
“Growing as a Stronger Clinician in Adverse Conditions”—A Snapshot of Clinical Training during COVID-19


Department of Clinical and Professional Practice, School of Clinical Medicine, University of KwaZulu-Natal, Durban 4041, South Africa
*
Author to whom correspondence should be addressed.
Educ. Sci. 2022, 12(3), 156; https://0-doi-org.brum.beds.ac.uk/10.3390/educsci12030156
Submission received: 20 December 2021
/
Revised: 12 January 2022
/
Accepted: 18 January 2022
/
Published: 24 February 2022
(This article belongs to the Special Issue Reshaping Higher Education for a Post-COVID-19 World: Lessons Learned and Moving Forward)
Abstract
:Transformative learning theory has been recommended as a pedagogy of uncertainty for accommodating new beliefs that enable humans to thrive amid the challenges and complexity of our world. As higher education institutions embrace new roles and responsibilities, few studies have focused on how the disruptions caused by COVID-19 may facilitate formative learning experiences. This study explored how registrars responded to the challenges facing clinical training during the first wave of COVID-19, and how the impact of these disruptions prompted personal and professional development. Registrars completed an online qualitative SWOT (strengths, weaknesses, opportunities, and threats) analysis of their training experiences during the COVID-19 pandemic. Data were thematically analysed. Four hundred and five responses were received from 54 registrars. Themes related to challenges included mental distress, resource constraints, and compromised and inadequate training. Themes related to strengths and opportunities included new learning experiences, resilience, coping strategies, and enhanced graduate competencies related to leadership, collaboration, communication, and health advocacy. The disruptive and disorienting elements of COVID-19, although situated in chaos, aggravating the constraints of training in under-resourced settings, also provided unexpected learning opportunities. These findings highlight the transformative potential of disrupted learning contexts and the need for responsive curricular to enhance graduate competencies, adaptability, and resilience.
1. Introduction
Pandemics can usher significant disruptive societal changes, requiring us to imagine society in new ways. As society changes, transformation becomes a primary medium through which adaptations to the changing environment may be viewed. For frontline health care workers (HCW), including registrars, who have been at the forefront of the changes ushered in by COVID-19, the need to adapt to the ever-changing demands of a rapidly evolving viral disease has been most acute [1,2]. COVID-19 has disrupted most learning contexts, with medical trainees responding to the crisis instead of focusing on academics [3]. Emergency departments in the COVID-19 responses became the new learning context in the absence of traditional academic learning contexts.
The literature on the pandemic has mainly focused on the impact, concerns, and challenges of COVID-19 [4,5,6], and on adapting medical education programmes [3,7,8,9]. The solutions to such problems have rested on the innovative power of online learning platforms and the ability of such innovations to overcome the challenge of disrupted learning [3,10]. Hence, for the most part, the medical education literature has focused on the institutional resources needed to respond to the challenges facing medical education during COVID-19 without paying sufficient attention to the transformations that students themselves need to make to meet the COVID-19-related challenges.
This study explores registrars’ experiences of clinical training during the COVID-19 crisis. Registrars are qualified doctors who undertake postgraduate specialist training in different medical disciplines [11]. Registrar roles are often perceived to be one of the most challenging in hospitals, as they constantly juggle training and service needs, especially in resource-constrained environments [5]. The importance of creating effective ways to foster the development of fully competent registrars [11] who are entering unpredictable medical environments [6] has highlighted the need for congruence between registrars’ training environments and learning requirements. However, COVID-19 disruptions have prevented registrars from working in ways that are in tandem with their training needs due to the refocus of resources towards dealing with a highly complex global pandemic. Al-Benna [12] has highlighted how surgical registrars deployed to areas outside of their scope of practice because of the COVID-19 response may need assistance to orient themselves to unfamiliar settings and the performance of competency-related tasks.
Further, while studies have charted the ensuing disruption of the COVID-19 pandemic, few have explored how these disruptions may facilitate formative learning experiences and the development of competencies and other attributes. In this study, we aimed to explore how registrars responded to the challenges of COVID-19 by conducting a SWOT (strengths, weaknesses, opportunities, and threats) analysis of registrars’ clinical training in the first wave of the crisis. We also sought to understand how the impact of the disruptions of the COVID-19 crisis could potentially trigger transformational learning opportunities, prompting new learning perspectives for the registrars.
Transformative learning is based on a notion of change where learners are challenged to “critically question and assess the integrity of their deeply held assumptions about how they relate to the world around them” [12]. In transformative learning, a need for personal change is stimulated by identifying a disorienting dilemma, which poses a challenge to the learner’s ability to continue learning as before. During the COVID-19 pandemic, clinical trainees had to respond to challenges that included unfamiliar learning experiences and learning outside the typical learning environment [13]. At the heart of the critical questioning central to transformative learning are questions of self-perspective, meaning systems, identities, roles, and abilities, all of which are objects of transformation in transformative learning.
Transformative learning theory is recommended as a pedagogy of uncertainty for health professions education in the 21st century to accommodate new beliefs that enable humans to thrive amid the challenges and complexity of our world [13]. Van Schalkwyk et al. described the conditions that “trigger” transformative learning to be an unfamiliar or atypical learning experience that may be “an intense, authentic learning experience or event that usually create a disorienting dilemma” that “may produce feelings of fear, discomfort, uncertainty, and vulnerability” [13]. Hence, in this paper, we further argue that the disruptions of the COVID-19 crisis created a context that could have triggered transformative learning opportunities for registrars despite the challenges posed by the COVID-19 crisis.
2. Materials and Methods
We conducted a SWOT (strengths, weaknesses, opportunities, and threats) analysis using an online qualitative survey. Qualitative surveys overcome resource and time constraints for researchers and participants and offer “a wide-angle lens,” equipping researchers with the ability to capture a diversity of experiences for an area of interest [14]. The SWOT framework is an effective situation analysis technique and planning tool that is used to inform the strategies and resource capabilities of a system or situation [15].
2.1. Setting
Successful registrar training in South Africa (SA) certifies medical practitioners for independent specialty practice in the country. Registrar training occurs over a four-year salaried period, during which registrars register for a Master of Medicine (MMed) programme at an academic institution. The work-based MMed programme includes clinical training, a research methodology course, and a research project via publication or a dissertation. Registrars work in the frontlines of specialised public sector referral (regional) hospitals governed by the SA Department of Health. The registrars in this study work and train in the public healthcare hospitals across the largest cities and towns of Kwa-Zulu Natal (KZN). KZN is one of nine provinces in SA. Public hospitals in SA serve non-fee-paying patients from the lower-income sector.
2.2. Data Collection
Since registrars working in the frontline of the COVID-19 responses may have limited time to participate in traditional interviews, data were collected via a self-administered online survey created using SurveyMonkey® [16]. The survey included a biographical section and eight open-ended questions. The questions focused on the personal and professional strengths, weaknesses, opportunities, and threats related to clinical training during the COVID-19 pandemic (e.g., list any personal strengths related to training to clinical training during the COVID-19 pandemic; list any profession-related strengths to clinical training during the COVID-19 pandemic). The survey was piloted with three registrars for face validity before the online hyperlink was shared via the WhatsApp® social media platform. Repeated reminders were sent to encourage volunteers to participate in the study.
2.3. Sample
We tried to sample registrars across the medical and surgical disciplines using snowball sampling. Snowball sampling was adopted for use in this study due to the constraints of COVID-19, which restricted access to the respondents. Representatives based at the different hospitals in KZN and in different medical and surgical disciplines were contacted by the primary investigator, who asked them to participate in the study and share the survey link with other registrars. Hence, registrars were invited to participate via their university representatives (discipline-nominated senior registrars) during the first wave of the COVID-19 pandemic (June–September 2020) in SA. The survey was kept open for over a month and closed after no new responses were received.
2.4. Data Analysis
We used thematic analysis to analyse the data. Thematic analysis is a qualitative method used for organising and analysing human experiences [17,18], and it has been used in healthcare settings such as psychology [17] and nursing [19,20]. We relied on descriptive codes and in vivo codes to generate the themes [17] that would form the object of our analysis. To minimise bias and enhance the credibility of the data analysis, both the authors (V.S.S. and D.S.) and a trained research assistant analysed the data independently.
We began by formatting the data into separate Microsoft Word tables (from an Excel spreadsheet) to show all the text per SWOT theme. This allowed us to focus on each swot category more closely and to analyse individual responses. We analysed the data sets for the categories within the SWOT themes, starting with a thorough reading of the data and then drawing some concept maps. Through this process, we manually assigned “descriptive codes” [21] to the various issues that cropped up repeatedly within participants’ responses. These codes (short phrases/single words) were then organised into categories (combining similar codes) according to our interpretation of what was being communicated by the participants, and their views on how their clinical learning was affected by the onset of the COVID-19 pandemic. This process also served to “condense and summarise the data rather than simply reduce them” [17,21]. The constant comparative method was used throughout the data analysis where the codes used to develop themes were constantly compared to other coded responses in the data set for similarities and differences [22].
Discrepancies between data analysts were discussed until a consensus was reached to increase the trustworthiness of the data analysis, as we recognise that coders are influenced by their beliefs, perceptions, and prior knowledge [22]. The categorising was also informed by the current literature, which consisted of opinion pieces and empirical studies of how clinical learning had been affected by the COVID pandemic and previous outbreaks of infectious diseases elsewhere. Since the questionnaires were collected anonymously, the respondents were unknown to the researchers.
This study received approval from the University of KwaZulu-Natal ethics committee (HSSREC/00001306/2020). All participants consented to take part.
3. Results
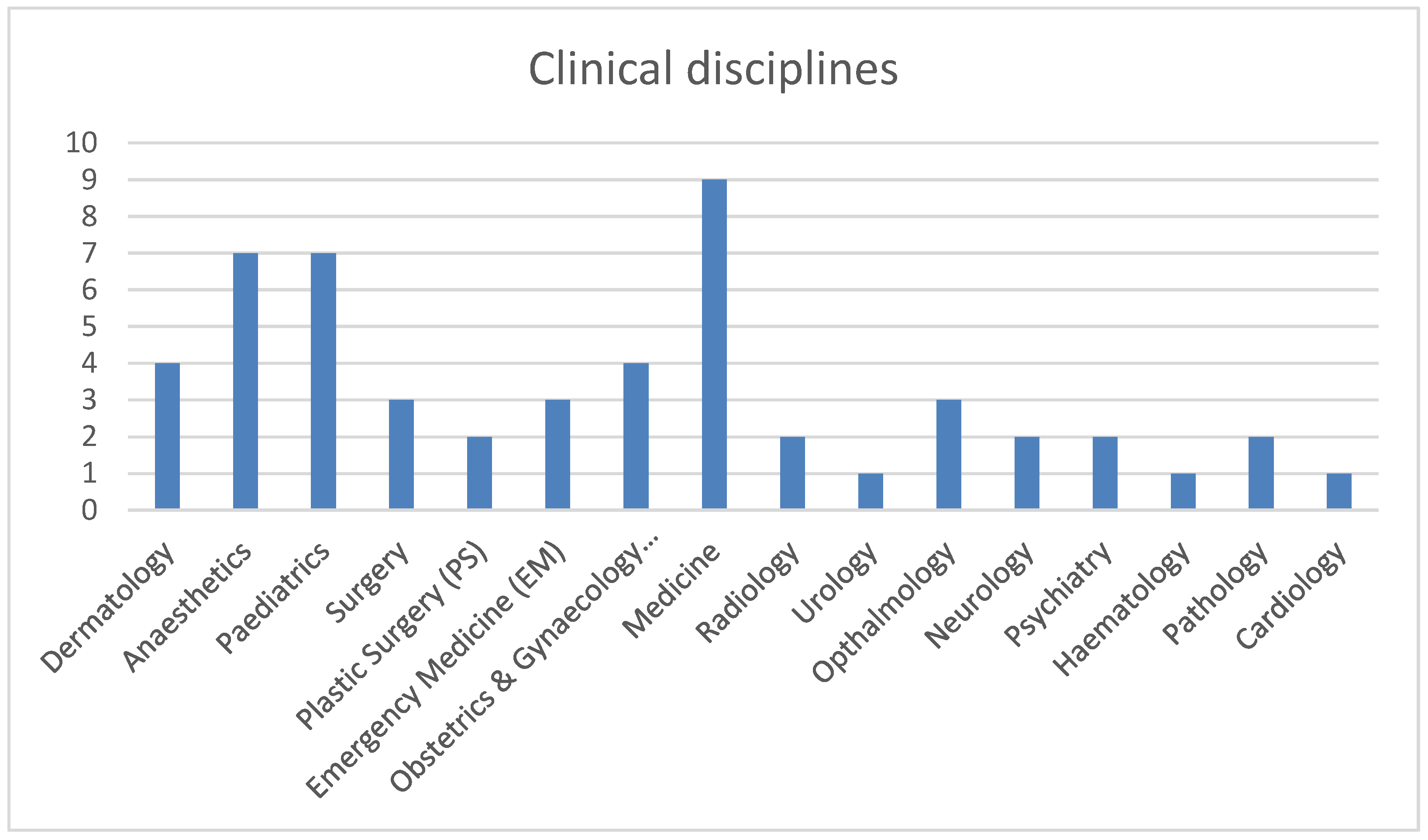
Fifty-four registrars from 16 clinical disciplines consented to participate in the study (Figure 1). The majority of the participants were women (74%), married (68%), and without children (57%). Figure 1 provides an overview of the participants’ disciplines. Four hundred and five responses were received across the SWOT domains. The majority of the responses related to weaknesses, closely followed by strengths, threats, and opportunities.
The major themes and subthemes are illustrated in Table 1. The themes emerging from weaknesses and threats were collectively described as challenges.
3.1. Challenges
3.1.1. Mental Distress
COVID-19 was described as a fear-provoking experience that was coupled with feelings of anxiety and uncertainty. Fear ranged from fear about the self (“COVID might kill me” (Anaesthetics-P18)) to family members (including a “constant fear of making our loved ones ill” (Paediatrics-P13) and “fear of hospital-acquired infection reaching elderly parents…and child” (Anaesthetics-P37)).
Registrars, especially those who had young children, described anxieties and uncertainty around the personal and professional sphere of their lives, which were exacerbated by the COVID-19 lockdown restrictions in South Africa, such as the closure of childcare facilities and travel restrictions:
“…very few childcare options …[and] kids are only at school intermittently… this means anything currently “optional” on a work-front is NOT getting done in my off time e.g., studying and MMED”.(Medicine-P32)
Other challenges reported by registrars related to the impact of isolation and lockdown measures occasioned by COVID-19:
“Being isolated from colleagues due to social distancing has had an impact on mental health”(Psychiatry-P43)
“Inability to see family has affected my psychological wellbeing so much, I’m not as productive as before”.(O&G-P41)
3.1.2. Resource Constraints and Systemic Deficiencies
Coupled with the pandemonium or chaos encountered during the COVID-19 crisis, registrars in already resource-constrained hospitals experienced even higher levels of stress and strain.
Registrars raised issues regarding the working conditions in their hospital settings as part of the weaknesses and threats experienced during clinical training:
“there are no resources or infrastructure”(Surgery-P28);
“extreme staff and resource shortages—gloves, masks”(EM-P14)
Inadequate human resources were also intensified, adding further strain on the existing skeleton staff “due to people contracting COVID” (Surgery-P9), with “inadequate nursing staff due to illness” (Ophthalmology-P27), and “sub-optimal consultant support on calls” (Medicine-P24). “Time constraints [and] Overload” (EM-P12) during a time when registrars found the “calibre of patients more demanding, requir[ing] more time to treat each patient” (Medicine-P24). Further, the “lack of protocols to deal with short-staffing, lack of testing following work exposure led to registrars [feeling like they] are the sacrificial lambs” (O&G-P30). Some registrars who were unable to identify or engage with any emergent learning opportunities were those who reported a lack of infrastructural and leadership support due to a “lack of support and empathy from seniors” (O&G-P15).
Registrars felt that not enough attention was given to the toll that the overwhelming COVID-19 pandemic would have on them, particularly by the leadership in these disciplines and institutions. They requested “better leadership and planning from the Department of Health” (Anaesthetics-P18) and felt that “COVID-19 has thrown every health care system into chaos, and the leaders at the top had time to plan but failed to do so adequately” (EM-P12).
3.1.3. Compromised and Inadequate Training
Clinical bedside teaching came to a halt during COVID-19. Further disaster management regulations and social distancing measures around learning in higher educational institutions meant that registrars could no longer attend academic and training sessions the way they used to, as “the pandemic ended ALL [sic] academic activities, and there is simply no time or capacity for anyone to attend any form of academic activity” (Medicine-P32). A registrar who reported “poor health” (Surgery-P28), both as a personal weakness and a personal threat, was unable to identify any learning opportunities that emerged during clinical training, indicating that perhaps their personal health concerns and fears may have hindered their learning opportunities.
Curtailed academic activity and training sessions led to registrars feeling anxious about missing contact time during training due to “limited ward rounds and teaching sessions around patients” (Neurology-P32). Due to COVID-19 demands, registrar training was redirected to deal with the COVID-19 crisis. Hence, registrars reported that “due to the pandemic I do not have gynae operating time” (O&G-P30). They also reported that they had “no elective surgical experience” (Surgery-P27) and “a lack of cases to practice clinical skills” (O&G-P41).
The lack of institutional communication regarding the completion of the training programmes were also described as challenges: “There is a lack of communication regarding where we as registrars stand in terms of continuation of training” (Surgery-P28). Due to the novelty of the COVID-19 crisis, registrars also highlighted their knowledge gaps and lack of training, as there was “minimal formal training on-site regarding updated protocols” (EM-P14)
3.2. Strengths and Opportunities
Resilience and Coping Strategies
Although three registrars were unable to identify any strengths and 14 were unable to identify any opportunities, others identified improvements in their “adaptive” (EM-P12) strengths, such as “courage and resilience” (O&G-P15), and found that they had the “opportunity to learn new coping mechanisms” (Pathology-P42).
In other cases, registrars recognised a psychological shift in themselves through “improved introspection” and “increased mindfulness of self and others during crisis” (Anaesthetics-P37). Registrars also began to appreciate the importance of self-care: “the fact that we are forced to do only urgent surgery has led to us being more rested, with stronger immune systems and more time to read” (Plastic Surgery-P10).
Further, help-seeking behaviours and self-awareness emerged amid the disruptions as registrars requested “more mental health support in [their] hospitals. Rather than just emails, look at sitting down with each registrar to assess mental health. We are all on the same journey, just taking different paths with different obstacles... all equally important” (O&G-P30).
3.3. Development of Graduate Competencies
3.3.1. Leadership
Though registrars felt overwhelmed with work, they also recognised the opportunities derived from “working out of [their] comfort zone” (EM-P12) and the opportunity to develop leadership competencies, such as “adaptability” and “flexibility” (Opthamology-P49). For example, one registrar reported that she saw an “opportunity to think outside of the box, i.e., devising systems to handle stable outpatients in order to avoid unnecessary influx of patients in the hospital environment” (Paediatrics-P33). In this instance, the registrar solved the problem of high patient influx by devising strategies that allowed them to overcome the problem of increased patient volumes. A registrar from Medicine (P32) reported “learning to triage patients with reference to who can I help and who can’t I help” to cope with the overload of patients. Registrars also “practice[d] ‘making a plan’ in severely sub-optimal conditions” (Medicine-P32) and reported “staying focused amidst all the uncertainty and fear whilst recognising the opportunity to be a “health advocate and leader” (Paediatrics-P13).
3.3.2. Health Advocacy, Collaboration, and Communication
Collaboration and communication were registered as positives alongside health advocacy during this crisis. Many Registrars reported that training during the COVID-19 crisis created opportunities for becoming “communicators and collaborators” (Anaesthetics-P4) and helped them “grow as a health advocate” (Anaesthetics-P18) as they were “able to be an advocate for patients and other colleagues” (Paediatrics-P50). Others also reported that in the COVID-19 crisis, “there has definitely been a need for more collaboration” (Psychiatry-P43) and an “opportunity to learn about other methods of communication” (O&G-P41). In the absence of formal counselling, another registrar reported the “counselling of nurses and appreciation for the ancillary staff” (Neurology-P34) as opportunities that arose during the pandemic. Registrars’ adoption of health advocacy could be linked to their criticism of the leadership responses described in the challenges reported in this analysis. Registrars took the lead in advocating responsively to gaps that they felt undermined their wellbeing and the wellbeing of others around them.
3.4. New Learning and Training Opportunities
Registrars found that the “increased availability and awareness of online learning opportunities” led to “increased academic activities due to online access platforms” (Ophthalmology-P27). Registrars also appreciated the new sharing and access to information created globally during the pandemic, reporting that “most courses are online” (Anaesthetics-P18). There was also an “improved attendance of clinical meetings with use of virtual platforms such as Zoom” (Paediatrics-P33), and “a sponsorship to attend virtual international conference” (Psychiatry-P43). Hence, registrars embraced the new learning and training opportunities, which also enhanced their self-directed, life-long learning skills: “I’m able to use evidence-based medicine” (Paediatrics-P50).
4. Discussion
In tandem with studies that have found fear amongst HCWs at the forefront of the COVID-19 response [23,24], our study also registered feelings of fear, anxiety, and despair amongst most registrars. However, registrars also recognised opportunities and developed strategies to help them allay these fears by utilising their personal and professional strengths. The registrars’ recognition of strengths and their ability to act on emerging opportunities in ways that transformed their personal and professional lives may be viewed as occurring within a learning context that, although characterised by disruption and disorientation, held great transformative learning potential [8,9]. However, this study also found that some registrars were unable to respond and engage “with the unfamiliar learning experiences” [25]; hence, transformative learning may not have occurred [13]. Registrars who were unable to identify any transformative shifts in the form of opportunities or abilities to act on emerging opportunities were those who reported a lack of leadership, infrastructural, and staff support, and poor health conditions. Registrars who reported negatively on personal or professional strengths in opposition to those who reported positive personal attributes, such as resilience, courage, or personal leadership skills, also did not list any opportunities. Research has demonstrated that learners have different transformative learning capacities and that not all learners may resolve disorienting dilemmas simultaneously [25]. These differences highlight individual, structural, and social factors that could hinder their transformative learning potential.
This study highlighted how the pandemic aggravated the constraints of under-resourced work-based healthcare training sectors, such as in SA, where there is one specialist doctor per 11,000 people in the public sector (as opposed to 1: <500 in the private sector) [26]. Similar to other countries [27], the registrars in this study also expressed concerns regarding the lack of resources and shortage of PPE. Given the double dilemma of having their worlds shifted and not having enough basic materials to keep themselves safe, registrars devised practical strategies to help them manage, such as the effective triaging of patients and thinking carefully about which patients to prioritise to reduce high patient loads under very demanding circumstances. Registrars spoke about developing a sense of mindfulness, which has been reported elsewhere, and which they found to be helpful [28,29]. We see, developing in connection to this mindfulness, themes around health advocacy, with registrars initiating solutions and changes in response to their patients’ and colleagues’ needs, developing skills outside of their usual scope of practice.
These developments included, for example, the registrars themselves taking up roles whereby they provided informal counselling to their peers and some of their patients in the absence of formal channels of psychological support. It has been found that frontline workers are usually psychologically the most impacted upon during frontline responses [30]. Although the provision of informal psychological and therapeutic support by healthcare workers to other healthcare workers has not yet been fully explored, Polizzi, Lynn, and Perry have commented on it in terms of trauma responses to other events, such as the September 9/11 attacks in the US [24]. They reported that, during the aftermath of the attacks, “many experienced a sense of control, self-esteem, and belonging by providing emotional and practical support to family, friends, and the larger community and interpreted their actions in a positive manner” [24]. By taking responsibility for providing psychological support to colleagues, registrars were able to allay fears and provide continuity for the settings they were in. As a development out of the crisis, we would recommend that the role of informal psychological techniques be investigated further.
The registrars highlighted an important facet of crisis response. As with other crises inflected by discourses of disorientation, the grand narrative directing the COVID-19 response rested on global as well as national experts, remaining focused only on the pandemic response without considering other less directly COVID-19-related aspects of communication to registrars. For example, the registrars lamented the lack of clarity around continuing their training from their academic institutions, something they would have found reassurance in, while responding to COVID-19. The registrars’ lamentation highlighted that no unit of communication is ever too small to reassure those affected by the crisis in such situations. Out of this realisation arose their criticism of some of the decisions taken at the broader national institutional level.
Further increased service loads brought on by the pandemic have exacerbated the constant conflict between service and training in registrar training [31]. This area warrants further attention post-pandemic, and extended training contracts should be considered to make up for the loss of clinical and operative experience due to the specialist training schedules being interrupted and replaced by COVID-19 rotations. The extended training contracts would ease the anxieties and concerns about not having time to acquire the necessary specialist-specific competencies.
Almost overnight, a significant transformation to have emerged from the COVID-19 pandemic in medical education is the move to online learning platforms [32] to deal with disruptions in education and training. Unlike other findings that have reported significant problems in HCWs’ ability to adapt to online platforms [33,34], we found that the registrars adapted with much ease and appreciation for online platforms. Registrars harnessed these online learning sessions, which seemed to encourage greater attendance and the development of life-long learning skills.
We also found that the COVID-19 crisis changed the registrars’ perspectives related to wellbeing and self-care. It highlighted, for them, the importance of investing in their physical and mental wellbeing. Registrars must continue to be encouraged and empowered to engage in self-care and improve their working lives during and after the pandemic [8].
An interesting finding of this study relates to instances where registrars had taken up leadership roles in ways that they felt would best suit the circumstances in which they found themselves. Registrars also embraced opportunities to develop other core competencies, such as collaboration, communication, and health advocacy, facets of learning that have been described as integral to developing competent clinicians [35,36]. These findings strengthen the call for organisations to “support these unsung heroes” by including formal leadership programmes to enhance registrar training [37] and graduate competencies. We argue that the COVID-19 crisis provided a space in which the registrars could take up these roles and add to their competencies in ways that may not have been immediately possible outside of the disorientating dilemmas created by COVID-19.
This study has highlighted how the disruptions of the pandemic could be viewed as transformational learning opportunities in a crisis, which could lead to new perspectives relating to personal coping strategies and enhanced graduate competencies in postgraduate clinical training. Registrars recognised and embraced the new learning experiences linked to their clinical knowledge and skills development, while also reflecting on their leadership, collaboration, health advocacy, and professionalism competencies. Our study also adds to the growing body of evidence highlighting the importance of the human factors of medicine’s hidden curriculum that are critical for healthcare today [5].
In conclusion, postgraduate medical training during the COVID-19 pandemic not only posed challenges for the registrars, but also contributed to them “growing as stronger clinician[s] in adverse conditions” (Anaesthetics-P45).
5. Limitations and Concluding Remarks
A limited sample size may limit the generalisability of the findings in this study due to bias, and because resources and infrastructure may differ between regions. However, this study aimed to provide a snapshot of work-based clinical training to facilitate and inform future interventions during the pandemic.
This study did not focus on sex and discipline differences between the registrars. Since the majority of respondents were women, there is a possibility of bias by way of the survey reflecting feelings and attitudes that may be sex specific. Further, the data were collectively analysed without considering discipline-specific nuances due to the small number of registrar responses within the different disciplines. Hence, gender and differences between disciplines warrant further investigation.
Survey-based studies may limit an in-depth analysis. Future studies should include interviews with the work-based trainers to provide a much more in-depth, inclusionary account of the formative experiences of clinical training during a pandemic.
Psychological stress has been identified as one of the major impacts on HCWs during the COVID-19 pandemic. The continued use of online platforms to implement wellbeing interventions, such as mindfulness training [38], and virtual training for registrars to provide a sense of continuity with the possibility of alleviating the negative impact of disruptions [2,3] are recommended. Such strategies should also be implemented in routine training to help registrars adapt and adjust to unpredictable learning environments. Recent research has looked towards the theoretical underpinnings of self-directed learning (SDL), where learners take the initiative to address their learning needs with or without the support of others in disrupted learning environments [39]. SDL was recommended as a core competency and as an essential component of responsive curricula that empowers trainees to identify and implement relevant learning strategies to optimise disrupted clinical training [39].
Our reflexivity statement in this study centres on issues of positionality and paradigmatic worldviews that may have impinged on our interpretation of the data. V.S.S. being a medical educationalist with interest in understanding the challenges and opportunities of constrained training contexts, especially during the pandemic, and positioned academically in a transformative learning theory paradigm, meant that there was a constant risk of confirmation bias in terms of transformative learning. D.S. being a postdoctoral researcher in medical education with a critical health psychology paradigmatic orientation, which is critical (and often suspicious) of institutional practices, there was the ever-present risk of this critical position impinging negatively on the researcher’s interpretation of participants challenges. To reduce both these potential biases, the data analysis process was kept transparent through constant consultations between V.S.S. and D.S. as we tried to read and interpret the data objectively.
Author Contributions
V.S.S. contributed to the study conception, design, and development of the survey instrument, and the development of the manuscript. D.A.N.S. assisted with the analysis of the data and the development of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study received approval from the University of KwaZulu-Natal ethics committee (HSSREC/00001306/2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request. The data are not publicly available for reasons pertaining to authors’ participant anonymity considerations.
Acknowledgments
Special thanks to S. Pillay, a senior clinician, for his valued comments on the final draft of the manuscript and the registrars who made time to respond and share the questionnaire with their colleagues.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Moonasar, D.; Pillay, A.; Leonard, E.; Naidoo, R.; Mngemane, S.; Ramkrishna, W.; Jamaloodien, K.; Lebese, L.; Chetty, K.; Bamford, L.; et al. COVID-19: Lessons and experiences from South Africa’ ’s first surge. BMJ Glob. Health 2021, 6, e004393. [Google Scholar] [CrossRef]
- Konopińska, J.; Obuchowska, I.; Lisowski, Ł.; Dub, N.; Dmuchowska, D.A.; Rękas, M. Impact of the COVID-19 pandemic on ophthalmic specialist training in Poland. PLoS ONE 2021, 16, e0257876. [Google Scholar] [CrossRef]
- Payne, A.; Rahman, R.; Bullingham, R.; Vamadeva, S.; Alfa-Wali, M. Redeployment of surgical trainees to intensive care during the COVID-19 pandemic: Evaluation of the impact on training and wellbeing. J. Surg. Educ. 2021, 78, 813–819. [Google Scholar] [CrossRef]
- Al-Hayouti, H.; Hinds, A.M.; Adams, G.G. Impact of COVID-19 on preparation for the Certificate of Eligibility for Specialist Registration (CESR) in Ophthalmology. Eye 2021, 27, 1–4. [Google Scholar] [CrossRef]
- Nedungadi, A.; Ming, C.; Woodward, F.; Lasoye, T.; Birns, J. Supporting the transition to becoming a medical registrar. Future Healthc. J. 2021, 8, e160–e163. [Google Scholar] [CrossRef] [PubMed]
- Clements, J.M.; Burke, J.; Nally, D.; Rabie, M.; Kane, E.; Barlow, E.; Mohamed, W.; King, M.; McClymont, L.; George, M.; et al. COVID-19 impact on Surgical Training and Recovery Planning (COVID-STAR)-A cross-sectional observational study. Int. J. Surg. 2021, 88, 105903. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.; Radke, H. Reshaping surgical specialist training in small animal surgery during and after the COVID-19 pandemic. Vet. Surg. 2021, 50, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Hilburg, R.; Patel, N.; Ambruso, S.; Biewald, M.A.; Farouk, S.S. Medical education during the Coronavirus Disease-2019 pandemic: Learning from a distance. Adv. Chronic Kidney Dis. 2020, 27, 412–417. [Google Scholar] [CrossRef]
- Woolliscroft, J.O. Innovation in response to the COVID-19 pandemic crisis. Acad. Med. 2020, 95, 1140–1142. [Google Scholar] [CrossRef]
- Forsythe, R.O.; Suttie, S.A. Enhancing junior doctors’ working lives. Surgery 2020, 38, 607–611. [Google Scholar] [CrossRef]
- Bagwandeen, C.I.; Singaram, V.S. Feedback as a means to improve clinical competencies: Registrars’ perceptions of the quality of feedback provided by consultants in an academic hospital setting. Afr. J. Health Prof. Educ. 2016, 8, 117–120. [Google Scholar] [CrossRef] [Green Version]
- Mezirow, J.; Taylor, E.W. Transformative Learning in Practice: Insights from Community, Workplace, and Higher Education; John Wiley & Sons: San Francisco, CA, USA, 2009. [Google Scholar]
- Van Schalkwyk, S.C.; Hafler, J.; Brewer, T.F.; Maley, M.A.; Margolis, C.; McNamee, L.; Meyer, I.; Peluso, M.J.; Schmutz, A.M.; Spak, J.M.; et al. Transformative learning as pedagogy for the health professions: A scoping review. Med. Educ. 2019, 53, 547–558. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V.; Boulton, E.; Davey, L.; McEvoy, C. The online survey as a qualitative research tool. Int. J. Soc. Res. Methodol. 2020, 16, 1–4. [Google Scholar] [CrossRef]
- Emet, G.; Tat, M. Swot analysis: A theoretical review. J. Int. Soc. Res. 2017, 10, 994–1006. [Google Scholar] [CrossRef]
- SurveyMonkey Inc. Available online: www.surveymonkey.com (accessed on 14 December 2021).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Boyatzis, R.E. Transforming Qualitative Information: Thematic Analysis and Code Development; Sage: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Jones, J.; Turunen, H.; Snelgrove, S. Theme development in qualitative content analysis and thematic analysis. J. Nurs. Educ. 2016, 6, 100–110. [Google Scholar] [CrossRef] [Green Version]
- Saldaña, J. The Coding Manual for Qualitative Researchers, 2nd ed.; SAGE: London, UK, 2013. [Google Scholar]
- Glaser, B.G. The constant comparative method of qualitative analysis. Soc. Probl. 1965, 12, 436–445. [Google Scholar] [CrossRef]
- Breakwell, G.M.; Jaspal, R. Identity change, uncertainty and mistrust in relation to fear and risk of COVID-19. J. Risk Res. 2020, 24, 335–351. [Google Scholar] [CrossRef]
- Polizzi, C.; Lynn, S.J.; Perry, A. Stress and coping in the time of COVID-19: Pathways to resilience and recovery. Clin. Neuropsychiatry 2020, 17, 59–62. [Google Scholar]
- Deveci, T. The transformative learning experiences of learners of English as a foreign language at a university preparatory programme. Transform. Dialogues Teach. Learn. J. 2014, 7, 1–19. [Google Scholar]
- Maseko, L.; Harris, B. People-centeredness in health system reform. Public perceptions of private and public hospitals in South Africa. S. Afr. J. Occup. Ther. 2018, 48, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Bradshaw, R.A.; Stahl, P.D. On pandemics, pandemonium, and possibilities…. FASEB BioAdv. 2020, 2, 329. [Google Scholar] [CrossRef] [Green Version]
- Matiz, A.; Fabbro, F.; Paschetto, A.; Cantone, D.; Paolone, A.R.; Crescentini, C. Positive impact of mindfulness meditation on mental health of female teachers during the COVID-19 outbreak in Italy. Int. J. Environ. Res. Public Health 2020, 17, 6450. [Google Scholar] [CrossRef]
- Yıldırım, M.; Arslan, G.; Özaslan, A. Perceived risk and mental health problems among healthcare professionals during COVID-19 pandemic: Exploring the mediating effects of resilience and coronavirus fear. Int. J. Ment. Health Addict. 2020, 16, 1–11. [Google Scholar] [CrossRef]
- Blake, H.; Bermingham, F.; Johnson, G.; Tabner, A. Mitigating the psychological impact of COVID-19 on healthcare workers: A digital learning package. Int. J. Environ. Res. Public Health 2020, 17, 2997. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, L.; Mash, B.; Derese, A. The national portfolio of learning for postgraduate family medicine training in South Africa: Experiences of registrars and supervisors in clinical practice. BMC Med. Educ. 2013, 13, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Sharma, D.; Bhaskar, S. Addressing the COVID-19 burden on medical education and training: The role of telemedicine and tele-education during and beyond the pandemic. Front. Public Health 2020, 8, 838. [Google Scholar] [CrossRef]
- Shufutinsky, A.; DePorres, D.; Long, B.; Sibel, J.R. Shock Leadership Development for the Modern Era of Pandemic Management and Preparedness. Int. J. Organ. Innov. 2020, 13, 1–23. [Google Scholar]
- Shehata, M.H.; Abouzeid, E.; Wasfy, N.F.; Abdelaziz, A.; Wells, R.L.; Ahmed, S.A. Medical education adaptations post COVID-19: An Egyptian reflection. J. Med. Educ. Curric. Dev. 2020, 7, 2382120520951819. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.R.; Danoff, D. The CanMEDS initiative: Implementing an outcomes-based framework of physician competencies. Med. Teach. 2007, 29, 642–647. [Google Scholar] [CrossRef]
- Wood, V.; Flavell, A.; Vanstolk, D.; Bainbridge, L.; Nasmith, L. The road to collaboration: Developing an interprofessional competency framework. J. Interprof. Care 2009, 23, 621–629. [Google Scholar] [CrossRef]
- Blake, T.; Whallett, A. Leadership and the medical registrar: How can organisations support these unsung heroes? Postgrad. Med. J. 2016, 92, 735–740. [Google Scholar] [CrossRef]
- Osman, I.; Hamid, S.; Singaram, V. Efficacy of a brief online mindfulness-based intervention on the psychological well-being of health care professionals and trainees during the COVID-19 pandemic: A mixed method design. Health SA Gesondheid 2021, 26, a1882. [Google Scholar] [CrossRef]
- Singaram, V.S.; Naidoo, K.L.; Singh, S. Self-Directed Learning during the COVID-19 Pandemic: Perspectives of South African Final-Year Health Professions Students. Adv. Med. Educ. Pract. 2022, 13, 1–13. [Google Scholar] [CrossRef]
Figure 1.
Number of registrar participants in the survey by clinical discipline.


{kind=link}
Table 1.
Major themes and subthemes.
| Challenges | Strengths and Opportunities |
|---|---|
| Mental distress Resource constraints/system deficiencies Compromised and inadequate training | Resilience and coping strategies Development of competencies
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Singaram, V.S.; Sofika, D.A.N. “Growing as a Stronger Clinician in Adverse Conditions”—A Snapshot of Clinical Training during COVID-19. Educ. Sci. 2022, 12, 156. https://0-doi-org.brum.beds.ac.uk/10.3390/educsci12030156
AMA Style
Singaram VS, Sofika DAN. “Growing as a Stronger Clinician in Adverse Conditions”—A Snapshot of Clinical Training during COVID-19. Education Sciences. 2022; 12(3):156. https://0-doi-org.brum.beds.ac.uk/10.3390/educsci12030156
Chicago/Turabian StyleSingaram, Veena S., and Dumisa A. N. Sofika. 2022. "“Growing as a Stronger Clinician in Adverse Conditions”—A Snapshot of Clinical Training during COVID-19" Education Sciences 12, no. 3: 156. https://0-doi-org.brum.beds.ac.uk/10.3390/educsci12030156
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.