
Efficacy of an Integrated Simulation-Based Education Approach to Train Non-Technical Skills in Medical Undergraduate Students

Abstract
:1. Introduction
2. Methods
2.1. Ethical Considerations
2.2. Study Setting and Participants
Exemplary Operational Sequence of a Training
2.3. Assessment of the Outcome Measures: NTS Performance
2.4. AS-NTS Is Composed of Three Dimensions
- Planning tasks, prioritising and problem-solving,
- Teamwork and leadership,
- Team orientation.
3. Statistical Analysis
4. Results
4.1. Participants and Assessment of NTS
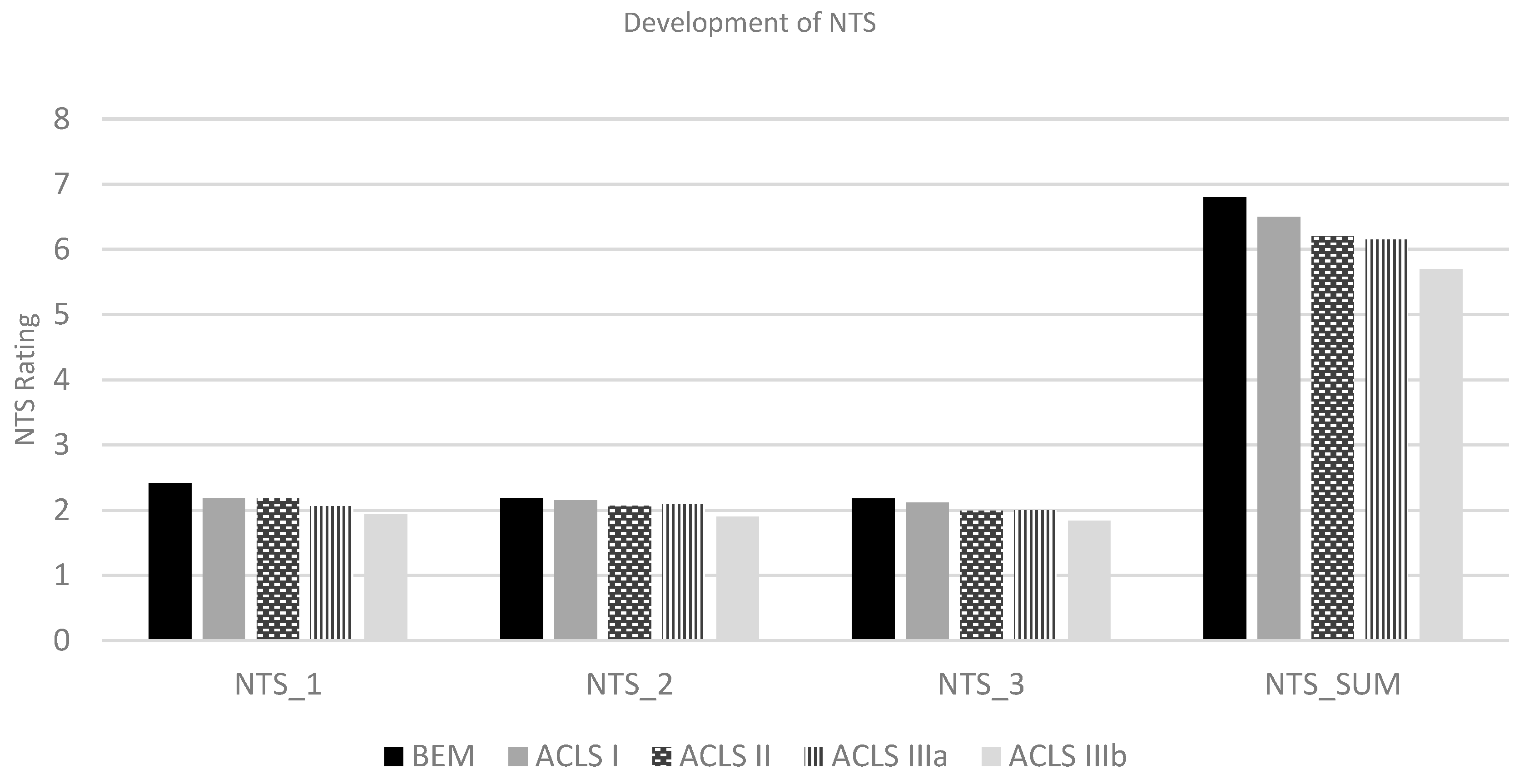
4.2. Outcome Measures: NTS Performance
4.3. Primary Endpoint: Overall NTS Performance
4.4. Secondary Endpoint: NTS Performance of Each Dimension
4.4.1. Dimension One: Planning Tasks, Prioritising and Problem-Solving
4.4.2. Dimension Two: Teamwork and Leadership
4.4.3. Dimension Three: Team Orientation
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Donaldson, M.S.; Corrigan, J.M.; Kohn, L.T. To Err Is Human: Building a Safer Health System; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Flin, R.H.; O’Connor, P.; Crichton, M. Safety at the Sharp End: A Guide to Non-Technical Skills; Ashgate Publishing, Ltd.: Farnham, UK, 2008. [Google Scholar]
- Stewart, G.L.; Barrick, M.R. Team structure and performance: Assessing the mediating role of intrateam process and the moderating role of task type. Acad. Manag. J. 2000, 43, 135–148. [Google Scholar] [CrossRef]
- Weinger, M.B. Experience ≠ ExpertiseCan Simulation Be Used to Tell the Difference? J. Am. Soc. Anesthesiol. 2007, 107, 691–694. [Google Scholar] [CrossRef] [PubMed]
- Prineas, S.; Mosier, K.; Mirko, C.; Guicciardi, S. Non-Technical Skills in Healthcare. In Textbook of Patient Safety and Clinical Risk Management; Springer: Berlin/Heidelberg, Germany, 2021; pp. 413–434. [Google Scholar]
- Cooper, J.B.; Newbower, R.S.; Long, C.D.; McPeek, B. Preventable anesthesia mishaps: A study of human factors. Anesthesiology 1978, 49, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Howard, S.K.; Gaba, D.M.; Fish, K.J.; Yang, G.; Sarnquist, F.H. Anesthesia crisis resource management training: Teaching anesthesiologists to handle critical incidents. Aviat. Space Environ. Med. 1992, 63, 763–770. [Google Scholar] [PubMed]
- Cannon-Bowers, J.A.; Salas, E. Team performance and training in complex environments: Recent findings from applied research. Curr. Dir. Psychol. Sci. 1998, 7, 83–87. [Google Scholar] [CrossRef]
- Cockpit Resource Management; Orlady, H.W.; Foushee, H.C. (Eds.) Training. In Cockpit Resource Management Training Workshop; Air Force Military Airlift Command; NASA Ames Research Center: Moffett Field, CA, USA, 1987. [Google Scholar]
- Helmiö, P.; Blomgren, K.; Takala, A.; Pauniaho, S.L.; Takala, R.; Ikonen, T. Towards better patient safety: WHO Surgical Safety Checklist in otorhinolaryngology. Clin. Otolaryngol. 2011, 36, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Dunsford, J. Structured communication: Improving patient safety with SBAR. Nurs. Women’s Health 2009, 13, 384–390. [Google Scholar] [CrossRef]
- Lee, M.; Fanelli, F.; Haage, P.; Hausegger, K.; Van Lienden, K. Patient safety in interventional radiology: A CIRSE IR checklist. Cardiovasc. Interv. Radiol. 2012, 35, 244–246. [Google Scholar] [CrossRef]
- Sevdalis, N.; Hull, L.; Birnbach, D. Improving patient safety in the operating theatre and perioperative care: Obstacles, interventions, and priorities for accelerating progress. Br. J. Anaesth. 2012, 109, i3–i16. [Google Scholar] [CrossRef]
- Kiesewetter, J.; Gutmann, J.; Drossard, S.; Salas, D.G.; Prodinger, W.; Mc Dermott, F.; Urban, B.; Staender, S.; Baschnegger, H.; Hoffmann, G.; et al. The Learning Objective Catalogue for Patient Safety in Undergraduate Medical Education—A Position Statement of the Committee for Patient Safety and Error Management of the German Association for Medical Education. GMS J. Med. Educ. 2016, 33. [Google Scholar] [CrossRef]
- Walton, M.; Woodward, H.; Van Staalduinen, S.; Lemer, C.; Greaves, F.; Noble, D.; Ellis, B.; Donaldson, L.; Barraclough, B. Republished paper: The WHO patient safety curriculum guide for medical schools. Postgrad. Med. J. 2011, 87, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Gassmann, B.; Haller, J.; Täuber, M.; Suter, P.M. Der Medizinischen Wissenschaften SA Projekt Zukunft Medizin Schweiz—Phase lll–Aus-und Weiterbildung in Patientensicherheit und Fehlerkultur; Schweizerische Akademie der Medizinischen Wissenschaften: Bern, Switzerland, 2007. [Google Scholar]
- WHO. WHO Patient Safety Curriculum Guide for Medical Schools 2009. Available online: https://www.who.int/patientsafety/activities/technical/who_ps_curriculum.pdf (accessed on 15 December 2021).
- Lee, A.; Finstad, A.; Gawad, N.; Boet, S.; Raiche, I.; Balaa, F. Nontechnical skills (NTS) in the undergraduate surgical and anesthesiology curricula: Are we adequately preparing medical students? J. Surg. Educ. 2021, 78, 502–511. [Google Scholar] [CrossRef] [PubMed]
- Greif, R.; Bhanji, F.; Bigham, B.L.; Bray, J.; Breckwoldt, J.; Cheng, A.; Duff, J.P.; Gilfoyle, E.; Hsieh, M.-J.; Iwami, T.; et al. Education, Implementation, and Teams: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2020, 142, S222–S283. [Google Scholar] [CrossRef] [PubMed]
- Lynch, A. (Ed.) Simulation-Based Acquisition of Non-Technical Skills to Improve Patient Safety. In Seminars in Pediatric Surgery; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- McGaghie, W.C. Assessing readiness for medical education: Evolution of the medical college admission test. JAMA 2002, 288, 1085–1090. [Google Scholar] [CrossRef] [PubMed]
- Yee, B.; Naik, V.N.; Joo, H.S.; Savoldelli, G.L.; Chung, D.Y.; Houston, P.L.; Karatzoglou, B.J.; Hamstra, S.J. Nontechnical skills in anesthesia crisis management with repeated exposure to simulation-based education. J. Am. Soc. Anesthesiol. 2005, 103, 241–248. [Google Scholar] [CrossRef]
- Moll-Khosrawi, P.; Zöllner, C.; Cencin, N.; Schulte-Uentrop, L. Flipped learning enhances non-technical skill performance in simulation-based education: A randomised controlled trial. BMC Med. Educ. 2021, 21, 353. [Google Scholar] [CrossRef]
- Hagemann, V.; Herbstreit, F.; Kehren, C.; Chittamadathil, J.; Wolfertz, S.; Dirkmann, D.; Kluge, A.; Peters, J. Does teaching non-technical skills to medical students improve those skills and simulated patient outcome? Int. J. Med. Educ. 2017, 8, 101. [Google Scholar] [CrossRef]
- Gordon, M.; Darbyshire, D.; Baker, P. Non-technical skills training to enhance patient safety: A systematic review. Med. Educ. 2012, 46, 1042–1054. [Google Scholar] [CrossRef]
- Zausig, Y.A.; Grube, C.; Boeker-Blum, T.; Busch, C.J.; Bayer, Y.; Sinner, B.; Zink, W.; Schaper, N.; Graf, B.M. Inefficacy of simulator-based training on anaesthesiologists’ non-technical skills. Acta Anaesthesiol. Scand. 2009, 53, 611–619. [Google Scholar] [CrossRef]
- O’Connor, P.; Campbell, J.; Newon, J.; Melton, J.; Salas, E.; Wilson, K.A. Crew resource management training effectiveness: A meta-analysis and some critical needs. Int. J. Aviat. Psychol. 2008, 18, 353–368. [Google Scholar] [CrossRef]
- Peters, S.; Clarebout, G.; Diemers, A.; Delvaux, N.; Verburgh, A.; Aertgeerts, B.; Roex, A. Enhancing the connection between the classroom and the clinical workplace: A systematic review. Perspect. Med. Educ. 2017, 6, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Brauer, D.G.; Ferguson, K.J. The integrated curriculum in medical education: AMEE Guide No. 96. Med. Teach. 2015, 37, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S. Concepts of vertical and horizontal integration as an approach to integrated curriculum. Educ. Med. J. 2013, 5, 1–5. [Google Scholar] [CrossRef]
- Wijnen-Meijer, M.; Van den Broek, S.; Koens, F.; Ten Cate, O. Vertical integration in medical education: The broader perspective. BMC Med. Educ. 2020, 20, 509. [Google Scholar] [CrossRef]
- Harden, R.M. What is a spiral curriculum? Med. Teach. 1999, 21, 141–143. [Google Scholar] [CrossRef]
- Krage, R.; Zwaan, L.; Len, L.T.S.; Kolenbrander, M.W.; Van Groeningen, D.; Loer, S.A.; Wagner, C.; Schober, P. Relationship between non-technical skills and technical performance during cardiopulmonary resuscitation: Does stress have an influence? Emerg. Med. J. 2017, 34, 728–733. [Google Scholar] [CrossRef]
- Groombridge, C.J.; Kim, Y.; Maini, A.; Fitzgerald, M.C. Stress and decision-making in resuscitation: A systematic review. Resuscitation 2019, 144, 115–122. [Google Scholar] [CrossRef]
- Sweller, J. Cognitive Load Theory. In Psychology of Learning and Motivation; Elsevier: Amsterdam, The Netherlands, 2011; pp. 37–76. [Google Scholar]
- Moll-Khosrawi, P.; Kamphausen, A.; Hampe, W.; Schulte-Uentrop, L.; Zimmermann, S.; Kubitz, J.C. Anaesthesiology students’ Non-Technical skills: Development and evaluation of a behavioural marker system for students (AS-NTS). BMC Med. Educ. 2019, 19, 205. [Google Scholar] [CrossRef]
- Peate, I.; Brent, D. Using the ABCDE approach for all critically unwell patients. Br. J. Healthc. Assist. 2021, 15, 84–89. [Google Scholar] [CrossRef]
- Lix, L.M.; Keselman, J.C.; Keselman, H.J. Consequences of Assumption Violations Revisited: A Quantitative Review of Alternatives to the One-Way Analysis of Variance F Test. Rev. Educ. Res. 1996, 66, 579–619. [Google Scholar]
- Sollid, S.J.; Dieckman, P.; Aase, K.; Søreide, E.; Ringsted, C.; Østergaard, D. Five topics health care simulation can address to improve patient safety: Results from a consensus process. J. Patient Saf. 2019, 15, 111. [Google Scholar] [CrossRef] [PubMed]
- Goldshtein, D.; Krensky, C.; Doshi, S.; Perelman, V.S. In situ simulation and its effects on patient outcomes: A systematic review. BMJ Simul. Technol. Enhanc. Learn. 2020, 6, 3. [Google Scholar] [CrossRef] [PubMed]
- Griffin, C.; Aydın, A.; Brunckhorst, O.; Raison, N.; Khan, M.S.; Dasgupta, P.; Ahmed, K. Non-technical skills: A review of training and evaluation in urology. World J. Urol. 2020, 38, 1653–1661. [Google Scholar] [CrossRef] [PubMed]
- Pena, G.; Altree, M.; Field, J.; Sainsbury, D.; Babidge, W.; Hewett, P.; Maddern, G. Nontechnical skills training for the operating room: A prospective study using simulation and didactic workshop. Surgery 2015, 158, 300–309. [Google Scholar] [CrossRef]
- Salas, E.B.C.; Bowers, C.A. Team training in the skies: Does crew resource management (CRM) training work? Hum. Factors 2001, 43, 641–674. [Google Scholar] [CrossRef]
- Dewey, J. The reflex arc concept in psychology. Psychol. Rev. 1896, 3, 357–370. [Google Scholar] [CrossRef]
- Issenberg, S.B.M.W.; Petrusa, E.R.; Lee Gordon, D.; Scalese, R.J. Features uses of high-fidelity medical simulations that lead to effective learning: A BEME systematic review. Med. Teach. 2005, 27, 10–28. [Google Scholar] [CrossRef]
- Raemer, D.; Anderson, M.; Cheng, A.; Fanning, R.; Nadkarni, V.; Savoldelli, G. Research regarding debriefing as part of the learning process. Simul. Healthc. 2011, 6, S52–S57. [Google Scholar] [CrossRef]
- May, G.L.; Kahnweiler, W.M. The effect of a mastery practice design on learning and transfer in behavior modeling training. Pers. Psychol. 2000, 53, 353–373. [Google Scholar] [CrossRef]
- Weber, K.; Schütz, A.E.; Fertig, T.; Weber, K.; Schütz, A.E.; Fertig, T. Erkenntnisse aus der Verhaltenspsychologie; Springer: Berlin/Heidelberg, Germany, 2019; pp. 15–18. [Google Scholar]
- Jerant, A.; Griffin, E.; Rainwater, J.; Henderson, M.; Sousa, F.; Bertakis, K.D.; Fenton, J.J.; Franks, P. Does applicant personality influence multiple mini-interview performance and medical school acceptance offers? Acad. Med. 2012, 87, 1250–1259. [Google Scholar] [CrossRef]
- Ekehammar, B. Interactionism in personality from a historical perspective. Psychol. Bull. 1974, 81, 1026. [Google Scholar] [CrossRef] [PubMed]
- Endler, N.S.; Parker, J.D. Interactionism revisited: Reflections on the continuing crisis in the personality area. Eur. J. Personal. 1992, 6, 177–198. [Google Scholar] [CrossRef]
- Lievens, F.; De Koster, L.; Schollaert, E. Current Theory and Practice of Assessment Centers: The Importance of Trait Activation. In The Oxford Handbook of Personnel Psychology; Oxford Academic: Oxford, UK, 2008. [Google Scholar]
- Walker, L.O.; Avant, K.C. Strategies for Theory Construction in Nursing; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2005. [Google Scholar]
- Xyrichis, A.; Ream, E. Teamwork: A concept analysis. J. Adv. Nurs. 2008, 61, 232–241. [Google Scholar] [CrossRef] [PubMed]
- DeChurch, L.A.; Mesmer-Magnus, J.R. Measuring shared team mental models: A meta-analysis. Group Dyn. Theory Res. Pract. 2010, 14, 1. [Google Scholar] [CrossRef]
- Rook, L. Mental models: A robust definition. Learn. Organ. 2013, 20, 38–47. [Google Scholar] [CrossRef]
- Sawyer, T.L.; Deering, S. Adaptation of the US Army’s after-action review for simulation debriefing in healthcare. Simul. Healthc. 2013, 8, 388–397. [Google Scholar] [CrossRef]
- Beck, S.; Doehn, C.; Funk, H.; Kosan, J.; Issleib, M.; Daubmann, A.; Zöllner, C.; Kubitz, J.C. Basic life support training using shared mental models improves team performance of first responders on normal wards: A randomised controlled simulation trial. Resuscitation 2019, 144, 33–39. [Google Scholar] [CrossRef]
- Cannon-Bowers, J. Fostering Mental Model Convergence through Training. In Multi-Level Issues in Organizations and Time (Research in Multi-Level Issues); Dansereau, F., Yammarino, F.J., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2007; Volume 6, pp. 149–157. [Google Scholar]
- Seel, N.M. Mental Models and Complex Problem Solving: Instructional Effects. In Handling Complexity in Learning Environments: Theory and Research; Elsevier: Amsterdam, The Netherlands, 2006; pp. 43–66. [Google Scholar]


{kind=link}
| Training Unit | Number of Complete AS-NTS Total N = 939 |
|---|---|
| BEM | 140 |
| ACLS I | 156 |
| ACLS II | 220 |
| ACLS IIIa | 222 |
| ACLS IIIb | 201 |
| Non-Technical Skills (AS-NTS Score) | BEM | ACLS I | ACLS II | ACLS IIIa | ACLS IIIb | ANOVA | ||
|---|---|---|---|---|---|---|---|---|
| Welch’s F (dfNum, dfDen) | p | η2 | ||||||
| NTS_1 | 2.42 (1.04) A,B | 2.19 (0.95) C | 2.18 (0.95) D | 2.06 (0.90) B | 1.94 (0.70) ACD | 6.75 (4, 434.5) | <0.001 * | 0.047 |
| NTS_2 | 2.19 (0.85) E | 2.15 (0.89) | 2.07 (0.91) | 2.09 (0.88) | 1.90 (0.78) E | 3.56 (4, 442.9) | 0.010 * | 0.026 |
| NTS_3 | 2.18 (0.83) F | 2.12 (0.93) | 1.99 (0.90) | 2.00 (0.84) | 1.84 (0.74) F | 4.50 (4, 441.0) | 0.001 * | 0.033 |
| Sum_Score | 6.79 (2.33) G | 6.45 (2.49) H | 6.23 (2.51) | 6.15 (2.32) | 5.66 (1.90) GH | 6.72 (4, 439.6) | <0.001 * | 0.042 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moll-Khosrawi, P.; Küllmei, J.; Zöllner, C.; Schulte-Uentrop, L. Efficacy of an Integrated Simulation-Based Education Approach to Train Non-Technical Skills in Medical Undergraduate Students. Educ. Sci. 2023, 13, 853. https://0-doi-org.brum.beds.ac.uk/10.3390/educsci13090853
Moll-Khosrawi P, Küllmei J, Zöllner C, Schulte-Uentrop L. Efficacy of an Integrated Simulation-Based Education Approach to Train Non-Technical Skills in Medical Undergraduate Students. Education Sciences. 2023; 13(9):853. https://0-doi-org.brum.beds.ac.uk/10.3390/educsci13090853
Chicago/Turabian StyleMoll-Khosrawi, Parisa, Josephine Küllmei, Christian Zöllner, and Leonie Schulte-Uentrop. 2023. "Efficacy of an Integrated Simulation-Based Education Approach to Train Non-Technical Skills in Medical Undergraduate Students" Education Sciences 13, no. 9: 853. https://0-doi-org.brum.beds.ac.uk/10.3390/educsci13090853