Impact of Scala Tympani Geometry on Insertion Forces during Implantation

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
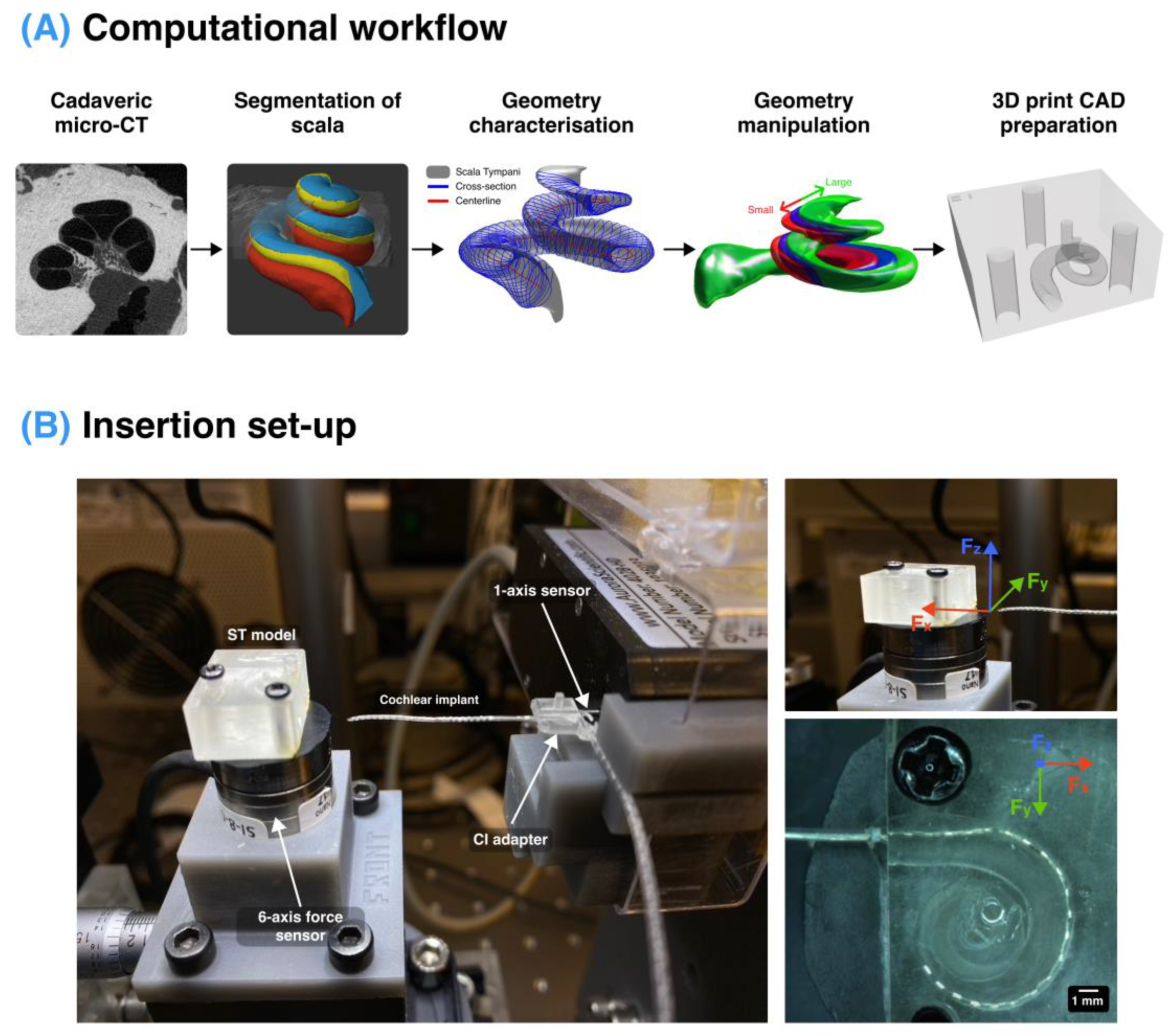
2.1. Micro-CT Segmentation of Scala Tympani
2.2. Characterisation of Scala Tympani
2.3. Manipulation of Scala Tympani Shape
2.3.1. Cochlear Size Manipulation
2.3.2. Vertical Trajectory Manipulation
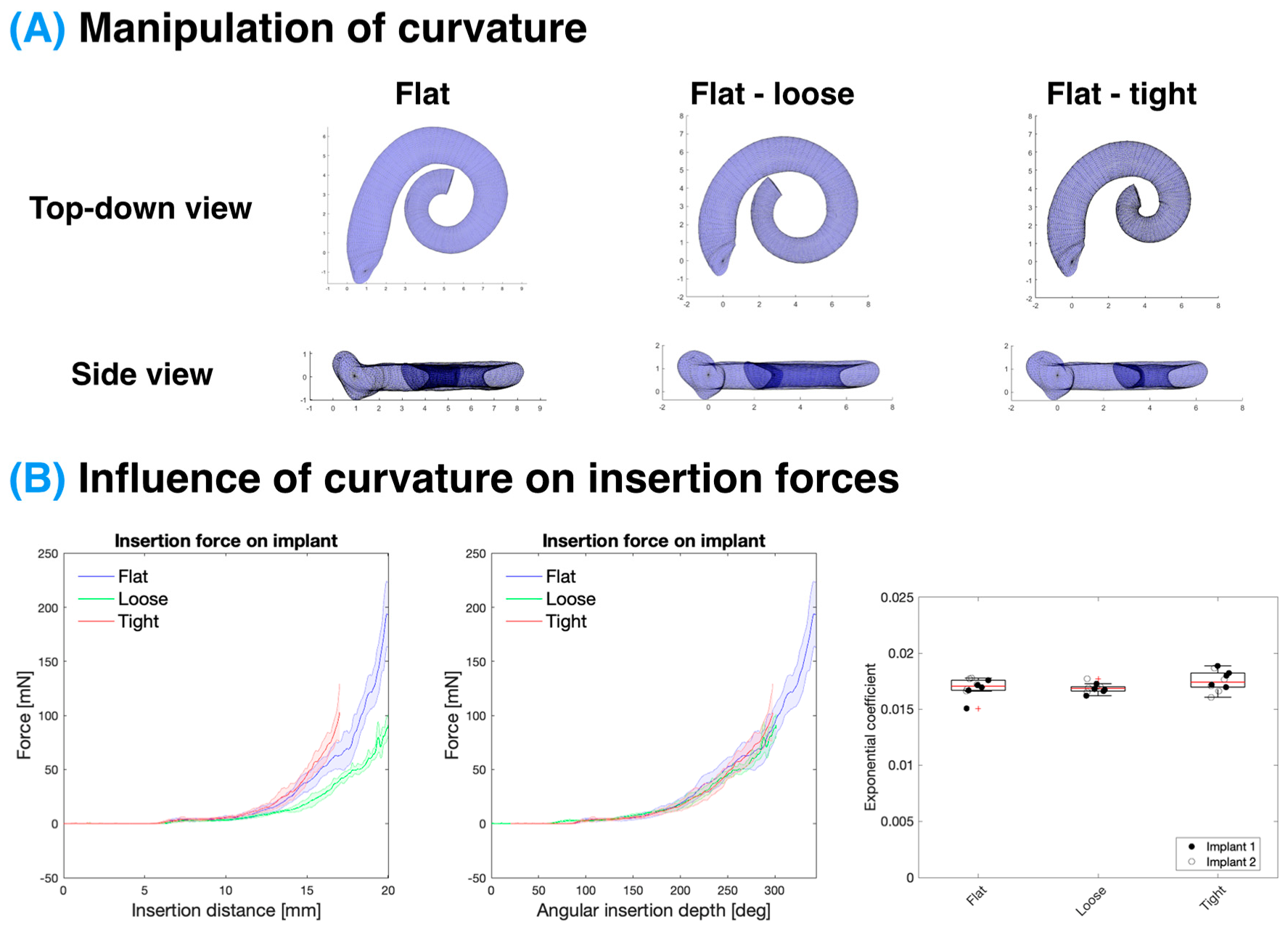
2.3.3. Curvature Manipulation
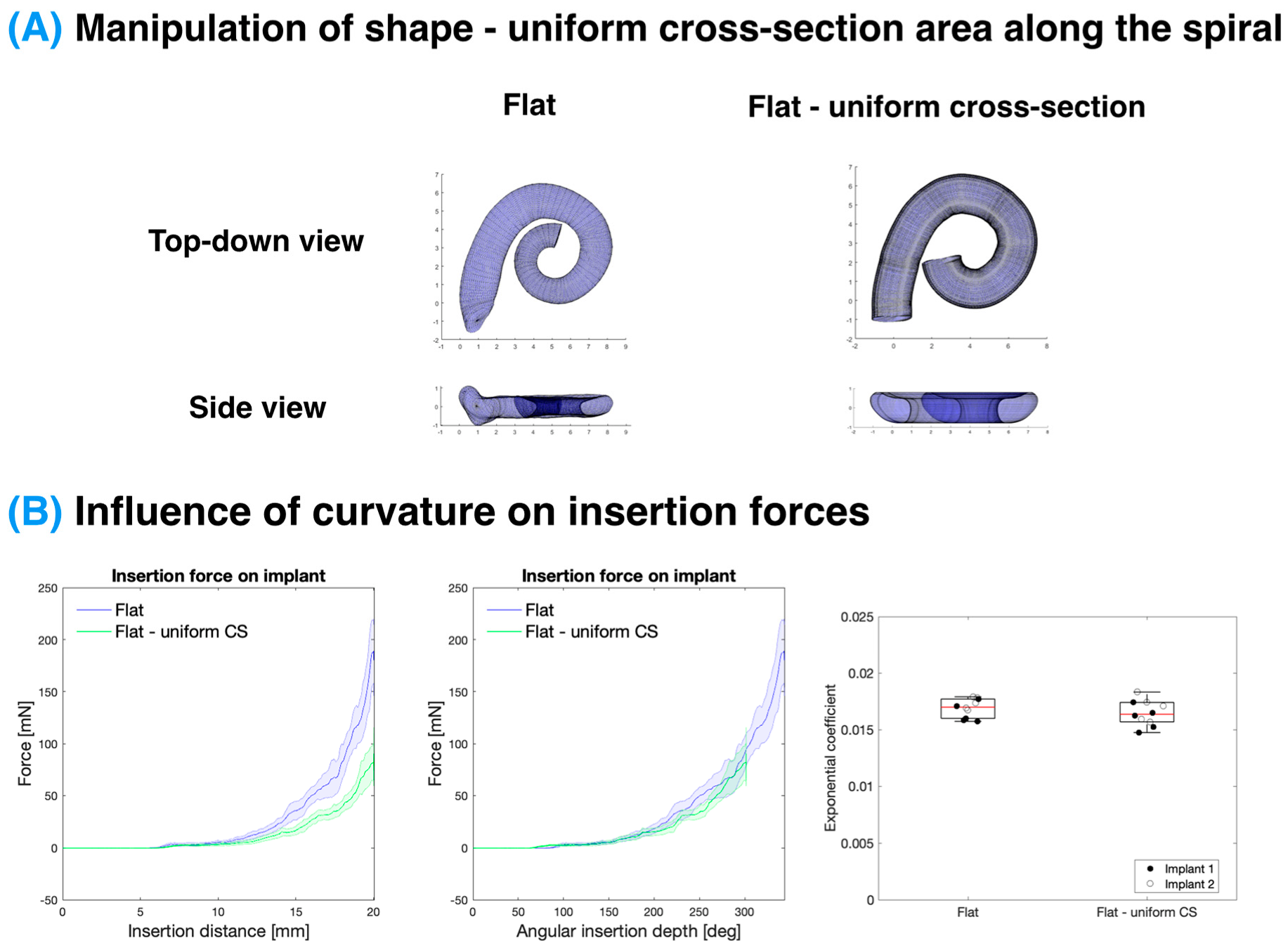
2.3.4. Uniform Cross-Section Models
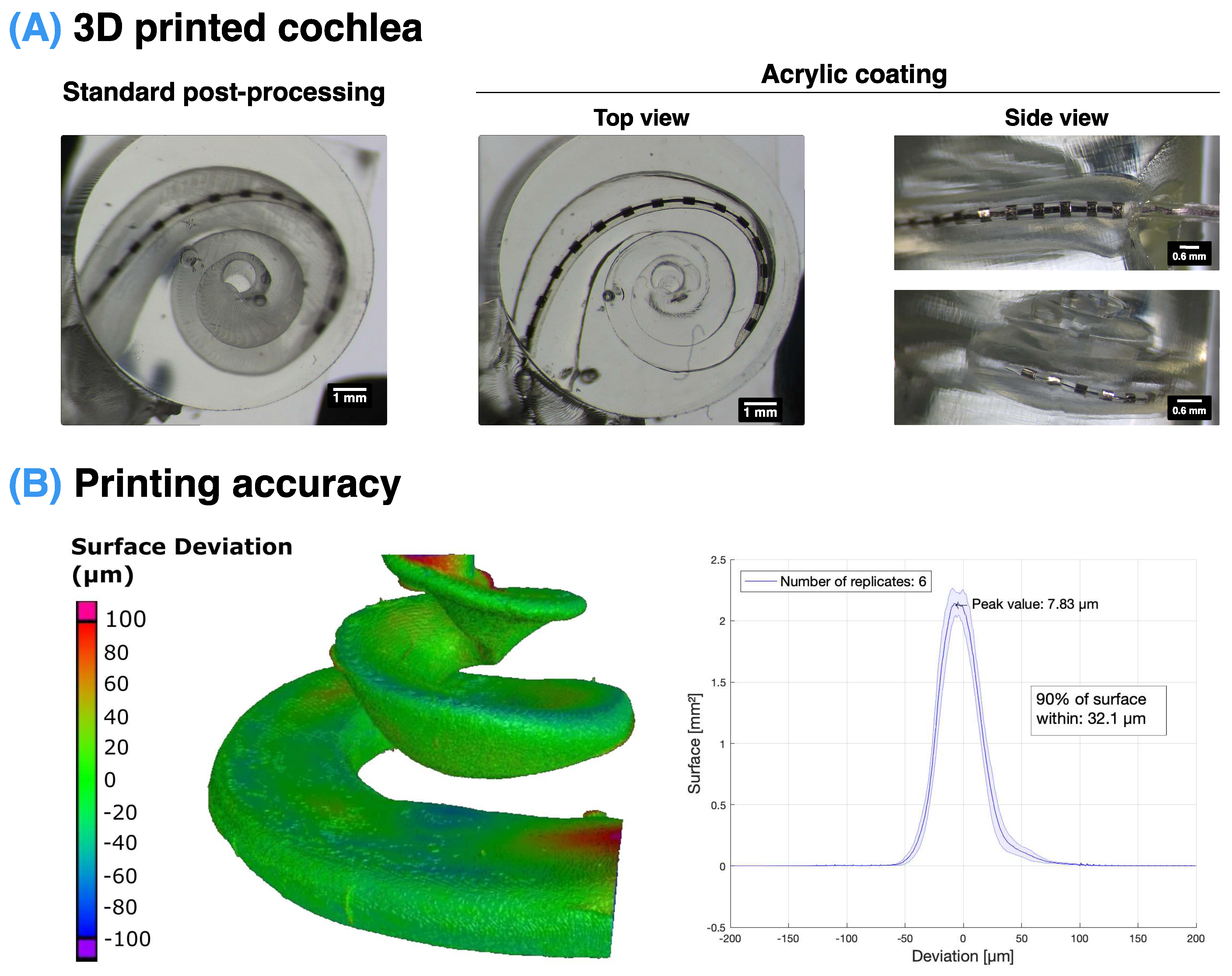
2.4. 3D Printing an Artificial Scala Tympani
2.5. Insertion Setup
2.6. Fitting of Insertion Forces to a Capstan Model
Capstan Model
2.7. Statistical Analysis
3. Results
3.1. Insertion Setup with Accurate Scala Tympani Model
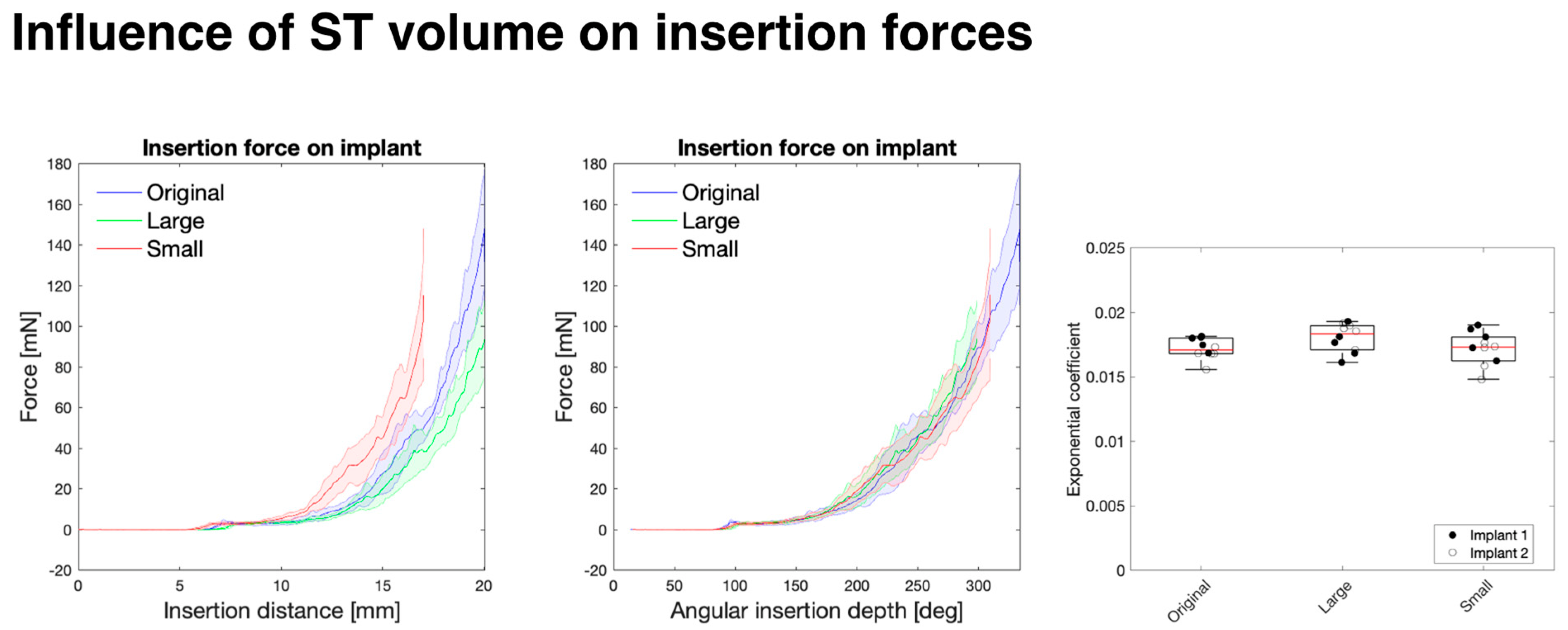
3.2. Influence of Overall Size on Insertion Force
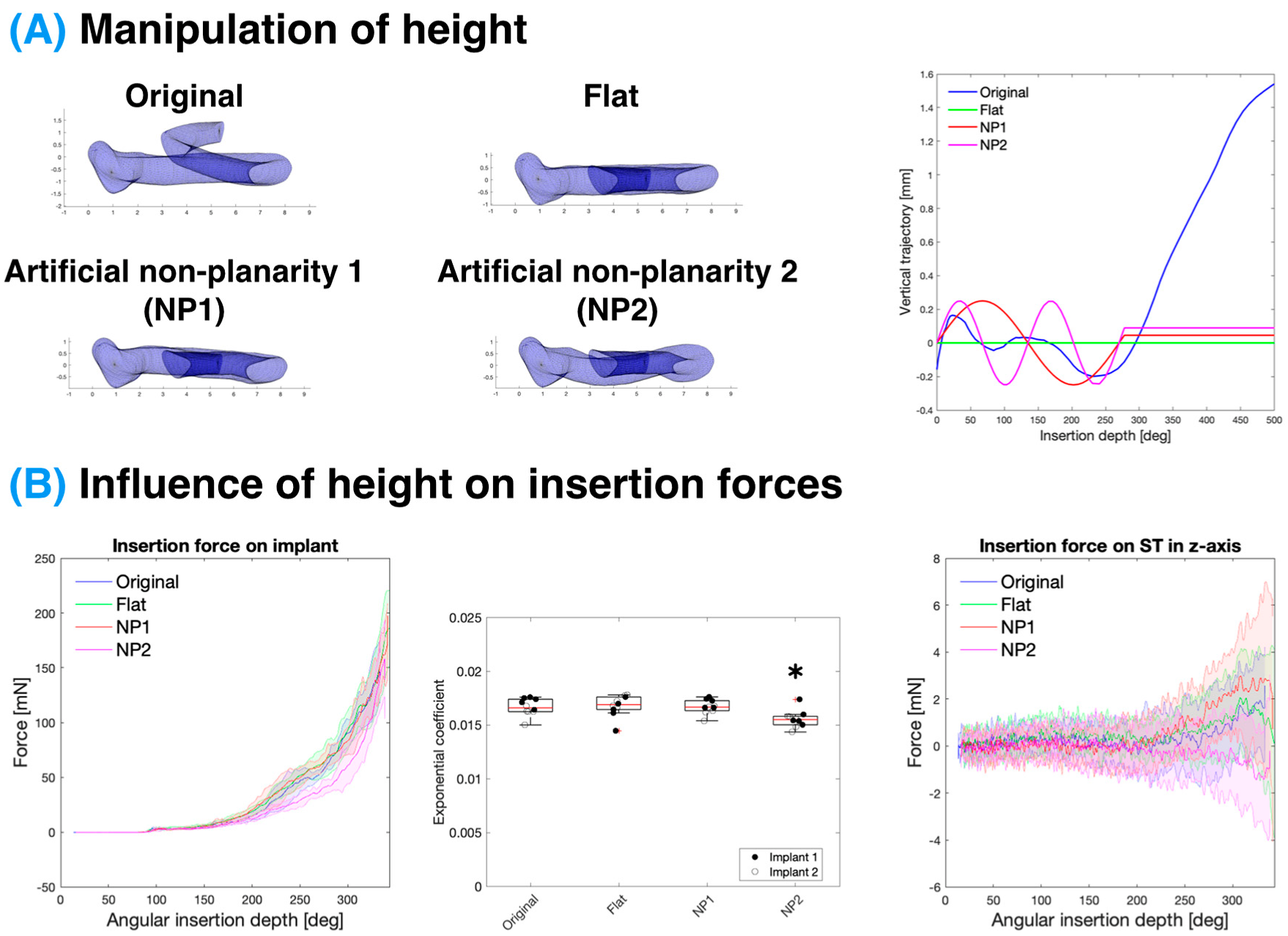
3.3. Influence of Scala Tympani Vertical Trajectory on Insertion Forces
3.4. Influence of ST Curvature on Insertion Forces
3.5. Influence of ST Cross-Sectional Area on Insertion Forces
4. Discussion
4.1. Comparison with Previous Work
4.2. Impact of ST Shape on Insertion Forces
4.2.1. Effect of ST Vertical Trajectory
4.2.2. Effect of Curvature
4.2.3. Effect of Cross-Sectional Area
4.3. Comparison with Surgical Approach
4.4. Impact of Vertical Forces
4.5. Stress Relaxation of CI
4.6. Consequences of Capstan Model
4.7. Limitations of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deafness and Hearing Loss. Available online: https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss (accessed on 22 June 2022).
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Adigun, O.T. Depression and Individuals with Hearing Loss: A Systematic Review. J. Psychol. Psychother. 2017, 7, 1000323. [Google Scholar] [CrossRef]
- Cosh, S.; Carriere, I.; Daien, V.; Amieva, H.; Tzourio, C.; Delcourt, C.; Helmer, C.; the Sense-Cog Consortium. The relationship between hearing loss in older adults and depression over 12 years: Findings from the Three-City prospective cohort study. Int. J. Geriatr. Psychiatry 2018, 33, 1654–1661. [Google Scholar] [CrossRef] [PubMed]
- Cosh, S.; Carriere, I.; Delcourt, C.; Helmer, C.; the Sense-Cog Consortium. A dimensional approach to understanding the relationship between self-reported hearing loss and depression over 12 years: The Three-City study. Aging Ment. Health 2021, 25, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Li, C.-M.; Zhang, X.; Hoffman, H.J.; Cotch, M.F.; Themann, C.L.; Wilson, M.R. Hearing Impairment Associated With Depression in US Adults, National Health and Nutrition Examination Survey 2005–2010. JAMA Otolaryngol. Neck Surg. 2014, 140, 293–302. [Google Scholar] [CrossRef] [Green Version]
- Mener, D.J.; Betz, J.; Genther, D.J.; Chen, D.; Lin, F.R. Hearing Loss and Depression in Older Adults. J. Am. Geriatr. Soc. 2013, 61, 1627–1629. [Google Scholar] [CrossRef] [Green Version]
- Ford, A.H.; Hankey, G.J.; Yeap, B.B.; Golledge, J.; Flicker, L.; Almeida, O.P. Hearing loss and the risk of dementia in later life. Maturitas 2018, 112, 1–11. [Google Scholar] [CrossRef]
- Hardy, C.J.D.; Marshall, C.R.; Golden, H.L.; Clark, C.N.; Mummery, C.J.; Griffiths, T.D.; Bamiou, D.-E.; Warren, J.D. Hearing and dementia. J. Neurol. 2016, 263, 2339–2354. [Google Scholar] [CrossRef] [Green Version]
- Nadhimi, Y.; Llano, D.A. Does hearing loss lead to dementia? A review of the literature. Hear. Res. 2021, 402, 108038. [Google Scholar] [CrossRef]
- Uhlmann, R.F.; Larson, E.B.; Rees, T.S.; Koepsell, T.D.; Duckert, L.G. Relationship of Hearing Impairment to Dementia and Cognitive Dysfunction in Older Adults. JAMA 1989, 261, 1916–1919. [Google Scholar] [CrossRef]
- Chen, D.S.; Genther, D.J.; Betz, J.; Lin, F.R. Association Between Hearing Impairment and Self-Reported Difficulty in Physical Functioning. J. Am. Geriatr. Soc. 2014, 62, 850–856. [Google Scholar] [CrossRef] [Green Version]
- Eriksson-Mangold, M.; Carlsson, S.G. Psychological and somatic distress in relation to perceived hearing disability, hearing handicap, and hearing measurements. J. Psychosom. Res. 1991, 35, 729–740. [Google Scholar] [CrossRef]
- Yamada, M.; Nishiwaki, Y.; Michikawa, T.; Takebayashi, T. Impact of hearing difficulty on dependence in activities of daily living (ADL) and mortality: A 3-year cohort study of community-dwelling Japanese older adults. Arch. Gerontol. Geriatr. 2011, 52, 245–249. [Google Scholar] [CrossRef]
- Jia, H.; Wang, J.; François, F.; Uziel, A.; Puel, J.-L.; Venail, F. Molecular and Cellular Mechanisms of Loss of Residual Hearing after Cochlear Implantation. Ann. Otol. Rhinol. Laryngol. 2013, 122, 33–39. [Google Scholar] [CrossRef]
- Zanetti, D.; Nassif, N.; Redaelli De Zinis, L.O. Fattori influenzanti la conservazione dei residui uditivi negli impianti cocleari. Acta Otorhinolaryngol. Ital. 2015, 35, 433–441. [Google Scholar] [CrossRef]
- Eshraghi, A.A.; Ahmed, J.; Krysiak, E.; Ila, K.; Ashman, P.; Telischi, F.F.; Angeli, S.; Prentiss, S.; Martinez, D.; Valendia, S. Clinical, surgical, and electrical factors impacting residual hearing in cochlear implant surgery. Acta Otolaryngol. 2017, 137, 384–388. [Google Scholar] [CrossRef]
- Hoskison, E.; Mitchell, S.; Coulson, C. Systematic review: Radiological and histological evidence of cochlear implant insertion trauma in adult patients. Cochlear Implants Int. 2017, 18, 192–197. [Google Scholar] [CrossRef]
- O’Leary, M.J.; House, W.F.; Fayad, J.; Linthicum, F.H. Electrode Insertion Trauma in Cochlear Implantation. Ann. Otol. Rhinol. Laryngol. 1991, 100, 695–699. [Google Scholar] [CrossRef]
- Zhou, L.; Friedmann, D.R.; Treaba, C.; Peng, R.; Roland, J.T., Jr. Does cochleostomy location influence electrode trajectory and intracochlear trauma? Laryngoscope 2015, 125, 966–971. [Google Scholar] [CrossRef]
- Shishodia, S.; Saurav, D. Round window versus conventional bony cochleostomy technique in pediatric cochlear implantation; A Randomized controlled double blinded trial. Int. J. Otorhinolaryngol. Head Neck Surg. 2021, 7, 1297. [Google Scholar] [CrossRef]
- Jiam, N.T.; Limb, C.J. The impact of round window vs cochleostomy surgical approaches on interscalar excursions in the cochlea: Preliminary results from a flat-panel computed tomography study. World J. Otorhinolaryngol.-Head Neck Surg. 2016, 2, 142–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demir, B.; Yüksel, M.; Atılgan, A.; Ciprut, A.; Batman, C. Spectral resolution and speech perception after cochlear implantation using the round window versus cochleostomy technique. J. Laryngol. Otol. 2021, 135, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Carlson, M.L.; O’Connell, B.P.; Lohse, C.M.; Driscoll, C.L.; Sweeney, A.D. Survey of the American Neurotology Society on Cochlear Implantation: Part 2, Surgical and Device-Related Practice Patterns. Otol. Neurotol. 2018, 39, e20. [Google Scholar] [CrossRef] [PubMed]
- Avasarala, V.S.; Jinka, S.K.; Jeyakumar, A. Complications of Cochleostomy Versus Round Window Surgical Approaches: A Systematic Review and Meta-Analysis. Cureus 2022, 14, e25451. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, E.R.; Waltzman, S.B.; Landsberger, D.M.; Friedmann, D.R. Acceptance and Benefits of Electro-Acoustic Stimulation for Conventional-Length Electrode Arrays. Audiol. Neurotol. 2021, 26, 17–26. [Google Scholar] [CrossRef]
- Irving, S.; Gillespie, L.; Richardson, R.; Rowe, D.; Fallon, J.B.; Wise, A.K. Electroacoustic Stimulation: Now and into the Future. BioMed Res. Int. 2014, 2014, e350504. [Google Scholar] [CrossRef] [Green Version]
- Incerti, P.V.; Ching, T.Y.C.; Cowan, R. A Systematic Review of Electric-Acoustic Stimulation: Device Fitting Ranges, Outcomes, and Clinical Fitting Practices. Trends Amplif. 2013, 17, 3–26. [Google Scholar] [CrossRef] [Green Version]
- Dorman, M.F.; Gifford, R.H.; Spahr, A.J.; McKarns, S.A. The Benefits of Combining Acoustic and Electric Stimulation for the Recognition of Speech, Voice and Melodies. Audiol. Neurotol. 2008, 13, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Kim, S.M.; Wang, W.; Cai, C.; Feng, Y.; Kong, W.; Lin, X. Cochlear Gene Therapy for Sensorineural Hearing Loss: Current Status and Major Remaining Hurdles for Translational Success. Front. Mol. Neurosci. 2018, 11, 221. [Google Scholar] [CrossRef]
- Roland, P.S.; Wright, C.G. Surgical Aspects of Cochlear Implantation: Mechanisms of Insertional Trauma. Cochlear Brainstem Implants 2006, 64, 11–30. [Google Scholar] [CrossRef]
- Boggess, W.J.; Baker, J.E.; Balkany, T.J. Loss of residual hearing after cochlear implantation. Laryngoscope 1989, 99, 1002–1005. [Google Scholar] [CrossRef]
- Kaufmann, C.R.; Henslee, A.M.; Claussen, A.; Hansen, M.R. Evaluation of Insertion Forces and Cochlea Trauma Following Robotics-Assisted Cochlear Implant Electrode Array Insertion. Otol. Neurotol. 2020, 41, 631–638. [Google Scholar] [CrossRef]
- Carlson, M.L.; Driscoll, C.L.W.; Gifford, R.H.; Service, G.J.; Tombers, N.M.; Hughes-Borst, B.J.; Neff, B.A.; Beatty, C.W. Implications of Minimizing Trauma During Conventional Cochlear Implantation. Otol. Neurotol. 2011, 32, 962–968. [Google Scholar] [CrossRef] [Green Version]
- Holden, L.K.; Finley, C.C.; Firszt, J.B.; Holden, T.A.; Brenner, C.; Potts, L.G.; Gotter, B.D.; Vanderhoof, S.S.; Mispagel, K.; Heydebrand, G.; et al. Factors affecting open-set word recognition in adults with cochlear implants. Ear Hear. 2013, 34, 342–360. [Google Scholar] [CrossRef] [Green Version]
- Choong, J.K.; Hampson, A.J.; Brody, K.M.; Lo, J.; Bester, C.W.; Gummer, A.W.; Reynolds, N.P.; O’Leary, S.J. Nanomechanical mapping reveals localized stiffening of the basilar membrane after cochlear implantation. Hear. Res. 2020, 385, 107846. [Google Scholar] [CrossRef]
- De Seta, D.; Torres, R.; Russo, F.Y.; Ferrary, E.; Kazmitcheff, G.; Heymann, D.; Amiaud, J.; Sterkers, O.; Bernardeschi, D.; Nguyen, Y. Damage to inner ear structure during cochlear implantation: Correlation between insertion force and radio-histological findings in temporal bone specimens. Hear. Res. 2017, 344, 90–97. [Google Scholar] [CrossRef] [Green Version]
- Wilkening, P.; Chien, W.; Gonenc, B.; Niparko, J.; Kang, J.U.; Iordachita, I.; Taylor, R.H. Evaluation of virtual fixtures for robot-assisted cochlear implant insertion. In Proceedings of the 5th IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics, Sao Paulo, Brazil, 12–15 August 2014; pp. 332–338. [Google Scholar]
- Henslee, A.M.; Kaufmann, C.R.; Andrick, M.D.; Reineke, P.T.; Tejani, V.D.; Hansen, M.R. Development and Characterization of an Electrocochleography-Guided Robotics-Assisted Cochlear Implant Array Insertion System. Otolaryngol. Neck Surg. 2022, 167, 334–340. [Google Scholar] [CrossRef]
- Hendricks, C.M.; Cavilla, M.S.; Usevitch, D.E.; Bruns, T.L.; Riojas, K.E.; Leon, L.; Webster, R.J.I.; Warren, F.M.; Abbott, J.J. Magnetic Steering of Robotically Inserted Lateral-wall Cochlear-implant Electrode Arrays Reduces Forces on the Basilar Membrane In Vitro. Otol. Neurotol. 2021, 42, 1022–1030. [Google Scholar] [CrossRef]
- Buchman, C.A.; Dillon, M.T.; King, E.R.; Adunka, M.C.; Adunka, O.F.; Pillsbury, H.C. Influence of Cochlear Implant Insertion Depth on Performance: A Prospective Randomized Trial. Otol. Neurotol. 2014, 35, 1773–1779. [Google Scholar] [CrossRef]
- Rebscher, S.J.; Hetherington, A.; Bonham, B.; Wardrop, P.; Whinney, D.; Leake, P.A. Considerations for the design of future cochlear implant electrode arrays: Electrode array stiffness, size and depth of insertion. J. Rehabil. Res. Dev. 2008, 45, 731–748. [Google Scholar] [CrossRef]
- Elgandy, M.S.; Mobashir, M.K. What physicians and patients should know about different designs of cochlear implant electrodes? Otorhinolaryngol.-Head Neck Surg. 2019, 4, 15. [Google Scholar] [CrossRef]
- Dhanasingh, A.; Jolly, C. An overview of cochlear implant electrode array designs. Hear. Res. 2017, 356, 93–103. [Google Scholar] [CrossRef]
- Leon, L.; Cavilla, M.S.; Doran, M.B.; Warren, F.M.; Abbott, J.J. Scala-Tympani Phantom With Cochleostomy and Round-Window Openings for Cochlear-Implant Insertion Experiments. J. Med. Devices 2014, 8, 041010. [Google Scholar] [CrossRef] [Green Version]
- Dhanasingh, A.; Swords, C.; Bance, M.; Van Rompaey, V.; Van de Heyning, P. Cochlear Size Assessment Predicts Scala Tympani Volume and Electrode Insertion Force- Implications in Robotic Assisted Cochlear Implant Surgery. Front. Surg. 2021, 8, 723897. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.R.; Warren, F.M.; Abbott, J.J. A Scalable Model for Human Scala-Tympani Phantoms. J. Med. Devices 2011, 5, 014501. [Google Scholar] [CrossRef]
- Aebischer, P.; Caversaccio, M.; Wimmer, W. Fabrication of human anatomy-based scala tympani models with a hydrophilic coating for cochlear implant insertion experiments. Hear. Res. 2021, 404, 108205. [Google Scholar] [CrossRef]
- Jacobson, A. Others Gptoolbox: Geometry Processing Toolbox. Available online: http://github.com/alecjacobson/gptoolbox (accessed on 18 October 2022).
- Geom3d. Available online: https://www.mathworks.com/matlabcentral/fileexchange/24484-geom3d (accessed on 23 August 2022).
- Gee, A.H.; Zhao, Y.; Treece, G.M.; Bance, M.L. Practicable assessment of cochlear size and shape from clinical CT images. Sci. Rep. 2021, 11, 3448. [Google Scholar] [CrossRef]
- Yoo, S.K.; Wang, G.; Rubinstein, J.T.; Vannier, M.W. Three-dimensional geometric modeling of the cochlea using helico-spiral approximation. IEEE Trans. Biomed. Eng. 2000, 47, 1392–1402. [Google Scholar] [CrossRef]
- Dang, K. Electrical Conduction Models for Cochlear Implant Stimulation. Ph.D. Thesis, Université Côte d’Azur, Nice, France, 2017. [Google Scholar]
- Cohen, L.T.; Xu, J.; Xu, S.A.; Clark, G.M. Improved and simplified methods for specifying positions of the electrode bands of a cochlear implant array. Am. J. Otol. 1996, 17, 859–865. [Google Scholar]
- Brochier, T.; Schlittenlacher, J.; Roberts, I.; Goehring, T.; Jiang, C.; Vickers, D.; Bance, M. From Microphone to Phoneme: An End-to-End Computational Neural Model for Predicting Speech Perception with Cochlear Implants. IEEE Trans. Biomed. Eng. 2022, 69, 3300–3312. [Google Scholar] [CrossRef]
- Kontorinis, G.; Paasche, G.; Lenarz, T.; Stöver, T. The Effect of Different Lubricants on Cochlear Implant Electrode Insertion Forces. Otol. Neurotol. 2011, 32, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Dohr, D.; Fiedler, N.; Schmidt, W.; Grabow, N.; Mlynski, R.; Schraven, S.P. Frictional Behavior of Cochlear Electrode Array Is Dictated by Insertion Speed and Impacts Insertion Force. Appl. Sci. 2021, 11, 5162. [Google Scholar] [CrossRef]
- Aebischer, P.; Mantokoudis, G.; Weder, S.; Anschuetz, L.; Caversaccio, M.; Wimmer, W. In-Vitro Study of Speed and Alignment Angle in Cochlear Implant Electrode Array Insertions. IEEE Trans. Biomed. Eng. 2022, 69, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Kobler, J.-P.; Dhanasingh, A.; Kiran, R.; Jolly, C.; Ortmaier, T. Cochlear Dummy Electrodes for Insertion Training and Research Purposes: Fabrication, Mechanical Characterization, and Experimental Validation. BioMed Res. Int. 2015, 2015, 574209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, M.; Arai, Y.; Sakuma, N.; Yabuki, K.; Sano, D.; Nishimura, G.; Oridate, N.; Usami, S. Cochlear volume as a predictive factor for residual-hearing preservation after conventional cochlear implantation. Acta Otolaryngol. 2018, 138, 345–350. [Google Scholar] [CrossRef]
- Avci, E.; Nauwelaers, T.; Lenarz, T.; Hamacher, V.; Kral, A. Variations in microanatomy of the human cochlea: Variations in microanatomy of the human cochlea. J. Comp. Neurol. 2014, 522, 3245–3261. [Google Scholar] [CrossRef] [Green Version]
- Pietsch, M.; Aguirre Dávila, L.; Erfurt, P.; Avci, E.; Lenarz, T.; Kral, A. Spiral Form of the Human Cochlea Results from Spatial Constraints. Sci. Rep. 2017, 7, 7500. [Google Scholar] [CrossRef] [Green Version]
- Demarcy, T.; Vandersteen, C.; Guevara, N.; Raffaelli, C.; Gnansia, D.; Ayache, N.; Delingette, H. Automated analysis of human cochlea shape variability from segmented μCT images. Comput. Med. Imaging Graph. 2017, 59, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Rebscher, S.J.; Talbot, N.; Bruszewski, W.; Heilmann, M.; Brasell, J.; Merzenich, M.M. A transparent model of the human scala tympani cavity. J. Neurosci. Methods 1996, 64, 105–114. [Google Scholar] [CrossRef]
- Cornwall, H.L.; Marway, P.S.; Bance, M. A Micro-Computed Tomography Study of Round Window Anatomy and Implications for Atraumatic Cochlear Implant Insertion. Otol. Neurotol. 2021, 42, 327–334. [Google Scholar] [CrossRef]
- Adunka, O.; Kiefer, J.; Unkelbach, M.H.; Lehnert, T.; Gstoettner, W. Development and Evaluation of an Improved Cochlear Implant Electrode Design for Electric Acoustic Stimulation. Laryngoscope 2004, 114, 1237–1241. [Google Scholar] [CrossRef] [PubMed]
- Avci, E.; Nauwelaers, T.; Hamacher, V.; Kral, A. Three-Dimensional Force Profile During Cochlear Implantation Depends on Individual Geometry and Insertion Trauma. Ear Hear. 2017, 38, e168–e179. [Google Scholar] [CrossRef] [PubMed]
- Bruns, T.L.; Riojas, K.E.; Ropella, D.S.; Cavilla, M.S.; Petruska, A.J.; Freeman, M.H.; Labadie, R.F.; Abbott, J.J.; Webster, R.J. Magnetically Steered Robotic Insertion of Cochlear-Implant Electrode Arrays: System Integration and First-In-Cadaver Results. IEEE Robot. Autom. Lett. 2020, 5, 2240–2247. [Google Scholar] [CrossRef] [PubMed]
- Leon, L.; Warren, F.M.; Abbott, J.J. An In-Vitro Insertion-Force Study of Magnetically Guided Lateral-Wall Cochlear-Implant Electrode Arrays. Otol. Neurotol. 2018, 39, e63–e73. [Google Scholar] [CrossRef]
- Radeloff, A.; Unkelbach, M.H.; Mack, M.G.; Settevendemie, C.; Helbig, S.; Mueller, J.; Hagen, R.; Mlynski, R. A coated electrode carrier for cochlear implantation reduces insertion forces: A Coated Electrode Carrier for Cochlear Implantation. Laryngoscope 2009, 119, 959–963. [Google Scholar] [CrossRef]
- Jwair, S.; Prins, A.; Wegner, I.; Stokroos, R.J.; Versnel, H.; Thomeer, H.G.X.M. Scalar Translocation Comparison Between Lateral Wall and Perimodiolar Cochlear Implant Arrays—A Meta-Analysis. Laryngoscope 2021, 131, 1358–1368. [Google Scholar] [CrossRef]
- Schuster, D.; Kratchman, L.B.; Labadie, R.F. Characterization of Intracochlear Rupture Forces in Fresh Human Cadaveric Cochleae. Otol. Neurotol. 2015, 36, 657–661. [Google Scholar] [CrossRef] [Green Version]
- Stuart, I.M. Capstan equation for strings with rigidity. Br. J. Appl. Phys. 1961, 12, 559–562. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IMPACT ON: | ||||
|---|---|---|---|---|
| Height of LW | Trajectory in Vertical Axis | Trajectory in Horizontal Plane | ||
| MANIPULATION OF MODEL: | Volume |  | | |
| Basal planarity and rising spiral |  | | | |
| Curvature | | | | |
| Cross-section area | | | | |
| Impact on Insertion Force with Respect to Angular Insertion Depth | ||
|---|---|---|
| MANIPULATION OF MODEL: | Volume scaling | No statistically significant difference (p > 0.05) |
| Overall vertical trajectory/ rising spiral | No statistically significant difference (p > 0.05) | |
| Basal turn non-planarity | Higher non-planarity may decrease insertion force due to less contact (p > 0.01) | |
| Curvature | No statistically significant difference (p > 0.05) | |
| Cross-section area | No statistically significant difference (p > 0.05) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hrncirik, F.; Roberts, I.V.; Swords, C.; Christopher, P.J.; Chhabu, A.; Gee, A.H.; Bance, M.L. Impact of Scala Tympani Geometry on Insertion Forces during Implantation. Biosensors 2022, 12, 999. https://0-doi-org.brum.beds.ac.uk/10.3390/bios12110999
Hrncirik F, Roberts IV, Swords C, Christopher PJ, Chhabu A, Gee AH, Bance ML. Impact of Scala Tympani Geometry on Insertion Forces during Implantation. Biosensors. 2022; 12(11):999. https://0-doi-org.brum.beds.ac.uk/10.3390/bios12110999
Chicago/Turabian StyleHrncirik, Filip, Iwan V. Roberts, Chloe Swords, Peter J. Christopher, Akil Chhabu, Andrew H. Gee, and Manohar L. Bance. 2022. "Impact of Scala Tympani Geometry on Insertion Forces during Implantation" Biosensors 12, no. 11: 999. https://0-doi-org.brum.beds.ac.uk/10.3390/bios12110999