
Anti-MRSA Cephalosporin versus Vancomycin-Based Treatment for Acute Bacterial Skin and Skin Structure Infection: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

Abstract
:1. Introduction
2. Methods
2.1. Study Search and Selection
2.2. Outcome Measurement
2.3. Data Analysis
3. Results
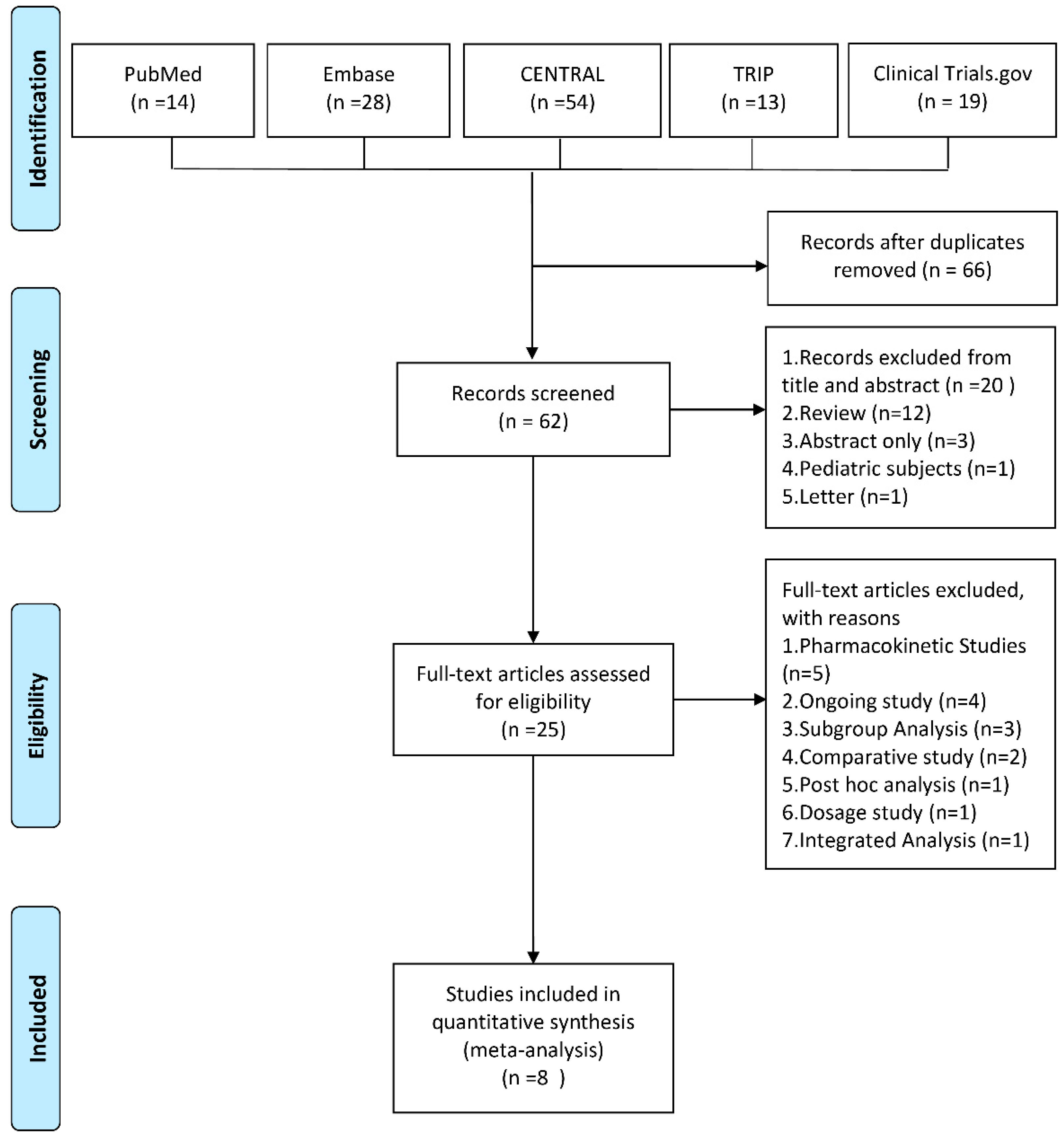
3.1. Study Selection
3.2. Study Characteristics
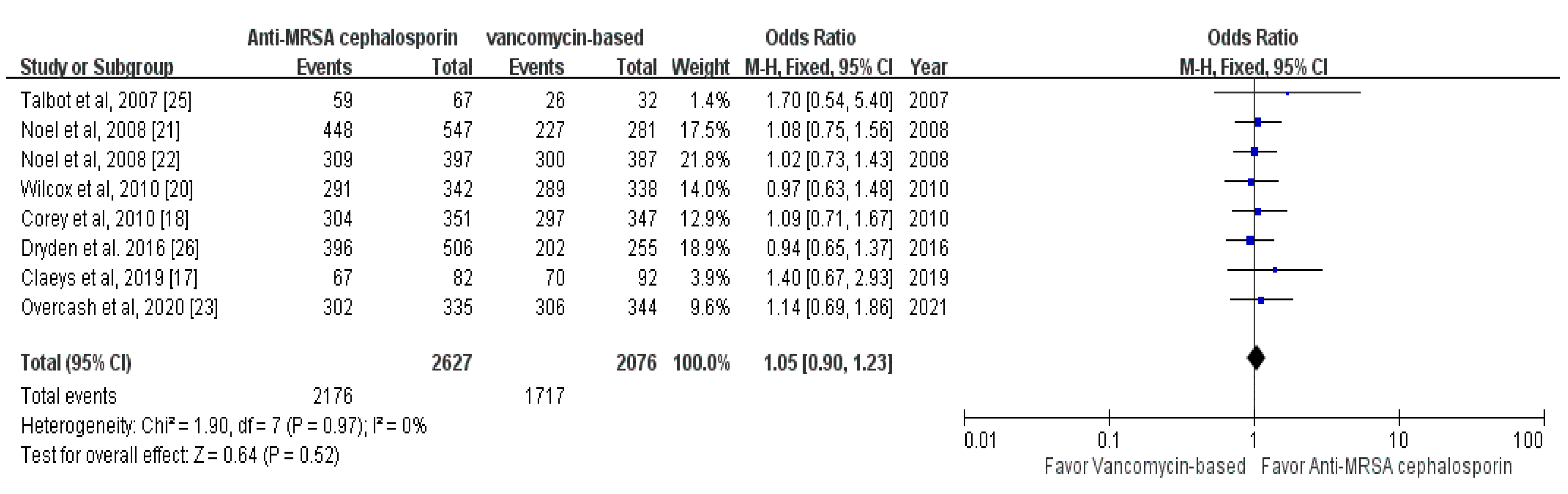
3.3. Clinical Efficacy
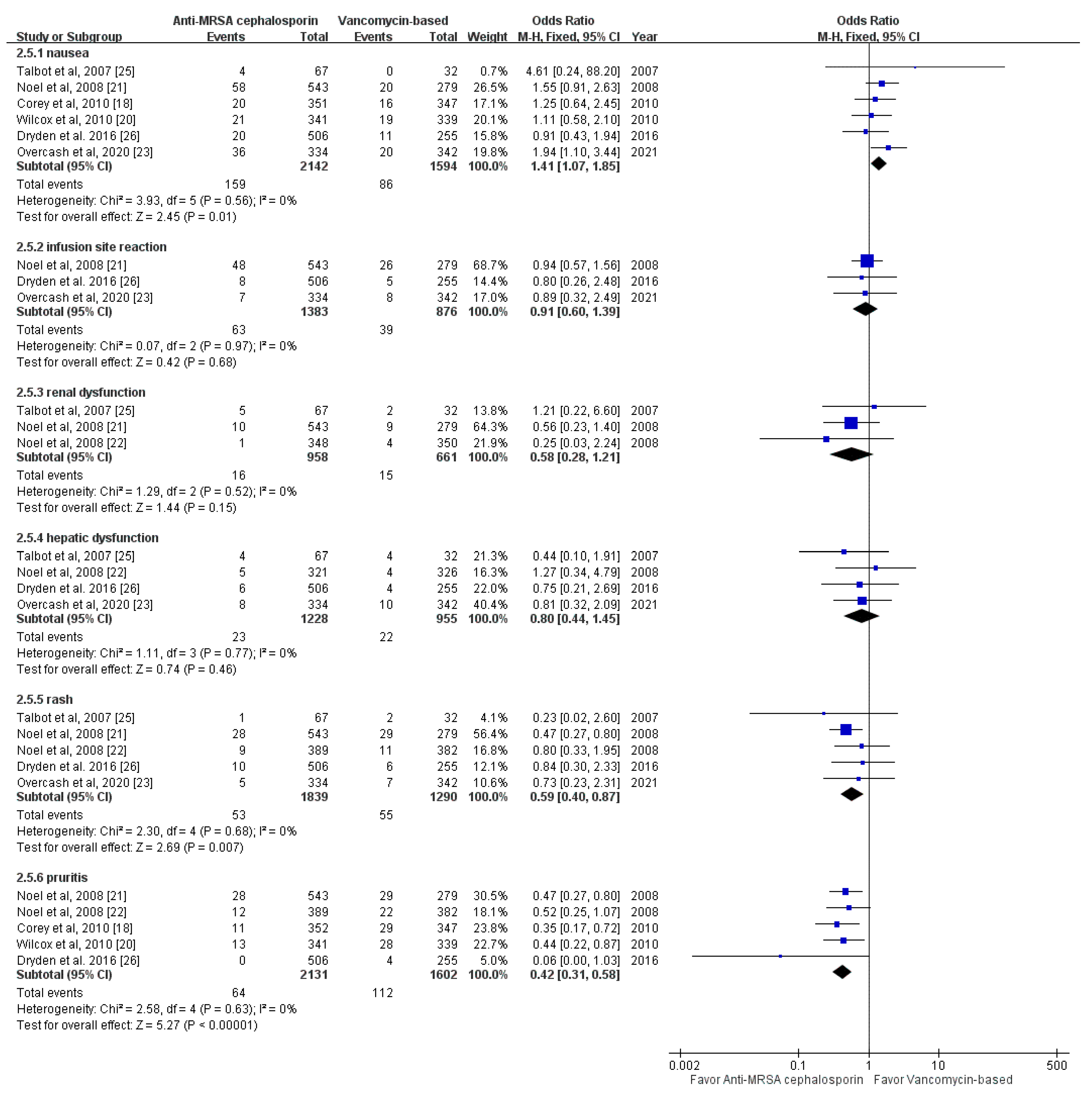
3.4. Adverse Events
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Edelsberg, J.; Taneja, C.; Zervos, M.; Haque, N.; Moore, C.; Reyes, K.; Spalding, J.; Jiang, J.; Oster, G. Trends in US hospital admissions for skin and soft tissue infections. Emerg. Infect. Dis. 2009, 15, 1516–1518. [Google Scholar] [CrossRef]
- Mistry, R.D. Skin and soft tsue infections in ambulatory care settings: Setting a new trend. Clin. Infect. Dis. 2020, 70, 2719–2720. [Google Scholar] [CrossRef]
- Hersh, A.L.; Chambers, H.F.; Maselli, J.H.; Gonzales, R. National trends in ambulatory visits and antibiotic prescribing for skin and soft-tissue infections. Arch. Intern. Med. 2008, 168, 1585–1591. [Google Scholar] [CrossRef] [PubMed]
- Fritz, S.A.; Shapiro, D.J.; Hersh, A.L. National trends in incidence of purulent skin and soft tissue infections in patients presenting to ambulatory and emergency department settings, 2000–2015. Clin. Infect. Dis. 2020, 70, 2715–2718. [Google Scholar] [CrossRef]
- Lopez, F.A.; Lartchenko, S. Skin and soft tissue infections. Infect. Dis. Clin. N. Am. 2006, 20, 759–772. [Google Scholar] [CrossRef] [PubMed]
- Breyre, A.; Frazee, B.W. Skin and soft tissue infections in the emergency department. Emerg. Med. Clin. N. Am. 2018, 36, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Frei, C.R.; Makos, B.R.; Daniels, K.R.; Oramasionwu, C.U. Emergence of community-acquired methicillin-resistant Staphylococcus aureus skin and soft tissue infections as a common cause of hospitalization in United States children. J. Pediatr. Surg. 2010, 45, 1967–1974. [Google Scholar] [CrossRef]
- Hatlen, T.J.; Miller, L.G. Staphylococcal skin and soft tissue infections. Infect. Dis. Clin. N. Am. 2021, 35, 81–105. [Google Scholar] [CrossRef] [PubMed]
- Odell, C.A. Community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) skin infections. Curr. Opin. Pediatr. 2010, 22, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Stevens, D.L.; Bisno, A.L.; Chambers, H.F.; Dellinger, E.P.; Goldstein, E.J.; Gorbach, S.L.; Hirschmann, J.V.; Kaplan, S.L.; Montoya, J.G.; Wade, J.C.; et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2014, 59, e10–e52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barberán, J. Possible clinical indications of ceftobiprole. Rev. Esp. Quimioter. 2019, 32 (Suppl. 3), 29–33. [Google Scholar]
- Scott, L.J. Ceftaroline fosamil: A review in complicated skin and soft tissue infections and community-acquired pneumonia. Drugs 2016, 76, 1659–1674. [Google Scholar] [CrossRef]
- Rolston, K.V.I.; Jamal, M.A.; Nesher, L.; Shelburne, S.A.; Raad, I.; Prince, R.A. In vitro activity of ceftaroline and comparator agents against Gram-positive and Gram-negative clinical isolates from cancer patients. Int. J. Antimicrob. Agents 2017, 49, 416–421. [Google Scholar] [CrossRef]
- Sader, H.S.; Farrell, D.J.; Flamm, R.K.; Jones, R.N. Antimicrobial activity of ceftaroline tested against Staphylococcus aureus from surgical skin and skin structure infections in US medical centers. Surg. Infect. (Larchmt) 2016, 17, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Barbour, A.; Schmidt, S.; Rand, K.H.; Derendorf, H. Ceftobiprole: A novel cephalosporin with activity against Gram-positive and Gram-negative pathogens, including methicillin-resistant Staphylococcus aureus (MRSA). Int. J. Antimicrob. Agents 2009, 34, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Flamm, R.K.; Duncan, L.R.; Hamed, K.A.; Smart, J.I.; Mendes, R.E.; Pfaller, M.A. Ceftobiprole activity against bacteria from skin and skin structure infections in the United States from 2016 through 2018. Antimicrob. Agents Chemother. 2020, 64, e02566-e19. [Google Scholar] [CrossRef] [PubMed]
- Claeys, K.C.; Zasowski, E.J.; Trinh, T.D.; Casapao, A.M.; Pogue, J.M.; Bhatia, N.; Mynatt, R.P.; Wilson, S.S.; Arthur, C.; Welch, R.; et al. Open-label randomized trial of early clinical outcomes of ceftaroline fosamil versus vancomycin for the treatment of acute bacterial skin and skin structure infections at risk of methicillin-resistant Staphylococcus aureus. Infect. Dis. Ther. 2019, 8, 199–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corey, G.R.; Wilcox, M.H.; Talbot, G.H.; Thye, D.; Friedland, D.; Baculik, T. CANVAS 1, the first Phase III, randomized, double-blind study evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J. Antimicrob. Chemother. 2010, 65 (Suppl. 4), iv41–iv51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Hajj, M.S.; Turgeon, R.D.; Wilby, K.J. Ceftaroline fosamil for community-acquired pneumonia and skin and skin structure infections: A systematic review. Int. J. Clin. Pharm. 2017, 39, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, M.H.; Corey, G.R.; Talbot, G.H.; Thye, D.; Friedland, D.; Baculik, T. CANVAS 2, the second phase III, randomized, double-blind study evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J. Antimicrob. Chemother. 2010, 65 (Suppl. 4), iv53–iv65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noel, G.J.; Bush, K.; Bagchi, P.; Ianus, J.; Strauss, R.S. A randomized, double-blind trial comparing ceftobiprole medocaril with vancomycin plus ceftazidime for the treatment of patients with complicated skin and skin-structure infections. Clin. Infect. Dis. 2008, 46, 647–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noel, G.J.; Strauss, R.S.; Amsler, K.; Heep, M.; Pypstra, R.; Solomkin, J.S. Results of a double-blind, randomized trial of ceftobiprole treatment of complicated skin and skin structure infections caused by gram-positive bacteria. Antimicrob. Agents Chemother. 2008, 52, 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overcash, J.S.; Kim, C.; Keech, R.; Gumenchuk, I.; Ninov, B.; Gonzalez-Rojas, Y.; Waters, M.; Simeonov, S.; Engelhardt, M.; Saulay, M.; et al. Ceftobiprole compared with vancomycin plus aztreonam in the treatment of acute bacterial skin and skin structure infections: Results of a phase 3, randomized, double-blind Trial (TARGET). Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Talbot, G.H.; Thye, D.; Das, A.; Ge, Y. Phase 2 study of ceftaroline versus standard therapy in treatment of complicated skin and skin structure infections. Antimicrob. Agents Chemother. 2007, 51, 3612–3616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dryden, M.; Zhang, Y.; Wilson, D.; Iaconis, J.P.; Gonzalez, J. A Phase III, randomized, controlled, non-inferiority trial of ceftaroline fosamil 600 mg every 8 h versus vancomycin plus aztreonam in patients with complicated skin and soft tissue infection with systemic inflammatory response or underlying comorbidities. J. Antimicrob. Chemother. 2016, 71, 3575–3584. [Google Scholar] [CrossRef] [PubMed]
- Lan, S.H.; Chang, S.P.; Lai, C.C.; Lu, L.C.; Chao, C.M. Ceftaroline efficacy and safety in treatment of complicated skin and soft tissue infection: A systemic review and meta-analysis of randomized controlled trials. J. Clin. Med. 2019, 8, 776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lan, S.H.; Lee, H.Z.; Lai, C.C.; Chang, S.P.; Lu, L.C.; Hung, S.H.; Lin, W.T. Clinical efficacy and safety of ceftobiprole in the treatment of acute bacterial skin and skin structure infection: A systematic review and meta-analysis of randomized controlled trials. Expert Rev. Anti-Infect. Ther. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Design | Study Sites | Inclusion Criteria | Study Drug | Comparator | No of ITT Population | Primary Outcome | |
|---|---|---|---|---|---|---|---|---|
| Study Drug | Comparator | |||||||
| Talbot et al., 2007 [25] | Randomized, observer-blinded, phase 2 trial | 15 sites in the US, South America, South Africa, and Russia | Adults with cSSSI requiring hospitalization and intravenous antibiotic | Ceftaroline | Vancomycin with or without aztreonam | 67 | 32 | Clinical cure rate at TOC |
| Claeys et al., 2019 [17] | Prospective, open-label, randomized trial | 3 centers in the US | Adult patients with ABSSSI required intravenous antibiotic and at risk for MRSA | Ceftaroline | Vancomycin | 82 | 92 | Early clinical response rate |
| Dryden et al. 2016 [26] | Prospective, randomized, double-blind trial | 111 centers in 28 countries | Adults with cSSSI requiring hospitalization and intravenous antibiotic | Ceftaroline | Vancomycin plus aztreonam | 514 | 258 | Clinical cure rate at TOC |
| Corey et al., 2010 [18] | Randomized, double-blind, active-controlled, parallel group trial | 55 centers in 10 countries | Adults with cSSSI requiring hospitalization and intravenous antibiotic | Ceftaroline | Vancomycin plus aztreonam | 353 | 349 | Clinical cure rate at TOC |
| Wilcox et al., 2010 [20] | Randomized, double-blind, active-controlled, parallel group trial | 56 centers in 12 countries | Adults with cSSSI requiring intravenous antibiotic | Ceftaroline | Vancomycin plus aztreonam | 348 | 346 | Clinical cure rate at TOC |
| Noel et al., 2008 [21] | Randomized, double-blind trial | 129 sites in North America, Europe, South America, Asia, and Africa | Adults with cSSSI requiring intravenous antibiotic | Ceftobiprole | Vancomycin plus ceftazidime | 547 | 281 | Clinical and microbiological outcomes at TOC |
| Noel et al., 2008 [22] | Randomized, double-blind trial | 129 sites in Europe, Asia, Africa, South America, and North America | Adults with cSSSI due to documented or suspected gram-positive pathogen | Ceftobiprole | Vancomycin | 397 | 387 | Clinical cure rate at TOC |
| Overcash et al., 2020 [23] | Randomized, double-blind, active-controlled, parallel-group trial | 32 sites in the US, Bulgaria, Hungary, and Ukraine | Adult patients with ABSSSI required hospitalization and intravenous antibiotic | Ceftobiprole | Vancomycin plus aztreonam | 335 | 344 | Early clinical response and clinical success at TOC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-Y.; Chen, W.-C.; Lai, C.-C.; Shih, T.-P.; Tang, H.-J. Anti-MRSA Cephalosporin versus Vancomycin-Based Treatment for Acute Bacterial Skin and Skin Structure Infection: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antibiotics 2021, 10, 1020. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10081020
Chen C-Y, Chen W-C, Lai C-C, Shih T-P, Tang H-J. Anti-MRSA Cephalosporin versus Vancomycin-Based Treatment for Acute Bacterial Skin and Skin Structure Infection: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antibiotics. 2021; 10(8):1020. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10081020
Chicago/Turabian StyleChen, Ching-Yi, Wang-Chun Chen, Chih-Cheng Lai, Tzu-Ping Shih, and Hung-Jen Tang. 2021. "Anti-MRSA Cephalosporin versus Vancomycin-Based Treatment for Acute Bacterial Skin and Skin Structure Infection: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Antibiotics 10, no. 8: 1020. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10081020