.; Zengerle, R.; Mitsakakis, K. Temperature change rate actuated bubble mixing for homogeneous rehydration of dry pre-stored reagents in centrifugal microfluidics. Lab Chip 2018, 18, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Mark, D.; Weber, P.; Lutz, S.; Focke, M.; Zengerle, R.; von Stetten, F. Aliquoting on the centrifugal microfluidic platform based on centrifugo-pneumatic valves. Microfluid. Nanofluid. 2011, 10, 1279–1288. [Google Scholar] [CrossRef]
- Focke, M.; Stumpf, F.; Faltin, B.; Reith, P.; Bamarni, D.; Wadle, S.; Müller, C.; Reinecke, H.; Schrenzel, J.; Francois, P. Microstructuring of polymer films for sensitive genotyping by real-time PCR on a centrifugal microfluidic platform. Lab Chip 2010, 10, 2519–2526. [Google Scholar] [CrossRef]
- Focke, M.; Kosse, D.; Al-Bamerni, D.; Lutz, S.; Müller, C.; Reinecke, H.; Zengerle, R.; von Stetten, F. Microthermoforming of microfluidic substrates by soft lithography (µTSL): Optimization using design of experiments. J. Micromech. Microeng. 2011, 21, 115002. [Google Scholar] [CrossRef]
- Hahn-Schickard, Lab-on-a-Chip Foundry Service. Available online: https://www.hahn-schickard.de/en/production/lab-on-a-chip-foundry (accessed on 30 September 2021).
- Rombach, M.; Kosse, D.; Faltin, B.; Wadle, S.; Roth, G.; Zengerle, R.; von Stetten, F. Real-time stability testing of air-dried primers and fluorogenic hydrolysis probes stabilized by trehalose and xanthan. BioTechniques 2014, 57, 151–155. [Google Scholar] [CrossRef] [Green Version]
- Hin, S.; Baumgartner, D.; Specht, M.; Lüddecke, J.; Arjmand, E.M.; Johannsen, B.; Schiedel, L.; Rombach, M.; Paust, N.; von Stetten, F.; et al. VectorDisk: A Microfluidic Platform Integrating Mosquito Vector Markers for Evidence Based Control Applications. Processes 2020, 8, 1677. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015; Available online: https://www.R-project.org/ (accessed on 23 October 2021).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; D’Agostino McGowan, L.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Mitsakakis, K.; D’Acremont, V.; Hin, S.; von Stetten, F.; Zengerle, R. Diagnostic tools for tackling febrile illness and enhancing patient management. Microelectron. Eng. 2018, 201, 26–59. [Google Scholar] [CrossRef]
- Righolt, A.; Jevdejvic, M.; Marcenes, W.; Listl, S. Global-, Regional-, and Country-Level Economic Impacts of Dental Diseases in 2015. J. Dent. Res. 2018, 97, 501–507. [Google Scholar] [CrossRef]
- Cullinan, M.P.; Ford, P.J.; Seymour, G.J. Periodontal disease and systemic health: Current status. Aust. Dent. J. 2009, 54 Suppl. 1, S62–S69. [Google Scholar] [CrossRef]
- Seymour, G.J.; Ford, P.J.; Cullinan, M.P.; Leishman, S.; Yamazaki, K. Relationship between periodontal infections and systemic disease. Clin. Microbiol. Infect. 2007, 13, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Grigoriadis, A.; Sorsa, T.; Raisanen, I.; Parnanen, P.; Tervahartiala, T.; Sakellari, D. Prediabetes/Diabetes Can Be Screened at the Dental Office by a Low-Cost and Fast Chair-Side/Point-of-Care aMMP-8 Immunotest. Diagnostics 2019, 9, 151. [Google Scholar] [CrossRef] [Green Version]
- Smits, K.P.J.; Listl, S.; Plachokova, A.S.; Van der Galien, O.; Kalmus, O. Effect of periodontal treatment on diabetes-related healthcare costs: A retrospective study. BMJ Open Diab. Res. Care 2020, 8, e001666. [Google Scholar] [CrossRef]
- Website of Dentognostics GmbH. Available online: https://www.dentognostics.de/en/ (accessed on 30 September 2021).
- Leppilahti, J.M.; Ahonen, M.M.; Hernandez, M.; Munjal, S.; Netuschil, L.; Uitto, V.J.; Sorsa, T.; Mantyla, P. Oral rinse MMP-8 point-of-care immuno test identifies patients with strong periodontal inflammatory burden. Oral Dis. 2011, 17, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Borujeni, S.I.; Mayer, M.; Eickholz, P. Activated matrix metalloproteinase-8 in saliva as diagnostic test for periodontal disease? A case-control study. Med. Microbiol. Immunol. 2015, 204, 665–672. [Google Scholar] [CrossRef]
- Al-Majid, A.; Alassiri, S.; Rathnayake, N.; Tervahartiala, T.; Gieselmann, D.R.; Sorsa, T. Matrix Metalloproteinase-8 as an Inflammatory and Prevention Biomarker in Periodontal and Peri-Implant Diseases. Int. J. Dent. 2018, 2018, 7891323. [Google Scholar] [CrossRef]
- Website of OralDNA Labs, MyPerioPath®. Available online: https://www.oraldna.com/test/myperiopath/ (accessed on 30 September 2021).
- Website of Direct Diagnostics. Available online: https://www.directdiagnostics.com/hr5 (accessed on 30 September 2021).
- Website of PerioPOC®. Available online: https://en.periopoc.com/ (accessed on 30 September 2021).
- Arweiler, N.B.; Marx, V.K.; Laugisch, O.; Sculean, A.; Auschill, T.M. Clinical evaluation of a newly developed chairside test to determine periodontal pathogens. J. Periodontol. 2019, 91, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Bellagambi, F.G.; Lomonaco, T.; Salvo, P.; Vivaldi, F.; Hangouet, M.; Ghimenti, S.; Biagini, D.; Di Francesco, F.; Fuoco, R.; Errachid, A. Saliva sampling: Methods and devices. An overview. TrAC Trends Anal. Chem. 2020, 124, 115781. [Google Scholar] [CrossRef]
- Khurshid, Z.; Zohaib, S.; Najeeb, S.; Zafar, M.S.; Slowey, P.D.; Almas, K. Human Saliva Collection Devices for Proteomics: An Update. Int. J. Mol. Sci. 2016, 17, 846. [Google Scholar] [CrossRef] [Green Version]
- Khanna, P.; Walt, D.R. Salivary diagnostics using a portable point-of-service platform: A Review. Clin. Ther. 2015, 37, 498–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, E.; Bond, K.; Zhang, B.; Putland, M.; Williamson, D.A. Saliva as a Noninvasive Specimen for Detection of SARS-CoV-2. J. Clin. Microbiol. 2020, 58, e00776-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- To, K.K.-W.; Tsang, O.T.-Y.; Yip, C.C.-Y.; Chan, K.-H.; Wu, T.-C.; Chan, J.M.-C.; Leung, W.-S.; Chik, T.S.-H.; Choi, C.Y.-C.; Kandamby, D.H.; et al. Consistent Detection of 2019 Novel Coronavirus in Saliva. Clin. Infect. Dis. 2020, 71, 841–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, R.; Maasdorp, E.; Malherbe, S.; Loxton, A.G.; Stanley, K.; van der Spuy, G.; Walzl, G.; Chegou, N.N. Diagnostic Potential of Novel Salivary Host Biomarkers as Candidates for the Immunological Diagnosis of Tuberculosis Disease and Monitoring of Tuberculosis Treatment Response. PLoS ONE 2016, 11, e0160546. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.S.; Khurshid, Z.; Asiri, F.Y.I. Advancing Point-of-Care (PoC) Testing Using Human Saliva as Liquid Biopsy. Diagnostics 2017, 7, 39. [Google Scholar] [CrossRef]
- Rathnayake, N.; Gieselmann, D.R.; Heikkinen, A.M.; Tervahartiala, T.; Sorsa, T. Salivary Diagnostics: Point-of-Care diagnostics of MMP-8 in dentistry and medicine. Diagnostics 2017, 7, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, S.; Choi, Y. Point-of-care diagnosis of periodontitis using saliva: Technically feasible but still a challenge. Front. Cell. Infect. Microbiol. 2015, 5, 65. [Google Scholar] [CrossRef]
- Johannsen, B.; Müller, L.; Baumgartner, D.; Karkossa, L.; Fruh, S.M.; Bostanci, N.; Karpisek, M.; Zengerle, R.; Paust, N.; Mitsakakis, K. Automated Pre-Analytic Processing of Whole Saliva Using Magnet-Beating for Point-of-Care Protein Biomarker Analysis. Micromachines 2019, 10, 833. [Google Scholar] [CrossRef] [Green Version]
- De Boer, R.; Peters, R.; Gierveld, S.; Schuurman, T.; Kooistra-Smid, M.; Savelkoul, P. Improved detection of microbial DNA after bead-beating before DNA isolation. J. Microbiol. Methods 2010, 80, 209–211. [Google Scholar] [CrossRef]
- Li, X.L.; Bosch-Tijhof, C.J.; Wei, X.; de Soet, J.J.; Crielaard, W.; van Loveren, C.; Deng, D.M. Efficiency of chemical versus mechanical disruption methods of DNA extraction for the identification of oral Gram-positive and Gram-negative bacteria. J. Int. Med. Res. 2020, 48, 0300060520925594. [Google Scholar]
- Larsen, T.; Fiehn, N.E. Dental biofilm infections—An update. Apmis 2017, 125, 376–384. [Google Scholar] [CrossRef]
- Belibasakis, G.N.; Bostanci, N.; Marsh, P.D.; Zaura, E. Applications of the oral microbiome in personalized dentistry. Arch. Oral Biol. 2019, 104, 7–12. [Google Scholar] [CrossRef]
- Paqué, P.N.; Herz, C.; Wiedemeier, D.B.; Mitsakakis, K.; Attin, T.; Bao, K.; Belibasakis, G.N.; Hays, J.P.; Jenzer, J.S.; Kaman, W.E.; et al. Salivary Biomarkers for Dental Caries Detection and Personalized Monitoring. J. Pers. Med. 2021, 11, 235. [Google Scholar] [CrossRef]
- Zhao, Y.; Czilwik, G.; Klein, V.; Mitsakakis, K.; Zengerle, R.; Paust, N. C-reactive protein and interleukin 6 microfluidic immunoassays with on-chip pre-stored reagents and centrifugo-pneumatic liquid control. Lab Chip 2017, 17, 1666–1677. [Google Scholar] [CrossRef]
- Johannsen, J.; Karpíšek, M.; Baumgartner, D.; Klein, V.; Bostanci, N.; Paust, N.; Früh, S.M.; Zengerle, R.; Mitsakakis, K. One-step, wash-free, bead-based immunoassay employing bound-free phase detection. Anal. Chim. Acta 2021, 1153, 338280. [Google Scholar] [CrossRef]
- Mitsakakis, K. Novel lab-on-a-disk platforms: A powerful tool for molecular fingerprinting of oral and respiratory tract infections. Expert Rev. Mol. Diagn. 2021, 21, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Seitz, M.W.; Haux, C.; Smits, K.P.J.; Kalmus, O.; Van Der Zande, M.M.; Lutyj, J.; Listl, S. Development and evaluation of a mobile patient application to enhance medical-dental integration for the treatment of periodontitis and diabetes. Int. J. Med. Inform. 2021, 152, 104495. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ch.1 | Ch.2 | Ch.3 | Ch.4 | Ch.5 | Ch.6 | Ch.7 | Ch.8 | Ch.9 | Ch.10 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| A. actinomycetemcomitans | C. rectus | F. nucleatum | P. intermedia | P. gingivalis | T. forsythia | T. denticola | Lactobacillus spp. | S. mutans | S. sobrinus | Number of Pos., Neg. over Total Assay Targets | |
| Lab-reference Pos. | 4 | 23 a | 23 a | 24 | 22 a | 22 a | 15 | 11 | 24 | 7 | 175/234 |
| Lab-reference Neg. | 20 | 0 | 0 | 0 | 0 | 0 | 9 | 13 | 0 | 17 | 59/234 |
| (a) OralDisk Pos. and Lab-reference Pos. | 1 | 21 | 16 | 22 | 22 | 22 | 15 | 7 | 22 | 6 | 154/175 (88.0%) |
| (b) OralDisk Pos. and Lab-reference Neg. | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 5 | 0 | 0 | 7/59 (11.9%) |
| (c) OralDisk Neg. and Lab-reference Neg. | 20 | 0 | 0 | 0 | 0 | 0 | 7 | 8 | 0 | 17 | 52/59 (88.1%) |
| (d) OralDisk Neg. and Lab-reference Pos. | 3 | 2 | 7 | 2 | 0 | 0 | 0 | 4 | 2 | 1 | 21/175 (12.0%) |
| Ch.1 | Ch.2 | Ch.3 | Ch.4 | Ch.5 | Ch.6 | Ch.7 | Ch.8 | Ch.9 | Ch.10 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| A. actinomycetemcomitans | C. rectus | F. nucleatum | P. intermedia | P. gingivalis | T. forsythia | T. denticola | Lactoba- cillus spp. | S. mutans | S. sobrinus | Number of Pos., Neg. Assay Targets | |
| OralDisk Pos. | 1 | 16 | 16 | 16 | 12 | 61 | |||||
| iai PadoTest Pos. | 0 | 7 | 8 | 3 | 10 | 28 | |||||
| OralDisk Neg. | 17 | 2 | 0 | 0 | 6 | 25 | |||||
| iai PadoTest Neg. | 18 | 11 | 8 | 13 | 8 | 58 |
| Number of Cases with Cq(Lab-Reference) > Cq(OralDisk) | Number of Cases with Cq(Lab-Reference) < Cq(OralDisk) | TOTAL Cases | |||
|---|---|---|---|---|---|
| For all bacteria in all groups | 80 | 51.9% | 74 | 48.1% | 154 |
| For all bacteria in healthy group | 12 | 35.3% | 22 | 64.7% | 34 |
| For all bacteria in caries group | 41 | 55.9% | 30 | 44.1% | 68 |
| For all bacteria in periodontitis group | 27 | 57.7% | 22 | 42.3% | 52 |
| For A. actinomycetemcomitans in all groups | 0 | 0.0% | 1 | 100.0% | 1 |
| For C. rectus in all groups | 15 | 71.4% | 6 | 28.6% | 21 |
| For F. nucleatum in all groups | 8 | 53.3% | 7 | 46.7% | 15 |
| For P. intermedia in all groups | 10 | 45.5% | 12 | 54.5% | 22 |
| For P. gingivalis in all groups | 17 | 77.3% | 5 | 22.7% | 22 |
| For T. forsythia in all groups | 16 | 72.7% | 6 | 27.3% | 22 |
| For T. denitcola in all groups | 8 | 50.0% | 8 | 50.0% | 16 |
| For Lactobacillus spp. in all groups | 1 | 14.3% | 6 | 85.7% | 7 |
| For S. mutans in all groups | 4 | 18.2% | 18 | 81.8% | 22 |
| For S. sobrinus in all groups | 1 | 16.7% | 5 | 83.3% | 6 |
| Characteristics | PerioSafe® | iai PadoTest | MyPerioPath® | PerioPOC® | HR5TM | OralDisk |
|---|---|---|---|---|---|---|
| Saliva sampling | Yes (Oral rinse) | No (Probe) | Yes | No (Probe) | Yes | Yes |
| Chair-side compatible | Yes | No (Requires lab) | No (Requires lab) | Yes | No (Requires lab) | Yes a |
| Quantitative capacity | Yes/No (LFT) b | Yes (qPCR) | Yes (qPCR) | No (LFT) c | Yes (qPCR) | Yes (qPCR) |
| Caries panel included | No | No | No | No | No | Yes |
| Number of bacteria in panel, tested per run | None (detects aMMP-8 biomarker) | 6 | 11 | 5 | 5 | 10 |
| Bacteria panel | ||||||
| Aggregatibacter actinomycetemcomitans | - | X | X | X | X | X |
| Tannerella forsythia | - | X | X | X | X | X |
| Porphyromonas gingivalis | - | X | X | X | X | X |
| Treponema denticola | - | X | X | X | - | X |
| Prevotella intermedia | - | X | X | X | X | X |
| Filifactor alocis | - | X | - | - | - | - |
| Fusobacterium nucleatum | - | - | X | - | X | X |
| Campylobacter rectus | - | - | X | - | - | X |
| Capnocytophaga species (gingivalis, ochracea, sputigena) | - | - | X | - | - | - |
| Streptococcus mutans | - | - | - | - | - | X |
| Streptococcus sobrinus | - | - | - | - | - | X |
| Lactobacillus spp. | - | - | - | - | - | X |
| Peptostreptococcus micros | - | - | X | - | - | - |
| Eikenella corrodens | - | - | X | - | - | - |
| Eubacterium nodatum | - | - | X | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baumgartner, D.; Johannsen, B.; Specht, M.; Lüddecke, J.; Rombach, M.; Hin, S.; Paust, N.; von Stetten, F.; Zengerle, R.; Herz, C.; et al. OralDisk: A Chair-Side Compatible Molecular Platform Using Whole Saliva for Monitoring Oral Health at the Dental Practice. Biosensors 2021, 11, 423. https://0-doi-org.brum.beds.ac.uk/10.3390/bios11110423
Baumgartner D, Johannsen B, Specht M, Lüddecke J, Rombach M, Hin S, Paust N, von Stetten F, Zengerle R, Herz C, et al. OralDisk: A Chair-Side Compatible Molecular Platform Using Whole Saliva for Monitoring Oral Health at the Dental Practice. Biosensors. 2021; 11(11):423. https://0-doi-org.brum.beds.ac.uk/10.3390/bios11110423
Chicago/Turabian StyleBaumgartner, Desirée, Benita Johannsen, Mara Specht, Jan Lüddecke, Markus Rombach, Sebastian Hin, Nils Paust, Felix von Stetten, Roland Zengerle, Christopher Herz, and et al. 2021. "OralDisk: A Chair-Side Compatible Molecular Platform Using Whole Saliva for Monitoring Oral Health at the Dental Practice" Biosensors 11, no. 11: 423. https://0-doi-org.brum.beds.ac.uk/10.3390/bios11110423