
Effect of Optical Properties of Lithium Disilicate Glass Ceramics and Light-Curing Protocols on the Curing Performance of Resin Cement


Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimens Preparation
2.1.1. Preparation of Glass Ceramic Specimens
2.1.2. Preparation of Resin Cement Specimens
2.2. Testing Methods
2.2.1. Determination of the Irradiance
2.2.2. Measurement of Light Transmittance
2.2.3. Degree of Conversion Measurement
2.2.4. Vickers Microhardness Measurement
2.3. Statistical Analysis
3. Results
3.1. Irradiance of the Light-Curing Unit
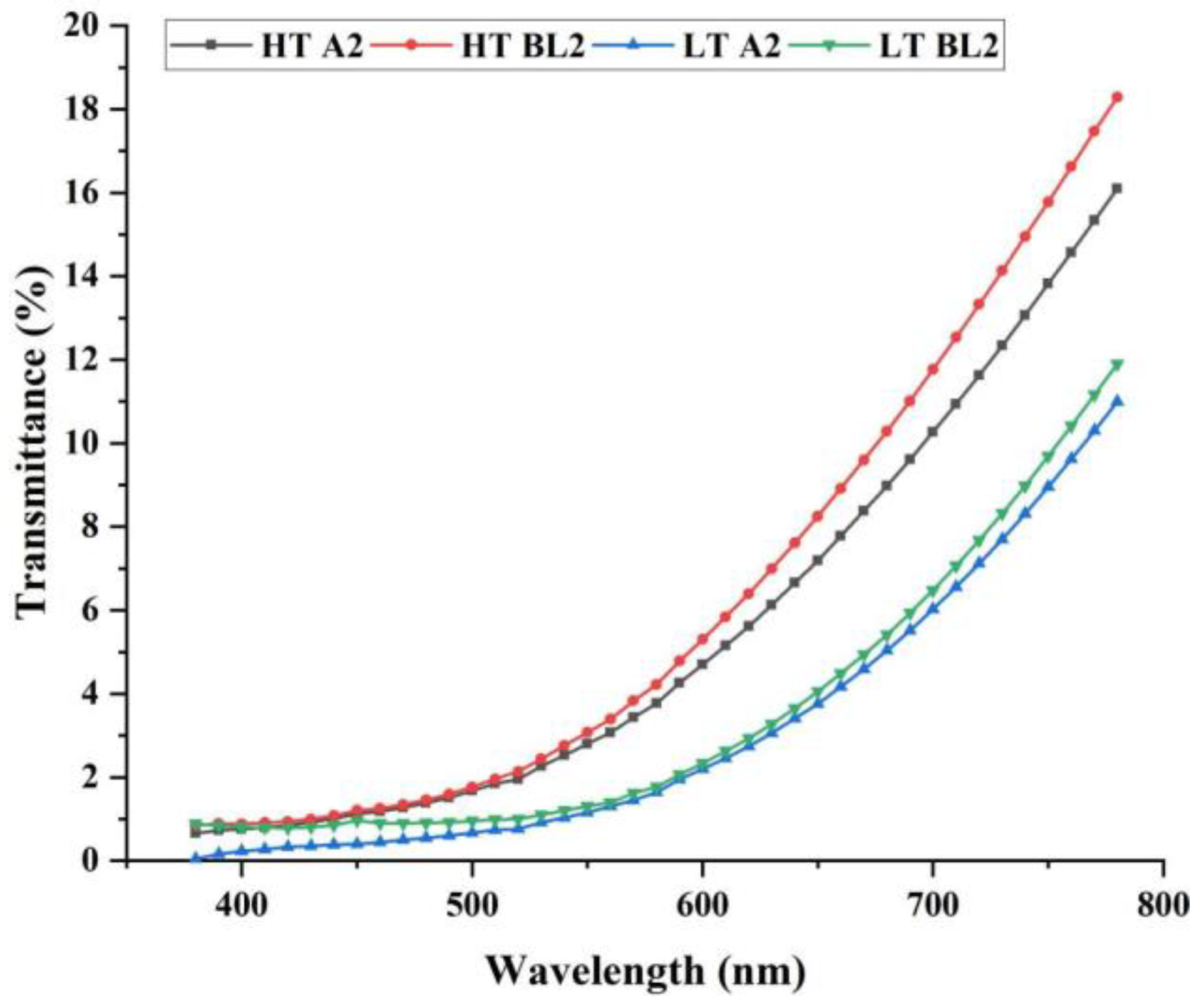
3.2. Light Transmittance
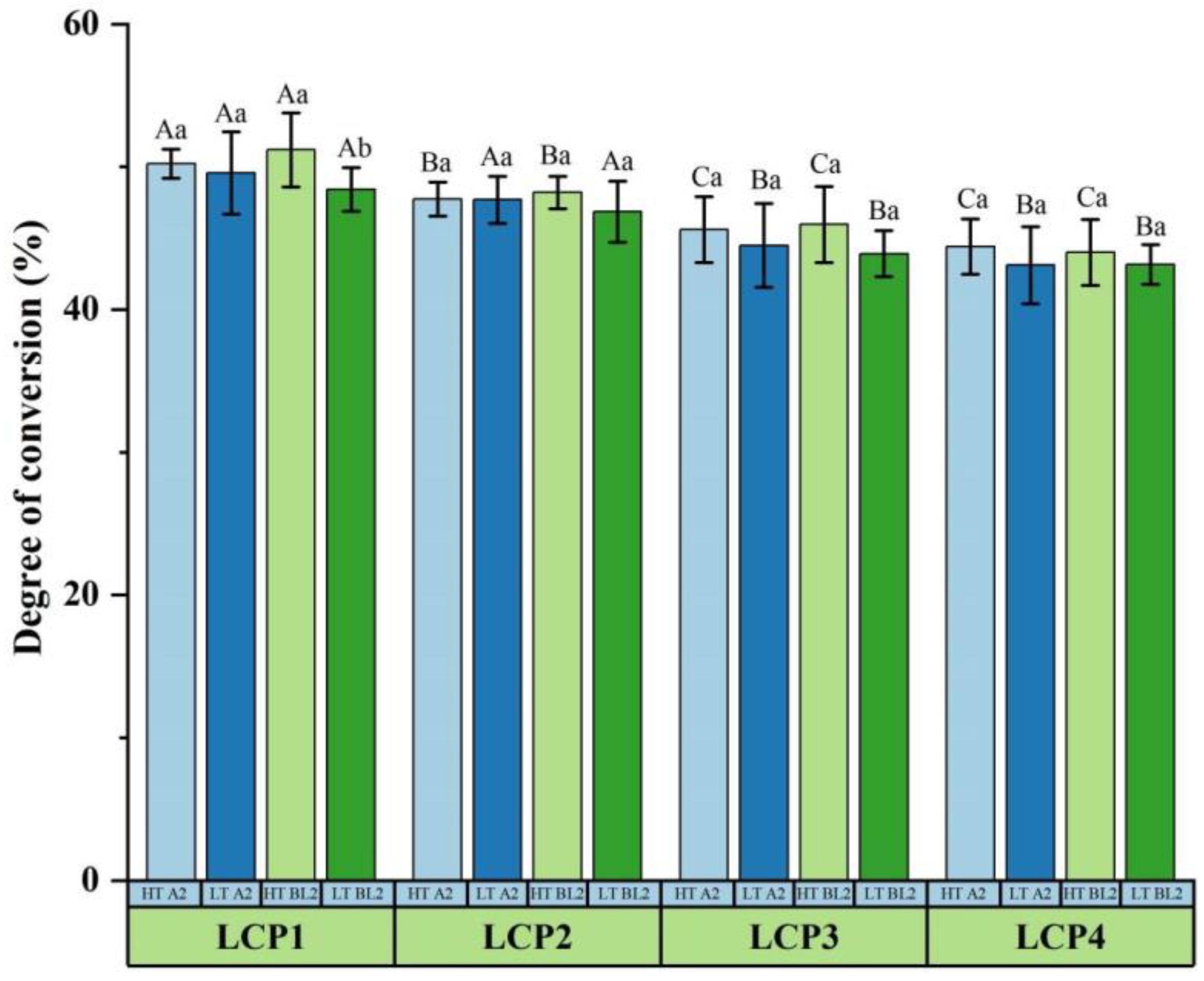
3.3. Degree of Conversion
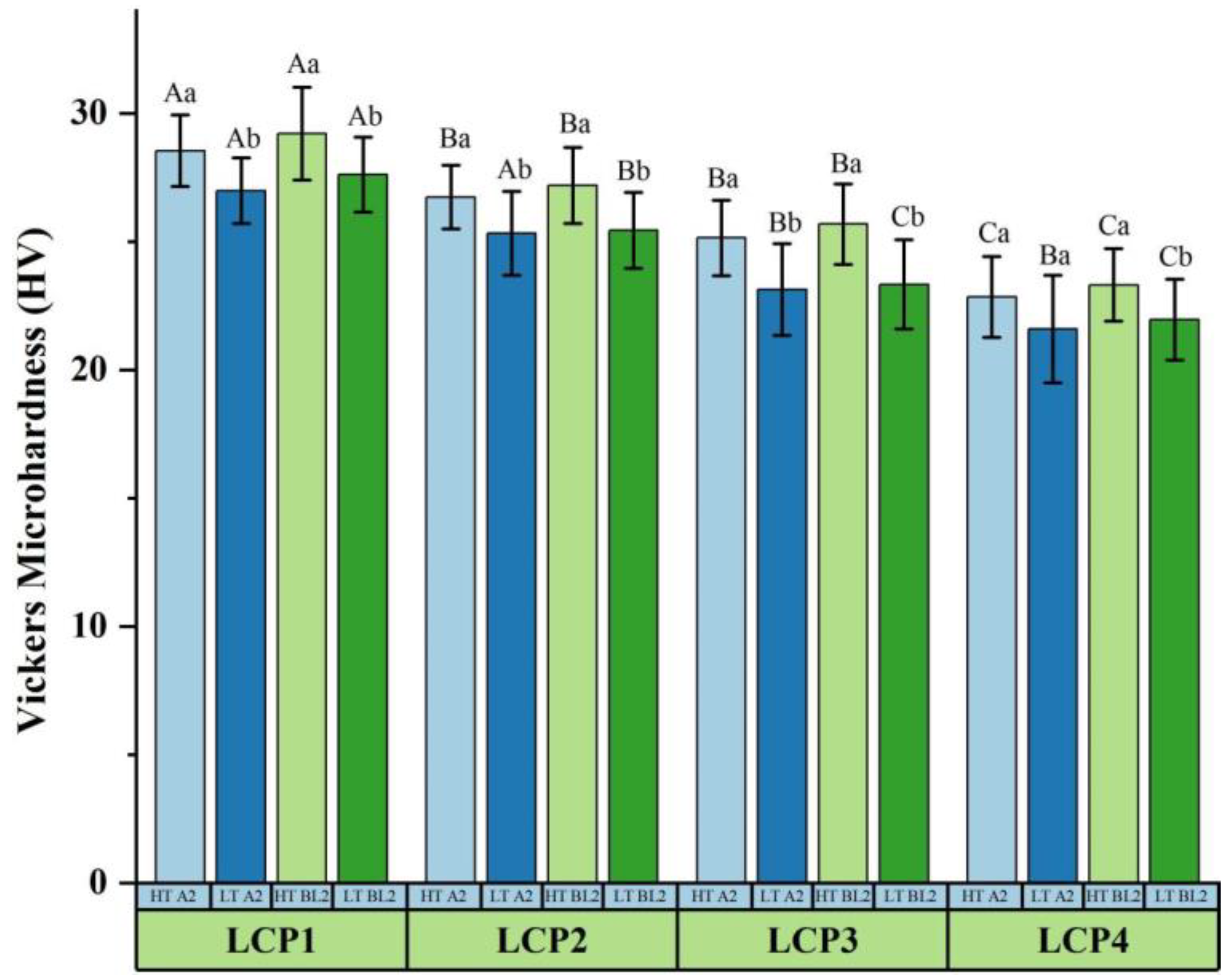
3.4. Vickers Microhardness
4. Discussion
5. Conclusions
- (1)
- When the thickness of lithium disilicate glass ceramics is 0.8 mm, the transparency has an influence on the irradiance, ceramic transmittance and the polymerization performance of the light-cured resin cement, and increases with the transparency of lithium disilicate glass-ceramics. Ceramics with high transparency have higher transmittance, less attenuation of irradiance and easier to obtain excellent polymerization properties. The shade of ceramic did not affect the ceramic transmittance and the curing performance of resin cement.
- (2)
- Light-curing protocols affect the polymerization performance of the resin cement. An appropriate increase in irradiance and exposure time can improve curing performance.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Calamia, J.R. The etched porcelain veneer technique. N. Y. State Dent. J. 1988, 54, 48–50. [Google Scholar] [PubMed]
- Land, M.F.; Hopp, C.D. Survival rates of all-ceramic systems differ by clinical indication and fabrication method. J. Evid. Based Dent. Pract. 2010, 10, 37–38. [Google Scholar] [CrossRef] [PubMed]
- Beier, U.S.; Kapferer, I.; Burtscher, D.; Dumfahrt, H. Clinical performance of porcelain laminate veneers for up to 20 years. Int. J. Prosthodont. 2012, 25, 79–85. [Google Scholar] [PubMed]
- Friedman, M.J. A 15-year review of porcelain veneer failure—A clinician’s observations. Compend. Contin. Educ. Dent. 1998, 19, 625–628, 630, 632 passim; quiz 638. [Google Scholar] [PubMed]
- Morimoto, S.; Albanesi, R.B.; Sesma, N.; Agra, C.M.; Braga, M.M. Main Clinical Outcomes of Feldspathic Porcelain and Glass-Ceramic Laminate Veneers: A Systematic Review and Meta-Analysis of Survival and Complication Rates. Int. J. Prosthodont. 2016, 29, 38–49. [Google Scholar] [CrossRef]
- Arif, R.; Dennison, J.B.; Garcia, D.; Yaman, P. Retrospective evaluation of the clinical performance and longevity of porcelain laminate veneers 7 to 14 years after cementation. J. Prosthet. Dent. 2019, 122, 31–37. [Google Scholar] [CrossRef]
- Romanini-Junior, J.C.; Hirata, R.; Bonfante, E.A.; Bordin, D.; Kumagai, R.Y.; Fardin, V.P.; Coelho, P.G.; Reis, A.F. Monolithic CAD/CAM laminate veneers: Reliability and failure modes. Dent. Mater. 2020, 36, 724–732. [Google Scholar] [CrossRef]
- Chen, Y.; Yeung, A.W.K.; Pow, E.H.N.; Tsoi, J.K.H. Current status and research trends of lithium disilicate in dentistry: A bibliometric analysis. J. Prosthet. Dent. 2021, 126, 512–522. [Google Scholar] [CrossRef]
- Wang, C.C.; Fu, P.S.; Wang, J.C.; Lan, T.H.; Lai, P.L.; Du, J.K.; Chen, W.C.; Hung, C.C. Comparison of optical and crystal properties of three translucent yttria-stabilized tetragonal zirconia polycrystals with those of lithium disilicate glass-ceramic material. J. Dent. Sci. 2021, 16, 1247–1254. [Google Scholar] [CrossRef]
- Haralur, S.B.; Alamri, A.A.; Alshehri, S.A.; Alzahrani, D.S.; Alfarsi, M. Influence of Occlusal Thickness and Radicular Extension on the Fracture Resistance of Premolar Endocrowns from Different All-Ceramic Materials. Appl. Sci. 2020, 10, 2696. [Google Scholar] [CrossRef] [Green Version]
- Kollmuss, M.; Kist, S.; Goeke, J.E.; Hickel, R.; Huth, K.C. Comparison of chairside and laboratory CAD/CAM to conventional produced all-ceramic crowns regarding morphology, occlusion, and aesthetics. Clin. Oral Investig. 2016, 20, 791–797. [Google Scholar] [CrossRef] [PubMed]
- De Souza, G.; Braga, R.R.; Cesar, P.F.; Lopes, G.C. Correlation between clinical performance and degree of conversion of resin cements: A literature review. J. Appl. Oral Sci. 2015, 23, 358–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, J.R.; Schmitt, G.U.; Kaizer, M.R.; Boscato, N.; Moraes, R.R. Resin-based luting agents and color stability of bonded ceramic veneers. J. Prosthet. Dent. 2015, 114, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, E.; Bolay, Ş.; Hickel, R.; Ilie, N. Shear bond strength of porcelain laminate veneers to enamel, dentine and enamel-dentine complex bonded with different adhesive luting systems. J. Dent. 2013, 41, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Kilinc, E.; Antonson, S.A.; Hardigan, P.C.; Kesercioglu, A. The effect of ceramic restoration shade and thickness on the polymerization of light- and dual-cure resin cements. Oper. Dent. 2011, 36, 661–669. [Google Scholar] [CrossRef]
- Hooshmand, T.; Mohajerfar, M.; Keshvad, A.; Motahhary, P. Microleakage and marginal gap of adhesive cements for noble alloy full cast crowns. Oper. Dent. 2011, 36, 258–265. [Google Scholar] [CrossRef]
- Goldberg, M. In Vitro and in vivo studies on the toxicity of dental resin components: A review. Clin. Oral Investig. 2008, 12, 1–8. [Google Scholar] [CrossRef]
- Janda, R.; Roulet, J.F.; Kaminsky, M.; Steffin, G.; Latta, M. Color stability of resin matrix restorative materials as a function of the method of light activation. Eur. J. Oral Sci. 2004, 112, 280–285. [Google Scholar] [CrossRef]
- Edelhoff, D.; Ozcan, M. To what extent does the longevity of fixed dental prostheses depend on the function of the cement? Working Group 4 materials: Cementation. Clin. Oral Implants Res. 2007, 18 (Suppl. S3), 193–204. [Google Scholar] [CrossRef]
- Oh, S.; Shin, S.M.; Kim, H.J.; Paek, J.; Kim, S.J.; Yoon, T.H.; Kim, S.Y. Influence of glass-based dental ceramic type and thickness with identical shade on the light transmittance and the degree of conversion of resin cement. Int. J. Oral Sci. 2018, 10, 5. [Google Scholar] [CrossRef]
- Passos, S.P.; Kimpara, E.T.; Bottino, M.A.; Santos, G.C., Jr.; Rizkalla, A.S. Effect of ceramic shade on the degree of conversion of a dual-cure resin cement analyzed by FTIR. Dent. Mater. 2013, 29, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Phua, E.M.J.; Waddell, J.N.; Choi, J.J.E. Curing through Ceramics: Influence of Different Light-Curing Units and Curing Modes on Bond Strength. Oral 2022, 2, 62–74. [Google Scholar] [CrossRef]
- Lee, I.B.; An, W.; Chang, J.; Um, C.M. Influence of ceramic thickness and curing mode on the polymerization shrinkage kinetics of dual-cured resin cements. Dent. Mater. 2008, 24, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Lin, H.L.; Zheng, M.; Ozcan, M.; Yu, H. Minimum Radiant Exposure and Irradiance for Triggering Adequate Polymerization of a Photo-Polymerized Resin Cement. Materials 2021, 14, 2341. [Google Scholar] [CrossRef] [PubMed]
- Kanamori, Y.; Takahashi, R.; Nikaido, T.; Bamidis, E.; Burrow, M.; Tagami, J. The effect of curing mode of a high-power LED unit on bond strengths of dualcure resin cements to dentin and CAD/CAM resin blocks. Dent. Mater. J. 2019, 38, 947–954. [Google Scholar] [CrossRef] [Green Version]
- Faria, E.S.A.L.; Pfeifer, C.S. Effectiveness of high-power LEDs to polymerize resin cements through ceramics: An in vitro study. J. Prosthet. Dent. 2017, 118, 631–636. [Google Scholar] [CrossRef]
- Shiraishi, T.; Wood, D.J.; Shinozaki, N.; Van Noort, R. Optical properties of base dentin ceramics for all-ceramic restorations. Dent. Mater. 2011, 27, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Shiraishi, T.; Watanabe, I. Thickness dependence of light transmittance, translucency and opalescence of a ceria-stabilized zirconia/alumina nanocomposite for dental applications. Dent. Mater. 2016, 32, 660–667. [Google Scholar] [CrossRef]
- Ferracane, J.L.; Greener, E.H. The effect of resin formulation on the degree of conversion and mechanical properties of dental restorative resins. J. Biomed. Mater. Res. 1986, 20, 121–131. [Google Scholar] [CrossRef]
- Dewaele, M.; Truffier-Boutry, D.; Devaux, J.; Leloup, G. Volume contraction in photocured dental resins: The shrinkage-conversion relationship revisited. Dent. Mater. 2006, 22, 359–365. [Google Scholar] [CrossRef]
- Kwaśny, M.; Bombalska, A.; Obroniecka, K. A Reliable Method of Measuring the Conversion Degrees of Methacrylate Dental Resins. Sensors 2022, 22, 2170. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, L.M.; Ramalho, I.S.; Lima, L.; Pires, L.A.; Pegoraro, T.A.; Pegoraro, L.F. Influence of the composition and shades of ceramics on light transmission and degree of conversion of dual-cured resin cements. J. Appl. Oral Sci. 2019, 27, e20180351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, C.B.; Magalhães, C.S.; Lages, F.S.; Ferreira, R.C.; Da Silva, E.H.; Da Silveira, R.R.; Corrêa, E.C.; Fantini, C.L.; Moreira, A.N. Degree of conversion and microhardness of resin cements photoactivated through glass ceramic. J. Clin. Exp. Dent. 2021, 13, e1068–e1075. [Google Scholar] [CrossRef] [PubMed]
- Jafari, Z.; Alaghehmand, H.; Samani, Y.; Mahdian, M.; Khafri, S. Light transmittance of CAD/CAM ceramics with different shades and thicknesses and microhardness of the underlying light-cured resin cement. Restor. Dent. Endod. 2018, 43, e27. [Google Scholar] [CrossRef]
- Strang, R.; Mccrosson, J.; Muirhead, G.M.; Richardson, S.A. The setting of visible-light-cured resins beneath etched porcelain veneers. Br. Dent. J. 1987, 163, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Oztürk, E.; Hickel, R.; Bolay, S.; Ilie, N. Micromechanical properties of veneer luting resins after curing through ceramics. Clin. Oral Investig. 2012, 16, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, A.; Shenoy, N. Dental ceramics: An update. J. Conserv. Dent. 2010, 13, 195–203. [Google Scholar] [CrossRef]
- Della Bona, A.; Nogueira, A.D.; Pecho, O.E. Optical properties of CAD-CAM ceramic systems. J. Dent. 2014, 42, 1202–1209. [Google Scholar] [CrossRef] [Green Version]
- Zorzin, J.; Maier, E.; Harre, S.; Fey, T.; Belli, R.; Lohbauer, U.; Petschelt, A.; Taschner, M. Bulk-fill resin composites: Polymerization properties and extended light curing. Dent. Mater. 2015, 31, 293–301. [Google Scholar] [CrossRef]
- Rizzante, F.A.P.; Locatelli, P.M.; Porto, T.S.; Borges, A.F.S.; Mondelli, R.F.L.; Ishikiriama, S.K. Physico-mechanical properties of resin cement light cured through different ceramic spacers. J. Mech. Behav. Biomed. Mater. 2018, 85, 170–174. [Google Scholar] [CrossRef]
- Sarosi, C.; Moldovan, M.; Soanca, A.; Roman, A.; Gherman, T.; Trifoi, A.; Chisnoiu, A.M.; Cuc, S.; Filip, M.; Gheorghe, G.F.; et al. Effects of Monomer Composition of Urethane Methacrylate Based Resins on the C=C Degree of Conversion, Residual Monomer Content and Mechanical Properties. Polymers 2021, 13, 4415. [Google Scholar] [CrossRef] [PubMed]
- Gaglianone, L.A.; Lima, A.F.; Araújo, L.S.; Cavalcanti, A.N.; Marchi, G.M. Influence of different shades and LED irradiance on the degree of conversion of composite resins. Braz. Oral Res. 2012, 26, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Almeida, R.; Manarte-Monteiro, P.; Domingues, J.; Falcão, C.; Herrero-Climent, M.; Ríos-Carrasco, B.; Lemos, B.F. High-Power LED Units Currently Available for Dental Resin-Based Materials-A Review. Polymers 2021, 13, 2165. [Google Scholar] [CrossRef] [PubMed]
- Bani, M.; Tirali, R.E. Effect of new light curing units on microleakage and microhardness of resin sealants. Dent. Mater. J. 2016, 35, 517–522. [Google Scholar] [CrossRef] [Green Version]
- Aguiar, F.H.; Braceiro, A.; Lima, D.A.; Ambrosano, G.M.; Lovadino, J.R. Effect of light curing modes and light curing time on the microhardness of a hybrid composite resin. J. Contemp. Dent. Pract. 2007, 8, 1–8. [Google Scholar]
- Haenel, T.; Hausnerová, B.; Steinhaus, J.; Price, R.B.; Sullivan, B.; Moeginger, B. Effect of the irradiance distribution from light curing units on the local micro-hardness of the surface of dental resins. Dent. Mater. 2015, 31, 93–104. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Experimental Groups | Low Irradiance Mode (mW/cm2) | High Irradiance Mode (mW/cm2) | |||
|---|---|---|---|---|---|
| Control | Control | 700 ± 10.00 Aa1 | Attenuation (%) | 1258 ± 8.37 Ba1 | Attenuation (%) |
| A2 | HT | 348 ± 8.37 Ab2 | 50.29 | 630 ± 7.07 Bb2 | 49.92 |
| A2 | LT | 308 ± 8.37 Ac2 | 56.00 | 468 ± 8.37 Bc2 | 62.80 |
| BL2 | HT | 408 ± 8.37 Ab3 | 41.71 | 726 ± 11.40 Bb3 | 42.29 |
| BL2 | LT | 330 ± 7.07 Ac3 | 52.86 | 588 ± 8.37 Bc3 | 53.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meng, K.; Wang, L.; Wang, J.; Yan, Z.; Zhao, B.; Li, B. Effect of Optical Properties of Lithium Disilicate Glass Ceramics and Light-Curing Protocols on the Curing Performance of Resin Cement. Coatings 2022, 12, 715. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings12060715
Meng K, Wang L, Wang J, Yan Z, Zhao B, Li B. Effect of Optical Properties of Lithium Disilicate Glass Ceramics and Light-Curing Protocols on the Curing Performance of Resin Cement. Coatings. 2022; 12(6):715. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings12060715
Chicago/Turabian StyleMeng, Kejing, Lu Wang, Jintao Wang, Zhuoqun Yan, Bin Zhao, and Bing Li. 2022. "Effect of Optical Properties of Lithium Disilicate Glass Ceramics and Light-Curing Protocols on the Curing Performance of Resin Cement" Coatings 12, no. 6: 715. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings12060715