
Cerebrospinal Fluid Concentrations of Meropenem and Vancomycin in Ventriculitis Patients Obtained by TDM-Guided Continuous Infusion

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
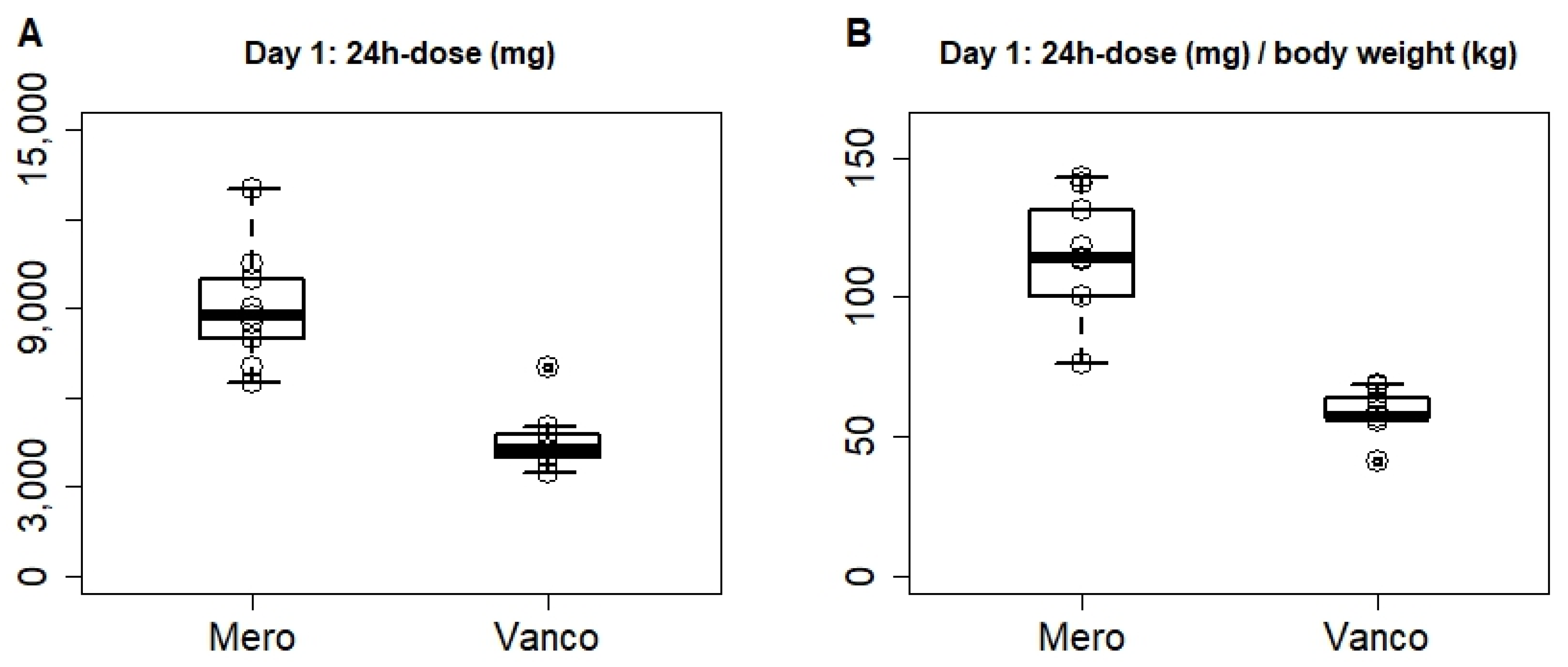
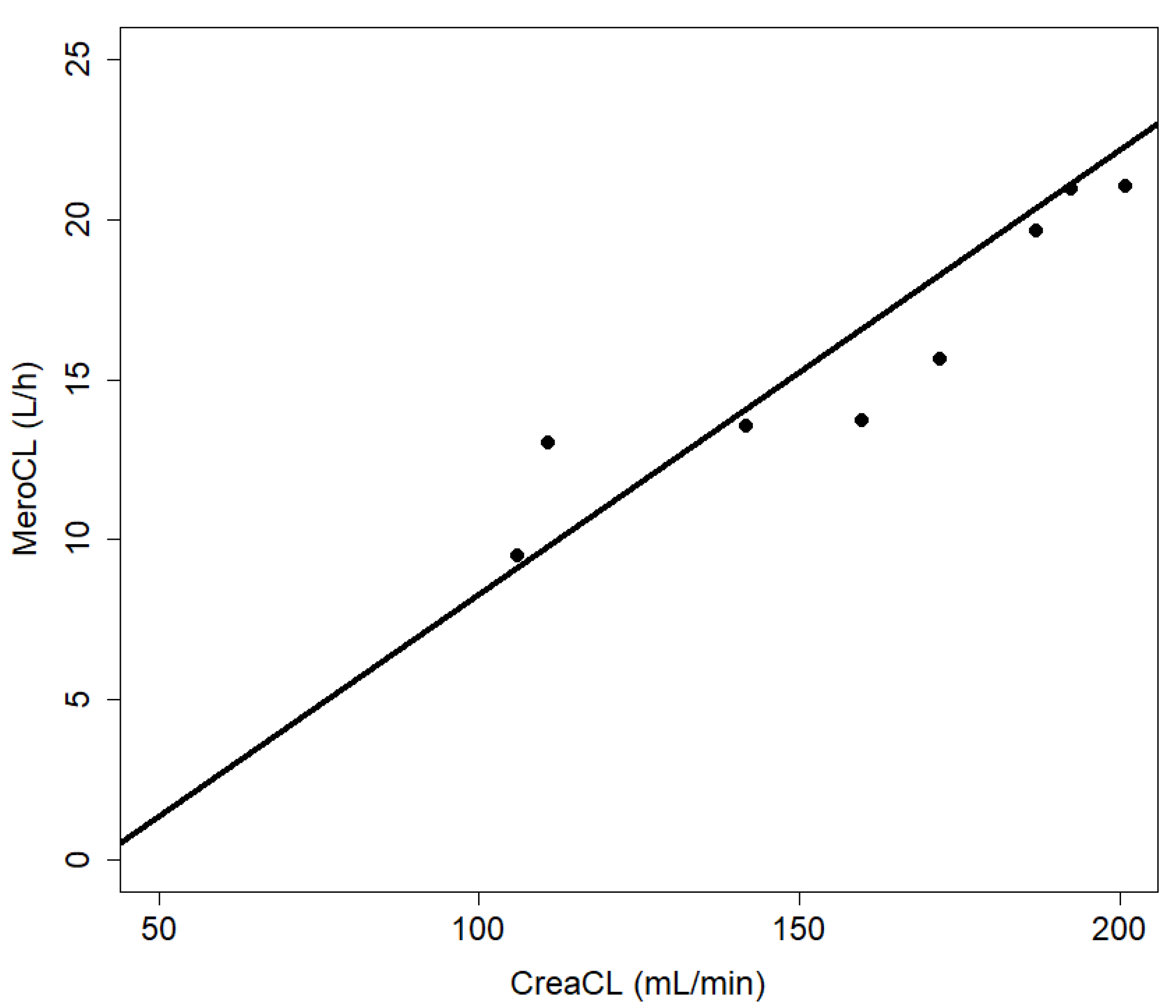
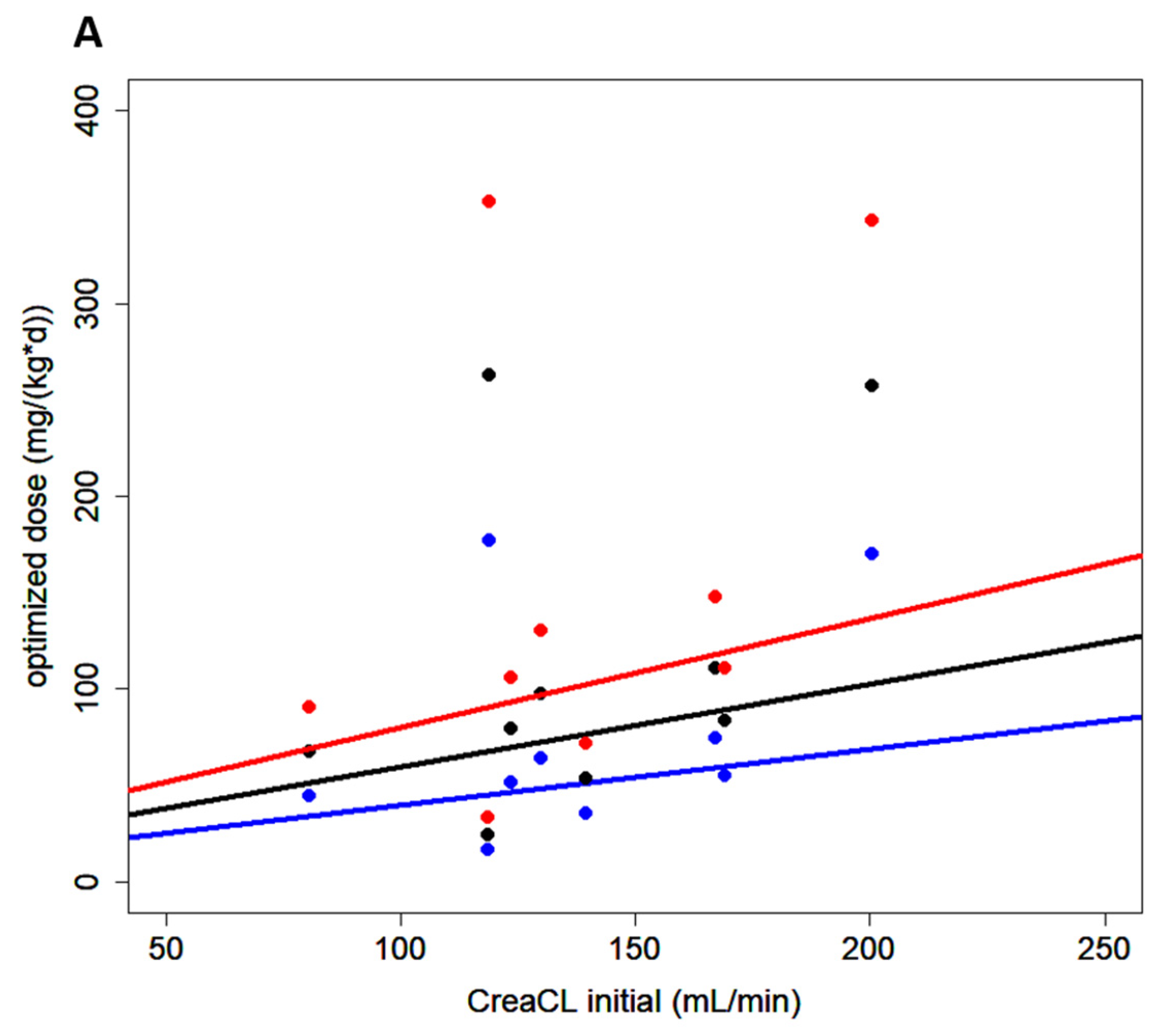
2.1. High Doses Required Due to Low Serum Creatinine Values in Neurosurgical Patients
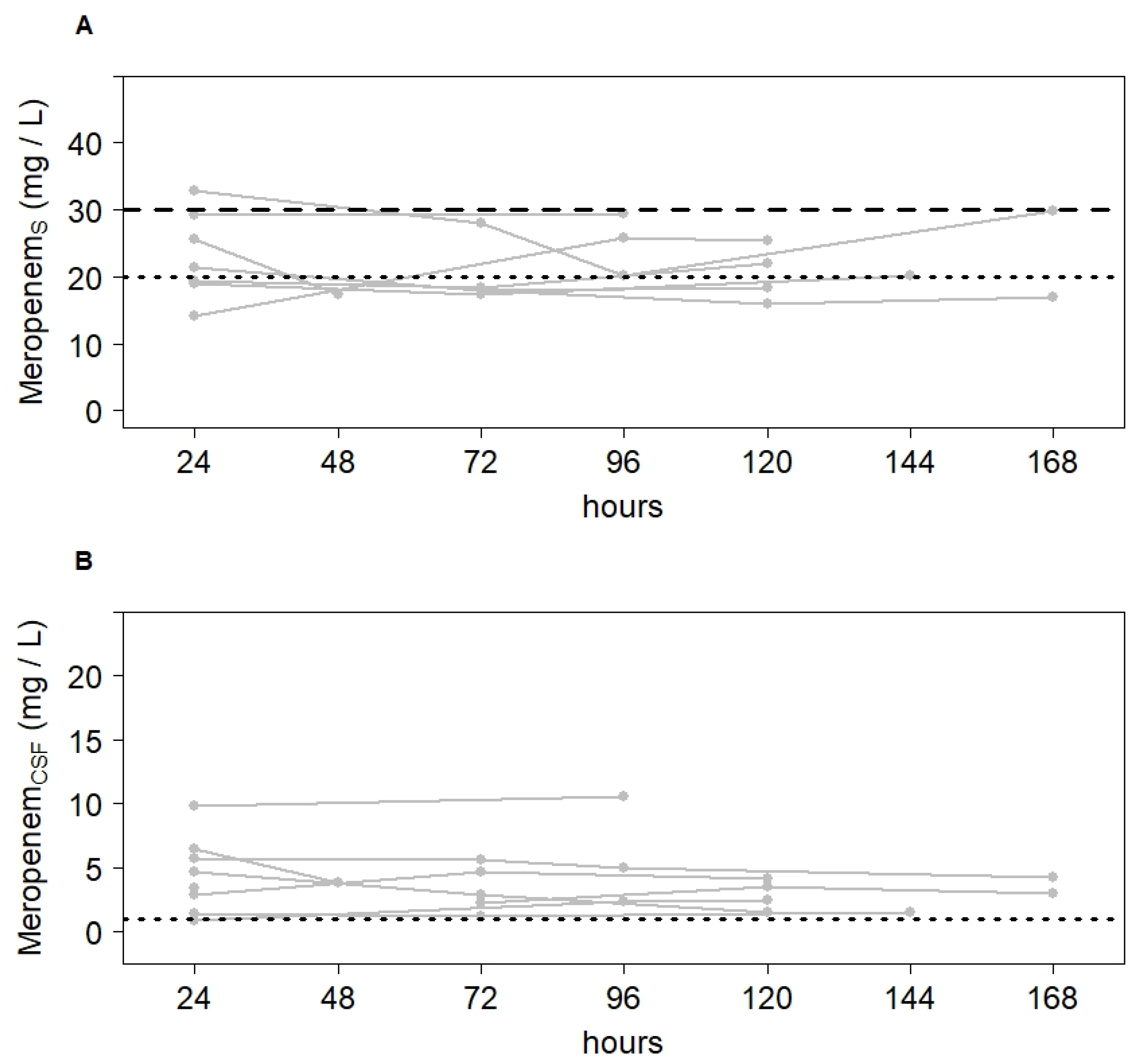
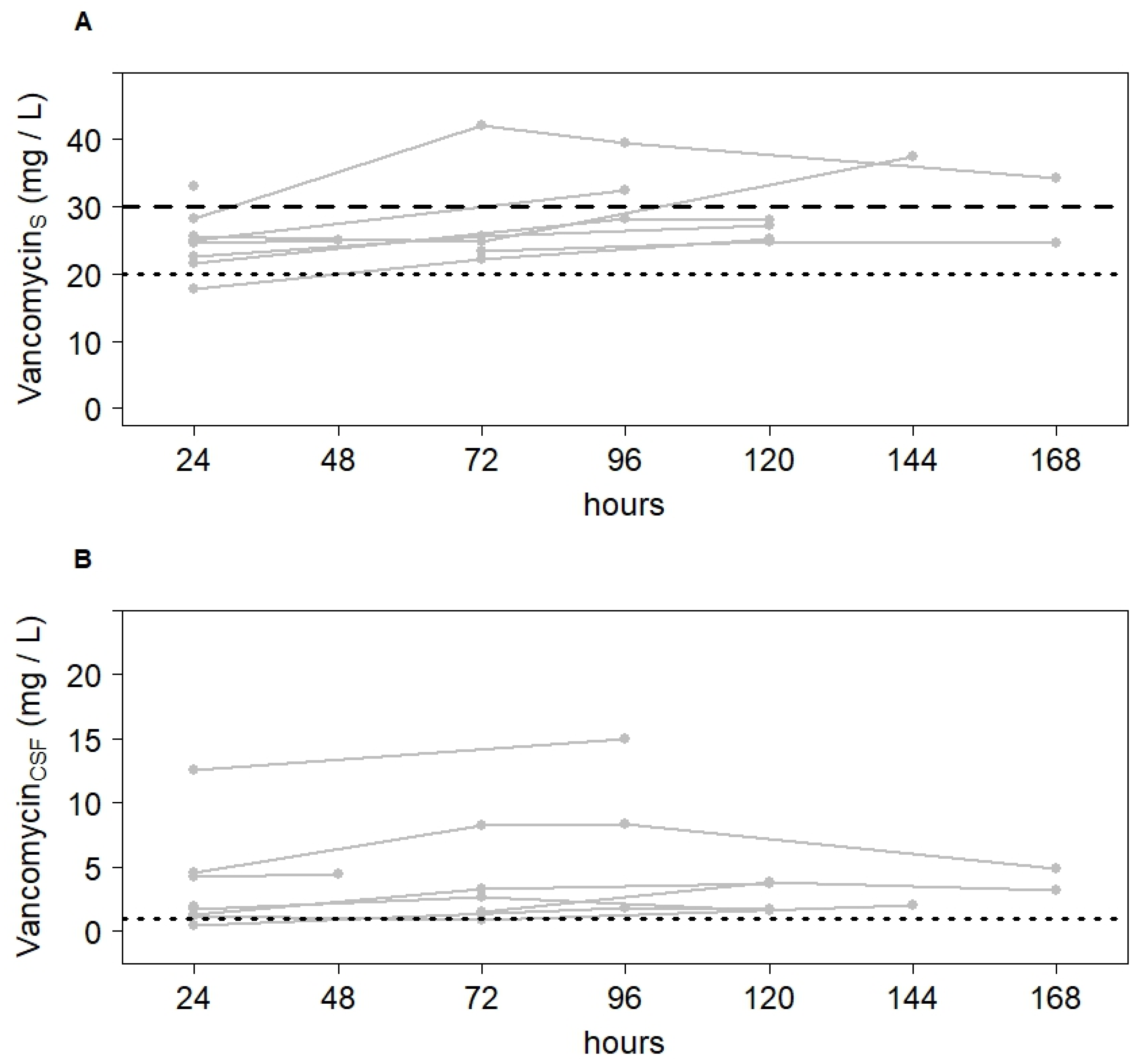
2.2. Meropenem and Vancomycin Concentrations in CSF within Target Range after Dose Adjustment
2.3. Initial Dosing Recommendation Based on Nomograms
3. Materials and Methods
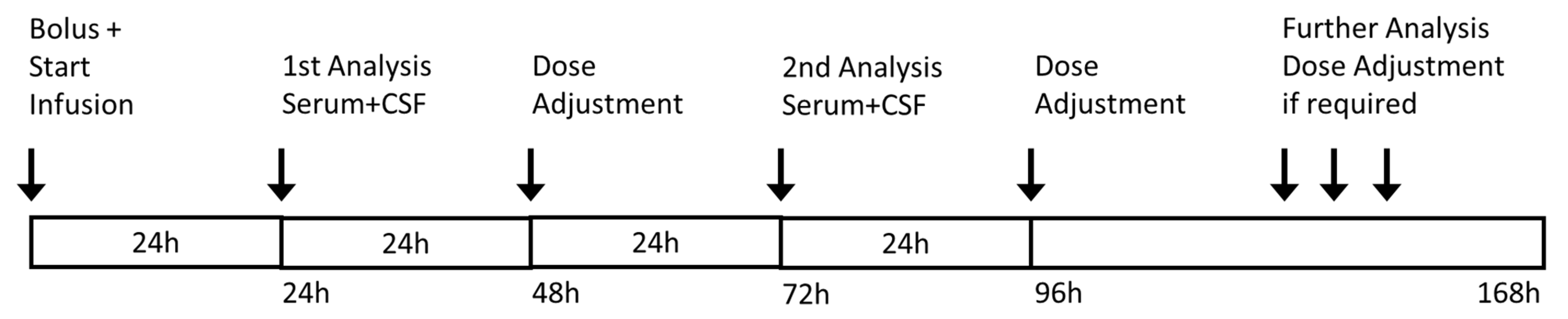
3.1. Study Design
3.2. Bioanalytical Methodology
3.3. Statistics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumta, N.; Roberts, J.A.; Lipman, J.; Cotta, M.O. Antibiotic Distribution into Cerebrospinal Fluid: Can Dosing Safely Account for Drug and Disease Factors in the Treatment of Ventriculostomy-Associated Infections? Clin. Pharmacokinet. 2018, 57, 439–454. [Google Scholar] [CrossRef]
- Widén, J.; Eriksson, B.-M.; Ronne-Engström, E.; Enblad, P.; Westman, G. Ventriculostomy-related infections in subarachnoid hemorrhage patients—A retrospective study of incidence, etiology, and antimicrobial therapy. Acta Neurochir. 2017, 159, 317–323. [Google Scholar] [CrossRef] [Green Version]
- Tunkel, A.R.; Hartman, B.J.; Kaplan, S.L.; Kaufman, B.A.; Roos, K.L.; Scheld, W.M.; Whitley, R.J. Practice Guidelines for the Management of Bacterial Meningitis. Clin. Infect. Dis. 2004, 39, 1267–1284. [Google Scholar] [CrossRef]
- Kumta, N.; Roberts, J.A.; Lipman, J.; Wong, W.T.; Joynt, G.M.; Cotta, M.O. A Systematic Review of Studies Reporting Antibiotic Pharmacokinetic Data in the Cerebrospinal Fluid of Critically Ill Patients with Uninflamed Meninges. Antimicrob. Agents Chemother. 2020, 65, e01998-20. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.; Boots, R.; Senthuran, S.; Stuart, J.; Deans, R.; Lassig-Smith, M.; Lipman, J. Augmented Creatinine Clearance in Traumatic Brain Injury. Anesth. Analg. 2010, 111, 1505–1510. [Google Scholar] [CrossRef]
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Kaukonen, K.-M.; Koulenti, D.; Martin, C.; Montravers, P.; et al. DALI: Defining Antibiotic Levels in Intensive Care Unit Patients: Are Current β-Lactam Antibiotic Doses Sufficient for Critically Ill Patients? Clin. Infect. Dis. 2014, 58, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Minichmayr, I.K.; Roberts, J.A.; Frey, O.R.; Roehr, A.C.; Kloft, C.; Brinkmann, A. Development of a dosing nomogram for continuous-infusion meropenem in critically ill patients based on a validated population pharmacokinetic model. J. Antimicrob. Chemother. 2018, 73, 1330–1339. [Google Scholar] [CrossRef] [PubMed]
- Mader, M.M.-D.; Czorlich, P.; König, C.; Fuhrmann, V.; Kluge, S.; Westphal, M.; Grensemann, J. Intrathecal penetration of meropenem and vancomycin administered by continuous infusion in patients suffering from ventriculitis—A retrospective analysis. Acta Neurochir. 2018, 160, 2099–2105. [Google Scholar] [CrossRef]
- Blassmann, U.; Roehr, A.C.; Frey, O.R.; Vetter-Kerkhoff, C.; Thon, N.; Hope, W.; Briegel, J.; Huge, V. Cerebrospinal fluid penetration of meropenem in neurocritical care patients with proven or suspected ventriculitis: A prospective observational study. Crit. Care 2016, 20, 343. [Google Scholar] [CrossRef] [Green Version]
- Blassmann, U.; Hope, W.; Roehr, A.C.; Frey, O.R.; Vetter-Kerkhoff, C.; Thon, N.; Briegel, J.; Huge, V. CSF penetration of vancomycin in critical care patients with proven or suspected ventriculitis: A prospective observational study. J. Antimicrob. Chemother. 2019, 74, 991–996. [Google Scholar] [CrossRef]
- Beach, J.E.; Perrott, J.; Turgeon, R.D.; Ensom, M.H.H. Penetration of Vancomycin into the Cerebrospinal Fluid: A Systematic Review. Clin. Pharmacokinet. 2017, 56, 1479–1490. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Alffenaar, J.-W.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.-A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef] [PubMed]
- Cataldo, M.A.; Tacconelli, E.; Grilli, E.; Pea, F.; Petrosillo, N. Continuous versus intermittent infusion of vancomycin for the treatment of Gram-positive infections: Systematic review and meta-analysis. J. Antimicrob. Chemother. 2012, 67, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Cies, J.J.; Moore, W.S.; Calaman, S.; Brown, M.; Narayan, P.; Parker, J.; Chopra, A. Pharmacokinetics of Continuous-Infusion Meropenem for the Treatment of Serratia marcescens Ventriculitis in a Pediatric Patient. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2015, 35, e32–e36. [Google Scholar] [CrossRef]
- Kerz, T.; von Loewenich, F.D.; Roberts, J.; Neulen, A.; Ringel, F. Cerebrospinal fluid penetration of very high-dose meropenem: A case report. Ann. Clin. Microbiol. Antimicrob. 2018, 17, 47. [Google Scholar] [CrossRef] [PubMed]
- Pea, F.; Viale, P.; Cojutti, P.; Furlanut, M. Dosing nomograms for attaining optimum concentrations of meropenem by continuous infusion in critically ill patients with severe gram-negative infections: A pharmacokinetics/pharmacodynamics-based approach. Antimicrob. Agents Chemother. 2012, 56, 6343–6348. [Google Scholar] [CrossRef] [Green Version]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am. J. Health Pharm. 2020, 77, 835–864. [Google Scholar] [CrossRef] [Green Version]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Roehr, A.C.; Frey, O.R.; Koeberer, A.; Fuchs, T.; Roberts, J.A.; Brinkmann, A. Anti-infective drugs during continuous hemodialysis—Using the bench to learn what to do at the bedside. Int. J. Artif. Organs 2015, 38, 17–22. [Google Scholar] [CrossRef]
- Imani, S.; Buscher, H.; Marriott, D.; Gentili, S.; Sandaradura, I. Too much of a good thing: A Retrospective Study of β-Lactam Concentration–Toxicity Relationships. J. Antimicrob. Chemother. 2017, 72, 2891–2897. [Google Scholar] [CrossRef]
- Tunkel, A.R.; Hasbun, R.; Bhimraj, A.; Byers, K.; Kaplan, S.L.; Scheld, W.M.; van de Beek, D.; Bleck, T.P.; Garton, H.J.L.; Zunt, J.R. 2017 Infectious Diseases Society of America’s Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis. Clin. Infect. Dis. 2017, 64, e34–e65. [Google Scholar] [CrossRef] [PubMed]
- Huttner, A.; Von Dach, E.; Renzoni, A.; Huttner, B.D.; Affaticati, M.; Pagani, L.; Daali, Y.; Pugin, J.; Karmime, A.; Fathi, M.; et al. Augmented renal clearance, low β-lactam concentrations and clinical outcomes in the critically ill: An observational prospective cohort study. Int. J. Antimicrob. Agents 2015, 45, 385–392. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | |
|---|---|
| Age, years, median (min, max) | 53 (29, 84) |
| Weight, kg, median (min, max) | 75 (62, 110) |
| Height, cm, median (min, max) | 180 (160, 190) |
| Body-Mass-Index, kg/m2, median (min, max) | 24.5 (22.9, 32.1) |
| Sex, male/female | 7/2 |
| Meropenem | Vancomycin | ||
|---|---|---|---|
| Patient 1 | Cserum [mg/L] | 25.7 | 24.5 |
| CCSF [mg/L] | 6.4 | 4.2 | |
| CCSF/Cserum | 0.25 | 0.17 | |
| Patient 2 | Cserum [mg/L] | 29.3 | 25.0 |
| CCSF [mg/L] | 9.8 | 12.5 | |
| CCSF/Cserum | 0.33 | 0.50 | |
| Patient 3 | Cserum [mg/L] | 21.3 | 22.5 |
| CCSF [mg/L] | 4.6 | 1.7 | |
| CCSF/Cserum | 0.22 | 0.07 | |
| Patient 4 | Cserum [mg/L] | 25.6 | 33.0 |
| CCSF [mg/L] | 3.4 | 1.9 | |
| CCSF/Cserum | 0.13 | 0.06 | |
| Patient 5 | Cserum [mg/L] | 19.3 | 17.8 |
| CCSF [mg/L] | 2.9 | 1.2 | |
| CCSF/Cserum | 0.15 | 0.07 | |
| Patient 6 | Cserum [mg/L] | 14.1 | 21.5 |
| CCSF [mg/L] | 0.8 | 0.5 | |
| CCSF/Cserum | 0.06 | 0.02 | |
| Patient 7 | Cserum [mg/L] | 18.9 | 25.7 |
| CCSF [mg/L] | 1.4 | 1.2 | |
| CCSF/Cserum | 0.07 | 0.05 | |
| Patient 8 | Cserum [mg/L] | 17.9 | 23.3 |
| CCSF [mg/L] | 2.2 | 1.5 | |
| CCSF/Cserum | 0.12 | 0.06 | |
| Patient 9 | Cserum [mg/L] | 32.9 | 28.2 |
| CCSF [mg/L] | 5.7 | 4.5 | |
| CCSF/Cserum | 0.17 | 0.16 | |
| Median | Cserum [mg/L] | 21.3 | 24.5 |
| CCSF [mg/L] | 3.4 | 1.7 | |
| CCSF/Cserum | 0.15 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiede, C.; Chiriac, U.; Dubinski, D.; Raimann, F.J.; Frey, O.R.; Röhr, A.C.; Wieduwilt, A.; Eibach, M.; Filmann, N.; Senft, C.; et al. Cerebrospinal Fluid Concentrations of Meropenem and Vancomycin in Ventriculitis Patients Obtained by TDM-Guided Continuous Infusion. Antibiotics 2021, 10, 1421. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111421
Tiede C, Chiriac U, Dubinski D, Raimann FJ, Frey OR, Röhr AC, Wieduwilt A, Eibach M, Filmann N, Senft C, et al. Cerebrospinal Fluid Concentrations of Meropenem and Vancomycin in Ventriculitis Patients Obtained by TDM-Guided Continuous Infusion. Antibiotics. 2021; 10(11):1421. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111421
Chicago/Turabian StyleTiede, Christoph, Ute Chiriac, Daniel Dubinski, Florian J. Raimann, Otto R. Frey, Anka C. Röhr, Anna Wieduwilt, Michael Eibach, Natalie Filmann, Christian Senft, and et al. 2021. "Cerebrospinal Fluid Concentrations of Meropenem and Vancomycin in Ventriculitis Patients Obtained by TDM-Guided Continuous Infusion" Antibiotics 10, no. 11: 1421. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111421