
JAK2 Phosphorylation Signals and Their Associated Cytokines Involved in Chronic Rhinosinusitis with Nasal Polyps and Correlated with Disease Severity

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Symptom Severity Assessment
2.2. Measurement of Cytokines
2.3. Enzyme-Linked Immunosorbent Assay
2.4. Tissue Microarray
2.5. Statistical Analysis
3. Results
3.1. Patient Demographics
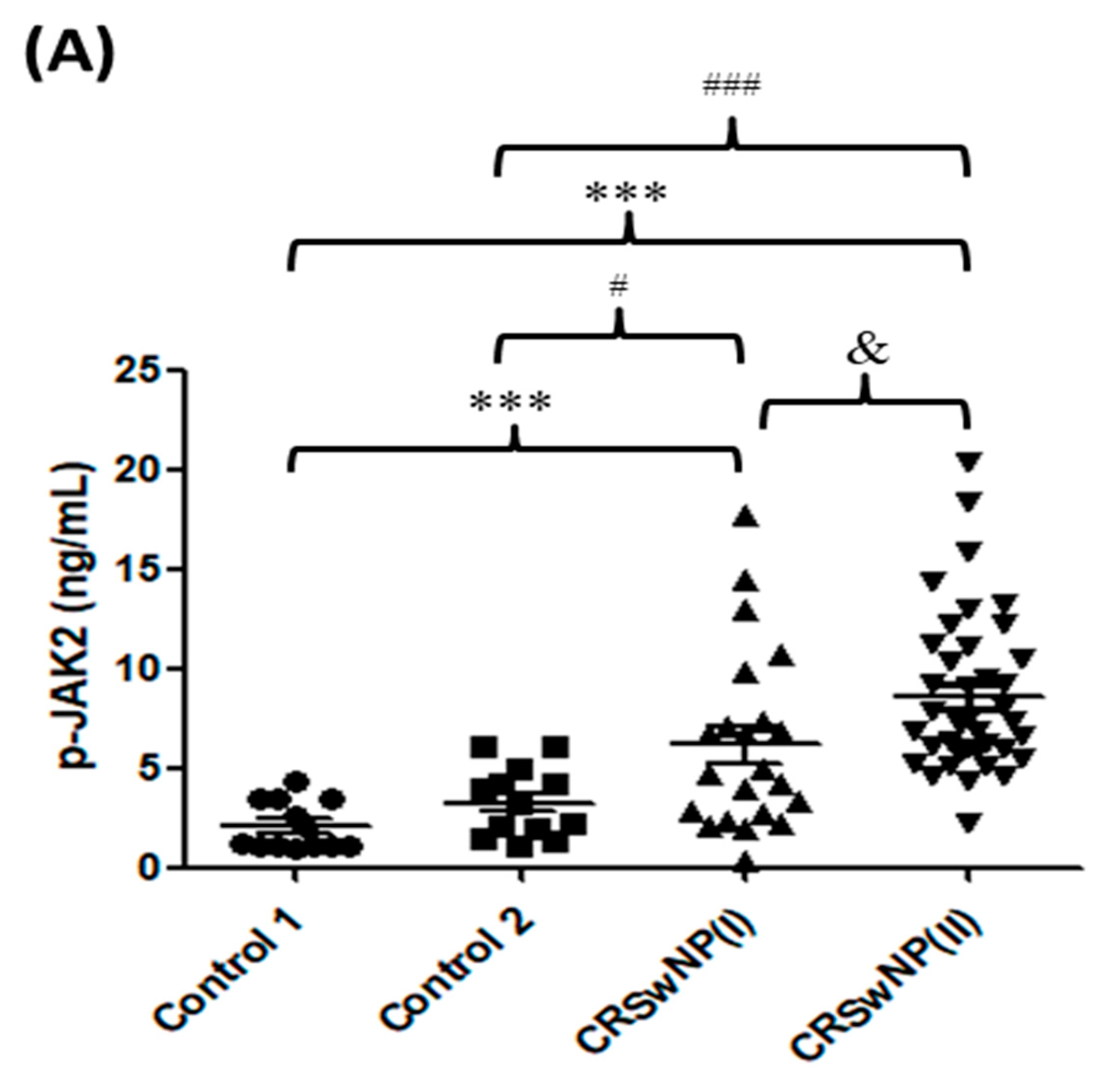
3.2. p-JAK2 Level and JAK2-Associated Cytokines in CRS
3.3. p-JAK2 and JAK2-Associated Cytokines Are Correlated with Disease Severity
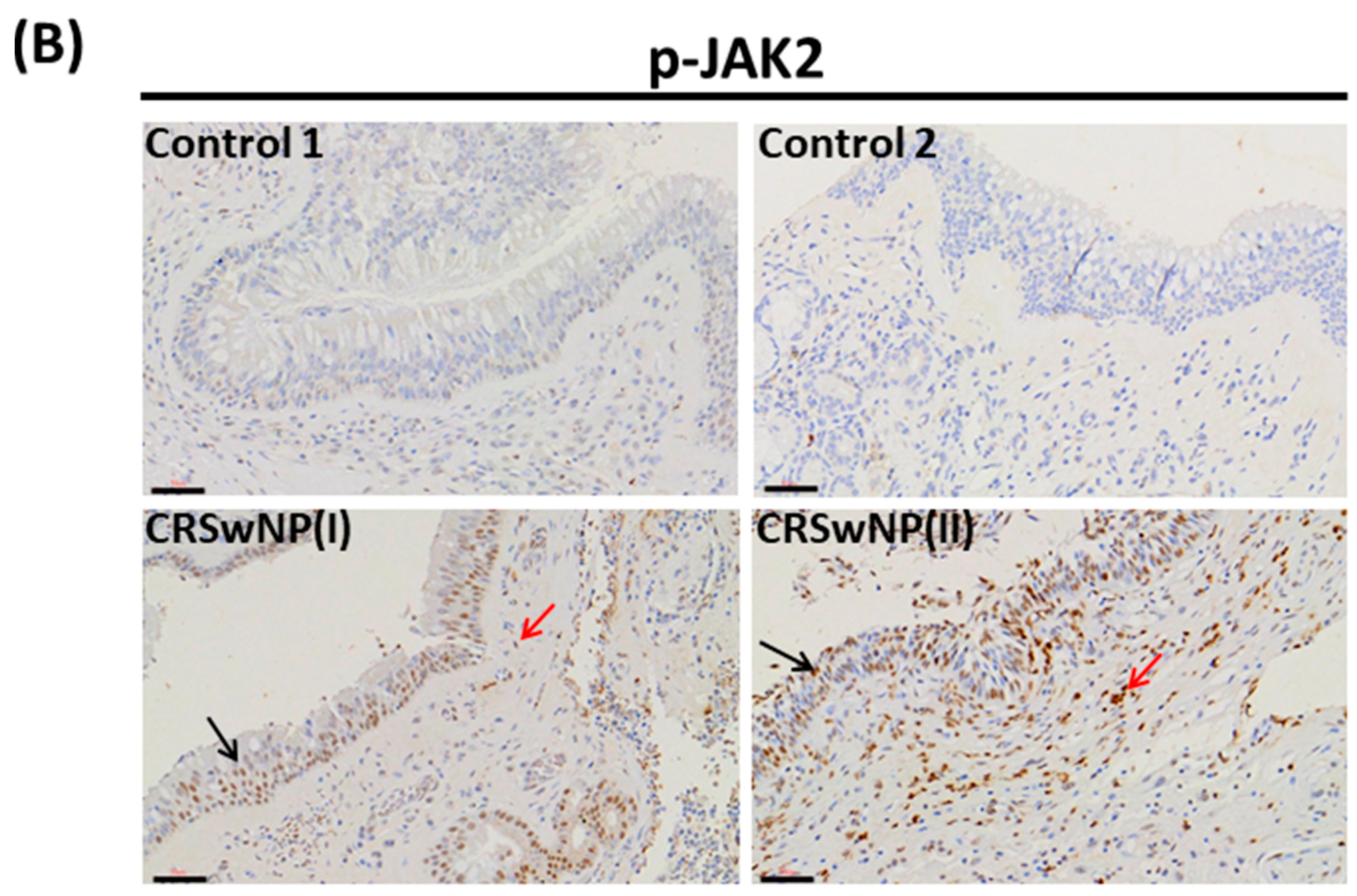
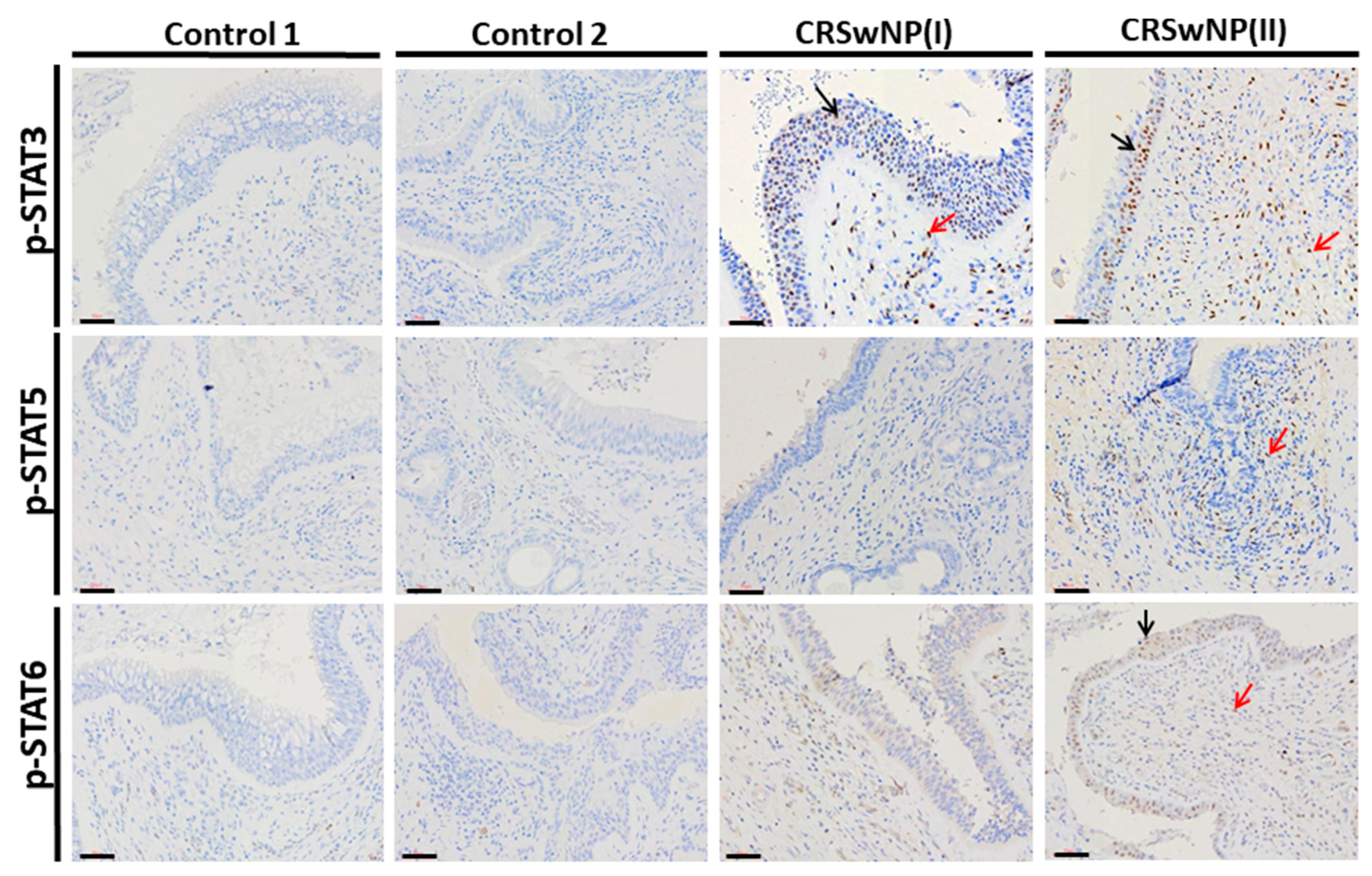
3.4. JAK2/STATs Phosphorylation Signaling in Nasal Polyps
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosenfeld, R.M.; Piccirillo, J.F.; Chandrasekhar, S.S.; Brook, I.; Kumar, K.A.; Kramper, M.; Orlandi, R.R.; Palmer, J.N.; Patel, Z.M.; Peters, A.; et al. Clinical practice guideline (update): Adult sinusitis. Otolaryngol. Head. Neck. Surg. 2015, 152, S1–S39. [Google Scholar] [CrossRef] [Green Version]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. EPOS 2020: European position paper on rhinosinusitis and nasal polyps 2020. Rhinology 2020, 58 (Suppl. S29), 1–464. [Google Scholar] [CrossRef]
- Smith, K.A.; Orlandi, R.R.; Rudmik, L. Cost of adult chronic rhinosinusitis: A systematic review. Laryngoscope 2015, 125, 1547–1556. [Google Scholar] [CrossRef] [PubMed]
- Liao, B.; Liu, J.X.; Li, Z.Y.; Zhen, Z.; Cao, P.P.; Yao, Y.; Long, X.B.; Wang, H.; Wang, Y.; Schleimer, R.; et al. Multidimensional endotypes of chronic rhinosinusitis and their association with treatment outcomes. Allergy 2018, 73, 1459–1469. [Google Scholar] [CrossRef]
- Wang, P.C.; Tai, C.J.; Lin, M.S.; Chu, C.C.; Liang, S.C. Quality of Life in Taiwanese Adults with Chronic Rhino-Sinusitis. Qual. Life. Res. 2003, 12, 443–448. [Google Scholar] [CrossRef]
- Barnes, P.J. Kinases as Novel Therapeutic Targets in Asthma and Chronic Obstructive Pulmonary Disease. Pharmacol. Rev. 2016, 68, 788–815. [Google Scholar] [CrossRef] [Green Version]
- Pernis, A.B.; Rothman, P.B. JAK-STAT signaling in asthma. J. Clin. Investig. 2002, 109, 1279–1283. [Google Scholar] [CrossRef] [PubMed]
- Tudhope, S.J.; Catley, M.C.; Fenwick, P.S.; Russell, R.E.K.; Rumsey, W.L.; Newton, R.; Barnes, P.J.; Donnelly, L.E. The role of IkappaB kinase 2, but not activation of NF-kappaB, in the release of CXCR3 ligands from IFN-γ-stimulated human bronchial epithelial cells. J. Immunol. 2007, 179, 6237–6245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Stefano, A.; Caramori, G.; Capelli, A.; Gnemmi, I.; Ricciardolo, F.L.; Oates, T.; Donner, C.F.; Chung, K.F.; Barnes, P.J.; Adcock, I.M. STAT4 activation in smokers and patients with chronic obstructive pulmonary disease. Eur. Respir. J. 2004, 24, 78–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yew-Booth, L.; Birrell, M.A.; Lau, M.S.; Baker, K.; Jones, V.; Kilty, I.; Belvisi, M.G. JAK-STAT pathway activation in COPD. Eur. Respir. J. 2015, 46, 843–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linke, R.; Pries, R.; Könnecke, M.; Bruchhage, K.L.; Böscke, R.; Gebhard, M.; Wollenberg, B. Increased phosphorylation of STAT5b, but not STAT5a, in nasal polyps. Am. J. Rhinol. Allergy 2015, 29, 182–187. [Google Scholar] [CrossRef]
- Kariyawasam, H.H.; James, L.K.; Gane, S.B. Dupilumab: Clinical efficacy of blocking IL-4/IL-13 signalling in chronic rhinosinusitis with nasal polyps. Drug Des. Devel. Ther. 2020, 14, 1757–1769. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Van Zele, T.; Perez-Novo, C.; Bruaene, N.V.; Holtappels, G.; DeRuyck, N.; Cauwenberge, P.V.; Bachert, C. Different types of T effector cells orchestrate mucosal inflammation in chronic sinus disease. J. Allergy Clin. Immunol. 2008, 122, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Chao, P.Z.; Chou, C.M.; Chen, C.H. Plasma RANTES and eotaxin levels are correlated with the severity of chronic rhinosinusitis. Eur. Arch. Otorhinolaryngol. 2012, 269, 2343–2348. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Gevaert, E.; Lou, H.; Wang, X.; Zhang, L.; Bachert, C.; Zhang, N. Chronic rhinosinusitis in Asia. J. Allergy. Clin. Immunol. 2017, 140, 1230–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lund, V.J.; Kennedy, D.W. Quantification for staging sinusitis. International Conference on Sinus Disease: Terminology, Staging, Therapy. Ann. Otol. Rhinol. Laryngol. Suppl. 1995, 104, 17–21. [Google Scholar]
- Lund, V.J.; Mackay, I.S. Staging in rhinosinusitus. Rhinology 1993, 31, 183–184. [Google Scholar] [PubMed]
- Meltzer, E.O.; Hamilos, D.L.; Hadley, J.A.; Lanza, D.C.; Marple, B.F.; Nicklas, R.A.; Adino, A.D.; Bachert, C.; Borish, L.; Chinchilli, V.M.; et al. Rhinosinusitis: Developing guidance for clinical trials. J. Allergy Clin. Immunol. 2006, 118, S17–S61. [Google Scholar] [CrossRef]
- Gevaert, P.; Calus, L.; Van Zele, T.; Blomme, K.; De Ruyck, N.; Bauters, W.; Hellings, P.; Brusselle, G.; De Bacquer, D.; van Cauwenberge, P.; et al. Omalizumab is effective in allergic and nonallergic patients with nasal polyps and asthma. J. Allergy Clin. Immunol. 2013, 131, 110–116.e1. [Google Scholar] [CrossRef]
- Hopkins, C.; Gillett, S.; Slack, R.; Lund, V.J.; Browne, J.P. Psychometric validity of the 22-item Sinonasal Outcome Test. Clin. Otolaryngol. 2009, 34, 447–454. [Google Scholar] [CrossRef]
- VanCrombruggen, K.; Zhang, N.; Gevaert, P.; Tomassen, P.; Bachert, C. Pathogenesis of chronic rhinosinusitis: Inflammation. J. Allergy Clin. Immunol. 2011, 128, 728–732. [Google Scholar] [CrossRef]
- Wills-Karp, M. Immunologic basis of antigen-induced airway hyperresponsiveness. Annu. Rev. Immunol. 1999, 17, 255–281. [Google Scholar] [CrossRef]
- Stout, B.A.; Bates, M.E.; Liu, L.Y.; Farrington, N.N.; Bertics, P.J. IL-5 and granulocyte-macrophage colony-stimulating factor activate STAT3 and STAT5 and promote Pim-1 and cyclin D3 protein expression in human eosinophils. J. Immunol. 2004, 173, 6409–6417. [Google Scholar] [CrossRef] [Green Version]
- Ruwanpura, S.M.; McLeod, L.; Miller, A.; Jones, J.; Vlahos, R.; Ramm, G.; Longano, A.; Bardin, P.G.; Bozinovski, S.; Anderson, G.P.; et al. Deregulated Stat3 signaling dissociates pulmonary inflammation from emphysema in gp130 mutant mice. Am. J. Physiol. Lung. Cell. Mol. Physiol. 2012, 302, L627–L639. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharjee, A.; Shukla, M.; Yakubenko, V.P.; Mulya, A.; Kundu, S.; Cathcart, M.K. IL-4 and IL-13 employ discrete signaling pathways for target gene expression in alternatively activated monocytes/macrophages. Free. Radic. Biol. Med. 2013, 54, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Thierfelder, W.E.; van Deursen, J.M.; Yamamoto, K.; Tripp, R.A.; Sarawar, S.R.; Carson, R.T.; Sangster, M.Y.; Vignali, D.A.; Doherty, P.C.; Grosveld, G.C.; et al. Requirement for Stat4 in interleukin-12- mediated responses of natural killer and T cells. Nature 1996, 382, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Venkataraman, C.; Leung, S.; Salvekar, A.; Mano, H.; Schindler, U. Repression of IL-4-induced gene expression by IFN-gammarequires Stat1 activation. J. Immunol. 1999, 162, 4053–4061. [Google Scholar] [PubMed]
- Croxford, A.L.; Lanzinger, M.; Hartmann, F.J.; Schreiner, B.; Mair, F.; Pelczar, P.; Clausen, B.E.; Jung, S.; Greter, M.; Becher, B. The Cytokine GM-CSF drives the inflammatory signature of CCR2+ monocytes and licenses qutoimmunity. Immunity 2015, 43, 502–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becher, B.; Tugues, S.; Greter, M. GM-CSF: From growth factor to central mediator of tissue inflammation. Immunity 2016, 45, 963–973. [Google Scholar] [CrossRef] [Green Version]
- Tsantikos, E.; Lau, M.; Castelino, C.M.; Maxwell, M.J.; Passey, S.L.; Hansen, M.J.; McGregor, N.E.; Sims, N.A.; Steinfort, D.P.; Irving, L.B.; et al. Granulocyte-CSF links destructive inflammation and comorbidities in obstructive lung disease. J. Clin. Investig 2018, 128, 2406–2418. [Google Scholar] [CrossRef]
- Marino, V.J.; Roguin, L.P. The granulocyte colony stimulating factor (G-CSF) activates JAK/STAT and MAPK pathways in a trophoblastic cell line. J. Cell Biochem. 2008, 103, 1512–1523. [Google Scholar] [CrossRef] [PubMed]
- McLemore, M.L.; Grewal, S.; Liu, F.; Archambault, A.; Poursine-Laurent, J.; Haug, J.; Link, D.C. STAT-3 activation is required for normal G-CSF-dependent proliferation and granulocytic differentiation. Immunity 2001, 14, 193–204. [Google Scholar] [CrossRef]
- Chung, K.F. Cytokines in chronic obstructive pulmonary disease. Eur. Respir. J. Suppl. 2001, 34, 50s–59s. [Google Scholar] [CrossRef] [Green Version]
- König, K.; Klemens, C.; Haack, M.; Nicoló, M.S.; Becker, S.; Kramer, M.F.; Gröger, M. Cytokine patterns in nasal secretion of non-atopic patients distinguish between chronic rhinosinusitis with or without nasal polys. Allergy Asthma. Clin. Immunol. 2016, 12, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, A.; Kato, A.; Zhang, N.; Conley, D.; Suh, L.; Tancowny, B.; Carter, D.; Carr, T.; Radtke, M.; Hulse, K.; et al. Evidence for altered activity of the IL-6 pathway in chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2010, 125, 397–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linke, R.; Pries, R.; Könnecke, M.; Bruchhage, K.L.; Böscke, R.; Gebhard, M.; Wollenberg, B. Increased Activation and Differentiated Localization of Native and Phosphorylated STAT3 in Nasal Polyps. Int. Arch. Allergy Immunol. 2013, 162, 290–298. [Google Scholar] [CrossRef]
- Lai, X.P.; Li, X.; Chang, L.H.; Chen, X.H.; Huang, Z.Z.; Bao, H.W.; Huang, J.C.; Yang, L.Y.; Wu, X.F.; Wang, Z.Y.; et al. IL-19 Up-Regulates Mucin 5AC Production in Patients With Chronic Rhinosinusitis via STAT3 Pathway. Front Immunol. 2019, 10, 1682. [Google Scholar] [CrossRef] [Green Version]
- Mfuna-Endam, L.; Zhang, Y.; Desrosiers, M.Y. Genetics of rhinosinusitis. Curr. Allergy. Asthma. Rep. 2011, 11, 236–246. [Google Scholar] [CrossRef]
- Li, J.Y.; Fang, S.Y. Allergic profiles in unilateral nasal polyps of bilateral chronic rhinosinusitis. Am. J. Rhinol. 2008, 22, 111–114. [Google Scholar] [CrossRef]
- Lee, T.J.; Fu, C.H.; Wang, C.H.; Huang, C.C.; Huang, C.C.; Chang, P.H.; Chen, Y.W.; Wu, C.C.; Wu, C.L.; Kuo, H.P. Impact of chronic rhinosinusitis on severe asthma patients. PLoS ONE 2017, 12, e0171047. [Google Scholar]
- Huang, C.C.; Wang, C.H.; Fu, C.H.; Huang, C.C.; Chang, P.H.; Chen, Y.W.; Wu, C.C.; Wu, P.W.; Lee, T.J. Association between cigarette smoking and interleukin-17A expression in nasal tissues of patients with chronic rhinosinusitis and asthma. Medicine 2016, 95, e5432. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Biehl, A.; Gadina, M.; Hasni, S.; Schwartz, D.M. Erratum to: JAK-STAT Signaling as a Target for Inflammatory and Autoimmune Diseases: Current and Future Prospects. Drugs 2017, 77, 939. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Subjects | |||||
|---|---|---|---|---|---|
| Demographics | Control 1 (n = 13) | Control 2 (n = 13) | CRSwNP(I) (n = 22) | CRSwNP(II) (n = 39) | p-Value |
| Gender (female), n (%) | 5 (38.5) | 7 (53.8) | 8 (36.4) | 8 (20.5) | 0.131 |
| Age (years), mean ± SE | 40.2 ± 3.6 | 36.6 ± 3.2 | 45.4 ± 2.6 | 49.4 ± 2.6 | 0.398 |
| Asthma, n (%) | 0 (0) | 0 (0) | 3 (13.6) | 5 (12.8) | 0.288 |
| Smoking, n (%) | 2 (15.3) | 3 (23.1) | 4 (18.2) | 6 (15.4) | 0.930 |
| Diabetes, n (%) | 1 (7.7) | 1 (7.7) | 2 (9.1) | 3 (7.7) | 0.998 |
| Peripheral eosinophil (%), mean ± SE | 3.2 ± 0.8 | 3.6 ± 0.7 | 4.1 ± 0.5 | 3.3 ± 0.4 | 0.774 |
| Atopic IgE (KU/L), mean ± SE | 65.4 ± 18.1 | 76.9 ± 19.3 | 115.2 ± 17.1 | 179.8 ± 36.4 | <0.001 |
| Cytokines | Control 1 (C1) | Control 2 (C2) | CRSwNP(I) | CRSwNP(II) | p-Value |
|---|---|---|---|---|---|
| Number | 13 | 13 | 22 | 39 | |
| Mean ± SE (Range) | |||||
| IL-5 | 12.23 ± 1.40 (4.88–21.26) | 13.24 ± 1.56 (4.13–25.87) | 36.84 ± 4.82 (10.05–90.86) | 56.86 ± 4.32 (10.96–112.34) | <0.001 |
| IL-6 | 51.77 ± 10.89 (23.07–164.01) | 129.77 ± 46.51 (22.56–518.56) | 255.34 ± 63.53 (24.51–976.91) | 356.81 ± 43.97 (142.40–1073.57) | 0.009 |
| IL-13 | 7.74 ± 1.79 (1.51–22.77) | 12.67 ± 1.53 (2.77–24.9) | 25.79 ± 3.92 (5.28–82.27) | 40.10 ± 2.86 (12.91–95.74) | <0.001 |
| G-CSF | 187.31 ± 47.28 (45.33–558.07) | 267.39 ± 98.87 (54.79–1032.31) | 1045.71 ± 203.12 (69.83–3579.17) | 2079.17 ± 331.99 (71.06–8847.96) | <0.0001 |
| GM-CSF | 0.90 ± 0.24 (0.09–2.3) | 1.50 ± 0.19 (0.13–2.73) | 1.51 ± 0.21 (0.11–2.78) | 1.6 ± 0.20 (0.12–3.43) | 0.2654 |
| IFN-γ | 34.83 ± 9.37 (5.78–113.43) | 92.43 ± 11.33 (15.28–172.53) | 98.5 ± 15.90 (16.12–330.92) | 119.59 ± 10.08 (14.15–363.48) | 0.006 |
| Cytokines | ||||||
|---|---|---|---|---|---|---|
| Groups | IL-5 | IL-6 | IL-13 | G-CSF | GM-CSF | IFN-γ |
| Control 1 vs. Control 2 | 0.6816 | 0.0812 | 0.0455 | 0.7976 | 0.1177 | 0.0012 |
| Control 1 vs. CRSwNP(I) | <0.001 | 0.0039 | 0.003 | 0.0016 | 0.1419 | 0.0025 |
| Control 1 vs. CRSwNP(II) | <0.001 | <0.001 | <0.001 | <0.0001 | 0.0869 | <0.001 |
| Control 2 vs. CRSwNP(I) | 0.01 | 0.0187 | 0.0212 | 0.006 | 0.8643 | 0.9184 |
| Control 2 vs. CRSwNP(II) | <0.001 | 0.0008 | <0.001 | <0.0001 | 0.8326 | 0.1663 |
| CRSwNP(I) vs. CRSwNP(II) | 0.0046 | 0.0124 | 0.008 | 0.0396 | 0.7753 | 0.1219 |
| Clinical Assessments of Disease Severity | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| LMK-CT | TPS | SNOT-22 | |||||||
| Expression | r | p-Value | 95% CI | r | p-Value | 95% CI | r | p-Value | 95% CI |
| p-JAK2 | 0.45 | 0.0002 | 0.192–0.598 | 0.31 | 0.0139 | 0.112–0.955 | 0.43 | 0.0005 | 0.0458–0.155 |
| IL-5 | 0.42 | 0.0007 | 1.050–3.677 | 0.30 | 0.0259 | 0.456–6.86 | 0.46 | 0.0002 | 0.0586–0.763 |
| IL-6 | 0.27 | 0.0344 | 1.204–30.41 | 0.09 | 0.4764 | −52.70–111.50 | 0.37 | 0.038 | 1.900–9.414 |
| IL-13 | 0.23 | 0.0699 | −0.0772–1.92 | 0.26 | 0.041 | 0.0870–4.05 | 0.23 | 0.0751 | −0.0251–0.506 |
| G-CSF | 0.44 | 0.0003 | 78.01–251.1 | 0.34 | 0.0073 | 68.72–423.3 | 0.38 | 0.0028 | 13.35 to 60.94 |
| IFN-γ | 0.13 | 0.3259 | −1.80–5.34 | 0.04 | 0.7351 | −6.146–8.65 | 0.05 | 0.7118 | −0.779–1.133 |
| Staining Intensity, n (%) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p-STAT3 ** | p-STAT5 | p-STAT6 | p-STAT1 | |||||||||
| Subjects | - | +/++ | +++ | - | +/++ | +++ | - | +/++ | +++ | - | +/++ | +++ |
| Control 1 (n = 13) | 92.3 (12) | 7.7 (1) | 0.0 (0) | 100.0 (13) | 0.0 (0) | 0.0 (0) | 100.0 (13) | 0.0 (0) | 0.0 (0) | 100.0 (13) | 0.0 (0) | 0.0 (0) |
| Control 2 (n = 13) | 84.6 (11) | 15.4 (2) | 0.0 (0) | 100.0 (13) | 0.0 (0) | 0.0 (0) | 100.0 (13) | 0.0 (0) | 0.0 (0) | 100.0 (13) | 0.0 (0) | 0.0 (0) |
| CRSwNP(I) (n = 22) | 9.1 (2) | 45.45 (10) | 45.45 (10) | 81.8 (18) | 18.2 (4) | 0.0 (0) | 90.9 (20) | 9.1 (2) | 0.0 (0) | 100.0 (22) | 0.0 (0) | 0.0 (0) |
| CRSwNP(II) (n = 39) | 5.1 (2) | 38.5 (15) | 56.4 (22) | 59.0 (23) | 41.0 (16) | 0.0 (0) | 79.5 (31) | 17.9 (7) | 2.6 (1) | 97.4 (38) | 2.6 (1) | 0.0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-T.; Chen, W.-C.; Tsai, M.-H.; Chen, J.-Y.; Chien, C.-Y.; Huang, S.-C. JAK2 Phosphorylation Signals and Their Associated Cytokines Involved in Chronic Rhinosinusitis with Nasal Polyps and Correlated with Disease Severity. Biomolecules 2021, 11, 1059. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11071059
Lin Y-T, Chen W-C, Tsai M-H, Chen J-Y, Chien C-Y, Huang S-C. JAK2 Phosphorylation Signals and Their Associated Cytokines Involved in Chronic Rhinosinusitis with Nasal Polyps and Correlated with Disease Severity. Biomolecules. 2021; 11(7):1059. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11071059
Chicago/Turabian StyleLin, Yu-Tsai, Wei-Chih Chen, Ming-Hsien Tsai, Jing-Ying Chen, Chih-Yen Chien, and Shun-Chen Huang. 2021. "JAK2 Phosphorylation Signals and Their Associated Cytokines Involved in Chronic Rhinosinusitis with Nasal Polyps and Correlated with Disease Severity" Biomolecules 11, no. 7: 1059. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11071059