
Enhancing Skin Anti-Aging through Healthy Lifestyle Factors
1
Global Research and Development, Nu Skin Enterprises, Provo, UT 84601, USA
2
Department of Cell Biology, Physiology and The Neuroscience Center, College of Life Sciences, Brigham Young University, Provo, UT 84602, USA
*
Author to whom correspondence should be addressed.
Cosmetics 2023, 10(5), 142; https://0-doi-org.brum.beds.ac.uk/10.3390/cosmetics10050142
Submission received: 29 August 2023
/
Revised: 19 September 2023
/
Accepted: 2 October 2023
/
Published: 12 October 2023
(This article belongs to the Collection Feature Papers in Cosmetics in 2023)
Abstract
:Lifestyle health has been recognized as an evidence-based innovation that defines how everyday behaviors and routines influence the avoidance and therapy of illness and provides an important adjunctive component to overall health. Specifically, an approach with small changes over time can have a dramatic impact on the health and well-being of individuals not only, in general, but also can be applied to skin health. However, lifestyle health factors to improve skin well-being have not been discussed extensively and/or well promulgated. The narrative for this overview focuses on providing a summary for topic background information, but more importantly, presents four lifestyle factors that can improve dermal health [i.e., factor 1: nutrition—diet; factor 2: rest (sleep); factor 3: movement/physical exercise, and factor 4: social and community associations]. This was accomplished by identifying preceding journal reports/reviews covering especially the last five years (January 2018 to July 2023; 164 out of 205 references cited or 80%) using scientific search databases. The main conclusions of this overview encourage the concept that lifestyle health factors such as nutrition/diet, rest/sleep, movement/physical exercise, and community/social interactions support enhanced skin health and well-being with aging. Plus, social media interventions that aim to promote dietary, sleep and physical activity changes might be an application to improve skin health in the future.
Keywords:
skin; anti-aging; health; lifestyle factors; diet; sleep; exercise; social interactions; polyphenols; vitamins1. Introduction
Everyone ages, the skin (being the largest organ of the body) is the most conspicuous visual indicator of aging, especially in the facial/neck and hand/arm/leg regions [1,2,3]. However, habits and actions (that may be positive or negative) have profound influences on short-term and long-term health and quality of life (QOL) [4,5]. This perspective is supported by numerous scientific studies and evidence-based guidelines for the prevention and/or treatment of age-related diseases [4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21]. For example, many studies have examined factors such as: (a) good nutrition via dietary choices [4,5,6,7,8,9,10], (b) regular rest with good sleep cycles for restoration and managing stressors [4,5,7,8,9,10,13,14,21], (c) physical activity including moderate to vigorous exercise to enhance cardiovascular health and to manage/control body weight [4,5,7,9,10,15,16,17,21], and (d) the importance of positive social relationships to stay mentally/emotionally connected with community associations with ideals engaged in worthy activities among like-mined people [4,5,10,12,14,16,18,19,20,21].
The concept of lifestyle choices was first proposed in 1999 by James Rippe in the textbook “Lifestyle Medicine”, which defined how daily habits and practices impact both the prevention and treatment of disease and provides an important adjunctive component to overall health [21]. In fact, a recent report presented at the annual meeting of the American Society of Nutrition 2023 looked at the lifestyle behaviors of nearly 720,000 military veterans between the ages of 40 to 99 years of age in the “Million Veteran Program”, a longitudinal study designed to investigate the health and wellness of United States (US) veterans [21]. The investigators found that lifestyle habits (like the list of factors outlined above) build on each other and could add up to 24 years of life extension, enhancing longevity and the QOL [21].
While healthy lifestyle factors have been examined for the prevention and/or treatment of age-related disease, this paradigm has been lacking for skin aging. Thus, this narrative overview examines the latest existing knowledge about how lifestyle factors influence skin aging, and how different modalities of daily habits and choices coalesce to advance/build various components to boost skin anti-aging toward better overall health. Specifically, the purpose of this review is not to present comprehensive coverage, but to provide an updated general summary on: (a) aging, (b) skin aging, and the four factors that can influence skin aging such as (1) nutrition and dietary selections, (2) rest (sleep), relaxation/recovery/rejuvenation and protection against stressors, (3) movement (exercise- moderate to vigorous levels to improve cardiovascular, weight control and well-being), and (4) community (covering social and community associations) to “become” better in managing the challenges of aging. This overview identified previous journal articles and reviews (with emphasis over the past five years) from January 2018 through July 2023 using the keywords: lifestyle health/medicine, skin, dermal, human and/or using different keyword combinations (retrieved from 1 July to 10 August 2023). The following databases were utilized: PubMed maintained by the US National Library of Medicine at the National Institutes of Health; Science Direct and Scopus by Elsevier and from Google Scholar. Also, background references (where appropriate) include the keywords: lifestyle health/medicine, diet, sleep, isolation, exercise, estrogens, skin aging, microbiome, phytoestrogens, phytochemicals, polyphenols, and/or combinations (without a year-limit range for searching the background topics). This overview is based on previously conducted studies and does not contain new data/results of human participants or animals performed by the authors.
2. Skin Aging
2.1. Skin
Of all the organs, the skin is the most conspicuous to display signs of aging or dermal changes [1,2,3]. Skin covers an area of around 2 m2 (however, more recent estimates accounting for dermal pores suggests 25 m2) and represents one-sixth of the total weight for an adult [2,3,22,23]. The skin serves a variety of functions such as acting as the body’s initial barrier protecting against foreign agents (pathogens), ultraviolet (UV) light, chemicals, mechanical or other injury, and it helps to maintain body temperature, prevent water loss from the body, produce vitamin D, detect/fight infections, and provides sensory information (touch, pressure, temperature, and pain-nociception) [2,3,22,23]. Trans-epidermal water loss (TEWL) has been determined to range from 120 to 240 g/m2/day, which is important for skin hydration [24,25].
There are seven skin layers, which are displayed in Figure 1. In summary, the epidermis is the major outer layer with keratinocytes as the major cell type (at 75–125 microns thick). The epidermis is further stratified into 5 distinct layers.
The first skin layer is the stratum corneum- keratinocytes become corneocytes, which are strong (dead keratinocytes) that provide barrier protection and prevents TEWL [2,3,22,23,24,25]. The water content of the stratum corneum (about 20–30%) is part of the natural moisturizing factor (NMF) array that maintains adequate skin hydration [2,3,22,23].
The stratum lucidum, the second skin layer is a thin, transparent layer of keratinocytes only found on the palms of the hands and soles of the feet [3,22].
The third layer- the stratum granulosum- contains glycolipids (keratohyalin granules) that keeps the skin layer together (these are filled with histidine and cysteine rich proteins to bind the keratin filaments together), along with desmosomal connections that help form a waterproof barrier [3,22,23,26] (see Figure 1).
The stratum spinosum, the fourth layer is 8 to 10 cells thick held together by sticky proteins called desmosomes, helping the skin be flexible and strong along with an abundant number of dendritic cells (Langerhans cells) for immune defense [3,22,23,27].
The fifth skin layer is the stratum basal- this is a single row of stem cells, continually producing keratocytes, and contains melanocytes (10–25% of the cells herein) [responsible for melanin pigment] [2,3,22,23].
The dermis represents the sixth layer comprised of collagen and elastin fibers, which are secreted by fibroblasts providing the structural components for flexibility and strength [1,2,3,22,23,28].
The dermis is composed of two regions or zones, the papillary dermis (that has fewer structural fibers and contains vascular networks that serve two functions-support the avascular epidermis with vital nutrients and thermoregulation) and the reticular dermis (that contains dense structural fibers, which provides the skin with overall strength and elasticity) [2,3,22,23] (see Figure 1).
2.2. Skin: Chronological Aging and Photoaging Aging
Skin aging is a complex process due to chronological (intrinsic) and photoaging (extrinsic) mechanisms that have been reviewed elsewhere, but will be covered herein, in brief [1,2,3,29,30,31,32,33,34,35].
2.2.1. Extrinsic Skin Aging
Extrinsic aging is an important collateral factor in cosmesis, appearance, diagnosis, and management of the skin in aging individuals, which is due mainly to the chronic exposure to various environmental elements such as the sun (UV light including tanning bed), air/water pollution, smoking (vaping), diet/exercise/stress, lifestyle, repetitive muscle contractions (smiling, frowning, etc.), gravity, sleeping positions and cutaneous or general diseases/disorders [2,7,29,31,34,35]. However, the main environmental element associated with extrinsic aging is photo-aging (exposure to UV light) resulting in a cascade of cellular and molecular signaling mechanisms that increase oxidative stress and inflammation [2,29,31,35,36]. These extrinsic aging factors may be independent of hormonal status and should be considered in the clinical management of aging skin [2,29,31,35,36].
2.2.2. Intrinsic Skin Aging
Intrinsic or chronological aging is a natural process caused by the accumulation of reactive oxygen species (ROS) resulting from oxidative cellular metabolism [36] and is influenced by genetics, metabolism, hormonal, immunological, cardiovascular, gastrointestinal, psychogenic (involving stress or affective disorders), degenerative, or neoplastic disease [2,29,35,36].
In women, the skin thickens to 25 to 30 years of age, then there is a progressive declination of all skin layers during aging [2,29,30,35,36]. Chronological or intrinsic aging is an inevitable biological process where deteriorating alterations in the production, quantity, and preservation of dermal cellular/protein elements takes place [2,29,32,35,36]. Throughout dermal aging, keratinocytes change shape, and the epidermal-dermal junction (rete pegs) becomes compressed, while there is a decline in the dermis thickness because of the deficit of collagen, elastin, and hyaluronic acid (elastosis). It is more noticeable in sun-exposed areas (solar elastosis) [2,29,32,36,37]. Skin turgor declines along with the increased appearance of fine lines/wrinkles, especially along normal areas of stress, gravity, and mechanical muscle contractions especially around the eyes and mouth [2,29,32,36]. Matrix metalloproteinases (MMPs) cause destruction of collagen and elastin fibers that in turn enhance mitochondrial oxidative stress and deletions of mitochondrial DNA via the c-Jun/AP-1 pathway in dermal fibroblasts [29,30,31,32] (see Figure 2).
Finally, blood vessels in the dermis become more fragile, leading to bruising (senile purpura), sebaceous glands produce less oil, sweat glands produce less sweat (challenging to keep cool), less subcutaneous fat layer reduces the ability to maintain body temperature and skin tags, pigmented spots (liver spots/lentigos) can appear with aging [2,29,31,33,36].
2.3. Hormonal Benefits/Changes with Aging (Estrogen in Women)
17β-Estradiol has numerous cutaneous benefits that are detailed elsewhere [2,38,39]. Recall 17β-estradiol is the most potent sex steroid hormone in humans and the major estrogen produced by the ovaries during the reproductive years [2,39,40]. 17β-Estradiol levels reach a maximum around the mid to late 20 s [2,39,40]. Interestingly, the levels of skin collagen and elastin also follow the estrogen profile during this interval. [2,38,39,40,41,42] (see Figure 3A,B). Around 30–35 years of age, estrogen levels begin to decline, and there are corresponding changes in the skin; wrinkles appear because of the declination in collagen and elastin fibers in the dermal layer (Figure 3A) [2,38,39,40,41,42,43].
17β-Estradiol production from the ovarian follicles declines after 35 years of age, and there is a progressive declination in estrogen levels by around 45 years [2]. Then there begins to be inconsistent oscillations in ovarian estrogen production as the follicles respond to gonadotrophins waves until they become exhausted with the onset of menopause (in the USA this milestone is around 51 years of age ± 4 years) [38,39,41,43] (Figure 3B). After menopause, estrogen production occurs not in the ovaries but at peripheral adipose tissue sites [36,38,39,43]. While it is known that skin cells can produce estrogens locally, the aromatase enzyme activity is dramatically reduced to approximately 30-times lower than in premenopausal ovarian follicular tissue [39,44]. Also, it should be noted that androgens have a negative influence on skin cells especially on collagen and elastin via the 5α-reductase type I enzyme located in fibroblasts. This enzyme can counteract the positive estrogenic influence, especially after menopause [2,38,39,43]. The lack of estradiol and/or agonist influences by selective estrogen receptor modulators (SERMs) actions, especially via ERβ activation, has been shown to account for the vivid loss in dermal fibers such as collagen and elastin causing atrophy, wrinkles, poor wound healing/barrier function/hydration [2,38,39,43,45] (Figure 3A) The declination of skin components is heightened by intrinsic and extrinsic aging, which are reviewed elsewhere [2,29,36,38].
Estrogens send their chemical hormonal messages via estrogen receptors (ER) throughout the body. Notably, it has been reported that there is specific-tissue regulation of how ERs are synthesized in humans; also, it is known that ER beta is more abundant in the epidermis and fibroblasts (and in the scalp region) compared to ER alpha [2,38,46]. In fact, ER beta activation has been shown to promote wound healing and cellular/tissue restoration in human skin via dermal structures such as collagen and elastin that occur via biomechanical processes [2,36,38,39,47,48,49]. Plus, ERβ agonists via SERM actions are known to provide similar positive actions on skin health compared to 17β-estradiol, which are seen in plant-derived molecules such as polyphenols (resveratrol, flavonoids and isoflavonoids, etc.) or phytoestrogens that selectively bind/activate ERβ in human skin [2,36,38,39,49,50]. Finally, the effects and benefits of 17β-estradiol on skin are shown in Figure 4.
2.4. Other Hormonal Influences on Skin
While 17β-estradiol is the most potent steroid hormone in the body, the skin is an endocrine organ that contains the biochemical enzymes for local hormone production to influence regional immune function [50,51]. Conversely, there are several hormones produced by the endocrine system from glands that secrete chemical messengers into the bloodstream that bind specific receptors in cells/tissues to maintain homeostasis, but other hormones are also known to influence the skin [36,50,52,53,54,55]. In addition to estrogens, androgens, cortisol (the stress hormone), progesterone and thyroid hormone are known to influence skin health (see Figure 5). Androgens along with cortisol are known to have a negative impact on skin where they decrease collagen and elastin, skin turgor, wound healing, and fibroblast viability, but increase MMPs, wrinkle formation and sebum production [2,36,38,39,54,55] (Figure 5). Progesterone like estrogens has positive influences on skin except that it stimulates sebum production [56,57,58]. Finally, thyroid hormone regulates the metabolic rate of the body and helps regulate epidermal cell proliferation, differentiation, hair and nail growth, wound healing, and skin hydration by affecting the function of dermal fibroblasts [50,52,53]. Thus, while estrogens play a leading role in skin, other hormones also have a significant influence on dermal health (Figure 5).
3. Health Lifestyle Factors
3.1. Aging
Various health and governmental agencies worldwide devote a broad scientific effort to understand the nature of aging and to extend healthy active years that enhance the quality of life (QOL). Aging has many aspects, but in general, it is defined as the gradual physical, psychological, and social changes in persons that lead to increased risk of weakness, disease, and ultimately death [59].
3.2. Population Aging around the World
The United Nations department of economic and social affairs announced on 20 February 2023, that “population aging is a defining global trend of our time” [60]. Where Asia is at the forefront of this trend with Hong Kong, South Korea, and Japan predicted to have the highest share of people aged 65 and older by 2050 [60] (see Figure 6).
3.3. Aging Related-Disorders
From a more biological perspective, aging is the progressive physiological changes in an organism that lead to senescence [40,61,62,63]. Or, in other words, a decline of biological functions and the lack of an organism’s ability to maintain homeostasis and adapt to various stressors (such as age-related disorders of the body’s organs/systems/tissues/cells involved in the operational aspects of metabolism/defense and unregulated growth like cancer) [40,61,62,63]. The nine hallmarks of aging have been reviewed elsewhere [40,61,62,63] that cover (1) gene variability, (2) shortening of telomers, (3) epigenetic factors, (4) protein instability or weakening of large molecules, (5) lack of detecting nutrient and metabolic communications, (6) cellular apoptosis, (7) fatigue/collapse of stem cells, (8) mitochondrial trauma/abnormality/impairment, and (9) breakdown of signaling between cells [40,61,62,63]. However, other investigators have proposed that the major cause of aging and age-related disorders is due to oxidative stress at the molecular level [62].
3.4. Aging and the Global Burden of Cancer Attributable to Lifestyle Risk Factors
Cancer is the second leading cause of death worldwide, and exposure to risk factors plays an important role in the burden of many cancer types [64,65]. Also, it is well established that cancer is more common as people age [64]. To gain a perspective on the magnitude and importance of lifestyle factors a recent study published in the Lancet 2022 analyzed 369 causes of death and disability along with 87 risk factors from 204 countries and territories on the global burden of cancer. In 2019, the top risk factors were (1) smoking (vaping), (2) alcohol use, (3) high body-mass index, (4) unsafe sex, (5) high fasting plasma glucose levels, (6) ambient particulate matter pollution, (7) occupational exposure to asbestos, (8) dietary intake low in whole grains, (9) dietary intake low in milk, (10) second-hand smoke, and (11) dietary intake low in fruits [65]. Remarkably, overall, 44 % of the cancer deaths were due to modifiable risk factors where behavioral and dietary/metabolic risk factors had the highest rates (that accounted for the most cancer deaths), while exposure to pollution represented moderate rates of cancer deaths [65].
In 2011, Alegria-Torres et al. published a landmark review on epigenetics and lifestyle, which predicted and supports the 2022 Lancet study on the global burden of cancer [66]. Notably, Alegria-Torres outlined environmental and lifestyle factors such as diet/nutrition, behavior (physical activity, sleep, working habits, stress, etc.), and smoking (vaping), and alcohol consumption that affects human health [66].
4. Factors of Lifestyle Health
Different Types of Lifestyle Health
Different lifestyle aspects leading to healthy outcomes have been reported from multiple perspectives. Kassis et al. (2023), reported how aging impacts five key biological functions (immune, digestive, nervous, musculoskeletal, and cardiovascular) with preventive strategies that focused on dietary intake, physical activity, and sleep quality [67]. Loef et al. (2023), found in a 30-year study that predictors of healthy aging suggested that long-term cardio- and metabolic parameters such as overweight and cholesterol levels were the most significant factors in predicting healthy physiological aging [68]. In 2019, Bosnes et al. examined lifestyle predictors of positive aging in a 20-year prospective study that found among the midlife variables (smoking, physical activity, alcohol consumption, obesity, and social support) that non-smoking and social support were the most significant predictors of successful aging [69]. When modification of lifestyles was studied in older age (40–80 years) individuals, Katz and Sakaniwa et al. found that adopting healthy lifestyles was correlated with lifetime benefits among subjects even with major co-morbidities (e.g., cardiovascular disorders, cancer, diabetes, and kidney disease) [70,71]. Furthermore, Wahl et al. reported in humans the intake of the Mediterranean, Finnish, and Okinawan diets were associated with improved age-related health variables and suggested that neurodegenerative disease including dementia could be ameliorated [72]. Finally, Buettner and Skemp, in 2016, reported the discovery of 5 places around the world where people consistently live over 100 years old [73]. The common factors among the 5 locations among the world’s centenarians include: (1) movement, (2) purpose in life, (3) managing stressors in life, (4) controlled decreased volume of dietary intake of plant-based foods, and (5) belonging to and interacting within a social community with strong relationships [73].
5. Four Factors of Lifestyle Health
5.1. Factor 1: Lifestyle Health—Nutrition, Diet and Skin Health
The purpose of this section and later sections is not to present comprehensive coverage on various aspects of lifestyle/habits and factors, but to summarize the recent progress reported in the scientific literature and how this applies to skin health and anti-aging.
5.2. Nutrition-Diet Lifestyle Benefits
Eating is directly associated with health. Good nutrition is essential to keeping current and future generations healthy across the lifespan [74]. A healthy diet helps children grow and develop properly and reduces their risk of chronic diseases. Adults who consume a healthy diet live longer and have a lower risk of disorders and certain cancers [30]. Additionally, healthy eating can help people with chronic diseases manage these conditions and avoid complications [59]. In other words, nutrition plays a key role in lifestyle habits and practices that impact virtually every chronic disease [4], and there is strong evidence for the role of nutrition in cardiovascular disease, diabetes, obesity, and certain cancers, among many other disorders [5,66]. For example, in 2022, La Vignera and Basile presented a report entitled “Diet and prostate health: an underrated tool?”, which described how dietary changes can notably impact prostate health and improve the benefit of traditional medical care (as reviewed by Stewart and Lephart, 2023) [75].
While diet has become a focus to enhance human health, the attention on what types of diets yield the best outcomes is paramount from the perspective of consumers. The “Mediterranean or Eastern” diets versus a “Western diet” have gained popularity to increase the general health status and well-being and address many diseases and disorders [8,66,76,77,78,79,80] (Figure 7). For example, the Mediterranean diet is one of the most widely described and evaluated dietary patterns in the scientific literature with validated health benefits [8,76,77,79,80]. It is characterized by high intakes of vegetables, legumes, fruits, nuts, whole grains, fish, some olive oil, moderate intake of red wine, where most proteins and fats are derived from vegetable sources with low intake of red meat, potatoes, processed meat, refined carbohydrates, and sweets [77,79,80]. Additionally, the Eastern (Asian) diet has high intake of plant-based foods (source of protein from vegetables like bean sprouts, spinach, eggplant, bok choy, cabbage, kale, snow peas, leeks, and mushrooms). Fruits and legumes, grapes, melons, cherries, dates, mangoes, etc.; steamed or stir-fried produce along with nuts, seeds, beans (soy, mung), lentils, tofu, or tempeh, plus rice and whole grains. Moderate intake of fish (dependent upon country’s coastline), dairy, eggs, and poultry. Very low intake of meat, processed meat, refined carbohydrates, and sweets [8,76,77]. Conversely, the Western diet, prevalent in high-income countries, contains refined carbohydrates, red meat, processed meats, fats/lipids/cholesterol, which increase sympathetic nervous system, oxidative stress, and inflammation and low intake of fruits and vegetables [75,76,77] (Figure 7). Additionally, a traditional Eastern European diet (in Russia, Poland, and the Czech Republic) may contribute to poor health status, particularly for the high cardiovascular disease rates reported by Stefler et al. in 2021 [81]. Notably, Europe and Central Asian (from the Caspian Sea in the west to Western China and Mongolia) are regions, where cardiovascular disease is responsible for more than half of all deaths across this area due to poor diets and daily habits (smoking) [82].
5.3. Nutrition, Diet and Skin Health
A reasonable balanced diet provides the nutritional components to delay aging, prolong life and enhance the QOL [4,8,34]. This narrative overview for this section demonstrates that a healthy diet is one of the most important factors to achieving healthy skin [8,34,76,83]. Certain nutrients, vitamins, minerals and other compounds/molecules and factors will be described herein, previous journal reports have presented more detailed information elsewhere as cited.
Various nutritional elements such as water, protein, trace elements (iron, iodine, zinc, copper, selenium, etc.), vitamins (A, B complex, C, D, and E) other dietary, daily habits and lifestyle heath choices are known to impact skin health.
For example, does dietary fluid intake affect skin hydration? The answer is basic and complex due to the nature and importance of water in the human body for normal physiological function, maintaining body volume (intracellular and extracellular), thermoregulation, and acting as a lubricant and shock absorbent [84,85]. It is also important in the character/composition of the avascular epidermis [2,22]. Drinking enough water is important to your overall health and to your skin (most individuals do not drink 8 to 10 glasses of water per day); however, it’s not clear whether drinking extra water affects skin hydration in healthy people [86]. Your skin is also affected by your diet, lifestyle, environment, and skin care routine [84]. However, in the case of the elderly or in obesity, dry skin is a common complaint [84]. Higher water intake in a regular dietary routine might positively impact skin physiology especially for its hydration and biomechanical properties, particularly in individuals with lower daily water consumption [84].
What about dietary protein intake? Protein is a critical nutrient for human growth, development, maintenance, and repair of body tissues/cells, which perform a large array of functions (as enzymes, structural components, transport/signaling, hormones, proper fluid, and acid-base balance, immune, and DNA replication) [87]. It is no surprise that protein intake is essential for healthy skin, particularly the two amino acids, i.e., lysine and proline that support collagen composition [88,89]. Notably, collagen is the most abundant protein in the body [88]. Protein deficiency in developed countries is rare, however, low-protein diets are associated with poor wound-healing and other skin problems, especially with aging [34]. Finally, oral intake of collagen supplements has been reported to enhance skin, nail, and hair health [88,90,91,92].
Vitamins in both topical and oral forms play a key role in many dermatological conditions [89,93]. Vitamin deficiencies can occur. Deficiencies of water-soluble vitamins, such as most B vitamins and vitamin C, may develop after weeks to months of under-nutrition, while deficiencies of fat-soluble vitamins, such as vitamins A, D, E and B12, can take up to a year to develop due to the body storage capacity for these nutrients [89,93]. Numerous reports suggest that oral supplementation of various vitamins can enhance general skin health and treat dermatological disorders [89,93,94,95]. In general, vitamins can have anti-aging effects such as [88,89,93,94,95], antioxidant, anti-inflammatory, hydration, skin barrier, turgor/tone/radiant, and repair/wound healing properties that are beneficial for skin health.
In fact, feeding the skin is a new trend in food and cosmetic treatments, where beauty is no longer dissociated from well-being, and where consumers consider nutrition as an important pillar in skin health. This is especially the case when ingredients/products contain food extracts or natural plant sources having nutricosmetic and/or nutraceutical benefits. [35,50,94,95].
Lifestyle health routines of dietary intake of plant-derived compounds such as carotenoids (astaxanthin, lutein, zeaxanthin, lycopene), chlorophyll, and polyphenols (resveratrol, flavonoids, isoflavonoids, green tea, etc.) have been shown to benefit skin health in a variety of ways [50,88,94,95] such as decreasing fine lines/wrinkles, dullness and roughness while enhancing healing, hydration, pigmentation, and radiance [36,50,88,94,95,96,97,98,99,100,101]. The mechanisms by which plant-derived compounds enhance skin health include: anti-aging (sirtuin activation), protection against UV damage, direct antioxidant actions and/or stimulation of nuclear factor erythroid 2-related factor (Nrf2) that is the master regulator for antioxidant responses, anti-inflammatory [by blocking nuclear factor-kB (NFkappB) and activator protein 1 (AP1), interleukins and oxidative stress], stimulation of collagen, elastin, tissue-inhibitor of matrix metalloproteinase(s) (TIMPs) and superoxide dismutase (SOD), blocking androgen hormone action and enhancing skin parameters (hydration, smoothness, radiance, pore size, firmness, and frown lines/wrinkles) [2,8,23,35,36,38,43,47,49,76,79,83,95,96,97,98,99,100,101,102,103].
Interestingly, chlorophyll, the most abundant plant pigment responsible for giving plants their green color, also blocks assaults to DNA from carcinogens, and chlorophyllin is a water-soluble derivative of chlorophyll [102]. Finally, chlorophyll also plays a role in regenerating Co-enzyme Q 10 (CoQ10) [102], where CoQ10 as an oxidant has been shown to: (a) reduce the production of free radicals, (b) be involved in the regeneration of vitamin E, (c) reduce keratinocyte DNA damage, (d) reduce UVA-induced MMP production from fibroblasts, (e) enhance collagen and elastin expression, inhibit IL-1alpha, IL-6 production, and melanin synthesis, and (f) inhibit MMPs and regulate the sulfide oxidation pathway [88].
Probiotics are active microorganisms that have beneficial effects on the host by altering the microbiota composition of a specific portion of the host’s flora [104]. Numerous studies have found a close relationship between the skin microbiome and skin health benefits along with the gut-skin axis, where the gut microbiome can influence the skin via various chemical messengers including hormone and immune signaling [23,104,105]. Several skin-related topics (acne, antioxidant activity, atopic dermatitis, barrier function, enzymatic regulation of the extracellular matrix, moisturization, photo-aging, pigmentation, rosacea, TEWL, suppression of pathogens, and UV protection, etc.) have been covered in diverse reviews on topical and oral probiotics in skin health [104,105,106,107,108,109]. Therefore, it is beyond the scope of this narrative overview to describe this topic further.
Diet lifestyle factors such as the role of whole-food, plant-based (WFPB) diet on skin health parameters was reported by Solway et al. in 2020 [102]. This WFPB diet was defined as “eating plant foods in their whole, unprocessed form, such as vegetables, fruits, beans, lentils, nuts, seeds, whole grains, and small amounts of healthy fats. It did not include animal products, such as red meat, poultry, fish, dairy, eggs or processed foods or sweets” [102]. Their findings showed that a WFPB diet maximized the antioxidant potential by providing the essential vitamins (A, C, and E) to help combat oxidative stress, advanced glycation end products (AGEs) and methylglyoxal [110,111,112,113], which resulted in lengthening telomeres that contributed to healthier, younger-looking skin [102]. The findings by Solway et al. are supported by numerous other scientific reports that have examined different aspects of diet/lifestyle health and skin parameters [3,34,42,83,95,108,114,115,116,117].
From a clinical perspective, there are some reports that investigated the role of lifestyle and nutrition (especially vitamins, minerals, and dietary supplementation) on dermatological conditions such as photo-aging, psoriasis, acne vulgaris, atopic dermatitis, rosacea, and hidradenitis suppurativa, etc. [118,119,120,121].
5.4. Lifestyle/Daily Habits- Negative Impact on Skin Health [AGEs, Alcohol, Smoking, High Fat, Body Mass Index (BMI)]
Advanced glycation end products (AGEs) are well studied toxins, where glycation is a non-enzymatic chemical process that involves the formation of a covalent bond between a sugar molecule (e.g., glucose or fructose) and a protein or lipid [110,111,112]. This differs from physiologic glycation that is under enzymatic control [102]. AGEs can accumulate within tissues/organs to disrupt structures and function, but in the skin, it causes alterations in collagen, elastin, vitronectin and laminin structures, delayed wound healing and declination of skin strength and flexibility [114,115]. Remarkably, external factors such UV irradiation, cigarette smoking, poor dietary choices (Western diets), alcohol, obesity, and cooking methods can increase the rate or abundance of AGEs, whereas whole-food plant-based (WFPD), Mediterranean or Eastern diets contain the least number of AGEs [102,122,123,124].
Alcohol consumption (two drinks per day) and smoking have damaging influences on skin health [115,116,125]. Alcohol’s two major effects on skin: (a) dehydration (diuretic water loss along with decline in vitamins and minerals) and (b) inflammation (increased oxidative stress along with peripheral vasodilation), which can impair quality of sleep, skin cell turnover and alter carotenoid concentrations to lessen antioxidant defense [115,116,125].
The are zero health benefits associated with smoking [125,126]. Smoking’s detrimental influence on skin is dependent upon history and level of use, which causes severe signs of aging (loss of skin tone/turgor and appearance of lines/wrinkles) [125]. Even in individuals with the shortest smoking history, facial and perceived age was advanced compared to their chronological age, especially in the facial region around the mouth and eyes [125]. Unfortunately, smoking and vaping have similar harmful influences on skin health [126], and a growing body of research has found that e-cigarettes (vaping), like regular cigarettes, results in serious respiratory disorders especially in youth and young adults [127].
Astonishingly, Gunn et al., in 2016, conducted a twin study entitled “Mortality is Written on the Face”, where nurses rated the perceived age of each twin from photographs and selected which twin had survived the other twin. The conclusions of study suggested that facial cues are the most important in linking perceived age and survival [128]. Notably, for women there is a strong link between estrogen levels with aging, attractiveness, facial appearance, and coloration, which are negatively influenced by alcohol and smoking [39,129,130].
High fat dietary intake and obesity (body mass index; BMI > 30) have been linked in reference to lifestyle health, an extensive range of chronic diseases, including dermal disorders [83,131,132,133,134]. In brief, obesity is now considered to be a global epidemic and is increasing in prevalence (by 2035 more than 50% of the world’s population will be obese) [132,133]. In general, the effect of a high-fat diet results in aging of the skin by inflammatory damage [83]. Almost 60–70 percent of obese patients present with a variety of skin disorders, such as eczema, psoriasis, atopic dermatitis, infections, poor wound healing, and other skin malignancies like melanoma [134,135]. Specifically, obesity is one of the important casual factors of many inflammatory diseases [136,137]. In the skin, functional changes in adipocytes, lymphatic vessels and epidermal keratinocytes are involved in obesity-induced exacerbation of skin inflammation [135,136,137]. Particularly, skin barrier health is directly related to the changes that occur in the composition and function of dermal immune cells that decline with aging [138,139]. Therefore, the profound impact of increased fat deposition and obesity on cutaneous immunology and its role in the pathophysiology of various chronic inflammatory dermatological conditions is without question [134,135,136,137,138,139]. However, semaglutide, a glucagon-like peptide 1 (GLP-1) receptor agonist, approved for the treatment of type 2 diabetes mellitus (T2DM) and more recently utilized for weight loss in overweight/obese individuals, has been shown to be highly effective against severe psoriasis in T2DM patients [140,141]. Thus, the importance of lifestyle health factors that may ameliorate the harmful influences of obesity and overweight conditions warrants further research and development of aids and treatments not only for the range of chronic diseases but to improve skin health [134].
Finally, all nutrients, dietary supplement ingredients or daily habits covered in the section above are summarized in Table 1 that display the various influences on the skin along with the cited reference(s).
6. Factor 2: Lifestyle Health—Rest, Relax, Recover (RRR) and Manage Stressors
Another important lifestyle health factor is rest, and the most important aspect of rest is sleep, which is essential for health and well-being [142,143,144]. Sleep is a fundamental physiological need to which humans devote approximately one-third of their lives. Sleep duration and quality of the sleep cycle determine health outcomes, because without this critical rest interval the body’s cells/tissues/organs, etc. and functions are adversely affected [142,143,144].
Each sleep cycle begins with non-REM sleep (for memory consolidation), while REM sleep is critical for processing sensory impressions and each cycle lasts between 70–100 min with an average of four to six cycles per night [142,143]. The sleep interval in healthy people decreases with aging, where newborns need 14–17 h of sleep per day, while adults sleep 7–9 h [142,143]. Less than 7 h of sleep is associated with poor health and decreased well-being [142,143,144].
For example, the function of sleep has many components which include: (a) reduction in energy consumption, body temperature, blood sugar, helps to control body weight and strengthens your heart, (b) immune cell production, restores defense mechanisms, decreases inflammation/stress and repairs cells/tissues, (c) removal of toxins from the brain (produced by cellular respiration) by increased blood flow to this organ, and increases memory consolidation/formation, (d) boosting mechanical/hormonal balance, executive functions, performing tasks on vigilance, motor speed, and post-exercise recovery [142,143,144].
It is estimated between 37 to 43 percent of the general population have sleep problems that contribute to a variety of mental and physical health disorders [142,144,145]. One of the potential integrative treatments for sleep disturbance is lifestyle health interventions because the encouragement is to make small changes in one’s routine that can have a large impact long-term for many disorders including skin health [1,33,142,145].
What are the factors that enhance sleep disturbance or improve the quality of sleep? First, a general list of factors that can impact sleep quality include a) diet (fats, protein, and carbohydrates), while caffeine, low vitamin D levels, alcohol, nicotine, enhanced calorie intake and obesity impair sleep quality [142,145,146,147,148,149,150,151,152,153,154,155,156,157]. Whereas a balanced diet with adequate vitamin intake and regular physical activity provides weight loss, enhanced melatonin levels, memory consolidation and improved quality of sleep [142,145,146,147,148,149,150,151,152,153,154,155,156,157] (Table 2). Assuredly, there are many other factors that influence sleep, but such coverage would be beyond the scope of this overview.
6.1. Sleep and Skin Health
Sleep is vital for health and healing because it has a bidirectional impact: poor sleep increases the risk of disease and illness as well as the converse, disease, illness, and other factors disrupt sleep [158]. The concept of lifestyle health where diet and exercise are beneficial, however, when individuals are fatigued and not mentally focused this lifestyle plan is unlikely to succeed. Sleep is vital in regulating skin physiology such as the skin surface pH, TEWL, blood flow and skin temperature [158,159]. For example, in reference to skin health a clinical study of post-menopausal women showed that those who slept less than five hours per day had higher TEWL loss, decreased skin barrier function and longer recovery after UV-induced erythema [159]. Even after a single night of disrupted sleep, periocular areas are known to show dark circles giving a tired appearance [160]. Sleep impairment is associated with chronic inflammatory skin conditions such as atopic dermatitis, eczema, psoriasis, rosacea [161,162,163,164,165]. In this regard, sleep deprivation is known to increase cortisol levels that suppress the immune response along with impairment of T cell function and antigen presentation that result in increased infections. Additionally, sleep loss has been shown to increase proinflammatory cytokines that further increase inflammatory skin disorders like psoriasis and eczema [163]. Finally, isotretinoin, a drug widely used in dermatology to treat acne, had been found to cause sleep disturbances [163].
6.2. Skin Health and Circadian Factors
Organisms have conserved over millennium an internal rhythm that helps them anticipate (to changes in radiation, temperature, and food availability) and adapt to daily changes in the environment [166]. Light synchronizes this internal circadian clock, when photons processed by the retina send neural information to a part of the brain called the suprachiasmatic nucleus (SCN) in the anterior hypothalamus [165]. Other factors (food intake, exercise, temperature, aging, trauma/injury, etc.) also affect “clocks” in peripheral tissues, including the skin [166,167,168]. The communications between the central SCN clock and the skin clock(s) coordinate various functions (i.e., homeostasis, proliferation/repair, immune and stress responses) [166,167,168], Notably, the circadian skin clock(s) in the epidermis, dermis and hypodermis can be altered/disrupted by sunburn (UV-induced erythema), aging, infections, hydration, inflammatory dermal disorders, food intake, sleep, and injury/wound healing [166,167,168,169,170,171,172]. The biological rhythms in the skin and skin clock genes have been reviewed in detail elsewhere [166,168,169,170]. However, the fluctuation in human skin characteristics as they cycle through the day and night (as regulated by skin clock genes) is shown in Figure 8. For example, in the epidermis, cellular proliferation in keratinocytes is 30-fold higher at night than at noon (12 PM) and epidermal stem cells show a similar pattern and have a higher rate of proliferation at night versus day [169]. Also, the circadian rhythms via modulation associated with skin clock genes altered aquaporin 3 (AQP3) expression impacting skin hydration [167]. Interestingly, it was shown that UV exposure, aging, and low temperature resulted in increased TEWL, while vitamin C, collagen and probiotics increased ceramide production and improved skin hydration [167]. Finally, understanding the role of circadian clock genes in the skin will provide new insights to the pathogenesis of skin disorders and novel aids and treatment, especially via lifestyle health approaches.
6.3. Skin Health and Exposome Factors (Stressors)
Miranda A. Farage from Procter and Gamble reported in 2008 that 50 to almost 70% of women reported skin sensitivity worldwide [173]. Later in 2013, Farage et al. confirmed their earlier findings, but also recognized that psychosocial influences, as well as biological and environmental factors contribute to skin sensitivity [174]. The first published reports on air pollution and skin aging appeared in the Journal of Investigative Dermatology in 2010 [175,176]. Both reports suggested that air pollution exposure was significantly correlated with extrinsic skin aging, particularly to pigment spots on the face and hands and, to a lesser extent, for wrinkles [175,176]. However, more recently a much broader perceptive of skin aging includes the concept of the exposome. For example, the exposome can be defined as the measure of all the exposures of an individual in a lifetime and how those exposures relate to health. An individual’s exposure begins before birth and includes insults from environmental and occupational sources, etc. Understanding how exposures from our environment, diet, lifestyle, etc. interact with our own unique characteristics such as genetics, physiology, and epigenetics impact our health is how the exposome will be articulated [177]. Thus, exposome factors that lead to stressed skin (via oxidative stress mechanisms) can be defined as any disturbance to skin homeostasis from environmental (meteorological factors like temperature, humidity, etc.), photo-aging, water/air pollution (external and household), tobacco use (smoking and/or vaping) and internal exposure like (unhealthy diets, hormonal variations/changes with menopause), lack of sleep, psychosocial or cultural stresses [2,14,116,178,179,180]. In general, exposome stress factors can influence six key skin functions, namely the skin barrier, pigmentation, defenses (antioxidant, immune cell mechanisms, microbial and microbiome maintenance), structure (extracellular matrix components), neuroendocrine and thermoregulatory functions [179,180]. The physical signs of stressed skin include dry skin, fine/moderate lines/wrinkles, oily skin, sensitive skin, pruritus, erythema, pale/dull skin, edema, and inflammatory skin conditions such as acne, atopic dermatitis, pigmentation disorders, rosacea, and skin infections [178,179,180]. Parreson et al., in 2021, suggested how to avoid exposome factors/stressor by: (a) getting adequate sun protection (sunscreen, sun avoidance, and protective clothing, (b) adopting a healthy lifestyle (eating a balanced diet, sleeping well, acquiring and using personal stress management skills and utilize psychosocial interventions for obtaining and exchanging ideas), and (c) enhancing the skin’s physical barrier and defenses against exposome factors with topical and oral antioxidants, antipollution products, probiotics, moisturizers and other personal care products [180].
Finally, in this regard, the emerging strategies for photoprotection (using sunscreens) [181,182], lifestyle health interventions [2,14,116,158,183] and the use of bioactive textiles to enhance the skin’s microbiota [184], along with the effects of spaceflight’s influence on human skin [185] have been reported.
7. Factor 3: Lifestyle Health—Physical Exercise and Skin Health
Regular moderate to intense exercise levels have long been known for its active role in improving physical fitness, sustained health and is widely accepted as a preventive and therapeutic strategy for many chronic and age-related diseases [186,187]. It has been proposed that exercise sustains health by: (a) helping to control body weight, (b) enhancing circadian rhythms, (c) promoting repair/regeneration, (d) protecting the integrity of barriers (from organelles to cells/tissues and organs), (e) benefiting turnover and recycling of cells/tissues, (f) providing cardiovascular and immune protection, (g) improving resilience, (h) boosting energy, (i) improving mood, (j) providing better sleep and (k) maintaining the body’s homeostatic balance of functional systems [186,187]. The concept and topic of the health benefits of exercise is easy to follow and understand, especially since the mitochondria with each cell in the body produces the energy needed [via the synthesis of adenosine triphosphate (ATP)] to carry out cellular respiration and the functions/thousands of biochemical reactions each second of life [188]. Each cell in the human body uses about 10–15 million molecules of ATP every second [188].
In dermatology, exercise has positive influences on: (a) skin aging, (b) skin cancer, (c) psoriasis, (d) venous ulcers, (e) androgenetic alopecia, and (f) skin moisturizing and hydration [189,190]. In brief, the known skin benefits of regular physical exercise include: (a) improving blood flow to nourish cells and remove toxins from the skin, (b) preventing the signs of aging by boosting collagen, elasticity, tone/turgor, the skin barrier, (c) inhibiting the anti-inflammatory actions of oxidative stress and MMPs, (d) decreasing stress by increasing dermal resilience, and (e) maintaining improved overall skin well-being [189,190,191]. However, it must be pointed out that individuals with inflammatory skin disorders (i.e., acne, atopic dermatitis, eczema, psoriasis, rosacea, etc.) should seek medical guidance before starting an exercise program, plus everyone should be cautious and wear protective clothing and limit their sun exposure [192].
8. Factor 4: Lifestyle Skin Health—Social/Community and Skin Health
Within the framework of lifestyle health, social interactions and/or isolation play important roles in determining an individual’s well-being because chronic and age-related disorders/diseases are linked to the lack of social contact with meaningful in person activities [193,194]. Social isolation is well known and common in older groups, but the increased isolation among younger adults is due to greater social media use [194].
In a recent study by Cudjoe et al., in 2022, found that social isolation in older adults is associated with higher levels of (the inflammatory biomarkers) interleukin-6 (IL-6) and C-reactive protein (CRP) that suggested a link between social isolation and morbidity/mortality [195]. Kottner et al., in 2023, showed that isolation in older individuals displayed skin changes (thinning of the epidermis, flattening of the dermal-epidermal junction, decreases in the fat layer (hypodermis) and collagen and elastin fibers in the dermis [196], which indicated that clinical practice guidelines to promote skin health in older people might be improved [196].
One factor associated with social isolation might be a negative body image that is common in men and women (usually associated with an increase in BMI and/or decreased skin health-lack of dermal elasticity and the appearance of wrinkles) [197]. However, physical activity and exercise, yoga, massage, dance therapy and body awareness therapy represent alternative methods to address negative body image issues, especially in women [197,198].
Social isolation was the norm during the COVID-19 pandemic. This isolation resulted in cutaneous changes in the general public, patients, and health care workers [198,199,200]. In general, there was an increase in atopic dermatitis, psoriasis, rosacea plus many other skin inflammatory diseases [199,200,201]. However, much of the increase was due to allergic dermatitis induced by hypersensitivity to personal protective equipment (PPE; masks, goggles, face shields, gloves, heat stress, etc.) [199,200]. Conversely, one study during the COVID-19 pandemic examined the connections between the neurological, neuroendocrine, and immune systems that triggered dermatoses influenced by factors such as stress, fear, negative thoughts, and anxiety, which resulted in skin inflammatory outbreaks not attributed to PPE use [201]. This suggested that a psychological component potentially linked to social isolation was the main cause, which was greater than only among those infected with COVID-19 [201]. This last study opens a perspective of how our environment interacts with human health and the interlinking of humans socially with each as well as through ecosystems like the microbiome, including that of the skin. [202].
Finally, it is well established that social relationships provide a clear link to improved health and well-being [193,194,203], including dermal health [196,201]. Just as the review of combined data for a variety of outcomes found that social media interventions that aim to increase physical activity and well-being were effective [204], this approach might be an application for improved skin health in the future.
9. Conclusions
Lifestyle health has been recognized as an evidence-based innovation that defines how daily habits and practices impact both the prevention and treatment of disease and provides an important adjunctive component to overall health [21]. Specifically, an approach with small changes over time can have a dramatic impact on the health and well-being of individuals not only, in general, but also can be applied to skin health. This narrative overview presented four lifestyle health factors to maintain and improve skin health. Lifestyle health factor 1: nutrition—diet and skin health; factor 2: rest (sleep) and skin health; factor 3: movement/physical exercise and skin health, and factor 4: social and community associations and skin health (see Figure 9).
Lifestyle change is often a gradual process involving multiple forward efforts and some setbacks, but this paradigm is a routine/program rather than an event. Finally, there are many ways to enhance skin health (especially with aging), if people alter their perspective and feelings about making changes based on short duration interventions with healthy goals in mind [2,5,9,11,17,38,49,50,79,96,116,205].
Author Contributions
Conceptualization, H.K. and E.D.L. research search literature methodology, E.D.L. formal analysis, journal report/review curation, E.D.L.; writing—original draft preparation, H.K. and E.D.L.; writing—review and editing, H.K. and E.D.L.; figure generation/visualization, H.K. and E.D.L.; funding acquisition, H.K. and E.D.L. All authors have read and agreed to the published version of the manuscript.
Funding
The work was supported, in part, by funding from Nu Skin Enterprises and from the TTO/Life Science College grant 19-2215 at Brigham Young University.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this overview are available in this manuscript, figures and/or cited references.
Acknowledgments
We thank Janet Faye Lephart for her editorial assistance in the preparation of the drafts for this manuscript.
Conflicts of Interest
Helen Knaggs has nothing to disclose. Edwin D. Lephart has no funding or sponsor conflict of interest in the decision of the data/research presented in this overview and regarding the publication of this manuscript. Edwin D. Lephart is an inventor on polyphenolic/vitamin/mineral patents (US and worldwide) on various human health applications.
References
- Krutmann, J.; Bouloc, A.; Sore, G.; Bernard, B.A.; Passerson, T. The skin aging exposome. J. Dermatol. Sci. 2017, 85, 152–161. [Google Scholar] [CrossRef]
- Lephart, E.D.; Naftolin, F. Factors influencing skin aging and the important role of estrogens and selective estrogen receptor modulators (SERMs). Clin. Cosmet. Investig. Dermatol. 2022, 15, 1695–1709. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Su, W.; Wang, F. Skin aging: A progressive, multi-factorial condition demanding and integrated, multilayer-targeted remedy. Clin. Cosmet. Investig. Dermatol. 2023, 16, 1215–1229. [Google Scholar] [CrossRef] [PubMed]
- Rippe, J.M. Lifestyle Medicine: The health promoting power of daily habits and practices. Am. J. Lifestyle Med. 2018, 12, 499–512. [Google Scholar] [CrossRef] [PubMed]
- Rippe, J.M. Lifestyle Medicine, 3rd ed.; CRC Press, Taylor & Francis Group: Boca Raton, FL, USA, 2019; pp. 1–1404. [Google Scholar]
- US Department of Health and Human Services; US Department of Agriculture. 2020–2025 Dietary Guidelines for Americans, 9th ed.; US Department of Health and Human Services: Washington, DC, USA; US Department of Agriculture: Washington, DC, USA, 2020. Available online: https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf (accessed on 31 July 2023).
- Abe, M.; Abe, H. Lifestyle medicine- An evidence based approach to nutrition, sleep, physical activity, and stress management on health and chronic illness. Pers. Med. Universe 2019, 8, 3–9. [Google Scholar] [CrossRef]
- Cena, H.; Calder, P.C. Defining a healthy diet: Evidence for the role of contemporary dietary patterns in health and disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef] [PubMed]
- Santos, L. The impact of nutrition and lifestyle modification on health. Eur. J. Intern. Med. 2022, 97, 18–25. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Research (NIHR). Healthy Lifestyles Increase Life Expectancy in People with Multiple Conditions (Multimorbidity) by as Much as in Other Groups. Public Health 2021. Available online: https://evidence.nihr.ac.uk/alert/healthy-lifestyles-increase-life-expectancy-in-people-with-multiple-conditions-multimorbidity-by-as-much-as-in-other-groups/#:~:text=The%20healthier%20the%20lifestyle%2C%20the,compared%20with%20the%20unhealthiest%20lifestyles (accessed on 31 July 2023).
- Wong, V.W.-H.; Ho, F.Y.-Y.; Wong, Y.S.-H.; Chung, F.-K.; Yeung, W.-F.; Ng, C.H.; Sarris, J. Efficacy of lifestyle medicine on sleep quality: A meta-analysis of randomized controlled trails. J. Affect. Disord. 2023, 330, 125–138. [Google Scholar] [CrossRef]
- Wong, V.W.-H.; Ho, F.Y.-Y.; Shi, N.-G.; Sarris, J.; Ng, C.H.; Tam, O.K.-Y. Lifestyle medicine for anxiety symptoms: A meta-analysis of randomized controlled trials. J. Affect. Disord. 2022, 10, 354–368. [Google Scholar] [CrossRef]
- Zhang, S.; Zhang, N.; Wang, S.; Hong, J.; Li, F.; Guo, H.; Lv, Z.; Wang, Y.; Wang, W.; Wu, W. Circadian rhythms and sleep quality among undergraduate students in China: The mediating role of health-promoting lifestyle behaviours. J. Affect. Disord. 2023, 333, 225–232. [Google Scholar] [CrossRef]
- Murad, H. Cultural stress: The undiagnosed epidemic of our time. J. Integr. Med. 2023. ahead-of-print. [Google Scholar] [CrossRef] [PubMed]
- Yanping, L.; Pan, A.; Wang, A.A.; Liu, Z.; Dhana, K.; Franco, O.H.; Kaptoge, S.; Di Angelantonio, E.; Stampfer, M.; Willett, W.C.; et al. Impact of health lifestyle factors on life expectancies in the US population. Circulation 2018, 138, 345–355. [Google Scholar]
- Hu, P.; Zheng, M.; Huang, J.; Fan, H.-Y.; Fan, C.-J.; Ruan, H.-H.; Yuan, Y.-S.; Zhao, W.; Wang, H.H.X.; Deng, H.; et al. Effect of healthy lifestyle index and lifestyle patterns on the risk of mortality: A community-based cohort study. Front. Med. 2022, 9, 920760. [Google Scholar] [CrossRef]
- Rozanski, A.; Blumenthal, J.A.; Hinderliter, A.L.; Cole, S.; Lavie, G.J. Cardiology and lifestyle medicine. Prog. Cardiovasc. Dis. 2023, 77, 4–13. [Google Scholar] [CrossRef]
- Cudjoe, T.K.M.; Roth, D.L.; Szanton, S.L.; Wolff, J.L.; Boyd, C.M.; Thorpe, R.J. The epidemiology of social isolation: National health and aging trends study. J. Gerontol. B Psycol. Sci. Soc. Sci. 2020, 75, 107–113. [Google Scholar] [CrossRef]
- Ding, Z.; Leung, P.-Y.; Lee, T.-I.; Chan, A.S. Effectiveness of lifestyle medicine on cognitive functions in mild cognitive impairments and dementia: A systematic review of randomized controlled trails. Ageing Res. Rev. 2023, 86, 101886. [Google Scholar] [CrossRef] [PubMed]
- Ye, K.X.; Sun, L.; Wang, L.; Khoo, A.L.Y.; Lim, K.X.; Lu, G.; Yu, L.; Li, C.; Maier, A.B.; Feng, L. The role of lifestyle factors in cognitive health and dementia in oldest-old: A systematic review. Neurosci. Biobehav. Rev. 2023, 152, 105286. [Google Scholar] [CrossRef]
- JoJack, B. Eight Healthy Habits that May Add 24 Years to Your Lifespan. Medical News Today. 25 July 2023. Available online: https://www.medicalnewstoday.com/articles/8-healthy-longevity-habits-add-24-years-to-lifespan (accessed on 31 July 2023).
- Standing, S. Skin and its appendage. In Gray’s Anatomy, 42nd ed.; Standing, S., Ed.; Elsevier: Philadelphia, PA, USA, 2021; Chapter 7. [Google Scholar]
- Lephart, E.D.; Naftolin, F. Estrogen action and gut microbiome metabolism in dermal health. Dermatol. Ther. 2022, 12, 1535–1550. [Google Scholar] [CrossRef]
- Bernatchez, S.; Bichel, J. The science of skin: Measuring damage and assessing risk. Adv. Wound Care 2023, 12, 187–204. [Google Scholar] [CrossRef]
- Jansen van Rensburg, S.; Franken, A.; Du Plessis, J.L. Measurement of transepidermal water loss, stratum corneum hydration and skin surface pH in occupational settings: A review. Skin Res. Technol. 2019, 25, 595–605. [Google Scholar] [CrossRef]
- Haniffa, M.; Gunawan, M.; Jardine, L. Human skin dendritic cells in health and disease. J. Dermatol. Sci. 2015, 77, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.M.; Yosipovitch, G. Skin pH: From basic science to basic skin care. Acta Derm. Venereol. 2013, 93, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Lupa, D.M.; Fakalah, F.; Safferling, K.; Boukamp, P.; Poschmann, G.; Volpo, E.; Gotz-Rosch, C.; Bernerd, F.; Haag, L.; Huebenthal, U.; et al. Characterization of skin aging- Associated secreted proteins (SSAAP) produced by dermal fiboblasts isolated from intrinsically aged skin. J. Investig. Dermatol. 2015, 135, 1954–1968. [Google Scholar] [CrossRef]
- Bonté, F.; Girard, D.; Archambault, J.-C. Chapter 10, Skin changes during aging, 9n. In Biochemistry & Cell Biology of Aging: Part II Clinical Sciences, Subcellular Biochemistry 91; Harris, J.R., Korolchuk, V.I., Eds.; Springer Nature: Singapore, 2019; pp. 249–280. [Google Scholar]
- Karim, P.L.; Npriyati, I.A.A. Anatomy and histology of intrinsic aging skin. Biosci. Med. 2021, 5, 1065–1077. [Google Scholar]
- Huang, A.H.; Chien, A.L. Photoaging: A review of the current literature. Curr. Dermatol. Rep. 2020, 9, 22–29. [Google Scholar] [CrossRef]
- Sparavigna, A. Role of the extracellular matrix in skin aging and dedicated treatment—State of the art. Plast. Aesthet. Res. 2020, 7, 14. [Google Scholar] [CrossRef]
- Lee, A.-Y. Skin pigmentation abnormalities and their possible relationship with skin aging. Int. J. Mol. Sci. 2021, 22, 3727. [Google Scholar] [CrossRef]
- Sant Anna Addor, F.A. Beyond photoaging: Additional factors involved in the process of skin aging. Clin. Cosmet. Investig. Dermatol. 2018, 11, 437–443. [Google Scholar] [CrossRef]
- Woodby, B.; Penta, K.; Pecorelli, A.; Lila, M.A.; Valacchi, G. Skin health from the inside out. Annu. Rev. Food Sci. Technol. 2020, 11, 235–254. [Google Scholar] [CrossRef]
- Lephart, E.D. Skin aging and oxidative stress: Equol’s anti-aging effects via biochemical and molecular mechanisms. Ageing Res. Rev. 2016, 31, 36–54. [Google Scholar] [CrossRef]
- Varani, J.; Dame, M.K.; Rittie, L.; Fligiel, S.E.G.; Kang, S.; Fisher, G.J.; Voorhees, J.J. Decreased collagen production in chronically aged skin. Am. J. Pathol. 2006, 168, 1861–1868. [Google Scholar] [CrossRef] [PubMed]
- Lephart, E.D.; Naftolin, F. Menopause and the skin: Old favorites and new innovations in cosmeceuticals for estrogen-deficient skin. Dermatol. Ther. 2021, 11, 53–69. [Google Scholar] [CrossRef] [PubMed]
- Lephart, E.D. A review of the role of estrogen in dermal aging and facial attractiveness in women. J. Cosmet. Dermatol. 2018, 17, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhang, Z.; Ren, Y.; Wang, Y.; Fang, J.; Yue, H.; Ma, S.; Guan, F. Aging and age-related disease: From mechanisms to therapeutic strategies. Biogerontology 2021, 22, 165–187. [Google Scholar] [CrossRef]
- Phuoung, C.; Maibach, H.I. Biological effects of estrogen on skin. In Textbook of Aging Skin; Farage, M.A., Miller, K.W., Maibach, H.I., Eds.; Springer: Berlin/Heidelburg, Germany, 2015; pp. 1–12. [Google Scholar]
- Reilly, D.M.; Lozano, J. Skin collagen through the lifestages: Importance for skin health and beauty. Plast. Aesthet. Res. 2021, 8, 2. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Blume-Peytavi, U.; Kosmadaki, M.; Roo, E.; Kerob, D.V.-R.D.; Goldstein, S.R. Skin, hair and beyond: The impact of menopause. Climacteric 2022, 25, 434–442. [Google Scholar] [CrossRef]
- Santen, R.J.; Simpson, E.R. History of estrogen: Its purification, structure, synthesis, biological actions, and clinical implications. Endocrinology 2019, 160, 605–625. [Google Scholar] [CrossRef]
- Rzepecki, A.K.; Murase, J.E.; Juran, R.; Fabi, S.G.; McLellan, N. Estrogen-deficient skin: The role of topical therapy. Int. J. Women’s Dermatol. 2019, 5, 85–90. [Google Scholar] [CrossRef]
- Thornton, M.J. Estrogens and skin aging. Dermatoendcrinology 2013, 5, 264–270. [Google Scholar] [CrossRef]
- Ceccarelli, I.; Bioletti, B.; Peparini, S. Estrogens and phytoestrogens in body functions. Neurosci. Biobehav. Rev. 2022, 132, 648–663. [Google Scholar] [CrossRef]
- Hong, H.-C.; Chang, W.-H.; Yeh, C.-C. Estrogen effects on wound healing. Int. J. Mol. Sci. 2017, 18, 2325. [Google Scholar] [CrossRef]
- Wilkinson, H.N.; Hardman, M.J. A role of estrogen in skin aging and dermal biomechanics. Mech. Ageing Dev. 2021, 197, 111513. [Google Scholar] [CrossRef] [PubMed]
- Lephart, E.D. Phytoestrogens (resveratrol and equol) for estrogen-deficient skin-controversies/misinformation versus anti-aging in vitro and clinical evidence via nutraceutical-cosmetics. Int. J. Mol. Sci. 2021, 11, 11218. [Google Scholar] [CrossRef] [PubMed]
- Slominski, A.; Zbytek, B.; Nikolakis, G.; Manna, P.R.; Skobowiat, C.; Zmijewski, M.; Li, W.; Janjetovic, Z.; Postlethwaite, A.; Zouboulis, C.C. Steroidogenesis in the skin: Implications for local immune function. J. Steroid Biochem. Mol. Biol. 2013, 137, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Antonini, D.; Siblo, A.; Dentice, M.; Missero, C. An intimate relationship between thyroid hormone and skin: Regulation of gene expression. Front. Endocrinol. 2013, 4, 104. [Google Scholar] [CrossRef]
- Safer, J.D. Thyroid hormone action on skin. Derm. Endocrinol. 2011, 3, 211–215. [Google Scholar] [CrossRef]
- Chen, Y.; Luga, J. Brain-skin connection: Stress, inflammation and skin health. Inflam. Allergy Drug Targets 2014, 13, 177–190. [Google Scholar] [CrossRef]
- Choe, S.J.; Kim, D.; Kim, E.J.; Ahn, J.-S.; Choi, E.-J.; Son, E.D.; Lee, T.R.; Choi, E.H. Psychological stress deteriorates skin barrier function by activating 11β-hydroxy steroid dehydrogenase 1 and the HPA axis. Sci. Rep. 2018, 8, 6344. [Google Scholar] [CrossRef]
- Huber, J.; Gruber, C. Immunological and dermatological impact of progesterone. Gynecol. Endocrinol. 2001, S6, 18–21. [Google Scholar] [CrossRef]
- Phillips, N.; Devaney, J. Beneficial regulation of type 1 collagen and matrixmetalloproteinase-1 expression by estrogen, progesterone, and its combination in skin fibroblasts. J. Am. Aging Assoc. 2003, 26, 59–62. [Google Scholar] [CrossRef]
- Gasser, S.; Heidemeyer, K.; von Wolff, M.; Stute, P. Impact of progesterone on skin and hair in menopause-a comprehensive review. Climacteric 2021, 24, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://nrd.gov/resource/detail/14117290/National+Institute+on+Aging (accessed on 5 August 2023).
- Available online: https://www.un.org/development/desa/dspd/2023/01/world-social-report-2023/ (accessed on 28 July 2023).
- Franceschi, C.; Garagnani, P.; Parini, P.; Giuliani, C.; Santoro, A. Inflammaging: A new immune-metabolic viewpoint for age-related diseases. Nat. Rev. Endocrinol. 2018, 14, 576–590. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.Y.; Cesare, M.; Anton, S.; Marzetti, E.; Giovannini, S.; Seo, A.Y.; Carter, C.; Yu, B.P.; Leeuwenburgh, C. Molecular inflammation: Underpinnings of aging and age-related disease. Ageing Res. Rev. 2009, 8, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Dumic, I.; Nordin, T.; Jecmenica, M.; Lalosevic, M.S.; Milosavljevic, T.; Milovanovic, T. Gastrointestinal tract disorders in older age. Can. J. Gastroenterol. Hepatol. 2019, 19, 6757524. [Google Scholar] [CrossRef]
- City of Hope. At What Age Is Cancer Most Common? 6 June 2023. Available online: https://www.cancercenter.com/community/blog/2023/06/cancer-risk-by-age#:~:text=By%20and%20large%2C%20the%20biggest,in%20between%20ages%2035%2D44 (accessed on 7 August 2023).
- Murray, C.J.L. (GBD 2019 Cancer Risk Factors Collaborators). The global burden of cancer attributed to risk factors, 2010–2019: A systematic analysis for the global burden of disease study 2019. Lancet 2022, 400, 563–591. [Google Scholar]
- Alegria-Torres, J.A.; Baccarelli, A.; Bollati, V. Epigenetics and lifestyle. Epigenetics 2011, 3, 267–277. [Google Scholar] [CrossRef]
- Kassis, A.; Fichot, M.-C.; Horcajada, M.-N.; Horstman, A.M.H.; Duncan, P.; Bergonzelli, G.; Preitner, N.; Zimmermann, D.; Bosco, N.; Vidal, K.; et al. Nutritional and lifestyle management of the aging journey: A narrative review. Front. Nutr. 2023, 9, 1087505. [Google Scholar] [CrossRef]
- Loef, B.; Herber, G.-C.M.; Wong, A.; Janssen, N.A.H.; Hoekstra, J.; Picavet, H.S.J.; Verschuren, W.M.M. Predictors of healthy physiological aging across generations in a 30-year population-based cohort study: The Doetinchem Cohort Study. BMC Geiratrics 2023, 23, 107. [Google Scholar] [CrossRef]
- Bosnes, I.; Norhahl, H.M.; Stordal, E.; Bosnes, O.; Myklebust, T.A.; Almkvist, O. Lifestyle predictors of successful aging: A 20-year prospective HUNT study. PLoS ONE 2019, 14, e0219200. [Google Scholar] [CrossRef]
- Katz, S. Active and successful aging. Lifestyle as a gerontological idea. Rech. Sociol. Et Anthropol. 2013, 44, 33–49. Available online: https://journals.openedition.org.ras.910 (accessed on 17 August 2023). [CrossRef]
- Sakaniwa, R.; Noguchi, M.; Imano, H.; Shirai, K.; Tamakoshi, A.; Iso, H.; The JACC Study Group. Impact of modifiable health lifestyle adoption on lifetime gain form middle to older age. Age Ageing 2022, 51, afac080. [Google Scholar] [CrossRef] [PubMed]
- Wahl, D.; Solon-Biet, S.M.; Cogger, V.C.; Fontana, L.; Simpson, S.J.; Le Couteur, D.G.; Ribeiro, R.V. Aging, lifestyle and dementia. Neurobiol. Dis. 2019, 130, 104481. [Google Scholar] [CrossRef] [PubMed]
- Buettner, D.; Skemp, S. Blue zones: Lessons from the world’s longest lived. Am. J. Lifestyle Med. 2016, 10, 318–322. [Google Scholar] [CrossRef] [PubMed]
- National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP). Poor Nutrition. Available online: https://www.cdc.gov/chronicdisease/resources/publications/factsheets/nutrition.htm#:~:text=A%20healthy%20diet%20helps%20children,2%20diabetes%2C%20and%20certain%20cancers (accessed on 9 August 2023).
- Stewart, K.L.; Lephart, E.D. Overview of BPH: Symptom relief with dietary polyphenols, vitamins, and phytochemicals by nutraceutical supplements with implications to the prostate microbiome. Int. J. Mol. Sci. 2023, 24, 5486. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean diet and health status: Active ingredients and pharmacological mechanisms. Br. J. Pharmacol. 2020, 177, 1241–1257. [Google Scholar] [CrossRef]
- Raits, E.; Kirse-Ozolina, A. Modern dietary patterns based on territorial origin—A review. Foodblat 2019. [Google Scholar] [CrossRef]
- Maleaza, I.J.; Malesza, M.; Walkowiak, J.; Mussin, N.; Walkowiak, D.; Aringazina, R.; Bartkowiak-Wieczorek, J.; Madry, E. High-fat, Western-style diet, systematic inflammation, and gut microbiota: A narrative review. Cells 2021, 10, 3164. [Google Scholar] [CrossRef]
- Mazza, E.; Ferro, Y.; Pujia, R.; Mare, R.; Maurotti, T.; Puijia, A. Mediterranean diet in healthy aging. J. Nutr. Health Aging 2021, 25, 1076–1083. [Google Scholar] [CrossRef]
- Galbete, C.; Schwingshackl, L.; Schwedheln, C.; Boeing, H.; Schulze, M.B. Evaluation of the Mediterranean diet and risk of chronic disease in cohort studies: An umbrella review of meta-analyses. Eur. J. Epidermiol. 2018, 33, 909–931. [Google Scholar] [CrossRef]
- Stefler, D.; Brett, D.; Sarkadi-Nagy, E.; Kopczynska, E.; Detchev, S.; Bati, A.; Scrob, M.; Koenker, D.; Aleksov, B.; Douarin, E.; et al. Traditional Eastern European diet and mortality: Prospective evidence for the HAPIEE study. Eur. J. Nutr. 2021, 60, 1091–1100. [Google Scholar] [CrossRef]
- World Heart Federation. 2023. Available online: https://world-heart-federation.org/where-we-work/europe-central-asia/ (accessed on 11 August 2023).
- Cao, C.; Xiao, Z.; Wu, Y.; Ge, C. Diet and skin aging-from the perspective of food nutrition. Nutrients 2020, 12, 870. [Google Scholar] [CrossRef]
- Palma, L.; Marques, L.T.; Bujan, J.; Rodrigues, L.M. Dietary water affects human skin hydration and biomechanics. Clin. Cosmet. Investig. Dermatol. 2015, 8, 413–421. [Google Scholar]
- Popkin, B.M.; Rosenberg, I.H. Water, hydration and health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Akdeniz, M.; Tomova-Simithieva, T.; Dobos, G.; Blume-Peytavi, U.; Kottner, J. Does dietary fluid intake affect skin hydration in healthy humans? A systematic literature review. Skin Res. Technol. 2018, 24, 459–465. [Google Scholar] [CrossRef]
- Wu, G. Dietary protein intake and human health. Food Funct. 2016, 7, 1251–1265. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, D.L.; West, V.A.; Lephart, E.D. Enhancing skin health: By oral administration of natural compounds and minerals with implications to the dermal microbiome. Int. J. Mol. Sci. 2018, 19, 3059. [Google Scholar] [CrossRef]
- Nieves, D.S.; Goldsmith, L.A. Cutaneous changes in nutritional disease. Chapter 145. In Fitzpatrick’s Dermatology in General Medicine, 6th ed.; Freedburg, I.M., Eisen, A., Wolff, K., Austen, K.F., Goldsmith, L.A., Katz, S.I., Eds.; McGraw-Hill: London, UK, 2003; pp. 1399–1411. [Google Scholar]
- Choi, F.D.; Sung, C.T.; Juhasz, J.L.W.; Mesinkovsk, N.A. Oral collagen supplementation: A systematic review of dermatological applications. J. Drugs Dermatol. 2019, 18, 9–16. [Google Scholar] [PubMed]
- de Miranda, R.B.; Weimer, R.; Rossi, R. Effects of hydrolyzed collagen supplementation on skin aging: A systematic review and meta-analysis. Int. J. Dermatol. 2021, 60, 1449–1461. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.G.; Lee, J.; Choi, S.; Suk, J.; Lee, J.H.; Yang, J.H.; Yang, J.S.; Kim, J. Oral supplementation of low-molecular weight collagen peptides reduces skin wrinkles and improves biophysical properties of skin: A randomized, double-blind, placebo-controlled study. J. Med. Food 2022, 24, 1146–1154. [Google Scholar] [CrossRef]
- Coerdt, K.M.; Goggins, C.A.; Khachemoune, A. Vitamins A, B, C, and D: A short review for the dermatologist. Altern. Ther. Health Med. 2021, 27, 41–49. [Google Scholar]
- Draelos, Z.D. An oral supplement and the nutrition-Skin connection. J. Clin. Aesthet. Dermatol. 2019, 12, 13–16. [Google Scholar] [PubMed]
- Faria-Silva, C.; Ascenso, A.; Costa, A.M.; Marto, J.; Carbalheiro, M.; Ribeiro, H.M.; Simoes, S. Feeding the skin: A new trend in food and cosmetics convergence. Trends Food Sci. Technol. 2020, 95, 21–32. [Google Scholar] [CrossRef]
- Liu, T.; Li, N.; Yan, Y.; Liu, Y.; Xiong, K.; Liu, Y.; Xia, Q.-M.; Zhang, H.; Liu, Z.-D. Recent advances in the anti-aging effects of phytoestrogens on collagen, water content, and oxidative stress. Phytotherapy Res. 2020, 34, 435–447. [Google Scholar] [CrossRef]
- Juturu, V.; Bowman, J.P.; Deshpande, J. Overall skin tone and skin-lightening-improving effects with oral supplementation of lutein and zeaxanthin isomers: A double-blind, placebo-controlled clinical trial. Clin. Cosmet. Investig. Derm. 2016, 9, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Fam, V.W.; Charoenwoodhipong, P.; Sivamani, R.J.; Holt, R.R.; Keen, C.L.; Hackman, R.M. Plant-based foods for skin health: A narrative review. J. Acad. Nutr. Diet. 2020, 122, 614–629. [Google Scholar] [CrossRef]
- Michalak, M. Plant-derived antioxidants: Significance in skin health and the ageing process. Int. J. Mol. Sci. 2022, 23, 585. [Google Scholar] [CrossRef]
- Darbre, P.D. Chapter 5-Plant-based ingredients in personal care products. In Personal Care Products and Human Health; Darbre, P.D., Ed.; Academic Press-Elsevier: London, UK, 2023; pp. 97–1112. [Google Scholar]
- Lee, J.H.; Park, J.; Skin, D.W. The molecular mechanism of polyphenols with anti-aging activity in aged human dermal fibroblasts. Molecules 2022, 27, 4351. [Google Scholar] [CrossRef]
- Solway, J.; McBride, M.; Haq, F.; Abdul, W.; Miller, R. Diet and dermatology: The role of a whole-food, plant-based diet in preventing and reversing skin aging, a review. J. Clin. Aesthet. Dermatol. 2020, 13, 38–43. [Google Scholar]
- Lephart, E.D. Determination of S-equol and/or R-equol in plant-based food products and efficacy of topical or oral 4′,7-isoflavandiol (R/S equol) to improve skin health in adult men, a placebo-controlled study. J. Funct. Foods 2021, 83, 104563. [Google Scholar] [CrossRef]
- Teng, Y.; Huang, Y.; Xu, D.; Tao, X.; Fan, Y. The role of probiotics in skin photoaging and related mechanisms: A review. Clin. Cosmet. Investig. Derm. 2022, 15, 2455–2464. [Google Scholar] [CrossRef]
- De Almeida, C.V.; Antiga, E.; Lulli, M. Oral and topical probiotics and postbiotics in skincare and dermatological therapy: A concise review. Microorganisms 2023, 11, 1420. [Google Scholar] [CrossRef] [PubMed]
- Gao, T.; Wang, X.; Li, Y.; Ren, F. The role of probiotics in skin health and related gut-skin axis: A review. Nutrients 2023, 15, 3123. [Google Scholar] [CrossRef]
- Szanto, M.; Dozsa, A.; Antal, D.; Szabo, K.; Kemeny, L.; Bai, P. Targeting the gut-skin axis-Probiotics as a new tool for skin disorder management. Exp. Dermatol. 2019, 28, 1210–1218. [Google Scholar] [CrossRef] [PubMed]
- Khmaladze, I.; Leonardi, M.; Fabre, S.; Messaraa, C.; Mavon, A. The skin interactome: A holistic “genone-microbiome-exposome” approach to understand and modulate skin health and aging. Clin. Cosmet. Investig. Dermatol. 2020, 13, 1021–1040. [Google Scholar] [CrossRef] [PubMed]
- Souak, D.; Barreau, M.; Courtois, A.; Andre, V.; Poc, C.D.; Feuilloley, M.G.J.; Gault, M. Challenging cosmetic innovation: The skin microbiota and probiotics protect the skin from UV-induced damage. Microorganisms 2021, 9, 936. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Qu, L.; Mijakovic, I.; Wei, Y. Advances in the human skin microbiota and its roles in cutaneous diseases. Microb. Cell Factories 2022, 21, 176. [Google Scholar] [CrossRef]
- Galland, L. Diet and inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef]
- Moldogazieva, N.T.; Mokhosoev, I.M.; Melnickova, U.I.; Porozov, Y.B.; Terrentiev, A.A. Oxidative stress and advanced lipoxidation and glycation end products (ALEs and AGEs) in aging and age-related diseases. Oxidative Med. Cell. Longev. 2019, 2019, 3085756. [Google Scholar] [CrossRef]
- Lai, S.W.T.; de Jesus Lopez Gonzales, E.; Zoukari, T.; Ki, P.; Shuck, S.C. Methylglyoxal and its adducts: Induction, repair, and association with disease. Chem. Res. Toxicol. 2022, 35, 1720–1746. [Google Scholar] [CrossRef]
- Kellow, N.J.; Coughlan, M.T.; Reid, C.M. Association between habitual dietary and lifestyle behaviours and skin autofluorescence (SAF), a marker of tissue accumulation of advanced glycation endproducts (AGEs), in healthy adults. Eur. J. Nutr. 2018, 57, 2209–2216. [Google Scholar] [CrossRef]
- Clatici, V.G.; Racoceanu, D.; Dalle, C.; Voicu, C.; Tomas-Aragones, L.; Marron, S.E.; Wollina, U.; Fica, S. Perceived age and life style. The specific contributions of seven factors involved in health and beauty. MAEDICA—J. Clin. Med. 2017, 12, 191–201. [Google Scholar]
- Hu, S.; Anand, P.; Laughter, M.; Maymone, M.B.C.; Dellavalle, R.P. Holistic dermatology: An evidence-based review of modifiable lifestyle factor associations with dermatologic disorders. J. Am. Acad. Dermatol. 2022, 86, 868–877. [Google Scholar] [CrossRef] [PubMed]
- Bajpai, V.; Singh, A.; Tripathi, S.; Kumar, A. Various aging factors significantly impact skin and its conclusion. Res. Rev. J. Health Prof. 2023, 13, 1–10. [Google Scholar]
- Soliman, Y.S.; Hashim, P.A.; Farberg, A.S.; Goldenberg, G. The role of diet in preventing photoaging and treating common skin conditions. Cosmet. Derm. 2019, 103, 153–156. [Google Scholar]
- Madden, S.K.; Flanagan, K.L.; Jones, G. How lifestyle factors and their associated pathogenetic mechanisms impact psoriasis. Clin. Nutr. 2020, 39, 1026–1040. [Google Scholar] [CrossRef]
- Jamochian, M.; Alamgir, M.; Rao, B. Diet and dermatology: Review of diet’s influence on the conditions of rosacea, hidradenitis, suppurativa, herpes labials, and vitiligo. Am. J. Lifestyle Med. 2021, 17, 152–160. [Google Scholar] [CrossRef]
- Musumeci, M.L.; Nasca, M.R.; Boscaglia, S.; Micali, G. The role of lifestyle and nutrition in psoriasis: Current status of knowledge and interventions. Dermatol. Ther. 2022, 35, e15685. [Google Scholar] [CrossRef]
- Hoonhorst, S.J.M.; Lo Tam Loi, A.T.; Pouwels, S.D.; Faiz, A.; Telenga, E.D.; van den Berge, M.; Koenderman, L.; Lammers, J.-W.J.; Boezen, H.M.; van Oosterhout, A.J.M.; et al. Advanced glycation endproducts and their receptor in different body compartments in COPD. Respir. Res. 2016, 17, 46. [Google Scholar] [CrossRef]
- Palimeri, S.; Palioura, E.; Diamanti-Kandarakis, E. Current perspectives on the health risks associated with the consumption of advanced glycation end products: Recommendations for dietary management. Diabetes Metab. Syndr. Obes. Targets Ther. 2015, 8, 415–426. [Google Scholar] [CrossRef]
- Rugratanwanich, W.; Qu, Y.; Wang, X.; Essa, M.M.; Song, B.-J. Advanced glycation end products (AGEs) and other adducts in aging-related disease and alcohol-mediated tissue injury. Exp. Mol. Med. 2021, 53, 168–188. [Google Scholar] [CrossRef]
- Goodman, G.D.; Kaufman, J.; Day, D.; Wiess, R.; Kawata, A.K.; Garcia, J.K.; Santangelo, S.; Gallagher, C.J. Impact of smoking and alcohol use on facial aging in women: Results of a large multinational, multiracial, cross-sectional survey. J. Clin. Aesthet. Dermatol. 2019, 12, 28–39. [Google Scholar] [PubMed]
- Mitri, A.; Lin, G.; Waldman, R.A.; Grant-Kels, J.M. Effects of tobacco and vaping on the skin. Clin. Dermatol. 2021, 39, 762–771. [Google Scholar] [CrossRef] [PubMed]
- Tackett, A.P.; Urman, R.; Barrington-Trimis, J.; Liu, F.; Hong, H.; Pentz, M.A.; Islam, T.S.; Eckel, S.P.; Rebuli, M.; Leventhal, A.; et al. Prospective study of e-cigarette use and respiratory symptoms in adolescents and young adults. Thorax 2023. ahead-of-print. [Google Scholar] [CrossRef] [PubMed]
- Gunn, D.A.; Larson, L.A.; Lall, J.S. Mortality is written on the face. J. Gerontol. Ser. A Biol. Med. Sci. 2016, 71, 72–77. [Google Scholar] [CrossRef]
- Emanuele, M.A.; Wezeman, F.; Emanuele, N.V. Alcohol’s effects on female reproductive function. Alcohol Res. Health 2002, 26, 274–281. [Google Scholar]
- McDivit, A.M.; Greendale, G.A.; Stanczyk, F.Z.; Huang, M.-H. Effects of alcohol and cigarette smoking on change in serum estrone levels in postmenopausal woman randomly assigned to fixed doses of conjugated equine estrogens with or without progestin. Menopause 2008, 15, 382–385. [Google Scholar] [CrossRef]
- Division Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion (CDC). Defining Adult Overweight and Obesity. 3 June 2022. Available online: https://www.cdc.gov/obesity/basics/adult-defining.html#:~:text=Adult%20Body%20Mass%20Index&text=If%20your%20BMI%20is%20less,falls%20within%20the%20obesity% (accessed on 17 August 2023).
- Boutari, C.; Mantzoros, C.S. A 2022 update on the epidemiology of obesity and a call to action: As its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism 2022, 133, 155217. [Google Scholar] [CrossRef]
- The GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. New Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Darlenski, R.; Mihaylova, V.; Handjieva-Darlenska, T. The link between obesity and the skin. Front. Nutr. 2022, 9, 855573. [Google Scholar] [CrossRef]
- Frasca, D.; Strbo, N. Effects of obesity on infections with emphasis on skin infections and wound healing. J. Dermatol. Skin Sci. 2022, 4, 5–10. [Google Scholar] [CrossRef]
- Nakamizo, S.; Honda, T.; Kabashima, K. Obesity and inflammatory skin diseases. Trends Immunother. 2019, 3, 50–57. [Google Scholar] [CrossRef]
- Palanivel, J.A.; Millington, G.W.M. Obesity-induced immunological effects on the skin. Ski. Health Dis. 2023, 3, e160. [Google Scholar] [CrossRef] [PubMed]
- Chambers, E.S.; Vukmanovic-Stejic, M. Skin barrier immunity and ageing. Immunology 2019, 160, 116–125. [Google Scholar] [CrossRef]
- Trompette, A.; Ubags, N.D. Skin barrier immunology from early life to adulthood. Mucosal Immunol. 2023, 16, 194–207. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, G.; Curatolo, S.; Busa, B.; Belfore, A.; Gullo, D. Two birds one stone: Semaglutide is highly effective against severe psoriasis in a type 2 diabetic patient. Endocrinol. Diabetes Metab. Case Rep. 2021. ahead-of-print. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Lin, L.; Chen, P.; Yu, Y.; Chen, S.; Chen, X.; Shao, Z. Treatment with liraglutide, a glucagon-like peptide-1 analogue, improves effectively skin lesions of psoriasis patients with type 2 diabetes: A prospective cohort study. Diabetes Res. Clin. Pract. 2019, 150, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.-P.; Dutil, C.; Featherstone, R.; Ross, R.; Giangregorio, L.; Saunders, T.J.; Janssen, I.; Poitras, V.J.; Kho, M.E.; Ross-White, A.; et al. Sleep timing, sleep consistency, and health in adults: A systematic review. Appl. Physiol. Nutr. Metab. 2020, 45, S232–S247. [Google Scholar] [CrossRef]
- McCarter, S.J.; Hagen, P.T.; St Louis, E.K.; Rieck, T.M.; Haider, C.R.; Holmes, D.R.; Morgenthaler, T.I. Physiological markers of sleep quality: A scoping review. Sleep Med. Rev. 2022, 64, 101657. [Google Scholar] [CrossRef] [PubMed]
- Troynikov, O.; Watson, C.G.; Nawaz, N. Sleep environments and sleep physiology: A review. J. Therm. Biol. 2018, 78, 192–203. [Google Scholar] [CrossRef]
- Lv, Y.; Jiang, G.; Tan, X.; Bao, W.; Chen, L.; Liu, L. Association of sleep patterns and lifestyles with incident hypertension: Evidence from a large population-based cohort study. Front. Cardiovasc. Med. 2022, 9, 847452. [Google Scholar] [CrossRef]
- Sejbuk, M.; Mironczuk-Chodakowska, I.; Witkowska, A.M. Sleep Quality: A narrative review on nutrition, stimulants, and physical activity as important factors. Nutrients 2022, 14, 1912. [Google Scholar] [CrossRef] [PubMed]
- Gangwisch, J.; Hale, L.; St-Onge, M.-P.; Choi, L.; LeBlanc, E.S.; Malaspina, D.; Opler, M.G.; Shadyab, A.H.; Shikany, J.M.; Snetselaar, L. High gylcemic index and glycemic load diets as risk factors for insomnia: Analyses from the women’s health initiative. Am. J. Clin. Nutr. 2020, 111, 429–439. [Google Scholar] [CrossRef] [PubMed]
- Binks, H.; Vincent, G.E.; Gupta, C.; Irwin, C.; Khalesi, S. Effects of diet on sleep: A narrative review. Nutrients 2020, 12, 936. [Google Scholar] [CrossRef] [PubMed]
- Stutanto, C.N.; Loh, W.W.; Toh, D.W.K.; Lee, D.P.S.; Kim, J.E. Association between dietary protein intake and sleep quality in middle-aged and older adults in Singapore. Front. Nutr. 2022, 9, 832341. [Google Scholar] [CrossRef]
- O’Callaghan, F.; Muurlink, O.; Reid, N. Effects of caffeine on sleep quality and daytime functioning. Risk Manag. Health Policy 2018, 11, 263–271. [Google Scholar] [CrossRef]
- Majid, M.S.; Ahmad, H.S.; Bizhan, H.; Hosein, H.Z.M.; Mohammad, A. The effects of vitamin D supplement on the score and quality of sleep in 20-50 year-old people with sleep disorders compared to control group. Nutr. Neurosci. 2018, 21, 511–519. [Google Scholar] [CrossRef]
- Zengin, L.; Aylaz, R. The effects of sleep hygiene education and reflexology on sleep quality and fatigue in patients receiving chemotherapy. Eur. J. Cancer Care 2019, 28, e13020. [Google Scholar] [CrossRef]
- Stein, M.D.; Friedman, P.D. Disturbed sleep and its relationship to alcohol use. Subst. Abus. 2006, 26, 1–13. [Google Scholar] [CrossRef]
- Purani, H.; Friedrichsen, S.; Allen, A.M. Sleep quality in cigarette smokers: Associations with smoking-related outcomes and exercise. Addict. Behav. 2018, 90, 71–76. [Google Scholar] [CrossRef]
- Al Ryalat, S.A.; Kussad, S.; Khatib, O.; Hamad, I.; Al-Tanjy, A.; Alshnneikat, M.; AbuMahfouz, B. Assessing the effect of nicotine dose in cigarette smoking on sleep quality. Sleep Breath. 2012, 25, 1319–1324. [Google Scholar] [CrossRef]
- Wilchens, K.A.; Erickson, K.I.; Wheeler, M.E. Physical activity and cognition: A mediating role of efficient sleep. Behav. Sleep Med. 2018, 16, 569–586. [Google Scholar] [CrossRef] [PubMed]
- Christie, A.D.; Seery, E.; Kent, J.A. Physical activity, sleep quality, and self-reported fatigue across the adult lifespan. Exp. Gerontol. 2016, 77, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Dedhia, P.; Maurer, R. Sleep and health- A lifestyle medicine approach. J. Fam. Pract. 2022, 71, S30–S34. [Google Scholar] [CrossRef]
- Oyetakin-White, P.; Suggs, A.; Koo, B. Does poor sleep quality affect skin aging? Clin. Exp. Dermatol. 2015, 40, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Sundelin, T.; Lekander, M.; Kecklund, G.; Van Sommeren, E.J.; Olsson, A.; Axelsson, J. Cues of fatigue: Effect of sleep deprivation on facial appearance. Sleep 2013, 36, 1355–1360. [Google Scholar] [CrossRef] [PubMed]
- Oliveria, C.; Torres, T. More than skin deep: The systemic nature of atopic dermatitis. Eur. J. Dermatol. 2019, 29, 250–258. [Google Scholar] [CrossRef]
- Xerfan, E.M.S.; Andersen, M.L.; Facina, A.S.; Tufik, S.; Tomimori, J. Rosacea, poor sleep quality, and obstructive sleep apnea: A commentary on potential interconnected features. J. Cosmet. Dermatol. 2022, 21, 4234–4236. [Google Scholar] [CrossRef]
- Mann, C.; Gorai, S.; Staubach-Renz, P.; Goldust, M. Sleep disorders in dermatology-a comprehensive review. JDDG J. Dtsch. Dermatol. Ges. 2023, 21, 577–584. [Google Scholar] [CrossRef]
- Duan, G.Y. Sleep impairment in patients with chronic inflammatory skin diseases: A review of mechanisms and management. J. Am. Acad. Dermatol. 2022, 88, 421–427. [Google Scholar] [CrossRef]
- Afzal, U.M.; Ali, F.R. Sleep deprivation and the skin. Clin. Exp. Dermatol. 2023, 48, 1113–1116. [Google Scholar] [CrossRef]
- Duan, J.; Greenberg, E.N.; Karri, S.S.; Anderson, B. The circadian clock and diseases of the skin. FEBS Lett. 2021, 595, 2413–2436. [Google Scholar] [CrossRef]
- Camilion, J.V.; Khanna, S.; Anasseri, S.; Laney, C.; Mayrovitz, H.N. Physiological, pathological, and circadian factors impacting skin hydration. Cureus 2022, 14, e27666. [Google Scholar] [CrossRef]
- Lyons, A.B.; Moy, L.; Moy, R.; Tung, R. Circadian rhythm and the skin: A review of the literature. J. Clin. Aesthet. Dermatol. 2019, 12, 42–45. [Google Scholar]
- Matsui, M.S.; Pelle, E.; Dong, K.; Pernodet, N. Biological rhythms in the skin. Int. J. Mol. Sci. 2016, 17, 801. [Google Scholar] [CrossRef] [PubMed]
- Pernodet, N.; Pelle, E. Chronobiology of the Skin, Skin Circadian Rhythm and Clock Genes: A New Approach to Slowing Down the Aging Process, 9th ed.; Chemical Publishing: Los Angeles, CA, USA, 2015; Volume 2. [Google Scholar]
- Sarkar, S.; Gaddameedhi, S. UV-B-Induced erythema in human skin: The circadian clock is ticking. J. Investig. Dermatol. 2018, 138, 248–251. [Google Scholar] [CrossRef]
- Nikkola, V.; Miettinen, M.E.; Karisola, P.; Gronroos, M.; Yianttia, L.; Alenius, H.; Snellman, E.; Pateonen, T. Ultraviolet B radiation modifies circadian time in epidermal skin and in subcutaneous adipose tissue. Photodermatol. Photoimmunol. Photomed. 2019, 35, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Farage, M.A. Perceptions of sensitive skin: Changes in perceived severity and associations with environmental causes. Contact Dermat. 2008, 59, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Farage, M.A.; Miller, K.W.; Wippel, A.M.; Berardesca, E.; Misery, L.; Mailbach, H. Sensitive skin in the United States: Survey of regional differences. Fam. Med. Med. Sci. Res. 2013, 2, 3. [Google Scholar]
- Lanuti, E.L.; Kirsner, R.S. Effects of pollution on skin aging. J. Investig. Dermatol. 2010, 130, 2696. [Google Scholar] [CrossRef]
- Vierkötter, A.; Schikowski, T.; Ranft, U.; Sugiri, D.; Matsui, M.; Krämer, U.; Krutmann, J. Airborne particle exposure and extrinsic skin aging. J. Investig. Dermatol. 2010, 130, 2719–2726. [Google Scholar] [CrossRef]
- CDC. Exposome. Available online: https://www.cdc.gov/niosh/topics/exposome/default.html#:~:text=The%20exposome%20can%20be%20defined,%2C%20diet%2C%20lifestyle%2C%20etc (accessed on 22 August 2023).
- Lephart, E.D. Equol’s anti-aging effects protect against environmental assaults by increasing skin antioxidant defense and ECM proteins while decreasing oxidative stress and inflammation. Cosmetics 2018, 5, 16. [Google Scholar] [CrossRef]
- Parrado, C.; Mercado-Saenz, S.; Perez-Davo, A.; Gilaberte, Y.; Gonzalez, S.; Juarranz, A. Environmental stressors on skin aging. Mechanistic insights. Front. Pharm. 2019, 10, 759. [Google Scholar] [CrossRef] [PubMed]
- Passeron, T.; Zouboulis, C.C.; Tan, J.; Andersen, M.L.; Katta, R.; Jyu, X.; Aguilar, L.; Kerob, D.; Morita, A.; Krutmann, J. Adult skin acute stress responses to short-term environmental and internal aggression from exposome factors. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1963–1975. [Google Scholar] [CrossRef] [PubMed]
- Reis-Mansur, M.C.P.; Goncalves da Luz, B.; Pereira dos Santos, E. Consumer behavior, skin phototype, sunscreens, and tools for photoprotection: A review. Cosmetics 2023, 10, 39. [Google Scholar] [CrossRef]
- Suozzi, K.; Turban, J.; Girardi, M. Cutaneous photoprotection: A review of the current status and evolving strategies. Yale J. Biol. Med. 2020, 93, 55–67. [Google Scholar]
- Pethank, N.; Pollard, K.J. Lifestyle medicine prescriptions for personal and planetary health. J. Clim. Change Health 2021, 4, 100077. [Google Scholar] [CrossRef]
- Ferro de Oliveira, C.S.; Tavaria, F.K. The impace of bioactive textiles on human skin microbiota. Eur. J. Pharm. Biopharm. 2023, 188, 66–77. [Google Scholar] [CrossRef]
- Farkas, A.; Farkes, G. Effects of spaceflight on human skin. Skin Pharm. Physiol. 2021, 34, 239–245. [Google Scholar] [CrossRef]
- Qui, Y.; Ferandez-Garcia, B.; Lehmann, H.I.; Li, G.; Kroemer, G.; Lopez-Otin, C.; Ziao, J. Exercise sustains the hallmarks of health. J. Sports Health Sci. 2023, 12, 8–35. [Google Scholar]
- Ruegsegger, G.N.; Booth, F.W. Health benefits of exercise. Cold-Spring Harb. Perspect. Med. 2018, 8, a029694. [Google Scholar] [CrossRef]
- Giacomello, M.; Pyakurel, A.; Glytsou, C.; Scorrano, L. The cell biology of mitochondrial membrane dynamics. Nat. Rev. Mol. Biol. 2020, 21, 204–224. [Google Scholar] [CrossRef] [PubMed]
- Yeb, C.; Flately, E.; Elkattawy, O.; Berger, L.; Rao, B. Exercise in dermatology: Exercise’s influence on skin aging, skin cancer, psoriasis, venous ulcers, androgenetic alopecia. J. Am Acad. Dermatol. Res. Lett. 2022, 87, 183–184. [Google Scholar]
- Ryosuke, O.; Yoshie, S.; Hiromi, A. The association between activity levels and skin moisturizing function in adults. Dermatol. Rep. 2021, 13, 8811. [Google Scholar]
- Franca, K.; Lotti, T. (Eds.) Advances in Integrative Dermatology; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- United States Environmental Protection Agency (EPA). Ultraviolet (UV) Radiation and Sun Exposure. Available online: https://www.epa.gov/radtown/ultraviolet-uv-radiation-and-sun-exposure (accessed on 21 August 2023).
- Leigh-Hunt, N.; BAgguley, D.; Bash, K.; Tirner, V.; Turnbull, S.; Valtorta, N.; Cann, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef]
- Cene, C.W.; Beckie, T.M.; Sims, M.; Suglia, S.F.; Aggarwal, B.; Moise, N.; Jimenez, M.C.; Gaye, B.; McCullough, L.D. Effects of objective and perceived social isolation on cardiovascular and brain health: A scientific statement from the American Heart Association. J. Am. Heart Assoc. 2022, 11, e026493. [Google Scholar] [CrossRef]
- Cudjoe, T.K.M.; Selvakumar, S.; Chung, S.-E.; Latkin, C.A.; Roth, D.L.; Thorpe, R.J.; Boyd, C.M. Getting under the skin: Social isolation and biological markers in the National Health and Aging trend study. J. Am. Geriatr. Soc. 2022, 70, 408–414. [Google Scholar] [CrossRef]
- Kottner, J.; Fastner, A.; Lintzeri, D.-A.; Griffths, C.E.M.; Blume-Peytavi, U. Improving skin health of community-dwelling older people: A scoping review protocol. BMJ Open 2023, 13, E071313. [Google Scholar] [CrossRef]
- Usgu, S.; Akinci, B.; Bali, K. Complementary therapies for women with body image issues. Anti-Aging East. Eur. 2023, 2, 97–108. [Google Scholar] [CrossRef]
- Rapaport, M.H.; Schettler, P.; Bresee, C. A preliminary study of the effects of repeated massage on hypothalamic-pituitary-adrenal and immune function in healthy individuals: A study of mechanisms of action and dosage. J. Altern. Comp. Med. 2012, 8, 789–797. [Google Scholar] [CrossRef]
- Almutairi, N.; Schwartz, R.A. COVID-19 with dermatologic manifestations and implications: An unfolding conundrum. Dermatol. Ther. 2020, 33, e13544. [Google Scholar] [CrossRef]
- Afshar, Z.M.; Babaxadeh, A.; Hasanpour, A.; Barray, M.; Sayad, S.; Janbakhsh, A.; Aryanian, Z.; Ebrahimpour, S. Dermatological manifestations associated with COVID-19: A comprehensive review of the current knowledge. J. Med. Virol. 2021, 93, 5756–5767. [Google Scholar] [CrossRef] [PubMed]
- Mangini, C.S.M.; Farias de Vaconcelos, R.C.; Rodriguez, E.V.R.; Lorenzon de Oliveira, I.R. Social isolation: Main dermatosis and impact of stress during the COVID-19 pandemic. Einstein 2022, 20, eAO6320. [Google Scholar] [CrossRef] [PubMed]
- Flandroy, L.; Poutadhidis, T.; Berg, G.; Clakrke, G.; Dao, M.-C.; Decaestecker, E.; Furman, E.; Haahtela, T.; Massart, S.; Plovier, H.; et al. The impact of human activities and lifestyle on the interlinked microbiota and health of humans and of ecosystems. Sci. Total Environ. 2018, 627, 1018–1038. [Google Scholar] [CrossRef]
- Umberson, D.; Montez, J.K. Social relationships and health: A flashpoint for health policy. J. Health Soc. Behav. 2010, 51, S54–S66. [Google Scholar] [CrossRef]
- Petkovic, J.; Duench, S.; Trawin, J.; Dewidar, O.; Pardo, J.; Simeon, R.; DesMeules, M.; Gagnon, D.; Robert, H.; Hossain, A.; et al. Behavioural interventions delivered through interactive social media for health behaviour change, health outcomes, and health equity in the adult population. Cochrane Database Syst. Rev. 2021, 31, CD012932. [Google Scholar]
- White, N.D.; Bautista, V.; Lenz, T.; Cosimano, A. Using the SMART-EST goals in lifestyle medicine prescription. Am. J. Lifestyle Med. 2020, 14, 271–273. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Cartoon Structure/Component(s)/Layers of Human Skin. Note: the stratum lucidum is not shown because it is only found on the palms of the hands and soles of the feet.
Figure 1.
Cartoon Structure/Component(s)/Layers of Human Skin. Note: the stratum lucidum is not shown because it is only found on the palms of the hands and soles of the feet.

Figure 2.
Chronological aging via the loss of skin homeostasis/oxidative metabolism, photo-aging by exposure to UV light and extrinsic aging (due to external factors and lifestyle) through cellular/molecular signaling mechanisms are shown. This diagram displays the sequence or production of reactive oxygen species (ROS) that is more commonly called oxidative stress (OS). Oxidative stress (OS) in the major factor associated with inflammation and alterations in the decline of collagen and elastin resulting in wrinkles. Abbreviations: Proinflammatory transcript factor (NFkB), AP-1 nuclear transcription element, Activator Protein—1 (AP-1), hyaluronic acid (HA), Tissue Inhibitor of Matrix Metallo-proteinase (TIMP) and Transforming Growth Factor beta (TGFβ). Estrogens and Selective Estrogen Receptor Modulators (SERMs) provide protection by binding especially to estrogen receptor (β) in chronological, photo-aging, and extrinsic aging. Adapted with permission from Lephart E.D. Naftolin, F. Factors Influencing Skin Aging and the Important Role Estrogens and Selective Estrogen Modulators (SERMs). Clin. Cosmet. Invest. Dermatol. 2022, 15, 1695–1709 [2].
Figure 2.
Chronological aging via the loss of skin homeostasis/oxidative metabolism, photo-aging by exposure to UV light and extrinsic aging (due to external factors and lifestyle) through cellular/molecular signaling mechanisms are shown. This diagram displays the sequence or production of reactive oxygen species (ROS) that is more commonly called oxidative stress (OS). Oxidative stress (OS) in the major factor associated with inflammation and alterations in the decline of collagen and elastin resulting in wrinkles. Abbreviations: Proinflammatory transcript factor (NFkB), AP-1 nuclear transcription element, Activator Protein—1 (AP-1), hyaluronic acid (HA), Tissue Inhibitor of Matrix Metallo-proteinase (TIMP) and Transforming Growth Factor beta (TGFβ). Estrogens and Selective Estrogen Receptor Modulators (SERMs) provide protection by binding especially to estrogen receptor (β) in chronological, photo-aging, and extrinsic aging. Adapted with permission from Lephart E.D. Naftolin, F. Factors Influencing Skin Aging and the Important Role Estrogens and Selective Estrogen Modulators (SERMs). Clin. Cosmet. Invest. Dermatol. 2022, 15, 1695–1709 [2].

Figure 3.
(A) Upper Panel displays the progressive decrease in dermal collagen and elastin fibers and the appearance of fine lines and wrinkles with the passage of time. (B) Lower Panel displays the levels of ovarian 17β-estradiol levels (red histogram bars) in women from the late teenage years to seventy years of age. After menopause the low estrogen levels (not shown) are derived from the aromatization of androgens in peripheral fat tissue sites. The profile of collagen expression in skin with aging is displayed (green histogram bars) while the elastin levels (blue histogram bars) follow the pattern of ovarian estrogen production with aging. Adapted with permission from Lephart E.D. Naftolin, F. Factors Influencing Skin Aging and the Important Role Estrogens and Selective Estrogen Modulators (SERMs). Clin. Cosmet. Invest. Dermatol. 2022, 15, 1695–1709 [2].
Figure 3.
(A) Upper Panel displays the progressive decrease in dermal collagen and elastin fibers and the appearance of fine lines and wrinkles with the passage of time. (B) Lower Panel displays the levels of ovarian 17β-estradiol levels (red histogram bars) in women from the late teenage years to seventy years of age. After menopause the low estrogen levels (not shown) are derived from the aromatization of androgens in peripheral fat tissue sites. The profile of collagen expression in skin with aging is displayed (green histogram bars) while the elastin levels (blue histogram bars) follow the pattern of ovarian estrogen production with aging. Adapted with permission from Lephart E.D. Naftolin, F. Factors Influencing Skin Aging and the Important Role Estrogens and Selective Estrogen Modulators (SERMs). Clin. Cosmet. Invest. Dermatol. 2022, 15, 1695–1709 [2].

Figure 4.
Effects and Benefits of 17β-Estradiol on Skin. Adapted, in part, from VectorStock license 3,264,406 to ED Lephart.
Figure 4.
Effects and Benefits of 17β-Estradiol on Skin. Adapted, in part, from VectorStock license 3,264,406 to ED Lephart.

Figure 5.
Other Hormonal Influences on Skin.

Figure 6.
The World’s Oldest Populations. Only includes countries/territories with a population of more than 1 million people. Source: United Nations Population Division [60]. Adapted with permission.
Figure 6.
The World’s Oldest Populations. Only includes countries/territories with a population of more than 1 million people. Source: United Nations Population Division [60]. Adapted with permission.

Figure 7.
Comparison Among Mediterranean, Western and Eastern (Asian) Diets. Adapted with permission from Stewart, K.L.; Lephart, E.D. Overview of BPH: Symptom relief with dietary polyphenols, vitamins, and phytochemicals by nutraceutical supplements with implications to the prostate microbiome. Internat. J. Mole. Sci. 2023, 24, 5486. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24065486 [75].
Figure 7.
Comparison Among Mediterranean, Western and Eastern (Asian) Diets. Adapted with permission from Stewart, K.L.; Lephart, E.D. Overview of BPH: Symptom relief with dietary polyphenols, vitamins, and phytochemicals by nutraceutical supplements with implications to the prostate microbiome. Internat. J. Mole. Sci. 2023, 24, 5486. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms24065486 [75].

Figure 8.
The fluctuation of human skin characteristics as they cycle from day to night in a circadian pattern [170]. Adapted with permission from, Pernodet, N.; Pelle, E. Chronobiology of the Skin, Skin Circadian Rhythm and Clock Genes: A New Approach to Slowing Down the Aging Process, 9th ed.; Chemical Publishing. Los Angeles, CA, USA, 2015, Volume 2.
Figure 8.
The fluctuation of human skin characteristics as they cycle from day to night in a circadian pattern [170]. Adapted with permission from, Pernodet, N.; Pelle, E. Chronobiology of the Skin, Skin Circadian Rhythm and Clock Genes: A New Approach to Slowing Down the Aging Process, 9th ed.; Chemical Publishing. Los Angeles, CA, USA, 2015, Volume 2.

Figure 9.
Summary of Enhancing Skin Anti-Aging Through Healthy Lifestyle Factors.


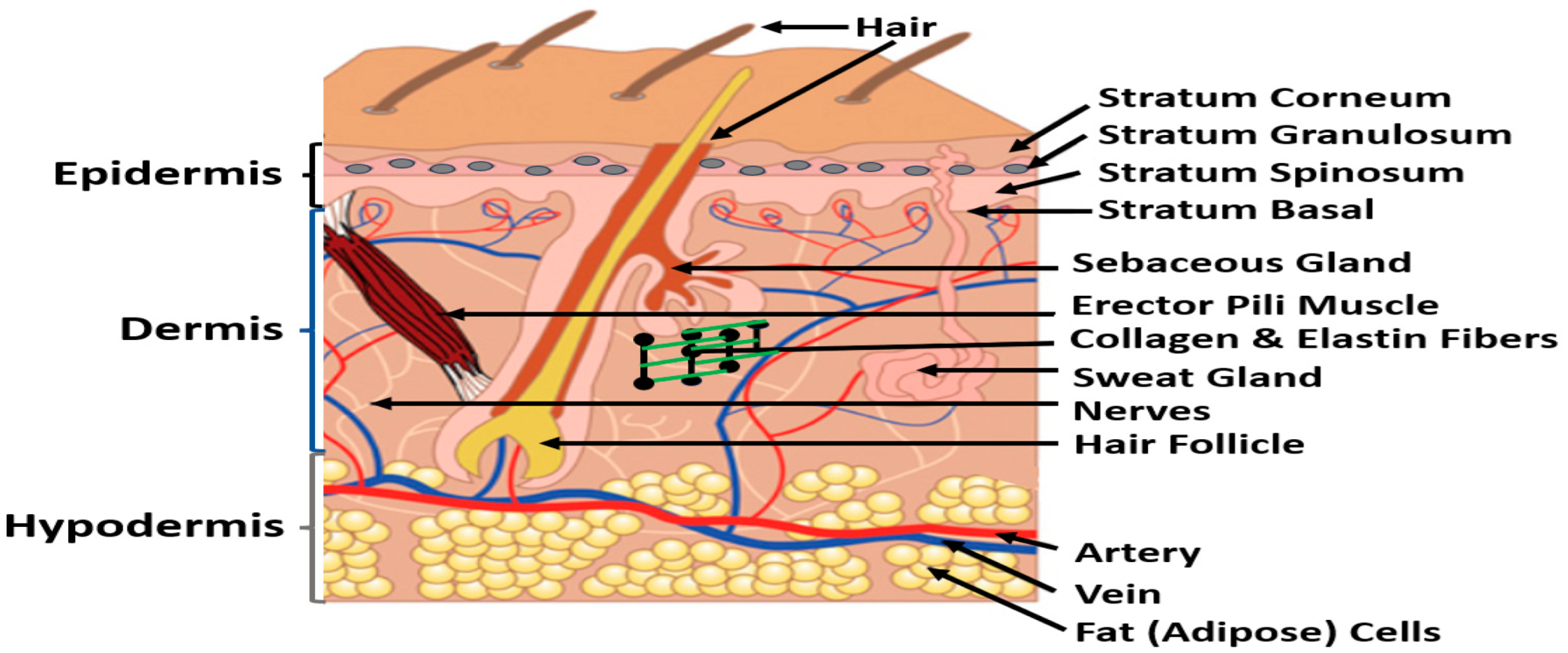{kind=link}
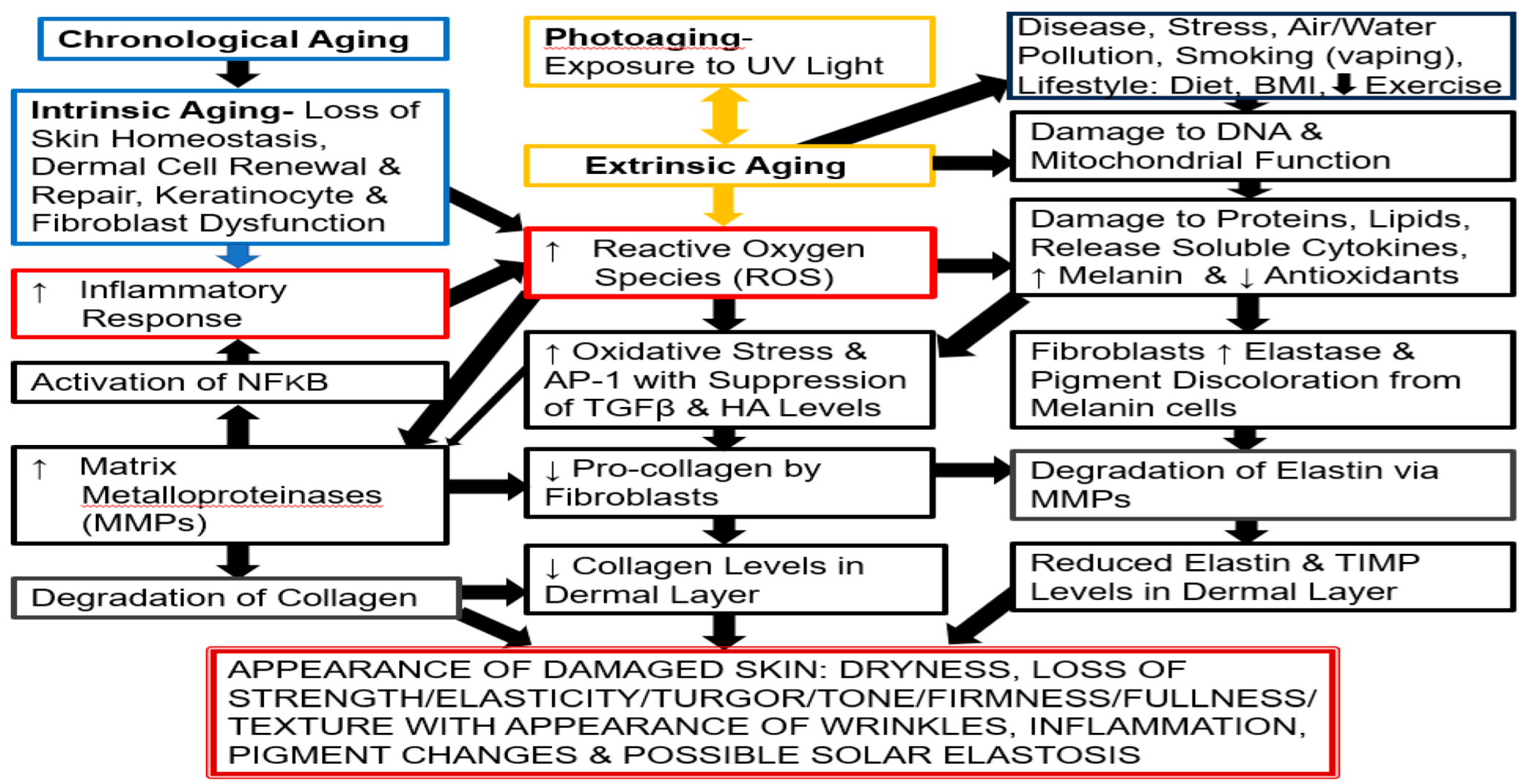{kind=link}
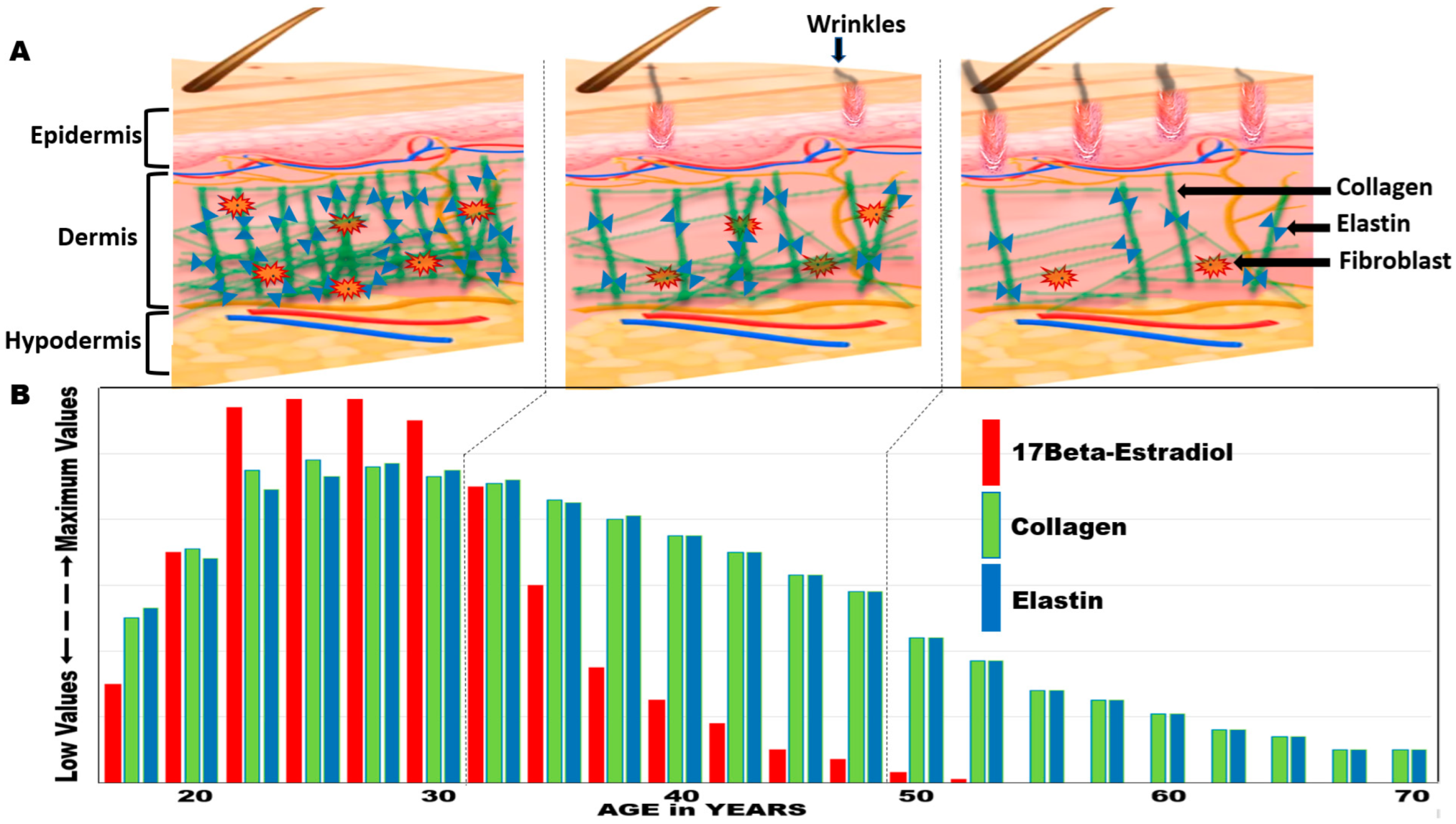{kind=link}
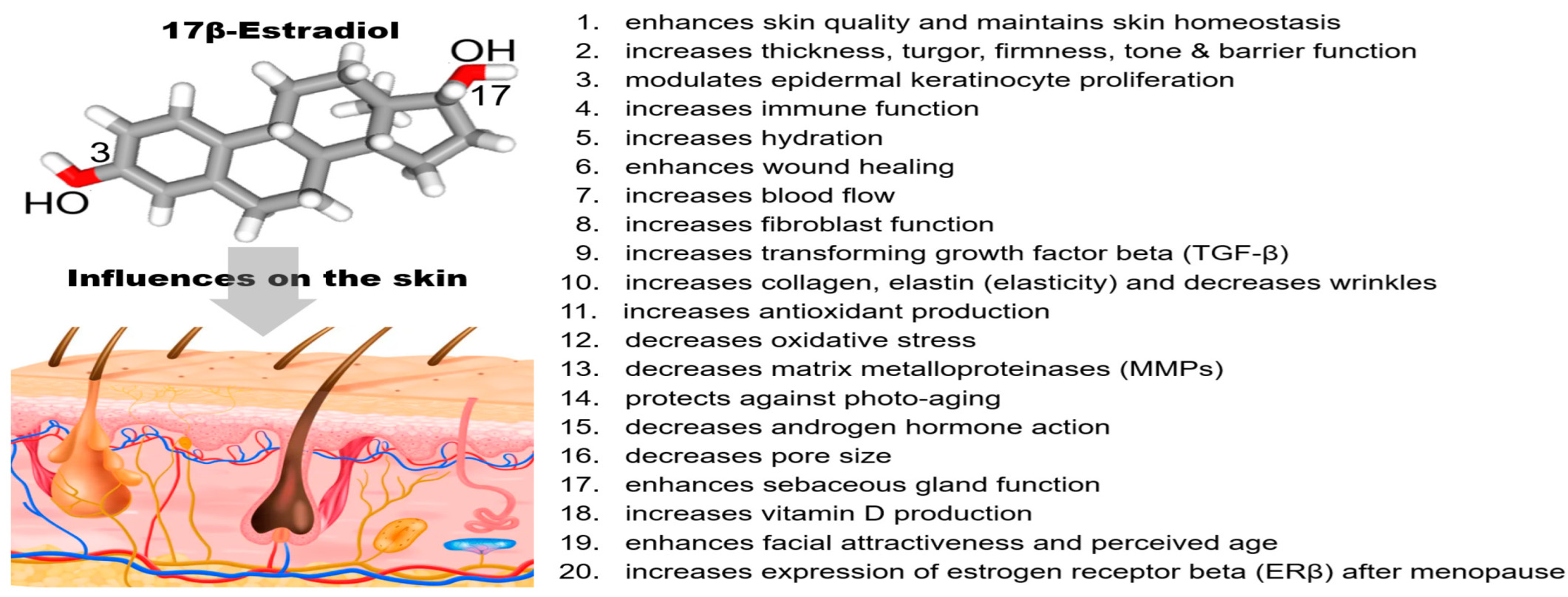{kind=link}
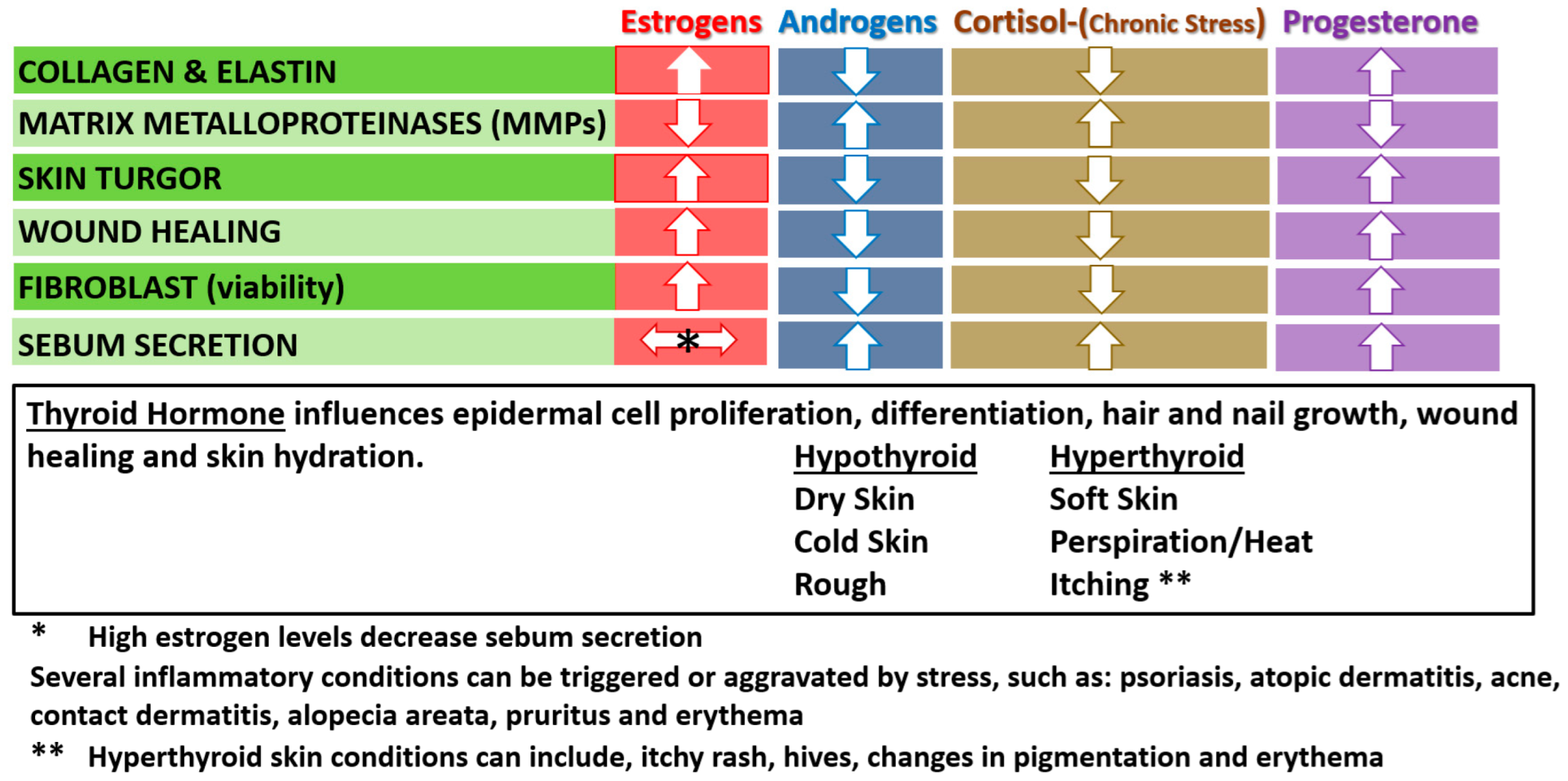{kind=link}
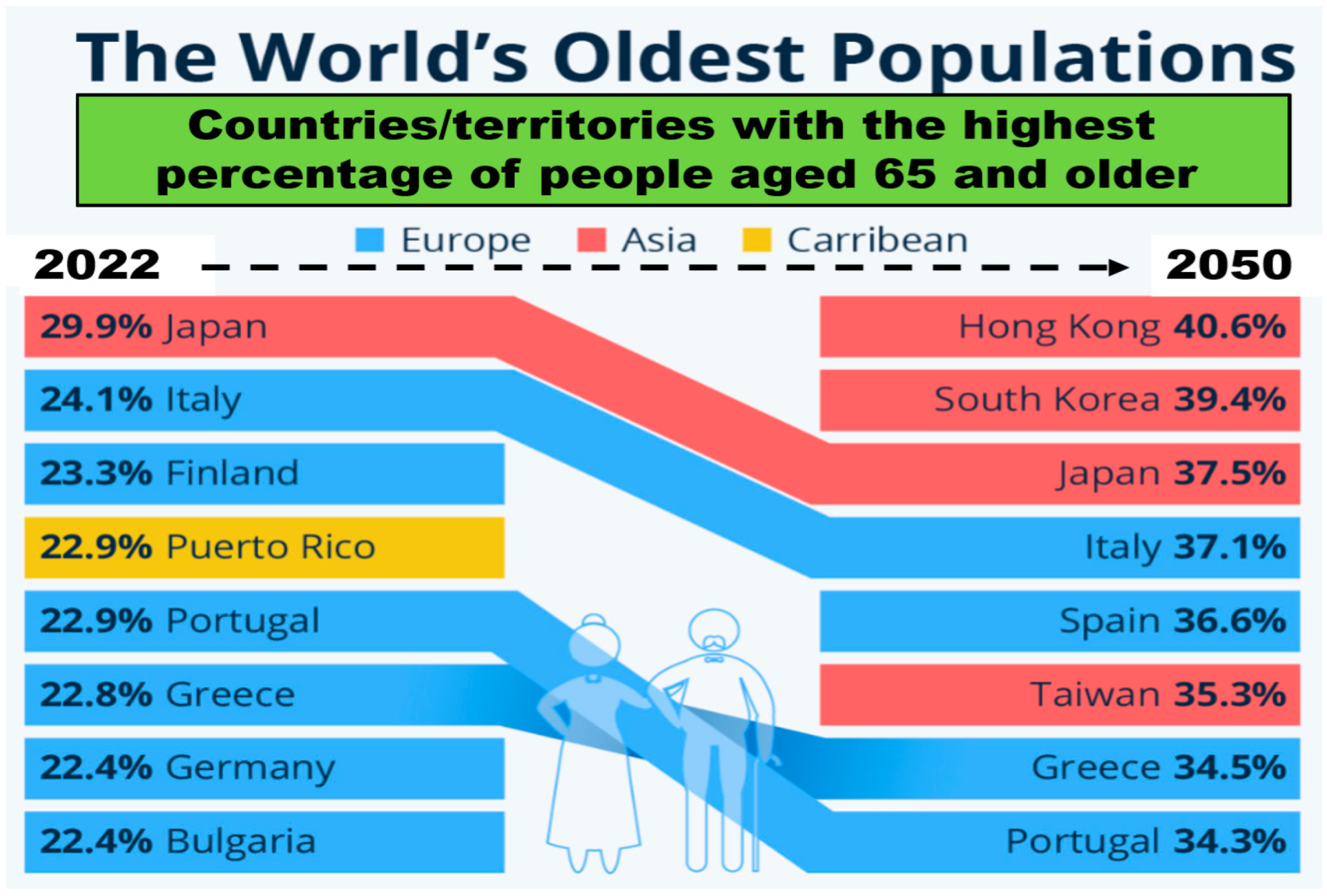{kind=link}
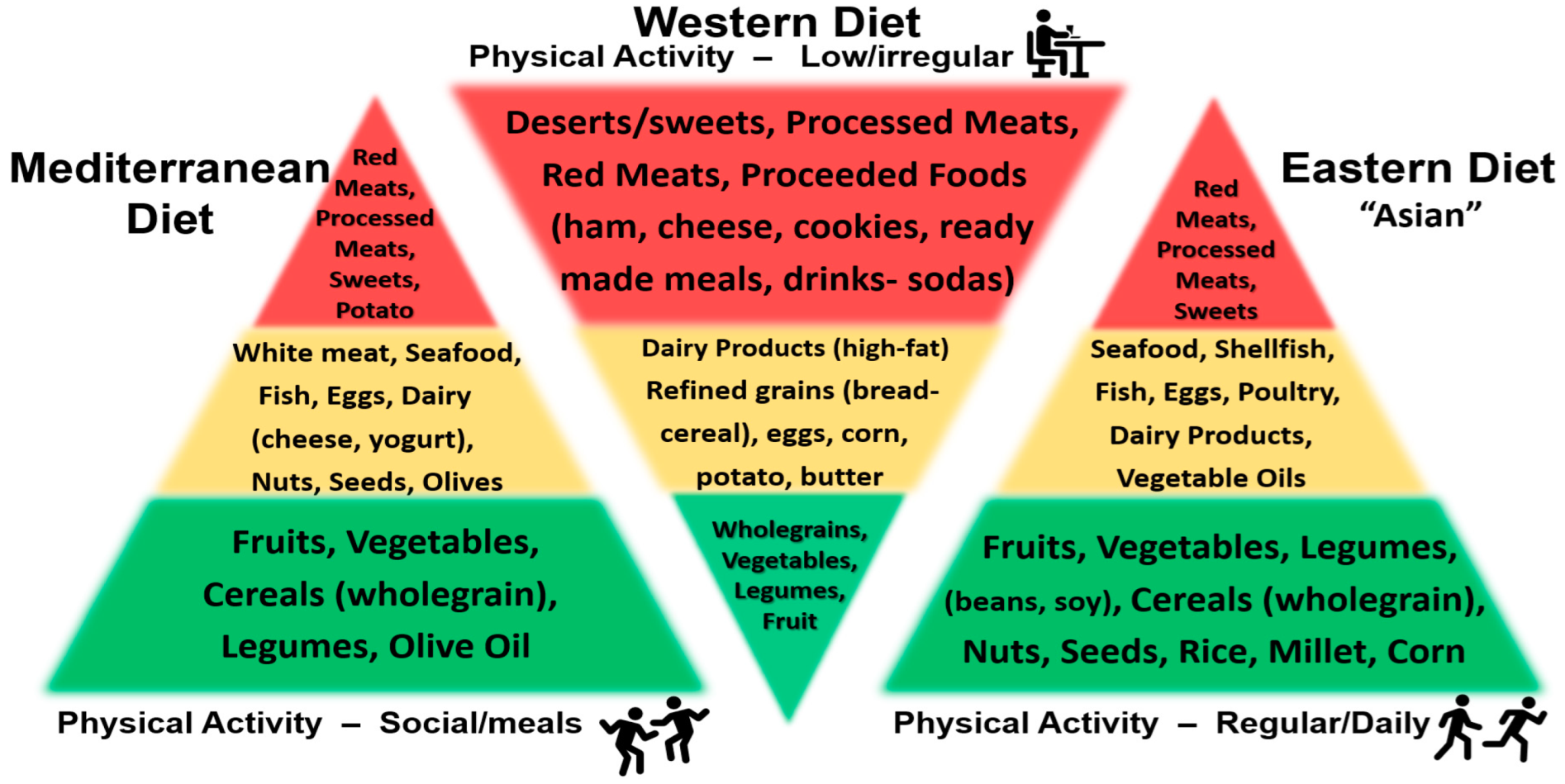{kind=link}
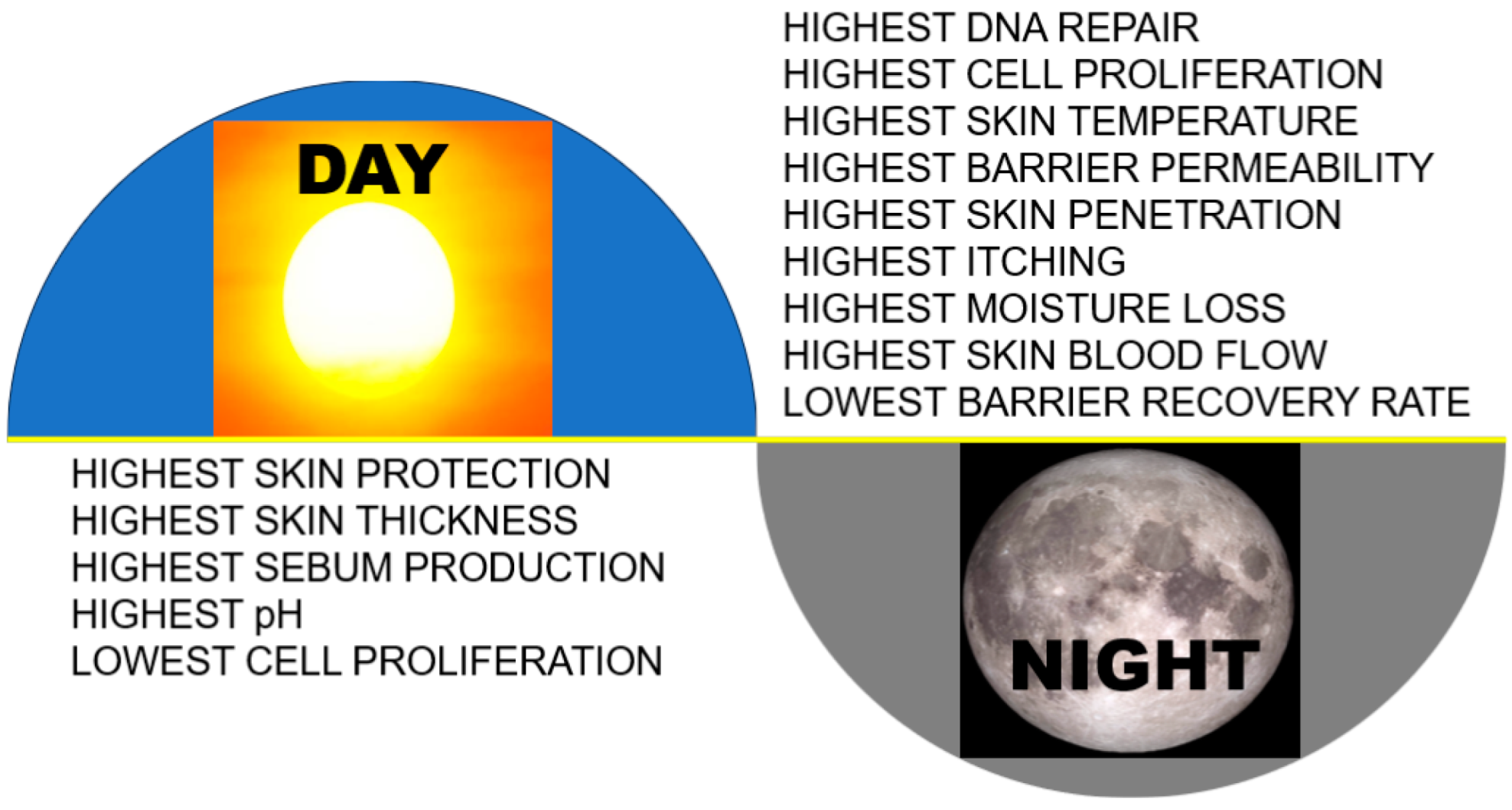{kind=link}
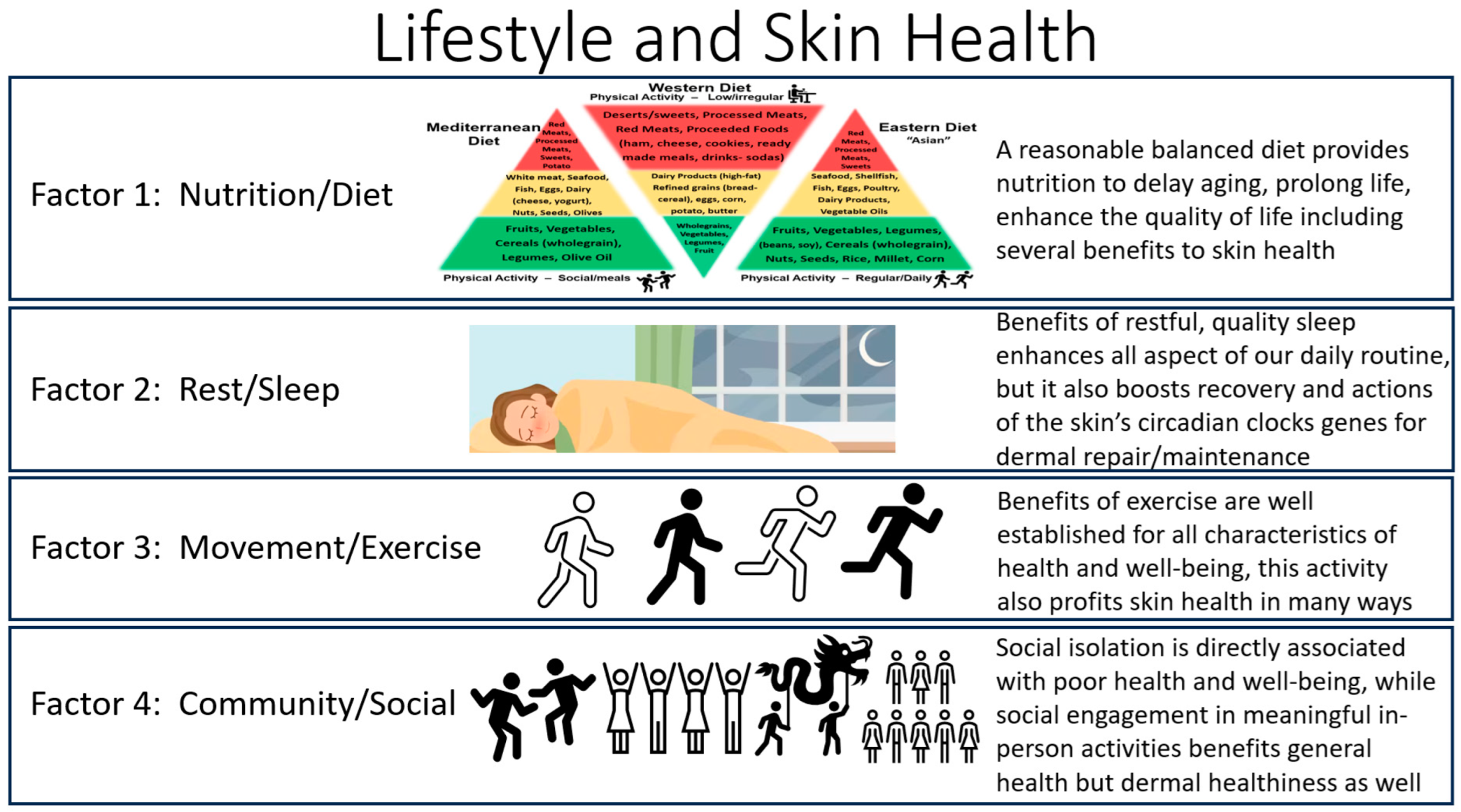{kind=link}
Table 1.
Summary of Key Nutrients/Vitamins/Dietary Intake and Other Factors Influencing Skin Aging.
| Nutrient/Diet/Habit | Influence on Skin Health | Reference |
|---|---|---|
| Water | skin hydration-biomechanics | [2,22,84,85] |
| Proteins | support/repair, extracellular matrix (collagen/elastin) | [88,90,91,92] |
| Trace Elements | ||
| Copper | extracellular matrix/angiogenesis | [89,94,95] |
| Iron | wound healing/antioxidant capacity | [89,94,95] |
| Selenium | keratinocyte function/antioxidant function | [88] |
| Zinc | /development-keratinocytes | [88] |
| Vitamins and Other Compounds | ||
| A | aging, improves wrinkles, stimulates dermis | [89,93,94,95] |
| B-Complex (below) | [88,89,94,95] | |
| B1 (thiamine) | hydration/anti-inflammatory | |
| B2 (riboflavin) | skin tone/radiant balance | |
| B3 (niacinamide) | keratin/barrier function | |
| B5 (pantothenic acid) | hydration/wound healing/anti-inflammatory | |
| B6 (pyridoxine) | anti-inflammatory/skin balance | |
| B7 (biotin) | if deficiency-improves skin, hair/nails | |
| B9 (folate) | skin support/tone/turgor | |
| B12 (cobalamin) | collagen/hydration, anti-inflammatory, deficiency-hyperpigmentation | |
| C | antioxidant/boost collagen/hydration | [89,93,94,95] |
| D | anti-inflammatory, skin protectant | [89,93,94,95] |
| E | antioxidant, anti-aging, improves wrinkles | [89,93,94,95] |
| Dietary Intake/Supplementation | ||
| Coenzyme Q 10 (CoQ10) | antioxidant (↓ oxidative stress), enhance vitamin E | [88] |
| Collagen peptides | boost collagen and elasticity (skin, hair, nails) | [88,90,91,92] |
| Carotenoids | antioxidant, increases collagen, elastin, | |
| Astaxanthin, Lutein | reduces appearance of wrinkles by inhibiting | |
| Zeaxanthin, Lycopene | oxidative stress and MMPs | [88,97,98,99,100,101] |
| Chlorophyll | antioxidant/anticancer | [102] |
| Polyphenols | antioxidant, anti-inflammatory, boost collagen and | |
| Resveratrol, Flavonoids, | elastin, TIMP, SOD, Nrf2, inhibits oxidative stress, | |
| Isoflavonoids, Green Tea, etc. | NFkappKB, Matrix Metalloproteinases (MMPs) | [8,36,50,75,96,98,99,100,101] |
| Probiotics | reduces oxidative stress and photoaging | [104,105,106] |
| Daily Habits/Negative Impact | ||
| Advanced Glycation | toxins causing skin damage | |
| End Products (AGEs) | skin inflammation/stiffening | [114,115] |
| Alcohol | dehydration/inflammation decrease skin barrier | [115,116,125] |
| Smoking (vaping) | damage skin/skin aging many negative influences | [125,126] |
| High Fat | skin inflammation/damage/infections | [83,134,135,136,137] |
| Increased BMI (Obesity) | skin inflammation/damage/infections | [83,134,135,136,137] |
Table 2.
Factors Influencing Sleep Quality.
| Factors Improving Sleep Quality | Factors Deteriorating Sleep Quality | References | |
|---|---|---|---|
| Diet | |||
| Balanced diet | Intake of inflammatory foods (sugar, alcohol, etc.) | [146,147] | |
| Carbohydrates | Low-carb diet and High-carb diet (>70% energy) | [146,147] | |
| Fats | Polyunsaturated Fatty Acids (PUFA) | Saturated Fatty Acids | [146,148] |
| (omega-3 > than omega-6 fatty acids) | Trans Fats | [146,148] | |
| Proteins | Appropriate intake of proteins | Too Low Protein or Too High Protein Intake; | |
| Red Meats and Processed Meats | [146,149] | ||
| Other Factors: | |||
| Caffeine (chocolate, coffee, tea, energy drinks) | [146,150] | ||
| Adequate Vitamin D Levels | Low Vitamin D Levels | [151] | |
| Alcohol (beer, wine, etc.) | [152,153] | ||
| Nicotine (cigarettes, chewing gum, e-cigarettes) | [154,155] | ||
| Regular Physical Exercise | Lack of exercise or obesity | [156,157] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Knaggs, H.; Lephart, E.D. Enhancing Skin Anti-Aging through Healthy Lifestyle Factors. Cosmetics 2023, 10, 142. https://0-doi-org.brum.beds.ac.uk/10.3390/cosmetics10050142
AMA Style
Knaggs H, Lephart ED. Enhancing Skin Anti-Aging through Healthy Lifestyle Factors. Cosmetics. 2023; 10(5):142. https://0-doi-org.brum.beds.ac.uk/10.3390/cosmetics10050142
Chicago/Turabian StyleKnaggs, Helen, and Edwin D. Lephart. 2023. "Enhancing Skin Anti-Aging through Healthy Lifestyle Factors" Cosmetics 10, no. 5: 142. https://0-doi-org.brum.beds.ac.uk/10.3390/cosmetics10050142
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.