
Treatment of Residual Periodontal Pockets Using a Hyaluronic Acid-Based Gel: A 12 Month Multicenter Randomized Triple-Blinded Clinical Trial

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Results
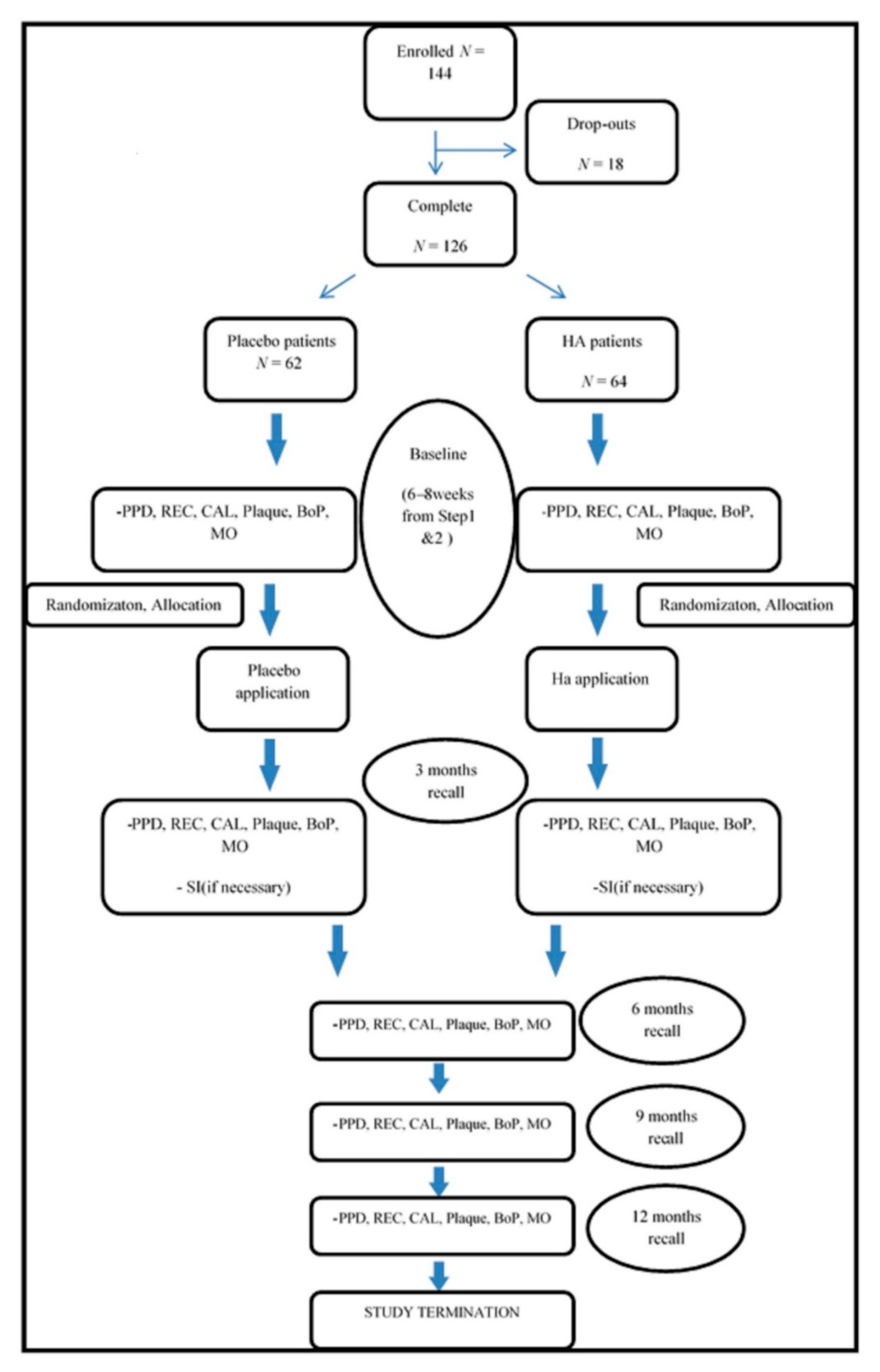
2.1. Population Characteristics
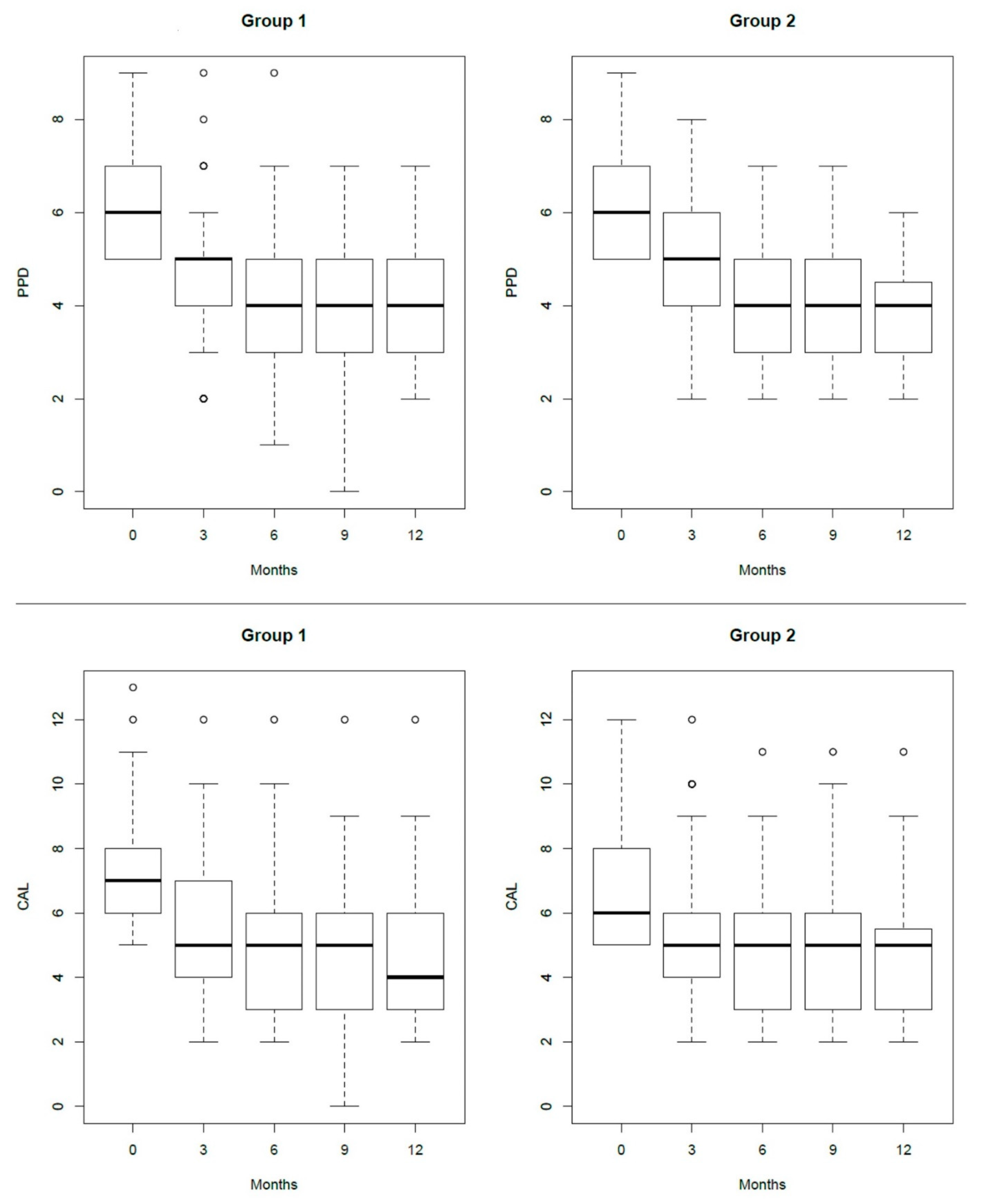
2.2. Clinical Evaluation
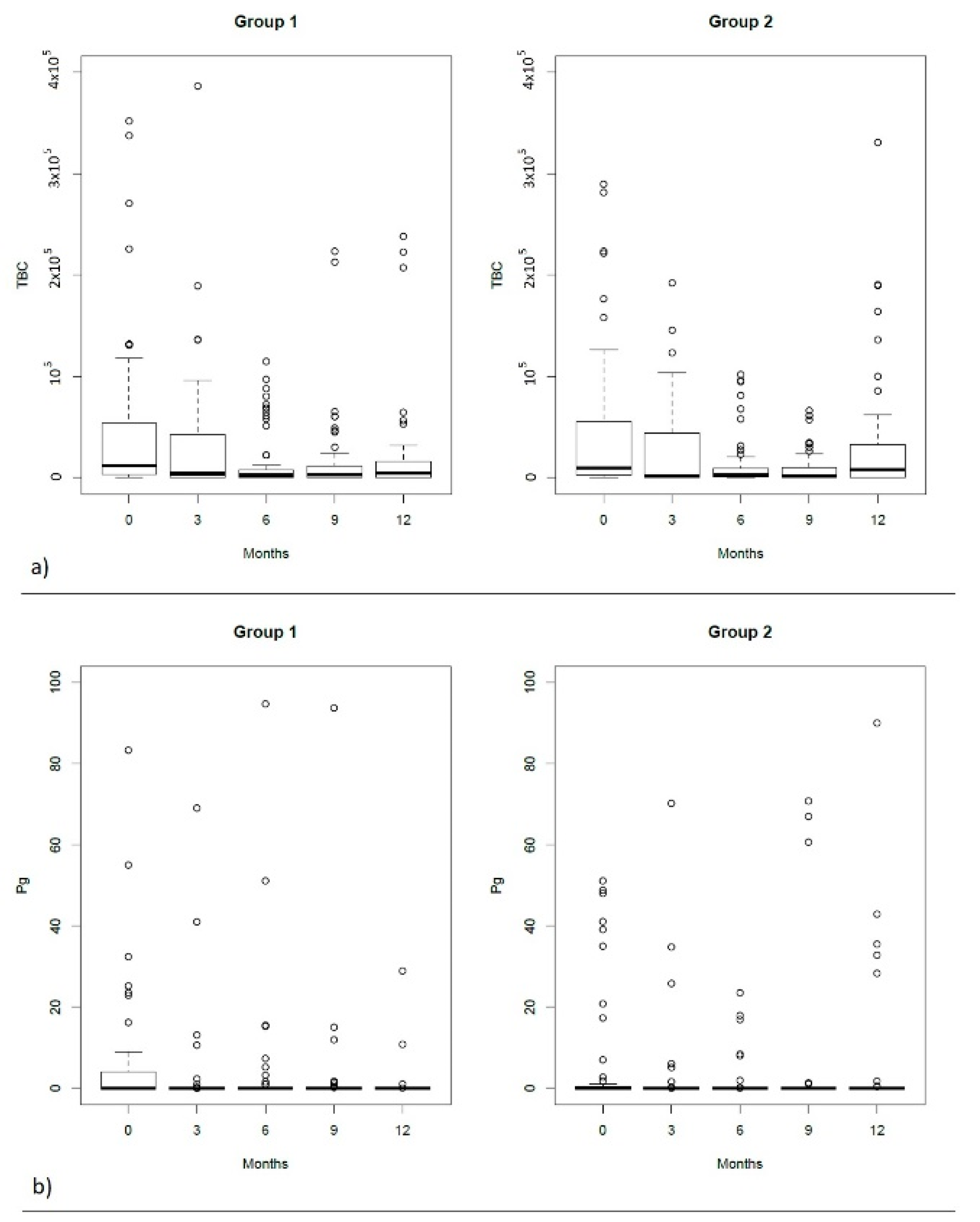
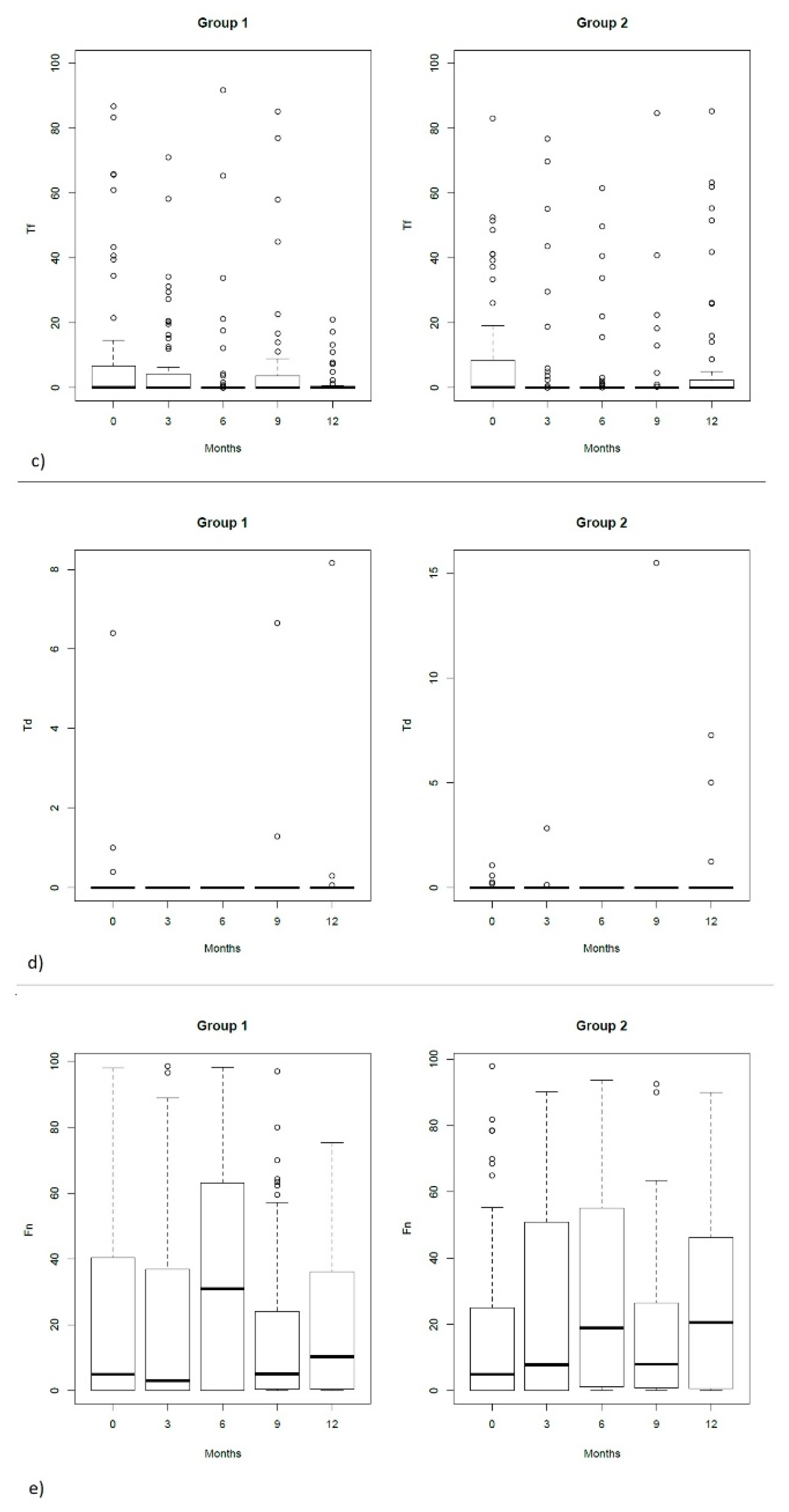
2.3. Microbiological Evaluation
3. Discussion
4. Materials and Methods
4.1. Population
4.2. Study Design, Randomization, Allocation Concealment and Blinding
4.3. Treatment Procedure
4.4. Treatment Assessment
4.4.1. Clinical Assessment
4.4.2. Microbiological Assessment
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holtfreter, B.; Schützhold, S.; Kocher, T. Is periodontitis prevalence declining? A review of the current literature. Curr. Oral Health Rep. 2014, 1, 251–261. [Google Scholar] [CrossRef] [Green Version]
- Norderyd, O.; Koch, G.; Papias, A.; Anastasaki Köhler, A.; Nydell Helkimo, A.; Brahm, C.O.; Lindmark, U.; Lindfors, N.; Mattsson, A.; Rolander, B.; et al. Oral health of individuals aged 3–80 years in Jonkoping, Sweden during 40 years (1973– 2013). II. Review of clinical and radiographic findings. Swed. Dent. J. 2015, 39, 69–86. [Google Scholar] [PubMed]
- Eke, P.I.; Wei, L.; Borgnakke, W.S.; Thornton-Evans, G.; Zhang, X.; Lu, H.; McGuire, L.C.; Genco, R.J. Periodontitis prevalence in adults ≥ 65 years of age, in the USA. Periodontol. 2000 2016, 72, 76–95. [Google Scholar] [CrossRef]
- Lindhe, J.; Nyman, S. Long-term maintenance of patients treated for advanced periodontal disease. J. Clin. Periodontol. 1984, 11, 504–514. [Google Scholar] [CrossRef]
- Matuliene, G.; Pjetursson, B.E.; Salvi, G.E.; Schmidlin, K.; Bragger, U.; Zwahlen, M.; Lang, N.P. Influence of residual pockets on progression of periodontitis and tooth loss: Results after 11 years of maintenance. J. Clin. Periodontol. 2008, 35, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Persson, G.R. A systematic review on the use of residual probing depth, bleeding on probing and furcation status following initial periodontal therapy to predict further attachment and tooth loss. J. Clin. Periodontol. 2002, 29, 82–89. [Google Scholar] [CrossRef]
- Loos, B.G.; Needleman, I. Endpoints of active periodontal therapy. J. Clin. Periodontol. 2020, 47, 61–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S.; EFP Workshop Participants and Methodological Consultants. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef]
- Dahiya, P.; Kamal, R. Hyaluronic Acid: A boon in periodontal therapy. N. Am. J. Med. Sci. 2013, 5, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Bertl, K.; Bruckmann, C.; Isberg, P.E.; Klinge, B.; Gotfredsen, K.; Stavropoulos, A. Hyaluronan in non-surgical and surgical periodontal therapy: A systematic review. J. Clin. Periodontol. 2015, 42, 236–246. [Google Scholar] [CrossRef]
- Susin, C.; Wikesjö, U.M. Regenerative periodontal therapy: 30 years of lessons learned and unlearned. Periodontol. 2000 2013, 62, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Shirakata, Y.; Imafuji, T.; Nakamura, T.; Kawakami, Y.; Shinohara, Y.; Noguchi, K.; Pilloni, A.; Sculean, A. Periodontal wound healing/regeneration of two-wall intrabony defects following reconstructive surgery with cross-linked hyaluronic acid-gel with or without a collagen matrix: A preclinical study in dogs. Quintessence Int. 2021, 308–316. [Google Scholar] [CrossRef]
- Asparuhova, M.B.; Kiryak, D.; Eliezer, M.; Mihov, D.; Sculean, A. Activity of two hyaluronan preparations on primary human oral fibroblasts. J. Periodontal Res. 2019, 54, 33–45. [Google Scholar] [CrossRef]
- Mueller, A.; Fujioka-Kobayashi, M.; Mueller, H.D.; Lussi, A.; Sculean, A.; Schmidlin, P.R.; Miron, R.J. Effect of hyaluronic acid on morphological changes to dentin surfaces and subsequent effect on periodontal ligament cell survival, attachment, and spreading. Clin. Oral Investig. 2017, 21, 1013–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujioka-Kobayashi, M.; Müller, H.D.; Mueller, A.; Lussi, A.; Sculean, A.; Schmidlin, P.R.; Miron, R.J. In vitro effects of hyaluronic acid on human periodontal ligament cells. BMC Oral Health 2017, 17, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilloni, A.; Rimondini, L.; de Luca, M.; Bernard, G.W. Effect of hyaluronan on calcification-nodule formation from human periodontal ligament cell culture. J. Appl. Biomater. Biomech. 2003, 1, 84–90. [Google Scholar]
- Asparuhova, M.B.; Chappuis, V.; Stähli, A.; Buser, D.; Sculean, A. Role of hyaluronan in regulating self-renewal and osteogenic differentiation of mesenchymal stromal cells and pre-osteoblasts. Clin. Oral Investig. 2020, 24, 3923–3937. [Google Scholar] [CrossRef] [Green Version]
- Pilloni, A.; Schmidlin, P.R.; Sahrmann, P.; Sculean, A.; Rojas, M.A. Effectiveness of adjunctive hyaluronic acid application in coronally advanced flap in Miller class I single gingival recession sites: A randomized controlled clinical trial. Clin. Oral Investig. 2019, 23, 1133–1141. [Google Scholar] [CrossRef] [Green Version]
- Lanzrein, C.; Guldener, K.; Imber, J.C.; Katsaros, C.; Stähli, A.; Sculean, A. Treatment of multiple adjacent recessions with the modified coronally advanced tunnel or laterally closed tunnel in conjunction with cross-linked hyaluronic acid and subepithelial connective tissue graft: A report of 15 cases. Quintessence Int. 2020, 51, 710–719. [Google Scholar]
- Pilloni, A.; Nardo, F.; Rojas, M.A. Surgical treatment of a cemental tear-associated bony defect using hyaluronic acid and a resorbable collagen membrane: A 2-year follow-up. Clin. Adv. Periodontics 2019, 9, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Pilloni, A.; Rojas, M.A.; Marini, L.; Russo, P.; Shirakata, Y.; Sculean, A.; Iacono, R. Healing of intrabony defects following regenerative surgery by means of single-flap approach in conjunction with either hyaluronic acid or an enamel matrix derivative: A 24-month randomized controlled clinical trial. Clin. Oral Investig. 2021. [Google Scholar] [CrossRef] [PubMed]
- Eliezer, M.; Imber, J.C.; Sculean, A.; Pandis, N.; Teich, S. Hyaluronic acid as adjunctive to non-surgical and surgical periodontal therapy: A systematic review and meta-analysis. Clin. Oral Investig. 2019, 23, 3423–3435. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Lang, N.P.; Karring, T.H. Clinical Periodontology and Implant. Dentistry; Blackwell Munksgaard: Oxford, UK, 2008; 1313p. [Google Scholar]
- Chauhan, A.S.; Bains, V.K.; Gupta, V.; Singh, G.P.; Patil, S.S. Comparative analysis of hyaluronan gel and xanthan-based chlorhexidine gel, as adjunct to scaling and root planing with scaling and root planing alone in the treatment of chronic periodontitis: A preliminary study. Contemp. Clin. Dent. 2013, 4, 54–61. [Google Scholar] [PubMed]
- Gontiya, G.; Galgali, S.R. Effect of hyaluronan on periodontitis: A clinical and histological study. J. Indian Soc. Periodontol. 2012, 16, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Eick, S.; Renatus, A.; Heinicke, M.; Pfister, W.; Stratul, S.I.; Jentsch, H. Hyaluronic acid as an adjunct after scaling and root planing: A prospective randomized clinical trial. J. Periodontol. 2013, 84, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Graziani, F.; Karapetsa, D.; Alonso, B.; Herrera, D. Nonsurgical and surgical treatment of periodontitis: How many options for one disease? Periodontol. 2000 2017, 75, 152–188. [Google Scholar] [CrossRef]
- Sahrmann, P.; Puhan, M.A.; Attin, T.; Schmidlin, P.R. Systematic review on the effect of rinsing with povidone-iodine during nonsurgical periodontal therapy. J. Periodontal Res. 2010, 45, 153–164. [Google Scholar] [CrossRef] [Green Version]
- Matesanz-Perez, P.; Garcıa-Gargallo, M.; Figuero, E.; Bascones-Martınez, A.; Sanz, M.; Herrera, D. A systematic review on the effects of local antimicrobials as adjuncts to subgingival debridement, compared with subgingival debridement alone, in the treatment of chronic periodontitis. J. Clin. Periodontol. 2013, 40, 227–241. [Google Scholar] [CrossRef]
- Bostanci, H.S.; Arpak, M.N. Long-term evaluation of surgical periodontal treatment with and without maintenance care. J. Nihon Univ. Sch. Dent. 1991, 33, 152–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera, D.; Alonso, B.; Leon, R.; Roldan, S.; Sanz, M. Antimicrobial therapy in periodontitis: The use of systemic antimicrobials against the subgingival biofilm. J. Clin. Periodontol. 2008, 35, 45–66. [Google Scholar] [CrossRef]
- Bonito, A.J.; Lux, L.; Lohr, K.N. Impact of local adjuncts to scaling and root planing in periodontal disease therapy: A systematic review. J. Periodontol. 2005, 76, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Hanes, P.J.; Purvis, J.P. Local anti-infective therapy: Pharmacological agents. A systematic review. Ann. Periodontol. 2003, 8, 79–98. [Google Scholar] [CrossRef] [PubMed]
- Sgolastra, F.; Gatto, R.; Petrucci, A.; Monaco, A. Effectiveness of systemic amoxicillin/metronidazole as adjunctive therapy to scaling and root planing in the treatment of chronic periodontitis: A systematic review and meta-analysis. J. Periodontol. 2012, 83, 1257–1269. [Google Scholar] [CrossRef] [Green Version]
- Martın-Cabezas, R.; Davideau, J.L.; Tenenbaum, H.; Huck, O. Clinical efficacy of probiotics as an adjunctive therapy to non-surgical periodontal treatment of chronic periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2016, 43, 520–530. [Google Scholar] [CrossRef]
- Tomasi, C.; Leyland, A.H.; Wennstrom, J.L. Factors influencing the outcome of non-surgical periodontal treatment: A multilevel approach. J. Clin. Periodontol. 2007, 34, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Offenbacher, S.; Salvi, G.E.; Beck, J.D.; Williams, R.C. The design and implementation of trials of host modulation agents. Ann. Periodontol. 1997, 2, 199–212. [Google Scholar] [CrossRef]
- Ebersole, J.L.; Dawson, D.A.; Emecen Huja, P.; Pandruvada, S.; Basu, A.; Nguyen, L.; Gonzalez, O.A. Age and periodontal health-immunological view. Curr. Oral Health Rep. 2018, 5, 229–241. [Google Scholar] [CrossRef]
- Ebersole, J.L.; Graves, C.L.; Gonzalez, O.A.; Dawson, D.; Morford, L.A.; Huja, P.E.; Wallet, S.M. Aging, inflammation, immunity and periodontal disease. Periodontol. 2000 2016, 72, 54–75. [Google Scholar] [CrossRef]
- Larsson, L. Current concepts of epigenetics and its role in periodontitis. Curr. Oral Health Rep. 2017, 4, 286–293. [Google Scholar] [CrossRef] [Green Version]
- Loos, B.G.; van Dyke, T.E. The role of inflammation and genetics in periodontal disease. Periodontol. 2000 2020, 83, 26–39. [Google Scholar] [CrossRef]
- Tettamanti, L.; Gaudio, R.M.; Cura, F.; Mucchi, D.; Illuzzi, N.; Tagliabue, A. Prevalence of periodontal pathogens among italian patients with chronic periodontitis: A retrospective study on 2992 patients. Oral Implantol. 2017, 10, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Apatzidou, D.A.; Riggio, M.P.; Kinane, D.F. Quadrant root planing versus same-day full-mouth root planing. II. Microbiological findings. J. Clin. Periodontol. 2004, 31, 141–148. [Google Scholar] [CrossRef]
- Pirnazar, P.; Wolinsky, L.; Nachnani, S.; Haake, S.; Pilloni, A.; Bernard, G.W. Bacteriostatic effects of hyaluronic acid. J. Periodontol. 1999, 70, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Carlson, G.A.; Dragoo, J.L.; Samimi, B.; Bruckner, D.A.; Bernard, G.W.; Hedrick, M.; Benhaim, P. Bacteriostatic properties of biomatrices against common orthopaedic pathogens. Biochem. Biophys Res. Commun. 2004, 321, 472–478. [Google Scholar] [CrossRef]
- Kang, J.H.; Kim, Y.Y.; Chang, J.Y.; Kho, H.S. Influences of hyaluronic acid on the anticandidal activities of lysozyme and the peroxidasesystem. Oral Dis. 2011, 17, 577–583. [Google Scholar] [CrossRef]
- Jentsch, H.F.R.; Roccuzzo, M.; Pilloni, A.; Kasaj, A.; Fimmers, R.; Jepsen, S. Flapless application of enamel matrix derivative in periodontal retreatment: A multicentre randomized feasibility trial. J. Clin. Periodontol. 2021, 48, 659–667. [Google Scholar] [CrossRef]
- Miron, R.J.; Bosshardt, D.D.; Laugisch, O.; Katsaros, C.; Buser, D.; Sculean, A. Enamel matrix protein adsorption to root surfaces in the presence or absence of human blood. J. Periodontol. 2012, 83, 885–892. [Google Scholar] [CrossRef]
- Scully, M.F.; Kakkar, V.V.; Goodwin, C.A.; O’Regan, M. Inhibition of fibrinolytic activity by hyaluronan and its alcohol ester derivatives. Thromb. Res. 1995, 78, 255–258. [Google Scholar] [CrossRef]
- West, D.C.; Hampson, I.N.; Arnold, F.; Kumar, S. Angiogenesis induced by degradation products of hyaluronic acid. Science 1985, 228, 1324–1326. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T0 | p Value 0–3 | T3 | p Value 3–6 | T6 | p Value 6–9 | T9 | p Value 9–12 | T12 | |
|---|---|---|---|---|---|---|---|---|---|
| PD1 | 6 (5–7) | <0.001 * | 5 (4–5) | <0.001 * | 4 (3–5) | 0.4 | 4 (3–5) | 0.4 | 4 (3–5) |
| PD2 | 6 (5–7) | <0.001 * | 5 (4–6) | 0.001 * | 4 (3–5) | 0.5 | 4 (3–5) | 0.003 * | 4 (3–4.5) |
| p value | 1.0 | 1.0 | 1.0 | 1.0 | 1.000 | ||||
| CAL1 | 7 (6–8) | <0.001 * | 5 (4–6.7) | <0.001 * | 5 (3–6) | 1.0 | 5 (3–6) | 1.0 | 4 (3–6) |
| CAL2 | 6 (5–8) | <0.001 * | 5 (4–6) | 0.002 * | 5 (3–6) | 0.5 | 5 (3–6) | 0.07 | 5 (3–5.5) |
| p value | 1.0 | 1.0 | 1.0 | 1.0 | 1.000 | ||||
| BoP1 | 48 (77.4%) | <0.001 * | 33 (53.2%) | 1.0 | 25 (40–3%) | 1.0 | 19 (31.1%) | 1.0 | 23 (37.7%) |
| BoP2 | 43 (67.2%) | <0.001 * | 33 (51.6%) | 0.8 | 30 (46.9%) | 0.8 | 16 (25.4%) | 0.8 | 15 (23.8%) |
| p value | 1.0 | 1.0 | 1.000 | 1.0 | 0.690 | ||||
| Plaque1 | 26 (41.9%) | <0.001 * | 21 (33.9%) | 0.2 | 14 (22.6%) | 1.0 | 21 (34.4%) | 1.0 | 16 (26.2%) |
| Plaque2 | 18 (28.1%) | <0.001 * | 14 (21.9%) | 0.2 | 14 (21.9%) | 0.5 | 23 (36.5%) | 0.2 | 20 (31.7%) |
| p value | 0.8 | 0.8 | 1.0 | 1.0 | 1.000 | ||||
| PD ≥ 5 mm1 | 64 (100%) | <0.001 * | 38 (59.4%) | 0.01 * | 29 (45.3%) | 1.0 | 25 (39.7%) | 1.0 | 16 (25.4%) |
| PD ≥ 5 mm2 | 62 (100%) | <0.001 * | 32 (51.6%) | 0.4 | 22 (35.5%) | 1.0 | 20 (33.3%) | 1.0 | 17 (27.9%) |
| p value | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| PPD0 = 5 mm | |||||
|---|---|---|---|---|---|
| T3 | T6 | T9 | T12 | ||
| PPD ≤ 3 mm | Ha | 53% (9/17) | 65% (11/17) | 65% (11/17) | 56% (9/16) |
| Placebo | 27% (6/22) | 50% (11/22) | 55% (12/22) | 59% (13/22) | |
| p value | 0.1 | 0.4 | 0.5 | 0.9 | |
| PPD ≤ 4 mm | Ha | 71% (12/17) | 82%(14/17) | 76% (13/17) | 81% (13/16) |
| Placebo | 55% (12/22) | 73% (16/22) | 86% (19/22) | 86% (19/22) | |
| p value | 0.3 | 0.5 | 0.4 | 0.7 | |
| PPD ≤ 4 mm without BOP | Ha | 59% (10/17) | 71% (12/17) | 76% (13/17) | 69% (11/16) |
| Placebo | 55% (12/22) | 59% (13/22) | 82% (18/22) | 82% (18/22) | |
| p value | 0.8 | 0.5 | 0.7 | 0.4 | |
| PPD0 ≥ 6 mm | |||||
| PPD ≤ 3 mm | Ha | 13% (6/45) | 29% (13/45) | 35% (15/43) | 44% (19/43) |
| Placebo | 19% (8/42) | 21% (9/42) | 24% (10/41) | 44% (18/41) | |
| p value | 0.5 | 0.4 | 0.3 | 1 | |
| PPD ≤ 4 mm | Ha | 40% (18/45) | 58% (26/45) | 60% (26/43) | 70% (30/43) |
| Placebo | 33% (14/42) | 45% (19/42) | 46% (19/41) | 68% (28/41) | |
| p value | 0.5 | 0.2 | 0.3 | 0.9 | |
| PPD ≤ 4 mm without BOP | Ha | 33% (15/45) | 53% (24/45) | 51% (22/43) | 58% (25/43) |
| Placebo | 24% (10/42) | 29% (12/42) | 37% (15/41) | 61% (25/41) | |
| p value | 0.3 | 0.02 * | 0.2 | 0.8 | |
| PPD0 Total | |||||
| PPD ≤ 3 mm | Ha | 24% (15/62) | 39% (24/62) | 43% (26/60) | 47% (28/60) |
| Placebo | 22% (14/64) | 31% (20/64) | 35% (22/63) | 49% (31/63) | |
| p value | 0.8 | 0.4 | 0.3 | 0.8 | |
| PPD ≤ 4 mm | Ha | 46% (30/62) | 89% (40/62) | 69% (39/60) | 77% (43/60) |
| Placebo | 40% (26/64) | 54% (35/64) | 62% (38/63) | 78% (47/63) | |
| p value | 0.8 | 0.5 | 0.1 | 0.6 | |
| PPD ≤ 4 mm without BOP | Ha | 40% (25/62) | 58% (36/62) | 59% (35/60) | 59% (36/60) |
| Placebo | 35% (22/64) | 37% (25/64) | 54% (33/63) | 68% (43/63) | |
| p value | 0.4 | 0.2 | 0.7 | 0.5 | |
| Table Title | T0 | p Value 0–3 | T3 | p Value 3–6 | T6 | p Value 6–9 | T9 | p Value 9–12 | T12 |
|---|---|---|---|---|---|---|---|---|---|
| TBC1 | 11,850 (3200–53,690) | 0.004 * | 4130 (326–42,865) | 0.2 | 2539 (468–7922) | 1.0 | 2882 (137–11,500) | 1.0 | 4626 (575–15,217) |
| TBC2 | 9813 (2917–54,970) | 0.001 * | 2125 (175–43,572) | 0.05 | 2670 (1000–8995) | 0.6 | 1700 (213–10,295) | 0.05 | 8335 (330–32,700) |
| p value | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | ||||
| Pg1 | 0 (0–4.1) | 0.03 * | 0 (0–0) | 1.0 | 0 (0–0) | 1.0 | 0 (0–0) | 1.0 | 0 (0–0) |
| Pg2 | 0 (0–0.5) | 0.1 | 0 (0–0) | 1.0 | 0 (0–0) | 1.0 | 0 (0–0) | 1.0 | 0 (0–0) |
| p value | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | ||||
| Td1 | 0 (0–0) | 1.0 | 0 (0–0) | 1.0 | 0 (0–0) | 1.0 | 0 (0–0) | 0.1 | 0 (0–0) |
| Td2 | 0 (0–0) | 1.0 | 0 (0–0) | 1.0 | 0 (0–0) | 1.0 | 0 (0–0) | 1.0 | 0 (0–0) |
| p value | 1.0 | 0.6 | 1.0 | 1.0 | 1.0 | ||||
| Tf1 | 0.1 (0–6.6) | 0.6 | 0 (0–3.6) | 1.0 | 0 (0–0) | 1.0 | 0 (0–3.7) | 1.0 | 0 (0–0.4) |
| Tf2 | 0.2 (0–7.7) | 0.3 | 0 (0–0) | 1.0 | 0 (0–0.1) | 1.0 | 0 (0–0) | 1.0 | 0 (0–2.3) |
| p value | 1.0 | 0.6 | 1.0 | 0.05 | 1.0 | ||||
| Fn1 | 5 (0.1–40.5) | 1.0 | 3.01 (0–36.9) | 0.04 * | 30.9 (0.04–63.1) | 0.01 | 5.1 (0.4–24) | 1.0 | 10.3 (0.6–35.6) |
| Fn2 | 4.95 (0.1–24.7) | 1.0 | 7.85 (0–50.8) | 1.0 | 18.9 (1.1–55) | 0.4 | 7.9 (0.9–26.6) | 1.0 | 20.6 (0.6–46.3) |
| p value | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pilloni, A.; Zeza, B.; Kuis, D.; Vrazic, D.; Domic, T.; Olszewska-Czyz, I.; Popova, C.; Kotsilkov, K.; Firkova, E.; Dermendzieva, Y.; et al. Treatment of Residual Periodontal Pockets Using a Hyaluronic Acid-Based Gel: A 12 Month Multicenter Randomized Triple-Blinded Clinical Trial. Antibiotics 2021, 10, 924. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10080924
Pilloni A, Zeza B, Kuis D, Vrazic D, Domic T, Olszewska-Czyz I, Popova C, Kotsilkov K, Firkova E, Dermendzieva Y, et al. Treatment of Residual Periodontal Pockets Using a Hyaluronic Acid-Based Gel: A 12 Month Multicenter Randomized Triple-Blinded Clinical Trial. Antibiotics. 2021; 10(8):924. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10080924
Chicago/Turabian StylePilloni, Andrea, Blerina Zeza, Davor Kuis, Domagoj Vrazic, Tomislav Domic, Iwona Olszewska-Czyz, Christina Popova, Kamen Kotsilkov, Elena Firkova, Yana Dermendzieva, and et al. 2021. "Treatment of Residual Periodontal Pockets Using a Hyaluronic Acid-Based Gel: A 12 Month Multicenter Randomized Triple-Blinded Clinical Trial" Antibiotics 10, no. 8: 924. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10080924