Surgeon-led 7-VINCut Antibiotic Stewardship Intervention Decreases Duration of Treatment and Carbapenem Use in a General Surgery Service

 , and
, and
Abstract
:1. Introduction
2. Results
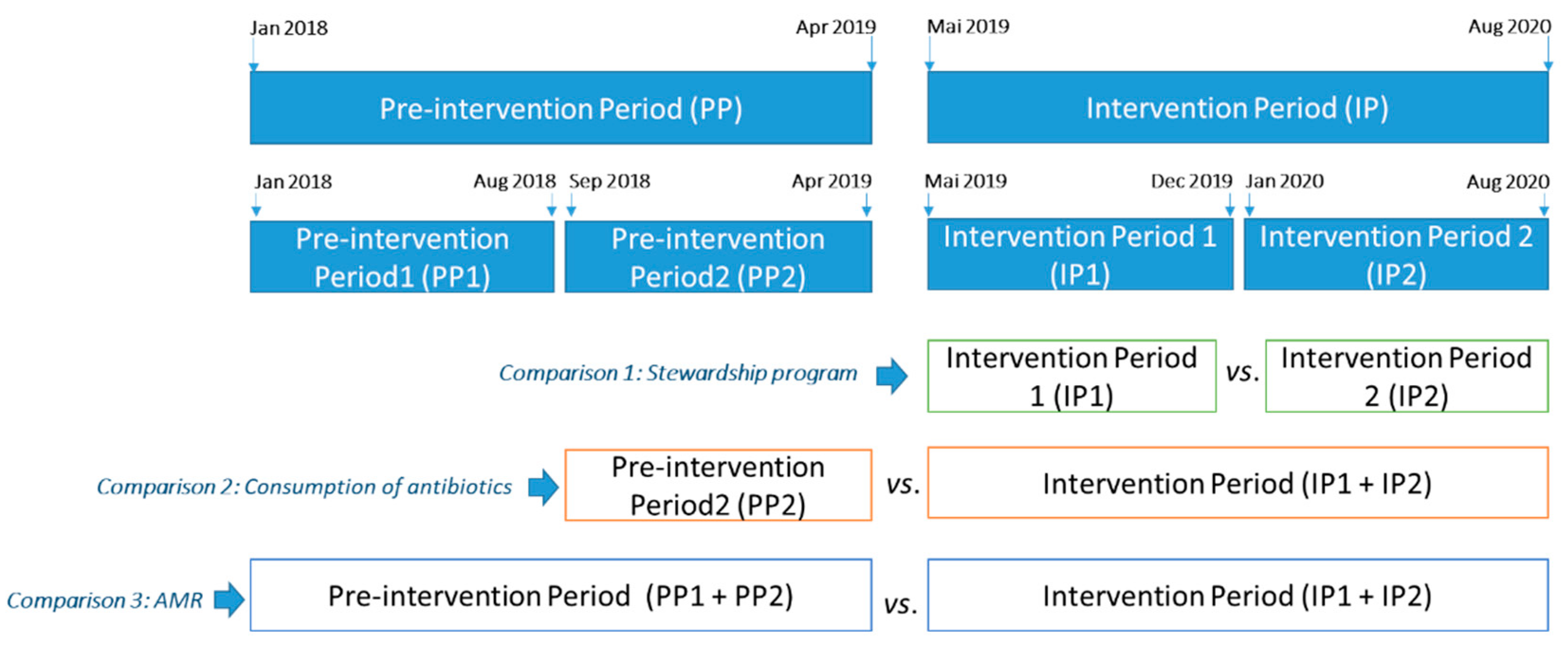
2.1. Stewardship Program
2.2. Consumption of Antibiotics
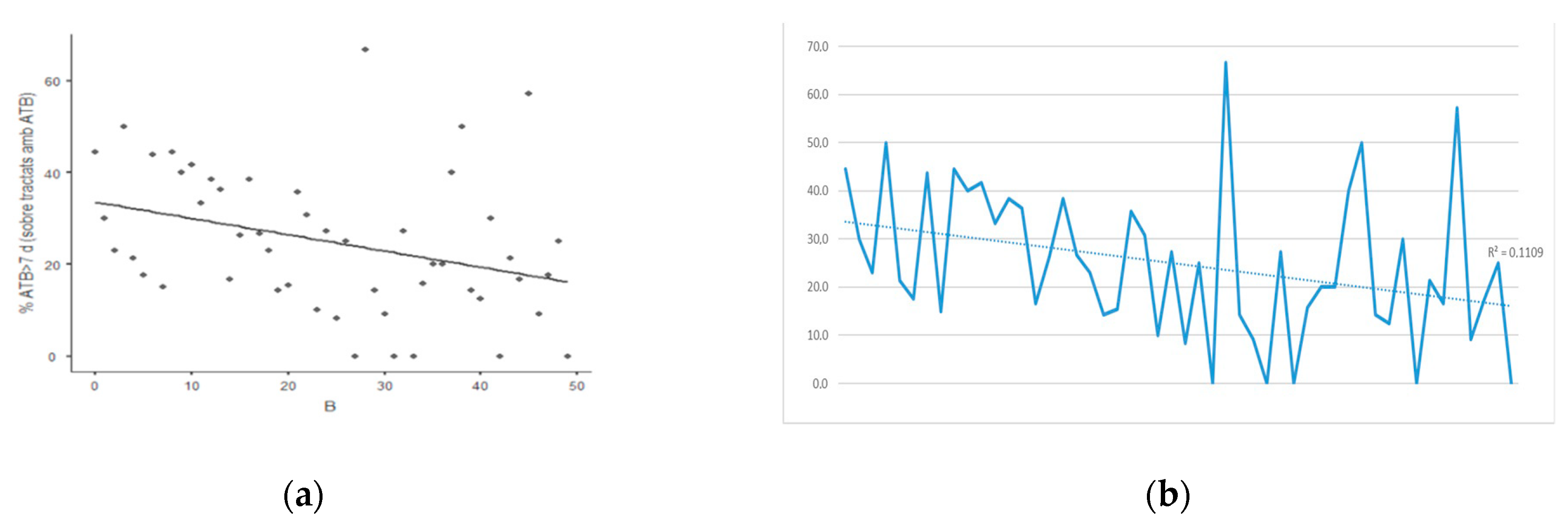
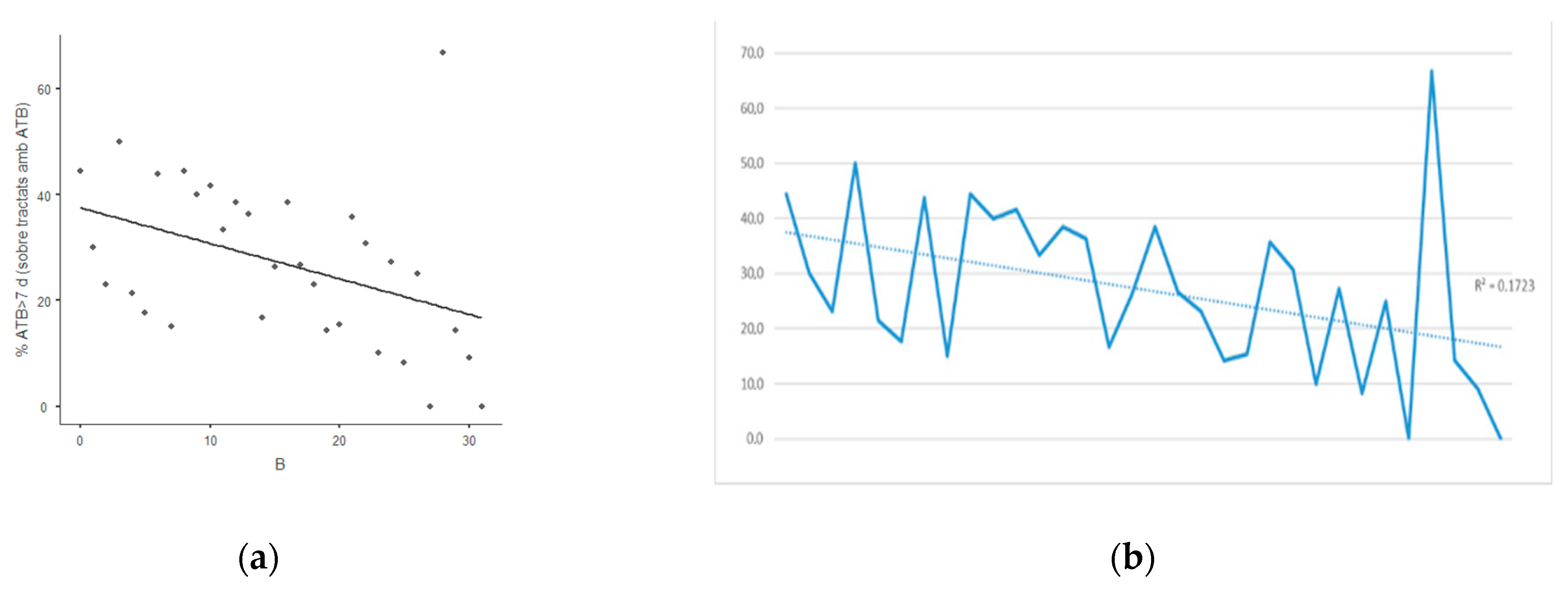
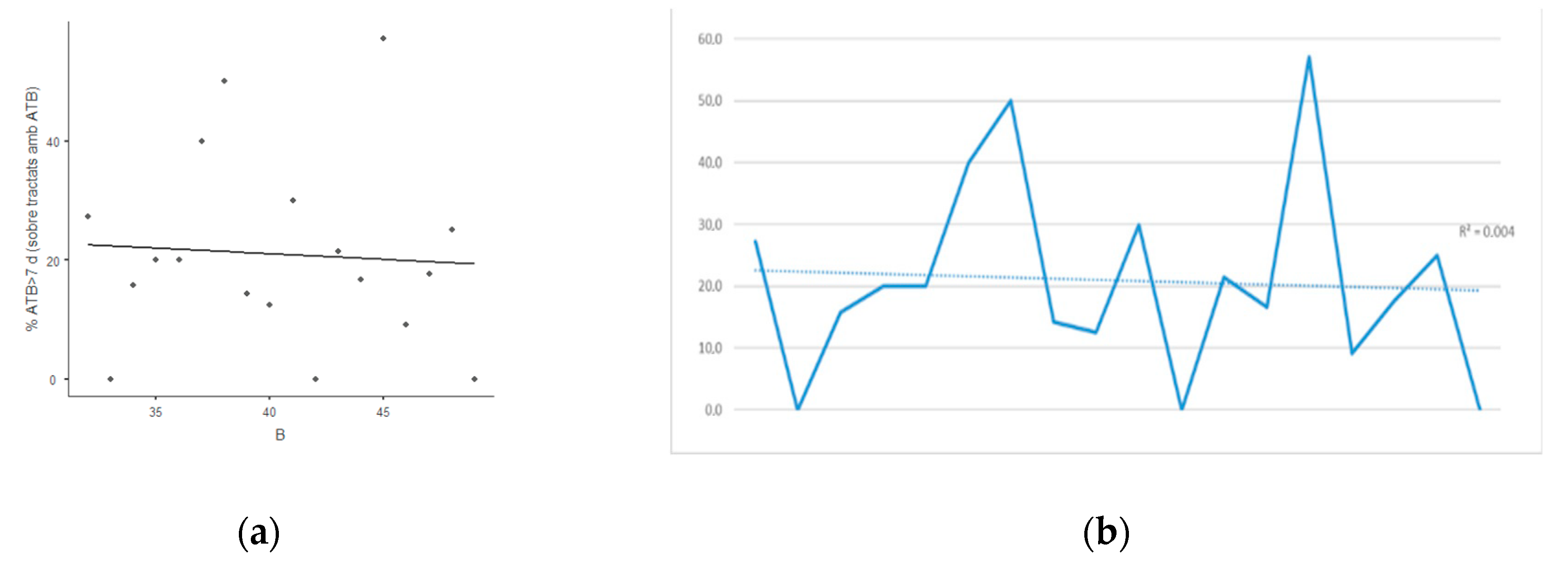
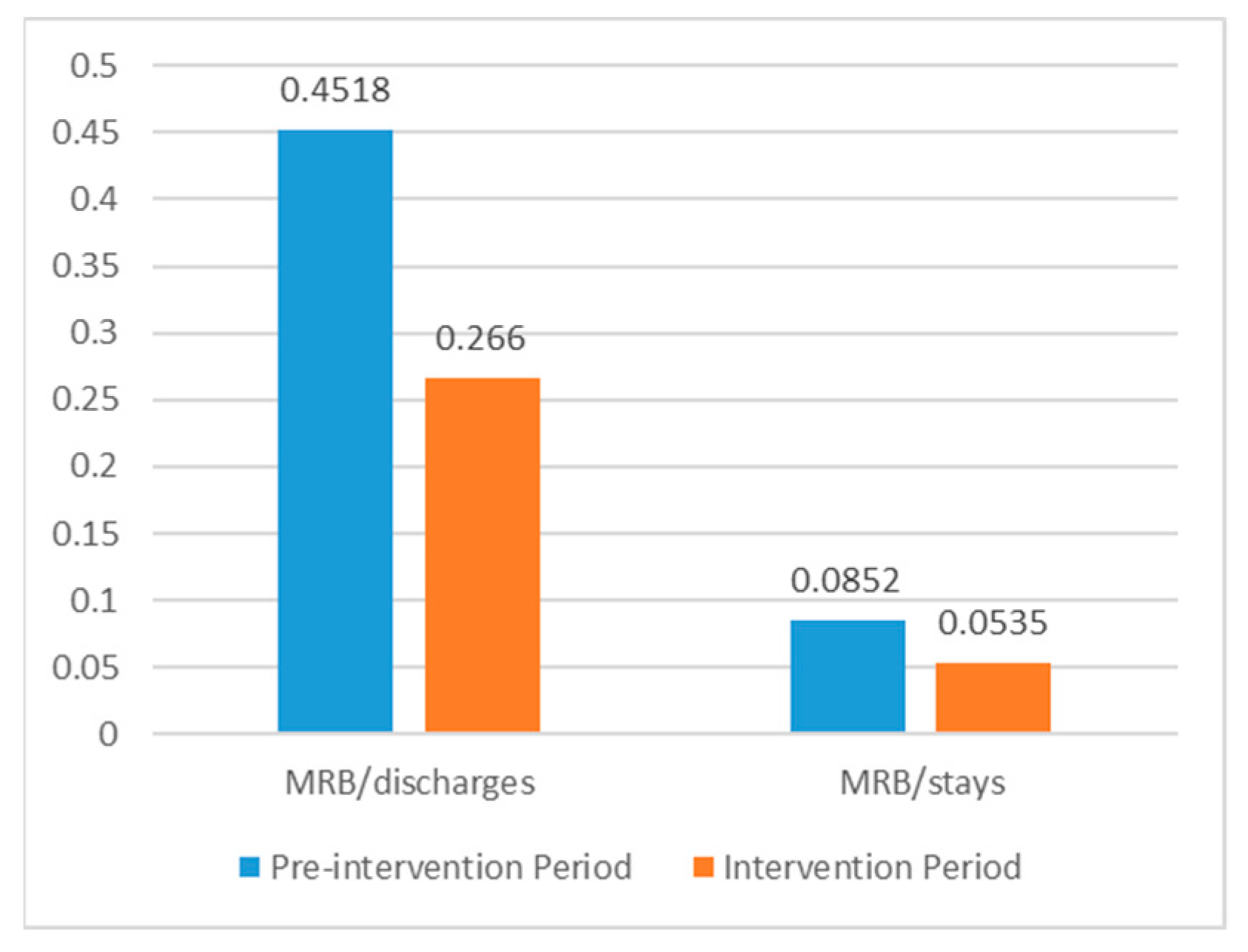
2.3. Evolution of Multiresistant Bacteria in the Department of Surgery
2.4. Internal Evaluation of the 7-VINCut Stewardship Program
3. Discussion
3.1. Stewardship Program
3.2. Consumption of Antibiotics
3.3. Multiresistant Bacteria Isolation
3.4. Acceptance of the Stewardship Program
3.5. Limitations of the Study
4. Materials and Methods
4.1. Stewardship Program
4.2. Consumption of Antibiotics
4.3. Multiresistant Bacteria in the Department of Surgery
4.4. Internal Evaluation of the 7-VINCut Stewardship Program
4.5. Ethics and Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Antibiotic Resistance. July 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 24 August 2020).
- Global Action Plan on Antimicrobial Resistance. Available online: https://www.who.int/antimicrobial-resistance/global-action-plan/en/ (accessed on 24 August 2020).
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensiv. Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Kardos, N. Overuse of Antibiotics and Antibiotic Resistance in Medical Applications Featuring Carbapenemase Resistant Enterobacteriaceae (CRE). SOJ Microbiol. Infect. Dis. 2017, 5, 1–21. [Google Scholar] [CrossRef]
- Fridkin, S.K.; Baggs, J.; Fagan, R.; Magill, S.; Pollack, L.A.; Malpiedi, P.; Slayton, R. Vital Signs: Improving Antibiotic Use among Hospitalized Patients. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 194–200. [Google Scholar] [PubMed]
- Bugnon-Reber, A.; De Torrenté, A.; Troillet, N.; Genné, D. Antibiotic misuse in medium-size Swiss hospitals. Swiss Med. Wkly. 2004, 134, 481–485. [Google Scholar]
- Dellit, T.H.; Owens, R.C.; McGowan, J.E., Jr.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America Guidelines for Developing an Institutional Program to Enhance Antimicrobial Stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef]
- Core Elements of Hospital Antibiotic Stewardship Programs. Available online: https://www.cdc.gov/antibiotic-use/core-elements/hospital.html (accessed on 24 August 2020).
- Vázquez, A.M.; Balibrea, J.M.; Ramia, J.M. Antimicrobial stewardship programs and surgery: What is our role? Cir. Esp. 2019, 97, 187–189. [Google Scholar] [CrossRef]
- Sartelli, M.; Duane, T.M.; Catena, F.; Tessier, J.M.; Coccolini, F.; Kao, L.S.; De Simone, B.; Labricciosa, F.M.; May, A.K.; Ansaloni, L.; et al. Antimicrobial Stewardship: A Call to Action for Surgeons. Surg. Infect. 2016, 17, 625–631. [Google Scholar] [CrossRef] [Green Version]
- Grau, S.; Fondevilla, E.; Echeverría-Esnal, D.; Alcorta, A.; Limon, E.; Gudiol, F. Widespread increase of empirical carbapenem use in acute care hospitals in Catalonia, Spain. Enferm. Infecc. Microbiol. Clin. 2019, 37, 36–40. [Google Scholar] [CrossRef]
- Gorecki, P.; Schein, M.; Rucinski, J.C.; Wise, L. Antibiotic Administration in Patients Undergoing Common Surgical Procedures in a Community Teaching Hospital: The Chaos Continues. World J. Surg. 1999, 23, 429–433. [Google Scholar] [CrossRef]
- Gorecki, P.J.; Schein, M.; Mehta, V.; Wise, L. Surgeons and Infectious Disease Specialists: Different Attitudes towards Antibiotic Treatment and Prophylaxis in Common Abdominal Surgical Infections. Surg. Infect. 2000, 1, 115–126. [Google Scholar] [CrossRef]
- Smith, S.E.; Rumbaugh, K.A.; May, A.K. Evaluation of a Short Course of Antimicrobial Therapy for Complicated Intra-Abdominal Infections in Critically Ill Surgical Patients. Surg. Infect. 2017, 18, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Hassinger, T.E.; Guidry, C.A.; Rotstein, O.D.; Duane, T.M.; Evans, H.L.; Cook, C.H.; O’Neill, P.J.; Mazuski, J.E.; Askari, R.; Napolitano, L.M.; et al. Longer-Duration Antimicrobial Therapy Does Not Prevent Treatment Failure in High-Risk Patients with Complicated Intra-Abdominal Infections. Surg. Infect. 2017, 18, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Cole, K.; Phlamon, M.; Petite, S.E. Comparison of Short-Course and Prolonged Antimicrobial Therapy in the Management of Intra-Abdominal Infections. Surg. Infect. 2019, 20, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Rattan, R.; Allen, C.J.; Sawyer, R.G.; Mazuski, J.; Duane, T.M.; Askari, R.; Banton, K.L.; Claridge, J.A.; Coimbra, R.; Cuschieri, J.; et al. Patients with Risk Factors for Complications Do Not Require Longer Antimicrobial Therapy for Complicated Intra-Abdominal Infection. Am. Surg. 2016, 82, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Rattan, R.; Allen, C.J.; Sawyer, R.G.; Askari, R.; Banton, K.L.; Claridge, J.A.; Cocanour, C.S.; Coimbra, R.; Cook, C.H.; Cuschieri, J.; et al. Patients with Complicated Intra-Abdominal Infection Presenting with Sepsis Do Not Require Longer Duration of Antimicrobial Therapy. J. Am. Coll. Surg. 2016, 222, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Taylor, E.; Dev, V.; Shah, D.; Festekjian, J.; Gaw, F. Complicated appendicitis: Is there a minimum intravenous antibiotic requirement? A prospective randomized trial. Am. Surg. 2000, 66, 887–890. [Google Scholar] [PubMed]
- Maseda, E.; Suarez-De-La-Rica, A.; Anillo, V.; Tamayo, E.; García-Bernedo, C.A.; Ramasco, F.; Villagran, M.-J.; Maggi, G.; Gimenez, M.-J.; Aguilar, L.; et al. Procalcitonin-guided therapy may reduce length of antibiotic treatment in intensive care unit patients with secondary peritonitis: A multicenter retrospective study. J. Crit. Care 2015, 30, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Montravers, P.; Tubach, F.; Lescot, T.; Veber, B.; Esposito-Farèse, M.; Seguin, P.; Paugam, C.; Lepape, A.; Meistelman, C.; Cousson, J.; et al. Short-course antibiotic therapy for critically ill patients treated for postoperative intra-abdominal infection: The DURAPOP randomised clinical trial. Intensiv. Care Med. 2018, 44, 300–310. [Google Scholar] [CrossRef]
- Sawyer, R.G.; Claridge, J.A.; Nathens, A.B.; Rotstein, O.D.; Duane, T.M.; Evans, H.L.; Cook, C.H.; O’Neill, P.J.; Mazuski, J.E.; Askari, R.; et al. Trial of Short-Course Antimicrobial Therapy for Intraabdominal Infection. N. Engl. J. Med. 2015, 372, 1996–2005. [Google Scholar] [CrossRef] [Green Version]
- Guidry, C.A.; Sawyer, R.G. Short-Course Antimicrobial Therapy for Intraabdominal Infection. N. Engl. J. Med. 2015, 373, 1578. [Google Scholar] [CrossRef]
- Riccio, L.M.; Popovsky, K.A.; Hranjec, T.; Politano, A.D.; Rosenberger, L.H.; Tura, K.C.; Sawyer, R.G. Association of Excessive Duration of Antibiotic Therapy for Intra-Abdominal Infection with Subsequent Extra-Abdominal Infection and Death: A Study of 2552 Consecutive Infections. Surg. Infect. 2014, 15, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guirao, X.; Arias, J.; Badía, J.M.; García-Rodríguez, J.A.; Mensa, J.; Alvarez-Lerma, F.; Borges, M.; Barberán, J.; Maseda, E.; Salavert, M.; et al. Recomendaciones en el tratamiento antibiótico empírico de la infección intraabdominal [Recommendations in the empiric anti-infective agents of intra-abdominal infection]. Cir. Esp. 2010, 87, 63–81. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Solomkin, J.S.; Mazuski, J.; Bradley, J.S.; Rodvold, K.A.; Goldstein, E.J.C.; Baron, E.J.; O’Neill, P.J.; Chow, A.W.; Dellinger, E.P.; Eachempati, S.R.; et al. Diagnosis and Management of Complicated Intra-abdominal Infection in Adults and Children: Guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 133–164, Erratum in 2010, 50, 1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazuski, J.E.; Tessier, J.M.; May, A.K.; Sawyer, R.G.; Nadler, E.P.; Rosengart, M.R.; Chang, P.K.; O’Neill, P.J.; Mollen, K.P.; Huston, J.M.; et al. The Surgical Infection Society Revised Guidelines on the Management of Intra-Abdominal Infection. Surg. Infect. 2017, 18, 1–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C.; ESGAP (ESCMID Study Group for Antimicrobial stewardshiP). What is antimicrobial stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulscher, M.E.J.L.; Prins, J.M. Antibiotic stewardship: Does it work in hospital practice? A review of the evidence base. Clin. Microbiol. Infect. 2017, 23, 799–805. [Google Scholar] [CrossRef] [Green Version]
- Wagner, B.; Filice, G.A.; Drekonja, D.; Greer, N.; Macdonald, R.; Rutks, I.; Butler, M.; Wilt, T.J. Antimicrobial Stewardship Programs in Inpatient Hospital Settings: A Systematic Review. Infect. Control. Hosp. Epidemiol. 2014, 35, 1209–1228. [Google Scholar] [CrossRef]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- Plan Nacional Frente a la Resistencia a Antibióticos. Available online: http://www.resistenciaantibioticos.es/es/system/files/field/files/prorgramas_de_optimizacion_de_uso_de_antibioticos_proa.pdf?file=1&type=node&id=363&force=0 (accessed on 24 August 2020).
- Tarchini, G.; Liau, K.H.; Solomkin, J.S. Antimicrobial Stewardship in Surgery: Challenges and Opportunities. Clin. Infect. Dis. 2017, 64 (Suppl. 2), S112–S114. [Google Scholar] [CrossRef]
- Saar, S.; Mihnovitš, V.; Lustenberger, T.; Rauk, M.; Noor, E.-H.; Lipping, E.; Isand, K.-G.; Lepp, J.; Lomp, A.; Lepner, U.; et al. Twenty-four hour versus extended antibiotic administration after surgery in complicated appendicitis: A randomized controlled trial. J. Trauma Acute Care Surg. 2019, 86, 36–42. [Google Scholar] [CrossRef]
- Boyle, L.I.; Boyle, A.; Jay, S.; Marnewick, J. COVID-19 lockdown impact on common general surgical acute presentations to a regional centre in New Zealand. N. Z. Med. J. 2020, 133, 96–105. [Google Scholar] [PubMed]
- Del Pozo, E.P.; Aparicio-Sánchez, D.; Ramírez, F.H.; Ciuró, F.P.; Muñoz-Cruzado, V.D.; Arteaga, A.S.; Barbeito, S.D.; Ruiz, F.J.P. A prospective cohort study of the impact of covid19 world pandemic on the management of emergency surgical pathology. Br. J. Surg. 2020, 13. [Google Scholar] [CrossRef] [PubMed]
- Gerall, C.D.; DeFazio, J.R.; Kahan, A.M.; Fan, W.; Fallon, E.M.; Middlesworth, W.; Stylianos, S.; Zitsman, J.L.; Kadenhe-Chiweshe, A.V.; Spigland, N.A.; et al. Delayed presentation and sub-optimal outcomes of pediatric patients with acute appendicitis during the COVID-19 pandemic. J. Pediatr. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.C.; Tomita, S.S.; Ginsburg, H.B.; Gordon, A.; Walker, D.; Kuenzler, K.A. Increase in Pediatric Perforated Appendicitis in the New York City Metropolitan Region at the Epicenter of the COVID-19 Outbreak. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- Spanish Association of Surgeons. General Recommendations for the Performance of Surgical Procedures in the Context of the COVID-19 Pandemic. Available online: https://www.aecirujanos.es/Documentos-de-posicionamiento-y-recomendaciones-de-la-AEC-en-relacion-con-la-cirugia-y-COVID19_es_116_508_0_345.html (accessed on 11 November 2020).
- Balibrea, J.M.; Badia, J.M.; Pérez, I.R.; Antona, E.M.; Peña, E.Á.; Botella, S.G.; Gallego, M.Á.; Pérez, E.M.; Cortijo, S.M.; Miguelañez, I.P.; et al. Surgical Management of Patients With COVID-19 Infection. Recommendations of the Spanish Association of Surgeons. Cir. Esp. 2020, 98, 251–259, (In English, Spanish). [Google Scholar] [CrossRef]
- Wee, L.E.; Chung, S.J.; Tang, S.L.S.; Liew, Y.X.; Tan, L.Y.; Cherng, P.Z.B.; Kwa, L.H.A.; Chlebicki, M.P. Who listens and who doesn’t? Factors associated with adherence to antibiotic stewardship intervention in a Singaporean tertiary hospital. J. Glob. Antimicrob. Resist. 2020, 22, 391–397. [Google Scholar] [CrossRef]
- Corcione, S.; Lupia, T.; Maraolo, A.E.; Pinna, S.M.; Gentile, I.; De Rosa, F.G. Carbapenem-sparing strategy: Carbapenemase, treatment, and stewardship. Curr. Opin. Infect. Dis. 2019, 32, 663–673. [Google Scholar] [CrossRef]
- Oteo, J.; Calbo, E.; Rodríguez-Baño, J.; Oliver, A.; Hornero, A.; Ruiz-Garbajosa, P.; Horcajada, J.P.; Del Pozo, J.L.; Riera, M.; Sierra, R.; et al. The threat of the carbapenemase-producing enterobacteriaceae in Spain: Positioning report of the SEIMC study groups, GEIH and GEMARA. Enferm. Infecc. Microbiol. Clin. 2014, 32, 666–670. [Google Scholar] [CrossRef]
- Gelband, H.; Miller-Petrie, M.; Pant, S.; Gandra, S.; Levinson, J.; Barter, D. The State of the World’s Antibiotics. Center for Disease Dynamics & Policy 2015b (CCDDEP). Available online: https://cddep.org/sites/default/files/swa_2015_final.pdf (accessed on 7 September 2020).
- Langford, B.J.; Nisenbaum, R.; Brown, K.A.; Chan, A.; Downing, M. Antibiotics: Easier to start than to stop? Predictors of antimicrobial stewardship recommendation acceptance. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- Sartelli, M.; Weber, D.G.; Ruppé, E.; Bassetti, M.; Wright, B.J.; Ansaloni, L.; Catena, F.; Coccolini, F.; Abu-Zidan, F.M.; Coimbra, R.; et al. Antimicrobials: A global alliance for optimizing their rational use in intra-abdominal infections (AGORA). World J. Emerg. Surg. 2016, 11, 1–32, Erratum in 2017, 12, 35. [Google Scholar] [CrossRef]
- Çakmakçi, M. Antibiotic stewardship programmes and the surgeon’s role. J. Hosp. Infect. 2015, 89, 264–266. [Google Scholar] [CrossRef] [PubMed]
- Labricciosa, F.M.; Sartelli, M.; Correia, S.; Abbo, L.M.; Severo, M.; Ansaloni, L.; Coccolini, F.; Alves, C.; Melo, R.B.; Baiocchi, G.L.; et al. Emergency surgeons’ perceptions and attitudes towards antibiotic prescribing and resistance: A worldwide cross-sectional survey. World J. Emerg. Surg. 2018, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- May, C. Towards a general theory of implementation. Implement. Sci. 2013, 8, 18–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elwyn, G.; Legare, F.; van der Weijden, T.; Edwards, A.; May, C. Arduous implementation: Does the normalisation process model explain why it is so difficult to embed decision support technologies in routine clinical practice. Implement. Sci. 2008, 3, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimshaw, J.M.; Shirran, L.; Thomas, R.; Mowatt, G.; Fraser, C.; Bero, L.; Grilli, R.; Harvey, E.; Oxman, A.; O’Brien, M. Changing provider behavior: An overview of systematic reviews of interventions. Med. Care 2001, 39 (Suppl. 2), II-2-45. [Google Scholar] [CrossRef]
- Grimshaw, J.M.; Eccles, M.P.; Walker, A.E.; Thomas, R.E. Changing physiciansʼ behavior: What works and thoughts on getting more things to work. J. Contin. Educ. Health Prof. 2002, 22, 237–243. [Google Scholar] [CrossRef] [PubMed]
- DDD Definition and General Considerations. Available online: https://www.whocc.no/ddd/definition_and_general_considera/ (accessed on 7 September 2020).
- Grau, S.; Bou, G.; Fondevilla, E.; Nicolás, J.; Rodríguez-Maresca, M.; Martínez-Martínez, L. How to measure and monitor antimicrobial consumption and resistance. Enferm. Infecc. Microbiol. Clin. 2013, 31 (Suppl. 4), 16–24. [Google Scholar] [CrossRef]
- Collado, R.; Losa, J.E.; Álvaro, E.A.; Toro, P.; Moreno, L.; Pérez, M. Evaluación del consumo de antimicrobianos mediante DDD/100 estancias versus DDD/100 altas en la implantación de un Programa de Optimización del Uso de Antimicrobianos [Measurement of antimicrobial consumption using DDD per 100 bed-days versus DDD per 100 discharges after the implementation of an antimicrobial stewardship program]. Rev. Esp. Quimioter. 2015, 28, 317–321. [Google Scholar]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Recommendation | Frequency |
|---|---|
| Withdraw | 66 (53.6%) |
| Maintain | 41 (33.3%) |
| De-escalate | 8 (6.5%) |
| Broaden | 5 (4.1%) |
| Change route | 2 (1.6%) |
| Optimize dose | 1 (0.8%) |
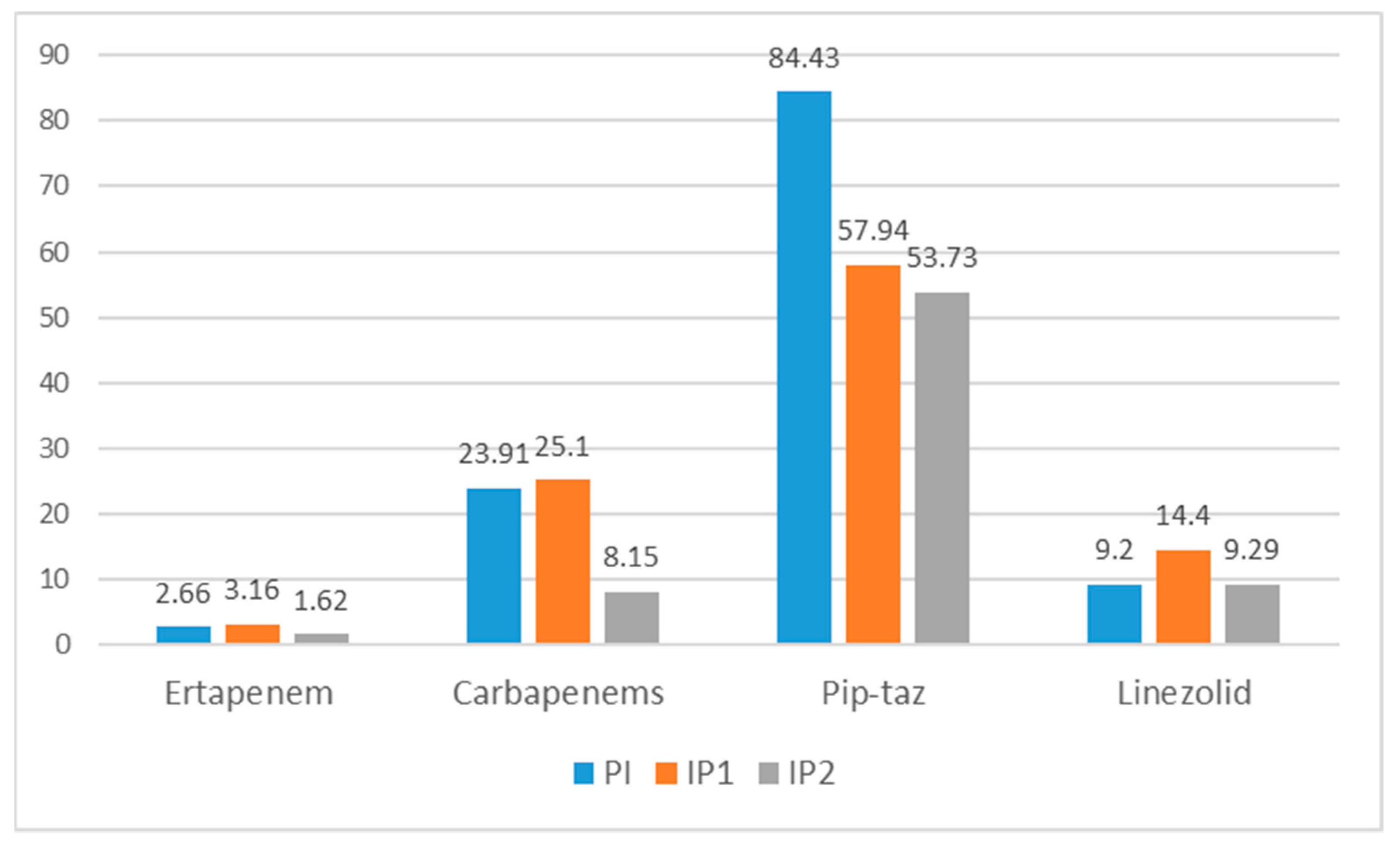
| Antibiotics | PI | IP1 | Variation (PI-IP1) | IP2 | Variation (IP1-IP2) |
|---|---|---|---|---|---|
| Ertapenem | 2.66 | 3.16 | ↑ 18% | 1.62 | ↓ 48% |
| Second-line carbapenems | 23.91 | 25.10 | ↑ 4% | 8.16 | ↓ 67% |
| Piperacillin-tazobactam | 84.43 | 57.94 | ↓ 31% | 53.73 | ↓ 7% |
| Linezolid | 9.20 | 14.40 | ↑ 56% | 9.29 | ↓ 35% |
| Antibiotics | PI | IP1 | Variation (PI-IP1) | IP2 | Variation (IP1-IP2) |
|---|---|---|---|---|---|
| Ertapenem | 0.48 | 0.58 | ↑ 20% | 0.37 | ↓ 36% |
| Second-line carbapenems | 4.34 | 4.57 | ↑ 5% | 1.87 | ↓ 59% |
| Piperacillin-tazobactam | 15.33 | 10.54 | ↓ 30% | 12.38 | ↑ 17% |
| Linezolid | 1.67 | 2.62 | ↑ 56% | 2.14 | ↓ 18% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badia, J.M.; Batlle, M.; Juvany, M.; Ruiz-de León, P.; Sagalés, M.; Pulido, M.A.; Molist, G.; Cuquet, J. Surgeon-led 7-VINCut Antibiotic Stewardship Intervention Decreases Duration of Treatment and Carbapenem Use in a General Surgery Service. Antibiotics 2021, 10, 11. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010011
Badia JM, Batlle M, Juvany M, Ruiz-de León P, Sagalés M, Pulido MA, Molist G, Cuquet J. Surgeon-led 7-VINCut Antibiotic Stewardship Intervention Decreases Duration of Treatment and Carbapenem Use in a General Surgery Service. Antibiotics. 2021; 10(1):11. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010011
Chicago/Turabian StyleBadia, Josep M., Maria Batlle, Montserrat Juvany, Patricia Ruiz-de León, Maria Sagalés, M Angeles Pulido, Gemma Molist, and Jordi Cuquet. 2021. "Surgeon-led 7-VINCut Antibiotic Stewardship Intervention Decreases Duration of Treatment and Carbapenem Use in a General Surgery Service" Antibiotics 10, no. 1: 11. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10010011