
Implant Periapical Lesion: A Narrative Review

1
Department of Dentistry, Chang Gung Memorial Hospital, Chiayi 61363, Taiwan
2
Institute of Nursing and Department of Nursing, Chang Gung University of Science and Technology, Chiayi 61363, Taiwan
Technologies 2021, 9(3), 65; https://0-doi-org.brum.beds.ac.uk/10.3390/technologies9030065
Submission received: 29 July 2021
/
Revised: 26 August 2021
/
Accepted: 1 September 2021
/
Published: 6 September 2021
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Implant periapical lesion (IPL) is an infectious-inflammatory alteration surrounding an implant apex. It is a multifactorial disease that may ultimately cause implant failure. The diagnosis of IPL is based on examination of clinical manifestations and apical radiolucency. Many etiologies have been attributed to IPL, including preexisting microbial pathology and surgical trauma. Moreover, many systems have been used to classify IPL based on different parameters. To date, non-surgical and surgical treatment, as well as removal of failed implants, have been considered to successfully manage IPL. However, prevention of IPL surpasses all modes of treatment. An increased number of IPL cases are expected as implants have become standard for tooth replacement in dentate arches. Therefore, it is necessary to understand IPL more comprehensively. Herein, an introduction to IPL, including its etiology, diagnosis, classification, treatment, and prevention, has been undertaken.
1. Introduction
Implant periapical lesion (IPL) is an infectious-inflammatory alternation surrounding implant apex that ultimately leads to implant failure [1,2,3,4]. IPL was first reported in 1992, when McAllister et al. showed two submerged implants with periapical radiolucency [5]. Different nomenclatures were used in literature to refer to IPL, including apical implantitis, apical peri-implantitis, early peri-implantitis, endodontic-implant pathology, inflammatory implant periapical lesion, periapical implant lesion, periapical implant pathology, retrograde peri-implant infection, and retrograde peri-implantitis [6,7,8,9]; however, these terms were defined somewhat differently [7,10]. For example, retrograde peri-implantitis was defined as a clinically symptomatic radiolucency around the apical area of an osseointegrated implant, which differed from apical infection in an implant without osseointegration [11].
The prevalence of IPL varies from 0.26% to 9.9%, and its incidence may reach 7.8% if adjacent teeth receive endodontic treatment [6,7,9,12,13]. Additionally, recent studies have shown that IPL occurs with a frequency of 0.34–3.8% [14,15,16]. In the maxilla and mandible, the incidence reported were 0.28–5.8% and 0.42–2.7%, respectively [11,14,15]. In contrast, other studies demonstrated a high prevalence in the maxillary premolar [10,17].
The endodontic status of the tooth extracted from the implant site and adjacent teeth could affect the occurrence of IPL [18]. An increased presence of IPL has been noted when endodontic treatment fails in adjacent teeth or prior to implant placement [10]. Therefore, the incidence was low when implant therapy was in its initial stages as implants were mostly placed in edentulous ridges. Currently, more IPL cases are expected as implants are used to replace single/multiple teeth in partially edentulous ridges [7,19,20]. There are some differences between IPL and peri-implantitis based on the involved pathogens (i.e., endodontic pathogens in IPL and periodontal pathogens in peri-implantitis), rate of expansion, and pathway of infection [7]. Therefore, modes of treatment and prevention of IPL mildly differ from those of peri-implantitis.
The aim of this narrative review article was to introduce IPL, including etiology, diagnosis, classification, treatment, and prevention.
2. Materials and Methods
A literature search was performed on PubMed for English papers on IPL, published between January 1992 and June 2021. We found 60 articles, using different search terms focused on title, including apical implantitis, apical peri-implantitis, endodontic-implant pathology, implant periapical lesion, periapical implant lesion, periapical implant pathology, retrograde peri-implant infection, and retrograde peri-implantitis. Eight papers were excluded after reviewing their abstracts. Exclusion criteria were only involving peri-implantitis, endodontic implant and knowledge towards IPL. Then, seven retrospective studies, seven review articles and other case report/case series papers were included. In addition, 37 papers were searched from the reference list of the above 52 papers. Therefore, a total of 89 papers are cited in present review.
3. Results
3.1. Etiology
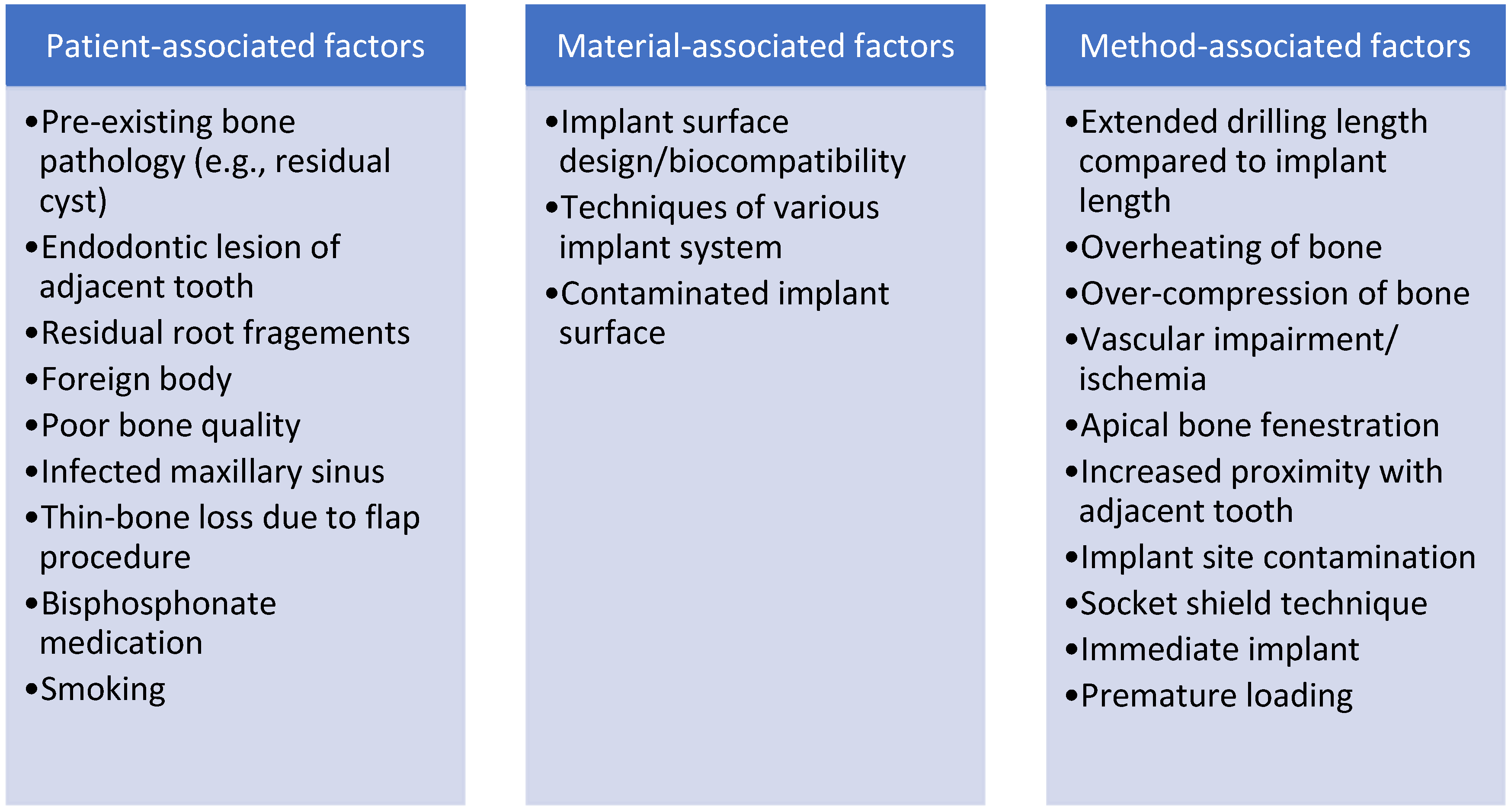
It is well known that IPL is a multifactorial disease [21]. However, there is no consensus on the etiology of IPL [22], and it remains unclear whether IPL is composed of healthy tissue, new tissue destruction, or activation of a preexisting condition [23]. Dental implants do not withstand any bacterial challenge during the first stage of osseointegration [24]. Thus, bacterial contamination appears to be the predominant cause, with several other contributing factors [17,25]. The possible etiologies of IPL may be divided into three categories: patient-associated factors, material-associated factors, and method-associated factors (Figure 1). However, local bone and intraoral factors (e.g., etiology of tooth extraction and the endodontic condition of adjacent teeth) were stronger than other factors associated with IPL [15].
3.1.1. Patient-Associated Factors
Patient-Associated Factors include the presence of pre-existing/adjacent bone pathology (e.g., residual cyst), residual root fragments or foreign bodies; implant placed into infected sinus or poor quality bone, and patient under long-term oral bisphosphonates or those with a smoking habit [8,17,23,26,27,28,29,30,31,32,33,34,35,36]. Wang showed implant periapical radiolucency lesions in one patient taking long-term oral bisphosphonates [33].
Bacteria from endodontic-failed tooth or residual lesion might be reactivated by implant site osteotomy and subsequent colonization on implant apex [16,37]. There was a significant difference observed between the presence and absence of IPL in terms of endodontic failure at implant site and/or adjacent location [10]. The apical region of endodontically treated teeth often reveals histological signs of inflammation or persistent micro-organisms, even if optimal bone healing is seen on radiographs [38,39]. Additionally, residual encapsulated bacteria maybe remain in bone even after debridement of extraction socket, leading to IPL initiation [5,11,24,27]. It is difficult to detect other pathologies in radiographs, even if cone beam computed tomography (CBCT) is used [11]. Therefore, the endodontic status of tooth extracted from the implant site has a major influence on IPL [11,40]. An IPL presented in 31.5% of implants with previous endodontic treatment, but only in 2.84% of implants without previous endodontic treatment [10]. The odds ratio for IPL was 7.2 for an extracted tooth with an endodontic treatment history when compared with a pathology free tooth. Moreover, the odds ratio for IPL was 8 for adjacent teeth with an endodontic treatment history when compared with pathology-free teeth [18]. Moreover, the odds of developing early IPL in implant sites with apical lesion was up to 26.3-fold [14]. However, recent retrospective study including 25 patients showed that previous endodontic surgery in implant site did not increase risk of IPL [41].
Residual root fragments at the implant site, commonly seen in maxillary premolars, is another possible etiology [17,42]. Pre-mature loading usually results in early implant failure; however, it is controversial whether early loading is an etiology of IPL [3,11]. Other than local factors associated with implant site or adjacent tooth, Wang et al. reported apical radiolucency around three implants in a patient under long-term use of oral bisphosphonates [33]. Thus, the medical status of patients should be evaluated before dental implant therapy.
3.1.2. Material-Associated Factors
Material-associated factors include implant surface design and biocompatibility, specific techniques of implant surgery, and implant surface contamination during production and insertion [23,28]. Further, external contamination of the implants might result in implant periapical lesions [23].
In addition, the incidence of IPL is higher for TiUnite implant surface than for machined implant surface. The machined implants usually show higher failure rate when contacting with endodontic pathology; however, TiUnite implants have coronal osseointegration before fibrous capsulation reached this area. Thus, there was a greater incidence of apical lesion and less failure rate in TiUnite implants than machined implants [11]. Nevertheless, the material factors associated with IPL are fewer than patient-associated factors and method-associated factors [7].
3.1.3. Method-Associated Factors
Method-associated factors include overheating of bone during implant site preparation, compression of bone due to excessive tightening, vascular impairment/ischemia, apical bone fenestration, implant close to adjacent teeth, and surgical bed contamination (bacteria, epithelial cells or starch of gloves) [2,23,29,30,43,44]. In addition, one IPL case associated with the “socket shield technique” was reported recently [45].
When an implant fixature is placed close to the adjacent tooth, the blood supply of the adjacent tooth may be compromised due to osteotomy and flap elevation [24]. Moreover, immediate implant treatment (odds: 21-fold) or an apical mesial distance of ≤1.5 mm between implant and tooth are risk factors (5.12-fold) associated with early IPL [14]. Overheating of bone during implant site preparation and compression of bone during tightening could result in bone necrosis, which is also associated with IPL [5,28]. The occurrence of IPL may be associated with traumatic implant placement, making it preventable [46].
3.2. Examination and Diagnosis
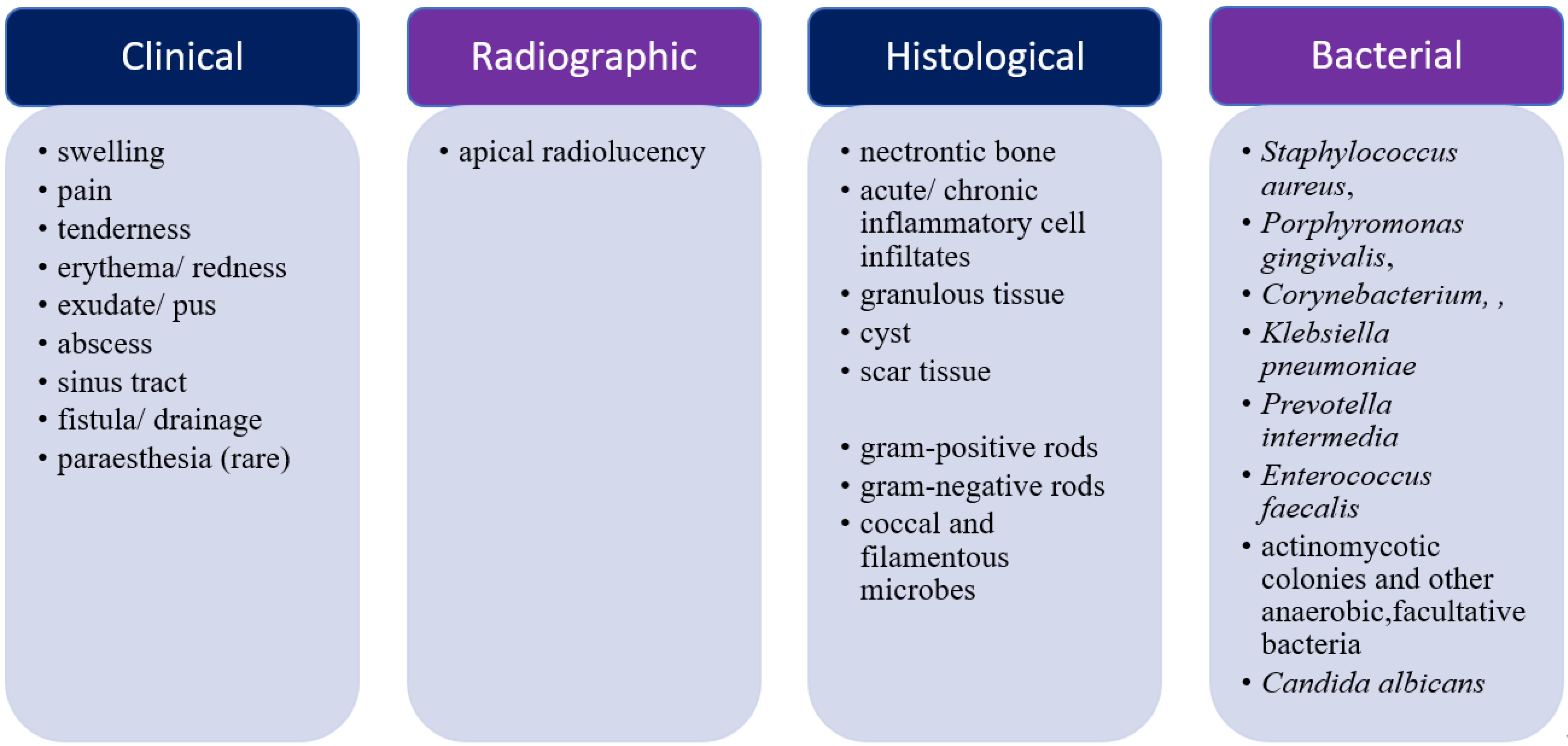
The findings of IPL are summarized in Figure 2. The symptoms and signs (S/S) of IPLs include: swelling, erythema, pain, tenderness, suppuration, sinus tract, fistula, abscess, and apical radiolucency [7]. Paraesthesia was also reported in one case with a large IPL [12]. Apical radiolucency is the prominent and commonest finding in IPL; however, the clinical signs may be different in each case, e.g., inactive IPL without infectious and/or inflammatory S/S clinically [30]. The sinus tract is the most common clinical expression; however, severe pain is uncommon and deep pockets are rare [17]. The time of diagnosis varies from 7 days to 4 years after implant surgery in reports, and it is commonly made within the first 6 months after implant placement [7,8,47]. The extent of active IPLs tends to increase with time, and thus, diagnosing IPL as early as possible is important to limit damage and initiate aggressive treatment if required [17]. Radiographic examination is valuable in early detection of IPL, even before sinus tract formation. Periapical radiographs are recommended immediately after implant placement as a baseline and at the third month of healing for detection of chronic ILP [5,17]. However, periapical radiographs have a high risk of false-negative results [8]. The lesion might not be evident on periapical radiographs of the mandible; therefore, occlusal view radiographs or CBCT (cone beam computed tomography) are used for confirmation of mandibular IPL [26].
Histologic examination of IPL has revealed necrotic bone, inflammatory infiltrate, and/or cyst, which may be related to vascular impairment and bone fracture in the apical area [8,29,30]. These findings are analogous with those of granuloma or abscess at the root apex of nonvital teeth [48]. In addition, gram-positive rods, gram-negative rods, and coccal and filamentous microbes were found in pathologic examination of IPL [5]. It is difficult to obtain a bacterial culture from IPL and there is a high risk of contamination during sampling of IPL [8]. There are higher counts of anaerobic bacteria than that of aerobic bacteria because of intrabony lesions [18]. Staphylococcus aureus, Porphyromonas gingivalis, Corynebacterium, Klebsiella pneumoniae, Prevotella intermedia, Enterococcus faecalis, actinomycotic colonies, and various anaerobic and facultative bacteria were found in IPL; Porphyromonas gingivalis was the prominent species and Candida albicans was found occasionally [7,8,18,49,50]. Thus, the microbiological findings must be taken into consideration for antibiotic selection [18], Klebsiella pneumonia, group D streptococci, Corynebacterium species, and alpha-hemolytic streptococci were discovered in the apical lesions of adjacent teeth [19]. The relationship between an extra-radicular infection and endodontic failure remains controversial [8]. Some authors suggested that rare extra-radicular infections are caused by Actinomyces and Propionibacterium. Different studies have shown that extra-radicular infections are common and involve Candida, Staphylococcus, Enterococcus, and Enterobacter [8]. In addition, Verdugo reported that periodontopathogen and Epstein-Barr virus (EB virus) associated periapical lesions may also induce IPL. It is suggested that saliva polymerase chain reaction for EB virus could be used to predict granulation tissue infection and as reference for antimicrobial therapy [51]. Saliva EBV-positive patients might have granulation tissue infection with Tannerella forsythia and Treponema denticola [51].
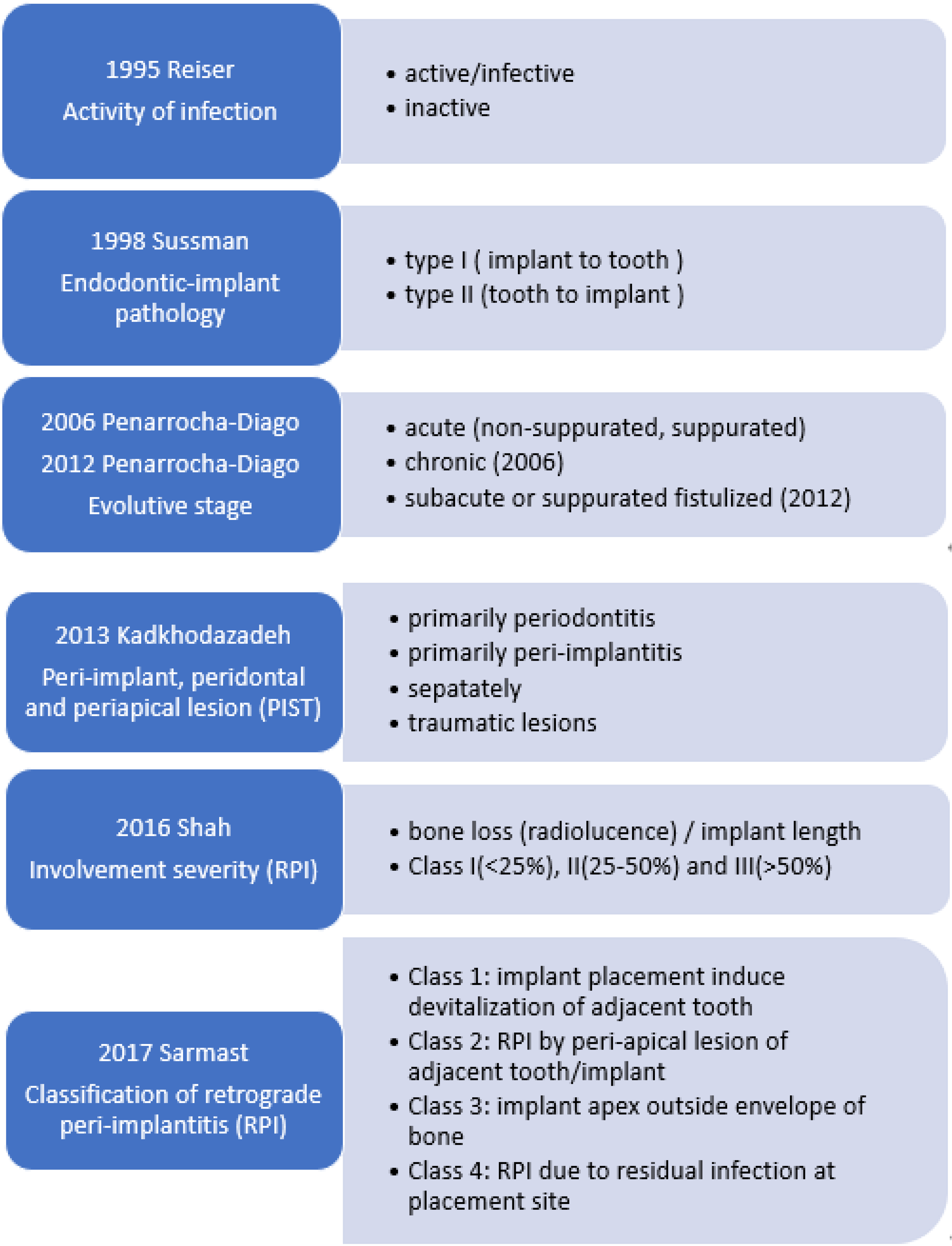
3.3. Classification
Different systems have been used to classify IPL (Figure 3). According to the activity of the infection, IPLs are classified into active/infective and inactive lesions [28]. An inactive lesion may be an apical scar resulting from placing an implant shorter than the prepared length. Active lesions are infected lesions with S/S, which include pain, tenderness, swelling and/or the presence of a fistulous tract [11]. Lesions are also classified according to their stage of progression into acute non-suppurative phase with inflammatory infiltrate, acute suppurative phase with periapical granuloma, and chronic phase with periapical abscess [1]. There were acute symptoms in non-suppurative stage, but no radiographic change was observed [6]. The categories in the classification system were modified as “acute non-suppurated,” “acute suppurated,” and “subacute or suppurated-fistulized” apical peri-implantitis [52]. Based on the endodontic-implant infection pathway, two different infection patterns were “from implant to tooth (type I)” and “from tooth to implant (type II).” [53] Devitalization of adjacent tooth pulp occurs during osteotomy preparation in the first pathway while IPL occurs shortly after placement of the implant when adjacent tooth develops a periapical pathology in the second pathway [53]. To treat lesions based on the classification of IPL, the “PIST” system and the retrograde peri-implantitis (PRI) system were developed in recent years. The PIST system classifies the different pathological conditions around dental implants into “primarily periodontitis (P-class; P-1, P-2, P-3),” “primarily peri-implantitis (I-class; I-1, I-2, I-3),” ”separately (S-class; S-1, S-2, S-3),” and traumatic lesions (T-class; T-0, T-1)” to determine the relationship between the periodontal, periapical, and peri-implant complications [54]. The “symptomatic T-1 lesion” is Sussman’s “type I infection pattern.” The PRI classification system was used in treatment planning and determination of prognosis in IPL based on the “bone loss/implant length” (in percentage) on periapical radiographs, which includes the following classes: mild—Class I (bone loss < 25%), moderate—Class II (bone loss 25% to 50%), and advanced—Class III (bone loss > 50%) [25,55]. Classes I and II lesions resolve completely; however, the prognosis of Class III lesions can range from fair to poor because the >50% bone loss may cause inadequate osseointegration [17,25]. Sarmast provided another classification in 2017 to aid decision-making for IPL: Class 1, implant placement induces devitalization of an adjacent previously vital tooth; Class 2, implant apex is infected by a peri-apical lesion on adjacent tooth/implant; Class 3, implant apex is outside the bone housing; and Class 4, implant apex lesion develops from residual infection of implant site. The endodontic treatment of involved tooth is suggested for Class 1 and Class 2 lesions per this classification. Endodontic evaluation of adjacent teeth before implant placement is helpful to prevent IPL [56].
3.4. Treatment
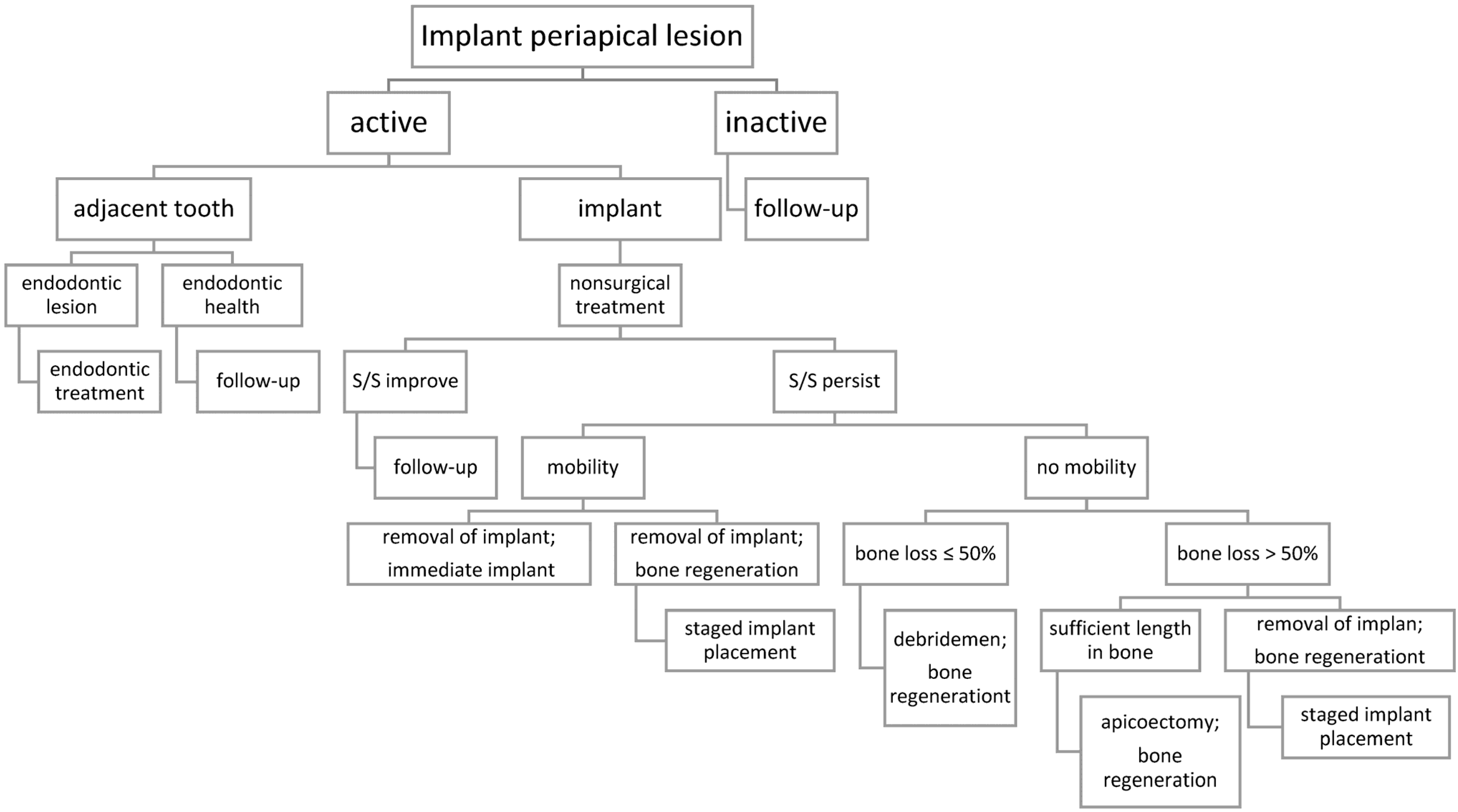
Though many materials and methods are used for treating IPL, there is no evidence on which is the best [22,28,47,57,58,59]. If the IPL is inactive, such as a scar, regular follow-up is suggested. Elimination of infection is the only point of concensus in the treatment protocol for active IPL [60]. Requirement of endodontic therapy/surgery for teeth adjacent to implants must be examined [61,62]. In addition, medications, such as bisphosphonates, used by the patient should be reevaluated. The prognosis of IPL may be based on the extent of radiolucency [25]. Herein, treatment for active IPL is divided into three major modes (Figure 4).
3.4.1. Nonsurgical Treatment
Antibiotics are usually used initially in active IPL to reduce the level of infection [3,17]. Systemic antibiotics might be used as adjuvant therapy, and definitive surgical intervention should be performed as early as possible to limit disease progression [3,17]. Antibiotic use alone is unlikely to be successful due to difficulties in eradicating bacterial colonies in IPL [19,21,59]. However, very few implants were treated successfully by non-surgical treatment alone, including one of the three implants with apical radiolucency in the patient under bisphosphosphonate medication [18,33,63,64]. Antibiotics are selected according to the etiology, presence or absence of pain and abscess, time of onset, and whether the endodontic lesion is open or closed [17]. Penicillin, amoxicillin, amoxicillin-clavulanate, metronidazole, and clindamycin are usually used to treat IPL; other drugs include azithromycin, cephalosporin, and tetracycline [6,7]. The combination of amoxicillin and metronidazole has also been used [5].
3.4.2. Surgical Treatment
This includes surgical debridement, regenerative treatment, resection of implant apex, and a combination of different approaches.
A surgical approach is chosen based on implant stability and the extension of IPL [1,17,47,55]. Surgical debridement alone or combined with regenerative treatment has been suggested for bone loss <50% of implant length [47]. Resection of the implant apex may be needed in cases with >50% bone loss and with difficulty in accessing the IPL [17,52,65]. However, maintenance of sufficient length be used after resection and keeping the implant unloaded for at least 6 months were found important for successful implant apicoectomy [20,66,67], and high success rates of implant apicoetomy have been reported [20,67,68].
The detoxication of implant surfaces is performed by chemical and physical methods. The universal implant Deplaquer (Straumann, USA) and an air-abrasive device with amino acid glycine powder were used for physical detoxication [69,70,71]. The chemical agents include chlorhexidine, tetracycline, citric acid, ethylenediaminetetraacetic acid (EDTA), and so on [65,72,73]. Moreover, calcium hydroxide is a better bacterial inhibitor than chlorhexidine for endodontic infections [27]. The use of lasers, such as Er,Cr:YSGG laser, is advantageous because of its bactericidal effect on oral pathogens and the ability to reach anatomically complex areas [71,74]. Moreover, laser supports rapid blood clot formation and graft containment in ridge preservation [75]. Therefore, laser may have the potential to detoxify the implant surface and apical lesion, and to improve the outcome of regenerative treatment in IPL [18]. The modes of bone regeneration used in the treatment of IPL and peri-implantitis are similar [76], and in critical size bone defects, the use of bone regeneration membrane or platelet rich fibrin (PRF) has been suggested [17,69,71,77]. However, it is difficult to gain re-osseointegration on a previously affected implant even with various regenerative materials and methods [3,17].
3.4.3. Removal of Failed Implants
In a recent review, Wiedemann concluded that mobile implants and/or more than 50% bone loss require removal of implant combined with immediate or delayed implant placement [59]. Removal of mobile teeth and new wider implant placement is only performed at non-infected sites. Bone regeneration after implant extraction and staged implant therapy is suggested at infected sites [17,46]. However, the exact etiology of implant failure should be confirmed and corrected before new implant placement, otherwise, implant failure may occur again [5,17].
4. Discussions
IPL is a preventable disease [56]. Hence, a detailed treatment plan, careful and sterile surgery, and regular follow-up would limit the incidence and extent of infection in active IPL, thereby reducing implant removal rate.
4.1. Detailed Treatment Plan
A thorough medical history, focusing on the possible influences on implant therapy, is paramount [8,33]. It is important to thoroughly evaluate the endodontic and periodontal condition of the extracted and adjacent teeth by clinical and radiographic examination [61]. However, it is difficult to detect histologic inflammation and infection in radiographs, even with CBCT [8,11]. Most of the infectious oral bacteria, such as streptococci, are susceptible to penicillin, and bacteria in periapical lesions are susceptible to metronidazole, cefoxitin, and clindamycin [27]. Therefore, antibiotic prophylaxis and postoperative use for 5–7 days may be considered in implant therapy, especially with a history of failed endodontic treatment [27,78]. Additionally, one way to reduce incidence of IPL could be through increasing the distance between implant and adjacent tooth as well as extending follow-up time after endodontic treatment of adjacent tooth [13]. Immediate implant placement in periapical infected sites remains controversial, as there is no consensus on appropriate surgical protocol and antibiotic prophylaxis [79,80,81,82]. Meticulous cleaning, thorough debridement/ curettage, and chemical irrigation (such as 0.12% chlorhexidine) prior to implant placement could improve implant survival rate at infected sites [18,83,84]. Currently, lasers, including Er-Cr:YSGG and Nd:YAG Laser, are used as adjuncts for the debridement after extraction, especially during immediate implant placement [85]. Laser has been demonstrated to be superior to chemical treatment [85]. To alleviate concerns of IPL, it may be helpful to decontaminate the socket after tooth extraction and to sterilize the site before implant placement with laser.
4.2. Careful and Sterile Surgery
This involves prevention of method-associated etiologic factors of IPL, by preventing contamination through sterile surgery, avoiding overheating of bone by adequate cooling and gentle drilling, avoiding compression of bone chip by optimal tightening, and accurate implant placement using a well-designed surgical stent [7]. The distance between the teeth and implants is crucial in preventing IPL [6]. In most cases, placement of implants did not affect the pulpal and apical condition of the adjacent teeth [86]. Less irrigation in the apical region and intermittent drilling (pumping) for proper cooling, every 15 to 20 s, is suggested during deep preparation [24,28]. Nonetheless, method-associated factors may be more easily handled than patient-associated factors.
4.3. Regular Follow-Up
Avoiding premature loading after implant surgery has been suggested to prevent IPL [11,87]. Radiolucency surrounding implant apex usually appears between 7 and 16 days after implant placement; however, in some cases, radiolucency has appeared even up to 3 months post-surgery [6,9]. The mean period for the appearance of clinical symptoms of IPL was 51.83 days [16]. Moreover, a mean period of 21.7 days was reported for the diagnosis of early IPL after dental implant placement [14]. A periapical X-ray is suggested at implant placement and post-surgery 6–8 weeks before prosthetic treatment [16]. However, periapical radiography within one month after implant surgery may be suggested in some cases.
The survival rate in IPL varies between 73.2% to 97.4% [6]. The cumulative survival rate of 78.3% with a mean survival time of 85.4 months was recently reported [88]. Early detection of active IPL could increase implant survival rate by over 91% [6,9,89]. Therefore, it is very crucial to detect IPL as early as possible. In addition, the diagnostic stage of IPL and the previous periapical lesion at the implant site significantly affect the survival of implants after surgical treatment [88].
5. Conclusions
Implant periapical lesion, with a multifactorial etiology, is an infectious-inflammatory lesion surrounding the implant apex. To date, many methods are used for treating IPL, including non-surgical and surgical techniques. Detection of IPL as early as possible by regular follow-up is necessary to avoid implant failure and removal. However, prevention is the best treatment, and the incidence of IPL could be reduced by detailed examination before dental implant therapy and careful surgical technique. Furthermore, a comprehensive understanding of IPL, including its etiology and treatment, is necessary.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Penarrocha Diago, M.; Boronat Lopez, A.; Lamas Pelayo, J. Update in dental implant periapical surgery. Med. Oral Patol. Oral Cir. Bucal 2006, 11, E429–E432. [Google Scholar]
- Mellonig, J.T.; Griffiths, G.; Mathys, E.; Spitznagel, J., Jr. Treatment of the failing implant: Case reports. Int. J. Periodontics Restor. Dent. 1995, 15, 384–395. [Google Scholar]
- Jalbout, Z.N.; Tarnow, D.P. The implant periapical lesion: Four case reports and review of the literature. Pract. Proced. Aesthet. Dent. 2001, 13, 107–112. [Google Scholar]
- Meffert, R.M. Maintenance and treatment of the ailing and failing implant. J. Indiana Dent. Assoc. 1994, 73, 22–24. [Google Scholar] [PubMed]
- McAllister, B.S.; Masters, D.; Meffert, R.M. Treatment of implants demonstrating periapical radiolucencies. Pract. Periodontics Aesthet. Dent. 1992, 4, 37–41. [Google Scholar] [PubMed]
- Blaya-Tarraga, J.A.; Cervera-Ballester, J.; Penarrocha-Oltra, D.; Penarrocha-Diago, M. Periapical implant lesion: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2017, 22, e737–e749. [Google Scholar] [CrossRef]
- Chang, L.C.; Hsu, C.S. Implant periapical lesion—Literature review. J. Dent. Sci. 2007, 2, 179–192. [Google Scholar]
- Marshall, G.; Canullo, L.; Logan, R.M.; Rossi-Fedele, G. Histopathological and microbiological findings associated with retrograde peri-implantitis of extra-radicular endodontic origin: A systematic and critical review. Int. J. Oral Maxillofac. Surg. 2019, 48, 1475–1484. [Google Scholar] [CrossRef]
- Penarrocha-Diago, M.; Penarrocha-Diago, M.; Blaya-Tarraga, J.A. State of the art and clinical recommendations in periapical implant lesions. 9th Mozo-Grau Ticare Conference in Quintanilla, Spain. J. Clin. Exp. Dent. 2017, 9, e471–e473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Martinez, F.; Gomez Moreno, G.; Olivares-Ponce, P.; Eduardo Jaramillo, D.; Eduardo Mate Sanchez de Val, J.; Calvo-Guirado, J.L. Implants failures related to endodontic treatment. An observational retrospective study. Clin. Oral Implant. Res. 2015, 26, 992–995. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Vogels, R.; Alsaadi, G.; Naert, I.; Jacobs, R.; van Steenberghe, D. Predisposing conditions for retrograde peri-implantitis, and treatment suggestions. Clin. Oral Implant. Res. 2005, 16, 599–608. [Google Scholar] [CrossRef]
- Jafarian, M.; Rayati, F.; Najafi, E. Successful treatment of a large implant periapical lesion that caused paraesthesia and perimandibular abscess. Dent. Res. J. 2016, 13, 188–192. [Google Scholar]
- Zhou, W.; Han, C.; Li, D.; Li, Y.; Song, Y.; Zhao, Y. Endodontic treatment of teeth induces retrograde peri-implantitis. Clin. Oral Implant. Res. 2009, 20, 1326–1332. [Google Scholar] [CrossRef]
- Penarrocha-Oltra, D.; Blaya-Tarraga, J.A.; Menendez-Nieto, I.; Penarrocha-Diago, M.; Penarrocha-Diago, M. Factors associated with early apical peri-implantitis: A retrospective study covering a 20-year period. Int. J. Oral Implantol. 2020, 13, 65–73. [Google Scholar]
- Burdurlu, M.C.; Dagasan, V.C.; Tunc, O.; Guler, N. Retrograde peri-implantitis: Evaluation and treatment protocols of a rare lesion. Quintessence Int. 2021, 52, 112–121. [Google Scholar]
- Di Murro, B.; Canullo, L.; Pompa, G.; Di Murro, C.; Papi, P. Prevalence and treatment of retrograde peri-implantitis: A retrospective cohort study covering a 20-year period. Clin. Oral Investig. 2021, 25, 4553–4561. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Sorensen, W.P.; Wang, H.L. Management and prevention of retrograde peri-implant infection from retained root tips: Two case reports. Int. J. Periodontics Restor. Dent. 2004, 24, 422–433. [Google Scholar] [CrossRef] [Green Version]
- Lefever, D.; Van Assche, N.; Temmerman, A.; Teughels, W.; Quirynen, M. Aetiology, microbiology and therapy of periapical lesions around oral implants: A retrospective analysis. J. Clin. Periodontol. 2013, 40, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, M.D.; Juruaz, D.A.; Haggerty, P.C. The effect of periradicular endodontic pathosis on the apical region of adjacent implants. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 86, 578–581. [Google Scholar] [CrossRef]
- Balshi, S.F.; Wolfinger, G.J.; Balshi, T.J. A retrospective evaluation of a treatment protocol for dental implant periapical lesions: Long-term results of 39 implant apicoectomies. Int. J. Oral Maxillofac. Implant. 2007, 22, 267–272. [Google Scholar]
- Romanos, G.E.; Froum, S.; Costa-Martins, S.; Meitner, S.; Tarnow, D.P. Implant periapical lesions: Etiology and treatment options. J. Oral Implantol. 2011, 37, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Temmerman, A.; Lefever, D.; Teughels, W.; Balshi, T.J.; Balshi, S.F.; Quirynen, M. Etiology and treatment of periapical lesions around dental implants. Periodontology 2000 2014, 66, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, A.; Scarano, A.; Piattelli, M.; Podda, G. Implant periapical lesions: Clinical, histologic, and histochemical aspects. A case report. Int. J. Periodontics Restor. Dent. 1998, 18, 181–187. [Google Scholar]
- Sussman, H.I.; Moss, S.S. Localized osteomyelitis secondary to endodontic-implant pathosis. A case report. J. Periodontol. 1993, 64, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Thomas, R.; Kumar, T.; Mehta, D.S. Assessment of Intraobserver and Interobserver Agreement of a New Classification System for Retrograde Periimplantitis. Implant. Dent. 2016, 25, 817–824. [Google Scholar] [CrossRef]
- Tozum, T.F.; Sencimen, M.; Ortakoglu, K.; Ozdemir, A.; Aydin, O.C.; Keles, M. Diagnosis and treatment of a large periapical implant lesion associated with adjacent natural tooth: A case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e132–e138. [Google Scholar] [CrossRef]
- Flanagan, D. Apical (retrograde) peri-implantitis: A case report of an active lesion. J. Oral Implantol. 2002, 28, 92–96. [Google Scholar] [CrossRef]
- Reiser, G.M.; Nevins, M. The implant periapical lesion: Etiology, prevention, and treatment. Compend. Contin. Educ. Dent. 1995, 16, 768–770. [Google Scholar]
- Piattelli, A.; Scarano, A.; Balleri, P.; Favero, G.A. Clinical and histologic evaluation of an active “implant periapical lesion”: A case report. Int. J. Oral Maxillofac. Implant. 1998, 13, 713–716. [Google Scholar]
- Scarano, A.; Di Domizio, P.; Petrone, G.; Iezzi, G.; Piattelli, A. Implant periapical lesion: A clinical and histologic case report. J. Oral Implant. 2000, 26, 109–113. [Google Scholar] [CrossRef]
- Sussman, H.I. Endodontic pathology leading to implant failure—A case report. J. Oral Implant. 1997, 23, 112–115. [Google Scholar]
- Tseng, C.C.; Chen, Y.H.; Pang, I.C.; Weber, H.P. Peri-implant pathology caused by periapical lesion of an adjacent natural tooth: A case report. Int. J. Oral Maxillofac. Implant. 2005, 20, 632–635. [Google Scholar]
- Wang, H.L.; Weber, D.; McCauley, L.K. Effect of long-term oral bisphosphonates on implant wound healing: Literature review and a case report. J. Periodontol. 2007, 78, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Sussman, H.I. Cortical bone resorption secondary to endodontic-implant pathology. A case report. NY State Dent. J. 1997, 63, 38–40. [Google Scholar]
- Sussman, H.I. Implant pathology associated with loss of periapical seal of adjacent tooth: Clinical report. Implant. Dent. 1997, 6, 33–37. [Google Scholar] [CrossRef]
- Pistilli, R.; Canullo, L.; Menini, M.; Pistilli, V.; Rossi-Fedele, G.; Pesce, P. Retrograde peri-implantitis associated with residual cysts: 3 Case reports. J. Am. Dent. Assoc. 2020, 151, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Di Murro, B.; Papi, P.; Di Murro, C.; Pompa, G.; Gambarini, G. Correlation between endodontic pulpal/periapical disease and retrograde peri-implantitis: A case series. Aust. Endod. J. 2020, 47, 358–364. [Google Scholar] [CrossRef]
- Green, T.L.; Walton, R.E.; Taylor, J.K.; Merrell, P. Radiographic and histologic periapical findings of root canal treated teeth in cadaver. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997, 83, 707–711. [Google Scholar] [CrossRef]
- Seltzer, S. Long-term radiographic and histological observations of endodontically treated teeth. J. Endod. 1999, 25, 818–822. [Google Scholar] [CrossRef]
- Brisman, D.L.; Brisman, A.S.; Moses, M.S. Implant failures associated with asymptomatic endodontically treated teeth. J. Am. Dent. Assoc. 2001, 132, 191–195. [Google Scholar] [CrossRef]
- Saleh, M.H.A.; Khurshid, H.; Travan, S.; Sinjab, K.; Bushahri, A.; Wang, H.L. Incidence of retrograde peri-implantitis in sites with previous apical surgeries: A retrospective study. J. Periodontol. 2021, 92, 54–61. [Google Scholar] [CrossRef]
- Langer, L.; Langer, B.; Salem, D. Unintentional root fragment retention in proximity to dental implants: A series of six human case reports. Int. J. Periodontics Restor. Dent. 2015, 35, 305–313. [Google Scholar] [CrossRef] [Green Version]
- Penarrocha-Diago, M.; Boronat-Lopez, A.; Garcia-Mira, B. Inflammatory implant periapical lesion: Etiology, diagnosis, and treatment-presentation of 7 cases. J. Oral Maxillofac. Surg. 2009, 67, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Nedir, R.; Bischof, M.; Pujol, O.; Houriet, R.; Samson, J.; Lombardi, T. Starch-induced implant periapical lesion: A case report. Int. J. Oral Maxillofac. Implant. 2007, 22, 1001–1006. [Google Scholar]
- Stuani, V.T.; Manfredi, G.; Sant’Ana, A.C.P.; de Rezende, M.L.R. Periapical Lesion on an Implant after Socket Shield Technique: A Case Report. J. Int. Acad. Periodontol. 2019, 21, 29–35. [Google Scholar]
- Oh, T.J.; Yoon, J.; Wang, H.L. Management of the implant periapical lesion: A case report. Implant. Dent. 2003, 12, 41–46. [Google Scholar] [CrossRef]
- Sarmast, N.D.; Wang, H.H.; Soldatos, N.K.; Angelov, N.; Dorn, S.; Yukna, R.; Iacono, V.J. A Novel Treatment Decision Tree and Literature Review of Retrograde Peri-Implantitis. J. Periodontol. 2016, 87, 1458–1467. [Google Scholar] [CrossRef] [PubMed]
- Feller, L.; Jadwat, Y.; Chandran, R.; Lager, I.; Altini, M.; Lemmer, J. Radiolucent inflammatory implant periapical lesions: A review of the literature. Implant. Dent. 2014, 23, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, D. Implant Placement in Failed Endodontic Sites: A Review. J. Oral Implant. 2016, 42, 224–230. [Google Scholar] [CrossRef]
- Rokadiya, S.; Malden, N.J. An implant periapical lesion leading to acute osteomyelitis with isolation of Staphylococcus aureus. Br. Dent. J. 2008, 205, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Verdugo, F.; Castillo, A.; Simonian, K.; Castillo, F.; Farez-Vidal, E.; D’Addona, A. Periodontopathogen and Epstein-Barr virus-associated periapical periodontitis may be the source of retrograde infectious peri-implantitis. Clin. Implant. Dent. Relat Res. 2015, 17, 199–207. [Google Scholar] [CrossRef]
- Penarrocha-Diago, M.; Maestre-Ferrin, L.; Cervera-Ballester, J.; Penarrocha-Oltra, D. Implant periapical lesion: Diagnosis and treatment. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e1023–e1027. [Google Scholar] [CrossRef]
- Sussman, H.I. Periapical implant pathology. J. Oral Implant. 1998, 24, 133–138. [Google Scholar] [CrossRef]
- Kadkhodazadeh, M.; Amid, R. A New Classification for the Relationship between Periodontal, Periapical, and Peri-implant Complications. Iran. Endod. J. 2013, 8, 103–108. [Google Scholar] [PubMed]
- Shah, R.; Thomas, R.; Kumar, A.B.; Mehta, D.S. A Radiographic Classification for Retrograde Peri-implantitis. J. Contemp. Dent. Pract. 2016, 17, 313–321. [Google Scholar] [CrossRef]
- Sarmast, N.D.; Wang, H.H.; Sajadi, A.S.; Angelov, N.; Dorn, S.O. Classification and Clinical Management of Retrograde Peri-implantitis Associated with Apical Periodontitis: A Proposed Classification System and Case Report. J. Endod. 2017, 43, 1921–1924. [Google Scholar] [CrossRef] [PubMed]
- Ramanauskaite, A.; Juodzbalys, G.; Tozum, T.F. Apical/Retrograde Periimplantitis/Implant Periapical Lesion: Etiology, Risk Factors, and Treatment Options: A Systematic Review. Implant. Dent. 2016, 25, 684–697. [Google Scholar] [CrossRef]
- Chan, H.L.; Wang, H.L.; Bashutski, J.D.; Edwards, P.C.; Fu, J.H.; Oh, T.J. Retrograde peri-implantitis: A case report introducing an approach to its management. J. Periodontol. 2011, 82, 1080–1088. [Google Scholar] [CrossRef] [PubMed]
- Wiedemann, T.G. A Clinical Approach to Treatment of Retrograde Peri-Implantitis. Compend. Contin. Educ. Dent. 2021, 42, 170–175. [Google Scholar]
- Qu, C.; Meng, H.; Han, J. Implant periapical lesion—A review and a case report with histological evaluation. Clin. Oral Implant. Res. 2014, 25, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Sarmast, N.D.; Wang, H.H.; Sajadi, A.S.; Munne, A.M.; Angelov, N. Nonsurgical Endodontic Treatment of Necrotic Teeth Resolved Apical Lesions on Adjacent Implants with Retrograde/Apical Peri-implantitis: A Case Series with 2-year Follow-up. J. Endod. 2019, 45, 645–650. [Google Scholar] [CrossRef]
- Chung, S.H.; Park, Y.S.; Bae, K.S.; Baek, S.H.; Kum, K.Y.; Lee, W.; Shon, W.J. Saving an Integrating Implant Involved with Endodontic Implant Pathology Using Surgical Treatment. Int. J. Periodontics Restor. Dent. 2016, 36, 893–898. [Google Scholar] [CrossRef] [Green Version]
- Chang, L.H.; Hsu, C.S.; Lee, Y.L. Successful Medical Treatment of an Implant Periapical Lesion: A Case Report. Chang Gung Med. J. 2011, 34, 108–113. [Google Scholar]
- Waasdorp, J.; Reynolds, M. Nonsurgical treatment of retrograde peri-implantitis: A case report. Int. J. Oral Maxillofac. Implant. 2010, 25, 831–833. [Google Scholar]
- Manfro, R.; Garcia, G.F.; Bortoluzzi, M.C.; Fabris, V.; Bacchi, A.; Elias, C.N. Apicoectomy and Scanning Electron Microscopy Analysis of an Implant Infected by Apical (Retrograde) Peri-implantitis: A Case Letter. J. Oral Implant. 2018, 44, 287–291. [Google Scholar] [CrossRef]
- Franceschi, D.; Giuliani, V.; Giuntini, V.; Pini Prato, G.P.; Chambrone, L. Retrograde Peri-implantitis: Report of a Case Successfully Treated by Resection of the Implant Apex. Int. J. Periodontics Restor. Dent. 2021, 41, 443–448. [Google Scholar] [CrossRef]
- Rosendahl, K.; Dahlberg, G.; Kisch, J.; Nilner, K. Implant periapical lesion. A case series report. Swed. Dent. J. 2009, 33, 49–58. [Google Scholar]
- Dahlin, C.; Nikfarid, H.; Alsen, B.; Kashani, H. Apical peri-implantitis: Possible predisposing factors, case reports, and surgical treatment suggestions. Clin. Implant. Dent. Relat. Res. 2009, 11, 222–227. [Google Scholar] [CrossRef]
- Mohamed, J.B.; Alam, M.N.; Singh, G.; Chandrasekaran, S.C. The management of retrograde peri-implantitis: A case report. J. Clin. Diagn. Res. 2012, 6, 1600–1602. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, J.B.; Shivakumar, B.; Sudarsan, S.; Arun, K.V.; Kumar, T.S. Retrograde peri-implantitis. J. Indian Soc. Periodontol. 2010, 14, 57–65. [Google Scholar]
- Soldatos, N.; Romanos, G.E.; Michaiel, M.; Sajadi, A.; Angelov, N.; Weltman, R. Management of Retrograde Peri-Implantitis Using an Air-Abrasive Device, Er,Cr:YSGG Laser, and Guided Bone Regeneration. Case Rep. Dent. 2018, 2018, 7283240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayangco, L.; Sheridan, P.J. Development and treatment of retrograde peri-implantitis involving a site with a history of failed endodontic and apicoectomy procedures: A series of reports. Int. J. Oral Maxillofac. Implant. 2001, 16, 412–417. [Google Scholar]
- Ataullah, K.; Chee, L.F.; Peng, L.L.; Lung, H.H. Management of retrograde peri-implantitis: A clinical case report. J. Oral Implant. 2006, 32, 308–312. [Google Scholar] [CrossRef]
- Kusek, E.R. Immediate implant placement into infected sites: Bacterial studies of the Hydroacoustic effects of the YSGG laser. J. Oral Implant. 2011, 37, 205–211. [Google Scholar] [CrossRef]
- Choi, A.Y.; Reddy, C.M.; McGary, R.T.; Hill, R.B.; Swenson, D.T.; Seibel, P.; Hoag, J.M.; Berridge, J.P.; Johnson, T.M. Adjunctive Nd:YAG Laser Irradiation for Ridge Preservation and Immediate Implant Procedures: A Consecutive Case Series. Clin. Adv. Periodontics 2019, 9, 125–134. [Google Scholar] [CrossRef]
- Bretz, W.A.; Matuck, A.N.; de Oliveira, G.; Moretti, A.J.; Bretz, W.A. Treatment of retrograde peri-implantitis: Clinical report. Implant. Dent. 1997, 6, 287–290. [Google Scholar] [CrossRef]
- Kutlu, H.B.; Genc, T.; Tozum, T.F. Treatment of Refractory Apical Peri-Implantitis: A Case Report. J. Oral Implant. 2016, 42, 104–109. [Google Scholar] [CrossRef]
- Blanco, J.; Carral, C.; Argibay, O.; Linares, A. Implant placement in fresh extraction sockets. Periodontology 2000 2019, 79, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Wu, Y.; Xu, C.; Zhang, F. Immediate dental implant placement into infected vs. non-infected sockets: A meta-analysis. Clin. Oral Implant. Res. 2016, 27, 1290–1296. [Google Scholar] [CrossRef]
- Chen, H.; Zhang, G.; Weigl, P.; Gu, X. Immediate placement of dental implants into infected versus noninfected sites in the esthetic zone: A systematic review and meta-analysis. J. Prosthet. Dent. 2018, 120, 658–667. [Google Scholar] [CrossRef]
- Lee, C.T.; Chuang, S.K.; Stoupel, J. Survival analysis and other clinical outcomes of immediate implant placement in sites with periapical lesions: Systematic review. Int. J. Oral Maxillofac. Implant. 2015, 30, 268–278. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Camino, J.C.; Valmaseda-Castellon, E.; Gay-Escoda, C. Immediate implants placed in fresh sockets associated to periapical infectious processes. A systematic review. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e780–e785. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Martins, M.D.; Wennerberg, A. Immediate placement of implants into infected sites: A systematic review. Clin. Implant. Dent. Relat. Res. 2015, 17, e1–e16. [Google Scholar] [CrossRef] [PubMed]
- Esfahrood, Z.R.; Kadkhodazadeh, M.; Amid, R.; Rokn, A. Is The Periapical lesion a Risk For Periimplantitis? (A review). J. Dent. 2012, 9, 162–173. [Google Scholar]
- Crippa, R.; Aiuto, R.; Dioguardi, M.; Penarrocha-Diago, M.; Penarrocha-Diago, M.; Angiero, F. Laser Therapy for Infected Sites and Immediate Dental Implants in the Esthetic Zone: A Case Report and Review of Literature. Case Rep. Dent. 2020, 2020, 2328398. [Google Scholar] [CrossRef]
- Duqum, I.; Barker, S.; Marshall, E.; Wang, R.; Preisser, J.S.; Khan, A. The effect of single tooth implant restorations on the survival, morbidity, pulpal, and periapical health of adjacent teeth: A chart review. Clin. Implant. Dent. Relat. Res. 2018, 20, 479–482. [Google Scholar] [CrossRef] [PubMed]
- Meffert, R.M. Treatment of failing dental implants. Curr. Opin. Dent. 1992, 2, 109–114. [Google Scholar]
- Penarrocha-Diago, M.A.; Blaya-Tarraga, J.A.; Menendez-Nieto, I.; Penarrocha-Diago, M.; Penarrocha-Oltra, D. Implant survival after surgical treatment of early apical peri-implantitis: An ambispective cohort study covering a 20-year period. Int. J. Oral Implant. 2020, 13, 161–170. [Google Scholar]
- Penarrocha-Diago, M.; Maestre-Ferrin, L.; Penarrocha-Oltra, D.; Canullo, L.; Piattelli, A.; Penarrocha-Diago, M. Inflammatory implant periapical lesion prior to osseointegration: A case series study. Int. J. Oral Maxillofac. Implant. 2013, 28, 158–162. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Possible etiologies of implant periapical lesion (IPL): subject-associated factors, material-associated factors, and method-associated factors.
Figure 1.
Possible etiologies of implant periapical lesion (IPL): subject-associated factors, material-associated factors, and method-associated factors.

Figure 2.
Different examination findings of implant periapical lesion.

Figure 3.
Classification systems of implant periapical lesion based on various parameters.

Figure 4.
Treatment flowchart of implant periapical lesion. GBR, guided bone regeneration; S/S, symptoms and signs.
Figure 4.
Treatment flowchart of implant periapical lesion. GBR, guided bone regeneration; S/S, symptoms and signs.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chang, L.-C. Implant Periapical Lesion: A Narrative Review. Technologies 2021, 9, 65. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies9030065
AMA Style
Chang L-C. Implant Periapical Lesion: A Narrative Review. Technologies. 2021; 9(3):65. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies9030065
Chicago/Turabian StyleChang, Li-Ching. 2021. "Implant Periapical Lesion: A Narrative Review" Technologies 9, no. 3: 65. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies9030065
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.