Antimicrobial Resistance Patterns in Clostridioides difficile Strains Isolated from Neonates in Germany

 , , , and
, , , and 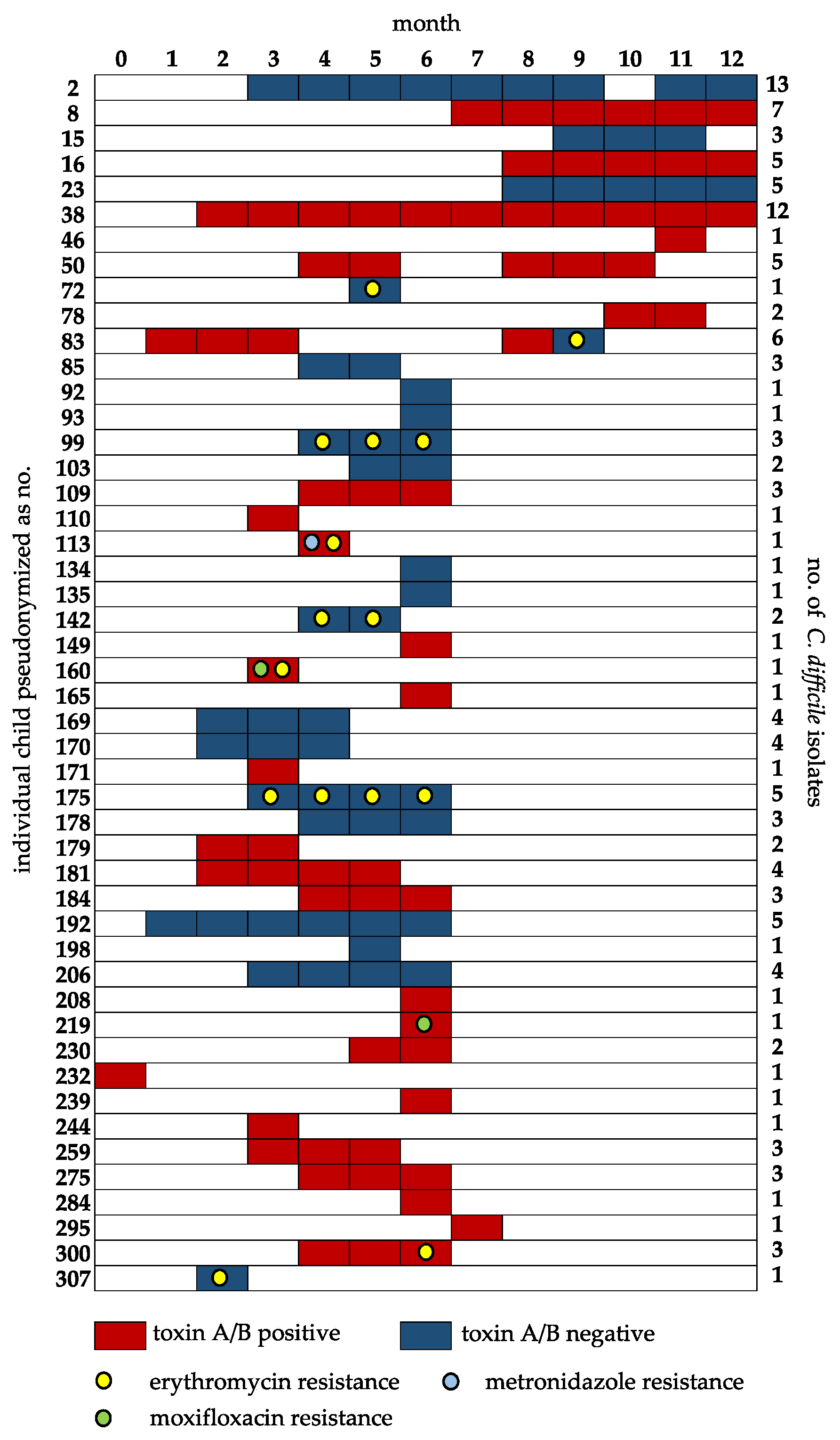{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Patient Samples
2.2. Isolation of C. difficile
2.3. Antimicrobial Resistance Testing
2.4. PCR Targeting Toxin Genes
2.5. Proteotyping for Detection of Ribotype 027 and 176
3. Results and Discussion
3.1. Recorded Antimicrobial Resistance
3.2. Recorded Distribution of Toxin Genes
3.3. Proteotyping-Based Assessment for the Ribotypes 027 and 176
3.4. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hensgens, M.P.; Goorhuis, A.; Dekkers, O.M.; Kuijper, E.J. Time interval of increased risk for Clostridium difficile infection after exposure to antibiotics. J. Antimicrob. Chemother. 2012, 67, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Curry, S.R. Clostridium difficile. Clin. Lab. Med. 2017, 37, 341–369. [Google Scholar] [CrossRef] [PubMed]
- Lübbert, C.; John, E.; von Müller, L. Clostridium difficile infection: Guideline-based diagnosis and treatment. Dtsch. Arztebl. Int. 2014, 111, 723–731. [Google Scholar] [PubMed] [Green Version]
- Bolton, R.P.; Tait, S.K.; Dear, P.R.; Losowsky, M.S. Asymptomatic neonatal colonization by Clostridium difficile. Arch. Dis. Child. 1984, 59, 466–472. [Google Scholar] [CrossRef] [Green Version]
- Penders, J.; Thijs, C.; Vink, C.; Stelma, F.F.; Snijders, B.; Kummeling, I.; van den Brandt, P.A.; Stobberingh, E.E. Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics. 2006, 118, 511–521. [Google Scholar] [CrossRef] [Green Version]
- Jangi, S.; Lamont, J.T. Asymptomatic colonization by Clostridium difficile in infants: Implications for disease in later life. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 2–7. [Google Scholar] [CrossRef]
- Rousseau, C.; Levenez, F.; Fouqueray, C.; Doré, J.; Collignon, A.; Lepage, P. Clostridium difficile colonization in early infancy is accompanied by changes in intestinal microbiota composition. J. Clin. Microbiol. 2011, 49, 858–865. [Google Scholar] [CrossRef] [Green Version]
- Rousseau, C.; Poilane, I.; De Pontual, L.; Maherault, A.C.; Le Monnier, A.; Collignon, A. Clostridium difficile carriage in healthy infants in the community: A potential reservoir for pathogenic strains. Clin. Infect. Dis. 2012, 55, 1209–1215. [Google Scholar] [CrossRef] [Green Version]
- Al-Jumaili, I.J.; Shibley, M.; Lishman, A.H.; Record, C.O. Incidence and origin of Clostridium difficile in neonates. J. Clin. Microbiol. 1984, 19, 77–78. [Google Scholar] [CrossRef] [Green Version]
- Delmée, M.; Verellen, G.; Avesani, V.; Francois, G. Clostridium difficile in neonates: Serogrouping and epidemiology. Eur. J. Pediatr. 1988, 147, 36–40. [Google Scholar] [CrossRef]
- Triadafilopoulos, G.; Shah, M.H.; Pothoulakis, C. The chemotactic response of human granulocytes to Clostridium difficile toxin A is age dependent. Am. J. Gastroenterol. 1991, 86, 1461–1465. [Google Scholar] [PubMed]
- Shin, J.H.; High, K.P.; Warren, C.A. Older Is Not Wiser, Immunologically Speaking: Effect of Aging on Host Response to Clostridium difficile Infections. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 916–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Govind, R.; Dupuy, B. Secretion of Clostridium difficile toxins A and B requires the holin-like protein TcdE. PLoS Pathog. 2012, 8, e1002727. [Google Scholar] [CrossRef] [PubMed]
- Di Bella, S.; Ascenzi, P.; Siarakas, S.; Petrosillo, N.; di Masi, A. Clostridium difficile Toxins A and B: Insights into Pathogenic Properties and Extraintestinal Effects. Toxins 2016, 8, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kociolek, L.K.; Espinosa, R.O.; Gerding, D.N.; Hauser, A.R.; Ozer, E.A.; Budz, M.; Balaji, A.; Chen, X.; Tanz, R.R.; Yalcinkaya, N.; et al. Natural Clostridioides difficile Toxin Immunization in Colonized Infants. Clin. Infect. Dis. 2020, 70, 2095–2102. [Google Scholar] [CrossRef]
- Spigaglia, P.; Barbanti, F.; Mastrantonio, P. European Study Group on Clostridium difficile (ESGCD). Multidrug resistance in European Clostridium difficile clinical isolates. J. Antimicrob. Chemother. 2011, 66, 2227–2234. [Google Scholar] [CrossRef] [Green Version]
- He, M.; Miyajima, F.; Roberts, P.; Ellison, L.; Pickard, D.J.; Martin, M.J.; Connor, T.R.; Harris, S.R.; Fairley, D.; Bamford, K.B.; et al. Emergence and global spread of epidemic healthcare-associated Clostridium difficile. Nat. Genet. 2013, 45, 109–113. [Google Scholar] [CrossRef]
- Peng, Z.; Jin, D.; Kim, H.B.; Stratton, C.W.; Wu, B.; Tang, Y.W.; Sun, X. Update on Antimicrobial Resistance in Clostridium difficile: Resistance Mechanisms and Antimicrobial Susceptibility Testing. J. Clin. Microbiol. 2017, 55, 1998–2008. [Google Scholar] [CrossRef] [Green Version]
- Pépin, J.; Valiquette, L.; Alary, M.E.; Villemure, P.; Pelletier, A.; Forget, K.; Pépin, K.; Chouinard, D. Clostridium difficile-associated diarrhea in a region of Quebec from 1991 to 2003: A changing pattern of disease severity. CMAJ 2004, 171, 466–472. [Google Scholar] [CrossRef] [Green Version]
- Clements, A.C.; Magalhães, R.J.; Tatem, A.J.; Paterson, D.L.; Riley, T.V. Clostridium difficile PCR ribotype 027: Assessing the risks of further worldwide spread. Lancet Infect. Dis. 2010, 10, 395–404. [Google Scholar] [CrossRef]
- Freeman, J.; Vernon, J.; Morris, K.; Nicholson, S.; Todhunter, S.; Longshaw, C.; Wilcox, M.H. Pan-European Longitudinal Surveillance of Antibiotic Resistance among Prevalent Clostridium difficile Ribotypes’ Study Group. Pan-European longitudinal surveillance of antibiotic resistance among prevalent Clostridium difficile ribotypes. Clin. Microbiol. Infect. 2015, 21, 248. [Google Scholar] [CrossRef] [Green Version]
- Emele, M.F.; Joppe, F.M.; Riedel, T.; Overmann, J.; Rupnik, M.; Cooper, P.; Kusumawati, R.L.; Berger, F.K.; Laukien, F.; Zimmermann, O.; et al. Proteotyping of Clostridioides difficile as Alternate Typing Method to Ribotyping Is Able to Distinguish the Ribotypes RT027 and RT176 From Other Ribotypes. Front. Microbiol. 2019, 10, 2087. [Google Scholar] [CrossRef]
- Jin, D.; Luo, Y.; Huang, C.; Cai, J.; Ye, J.; Zheng, Y.; Wang, L.; Zhao, P.; Liu, A.; Fang, W.; et al. Molecular Epidemiology of Clostridium difficile Infection in Hospitalized Patients in Eastern China. J. Clin. Microbiol. 2017, 55, 801–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snydman, D.R.; McDermott, L.A.; Jacobus, N.V.; Thorpe, C.; Stone, S.; Jenkins, S.G.; Goldstein, E.J.; Patel, R.; Forbes, B.A.; Mirrett, S.; et al. U.S.-Based National Sentinel Surveillance Study for the Epidemiology of Clostridium difficile-Associated Diarrheal Isolates and Their Susceptibility to Fidaxomicin. Antimicrob. Agents Chemother. 2015, 59, 6437–6443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoesser, N.E.; Martin, J.; Mawer, D.; Eyre, D.W.; Walker, A.S.; Peto, T.E.; Crook, D.W.; Wilcox, M.H. Risk factors for Clostridium difficile acquisition in infants: Importance of study design. Clin. Infect. Dis. 2013, 56, 1680–1681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toltzis, P.; Kim, J.; Dul, M.; Zoltanski, J.; Smathers, S.; Zaoutis, T. Presence of the epidemic North American Pulsed Field type 1 Clostridium difficile strain in hospitalized children. J. Pediatr. 2009, 154, 607–608. [Google Scholar] [CrossRef]
- Cloud, J.; Noddin, L.; Pressman, A.; Hu, M.; Kelly, C. Clostridium difficile strain NAP-1 is not associated with severe disease in a nonepidemic setting. Clin. Gastroenterol. Hepatol. 2009, 7, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Walk, S.T.; Micic, D.; Jain, R.; Lo, E.S.; Trivedi, I.; Liu, E.W.; Almassalha, L.M.; Ewing, S.A.; Ring, C.; Galecki, A.T.; et al. Clostridium difficile ribotype does not predict severe infection. Clin. Infect. Dis. 2012, 55, 1661–1668. [Google Scholar] [CrossRef] [PubMed]
- Hahn, A.; Meyer, C.G.; Frickmann, H. Impact of diagnostic methods on efficacy estimation—A proof-of-principle based on historical examples. Trop. Med. Int. Health 2020, 25, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Hahn, A.; Frickmann, H.; Zautner, A.E. Impact of Case Definitions on Efficacy Estimation in Clinical Trials-A Proof-of-Principle Based on Historical Examples. Antibiotics 2020, 9, 379. [Google Scholar] [CrossRef]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tilkorn, F.K.M.T.; Frickmann, H.; Simon, I.S.; Schwanbeck, J.; Horn, S.; Zimmermann, O.; Groß, U.; Bohne, W.; Zautner, A.E. Antimicrobial Resistance Patterns in Clostridioides difficile Strains Isolated from Neonates in Germany. Antibiotics 2020, 9, 481. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9080481
Tilkorn FKMT, Frickmann H, Simon IS, Schwanbeck J, Horn S, Zimmermann O, Groß U, Bohne W, Zautner AE. Antimicrobial Resistance Patterns in Clostridioides difficile Strains Isolated from Neonates in Germany. Antibiotics. 2020; 9(8):481. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9080481
Chicago/Turabian StyleTilkorn, Friederike K. M. T., Hagen Frickmann, Isabel S. Simon, Julian Schwanbeck, Sebastian Horn, Ortrud Zimmermann, Uwe Groß, Wolfgang Bohne, and Andreas E. Zautner. 2020. "Antimicrobial Resistance Patterns in Clostridioides difficile Strains Isolated from Neonates in Germany" Antibiotics 9, no. 8: 481. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9080481