
A Proposal of Quantum-Inspired Machine Learning for Medical Purposes: An Application Case

 , ,
, ,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Classification Systems: The CancerMath Example
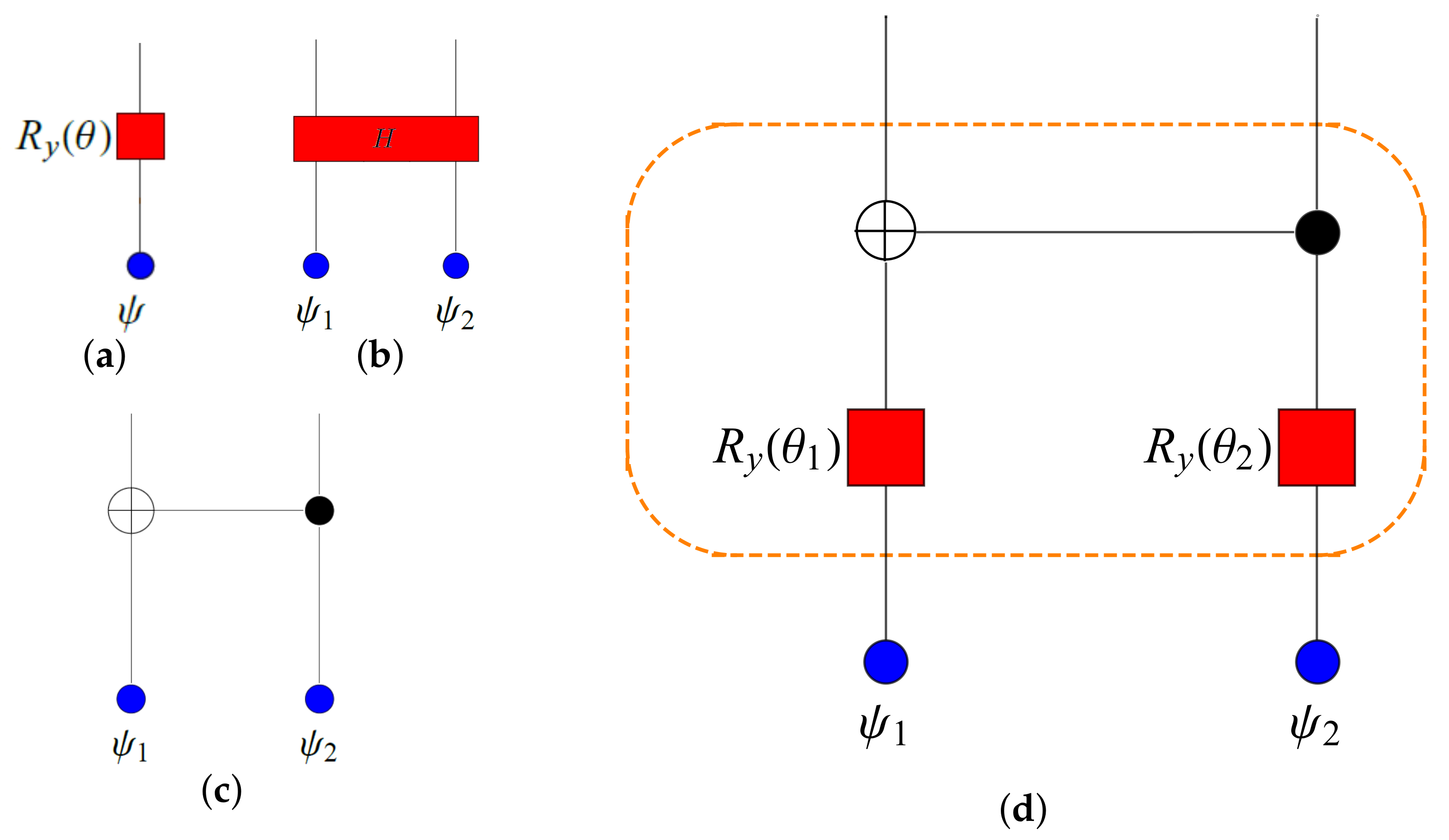
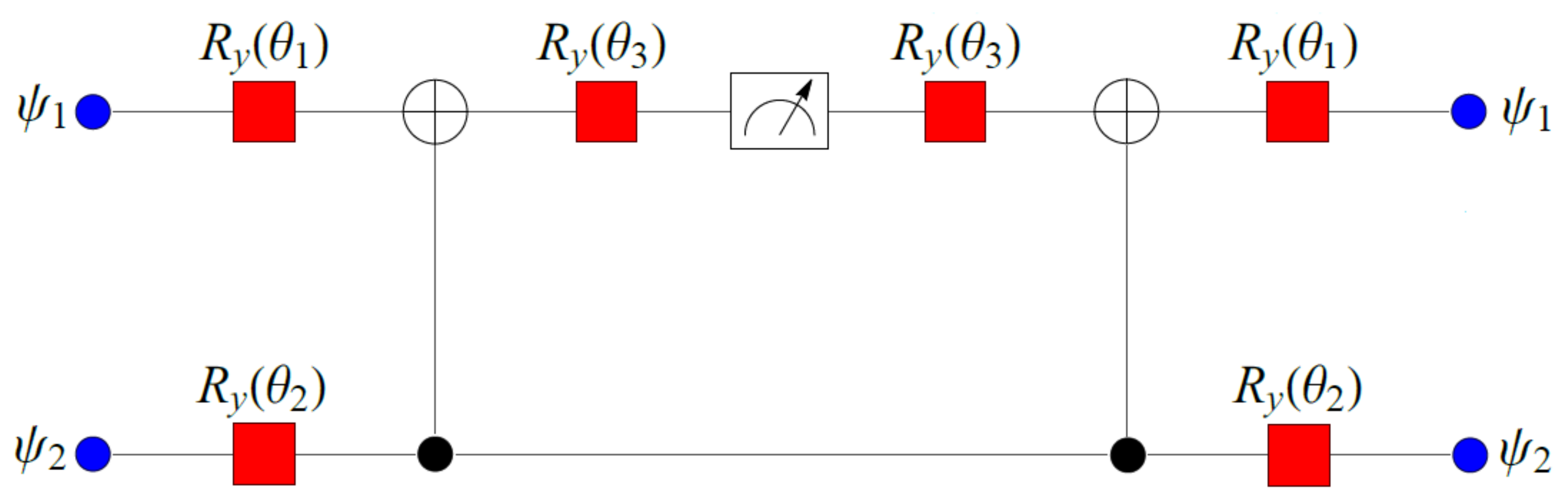
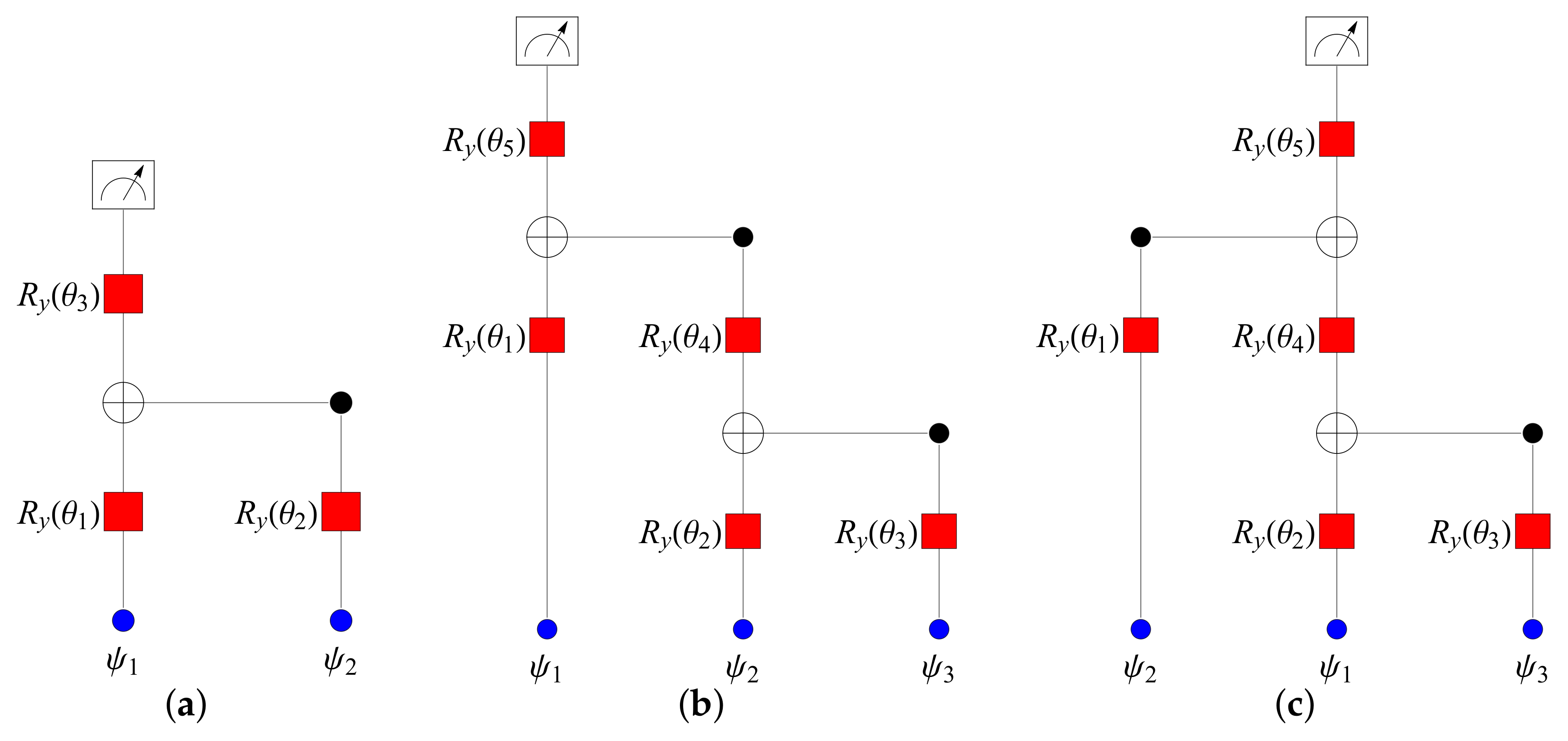
2.2. Least-Squares Problem via Quantum Measurements
2.3. Performance Evaluation
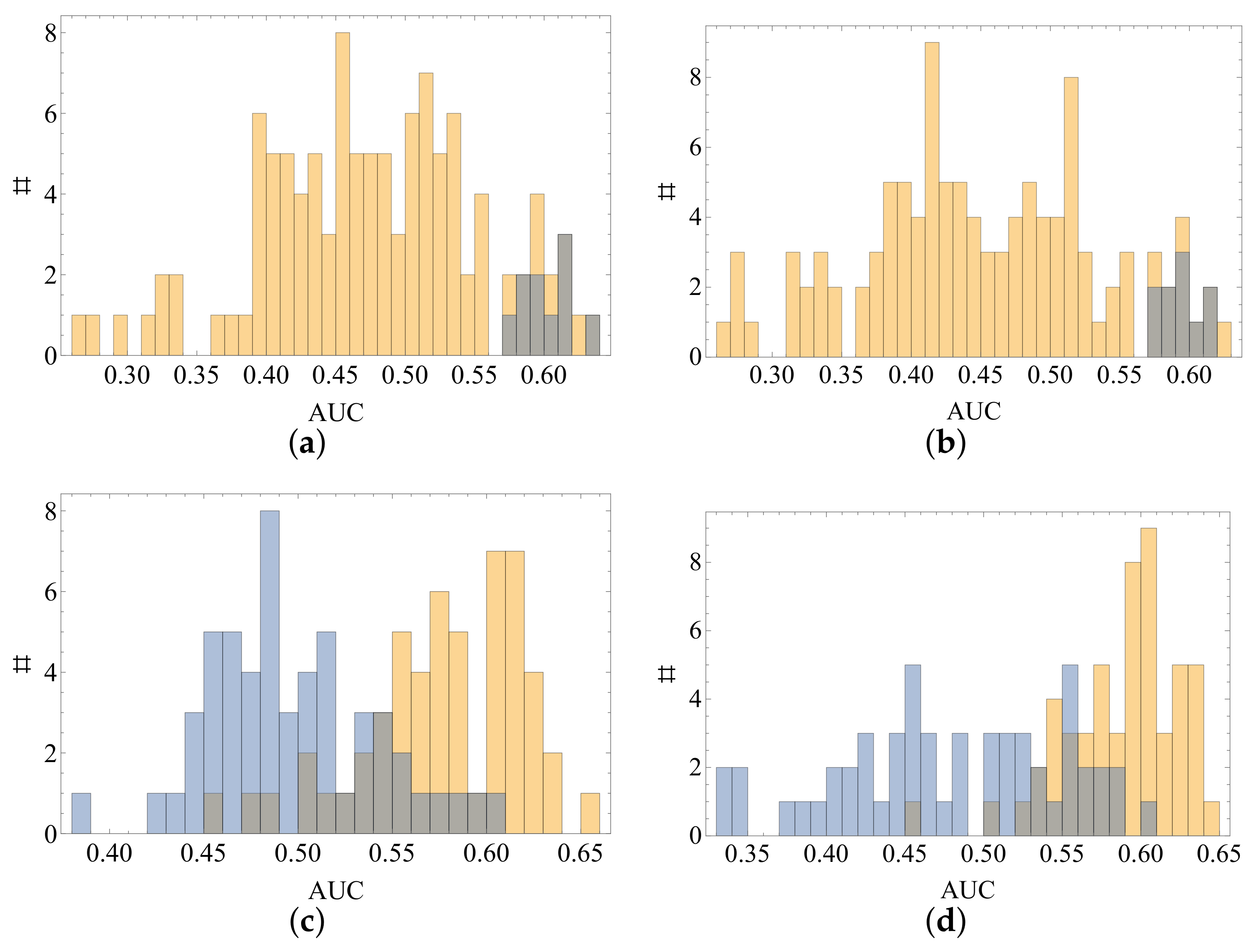
3. Results
4. Discussion
5. Conclusions and Future Developments
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schubert, C.M.; Thorsen, S.N.; Oxley, M.E. The ROC manifold for classification systems. Pattern Recognit. 2011, 44, 350–362. [Google Scholar] [CrossRef]
- Freund, Y. Boosting a Weak Learning Algorithm by Majority. Inf. Comput. 1995, 121, 256–285. [Google Scholar] [CrossRef]
- Cole, J.H.; Poudel, R.P.K.; Tsagkrasoulis, D.; Caan, M.W.A.; Steves, C.; Spector, T.D.; Montana, G. Predicting brain age with deep learning from raw imaging data results in a reliable and heritable biomarker. NeuroImage 2017, 163, 115–124. [Google Scholar] [CrossRef] [Green Version]
- Amoroso, N.; La Rocca, M.; Bellantuono, L.; Diacono, D.; Fanizzi, A.; Lella, E.; Lombardi, A.; Maggipinto, T.; Monaco, A.; Tangaro, S.; et al. Deep learning and multiplex networks for accurate modeling of brain age. Front. Aging Neurosci. 2019, 11, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellantuono, L.; Marzano, L.; La Rocca, M.; Duncan, D.; Lombardi, A.; Maggipinto, T.; Monaco, A.; Tangaro, S.; Amoroso, N.; Bellotti, R. Predicting brain age with complex networks: From adolescence to adulthood. NeuroImage 2020, 225, 117458. [Google Scholar] [CrossRef]
- Moradi, E.; Pepe, A.; Gaser, C.; Huttunen, H.; Tohka, J.; for the Alzheimer’s Disease Neuroimaging Initiative. Machine learning framework for early MRI-based Alzheimer’s conversion prediction in MCI subjects. Neuroimage 2015, 104, 398–412. [Google Scholar] [CrossRef] [Green Version]
- Tangaro, S.; Fanizzi, A.; Amoroso, N.; Bellotti, R.; for the Alzheimer’s Disease Neuroimaging Initiative. A fuzzy-based system reveals Alzheimer’s Disease onset in subjects with Mild Cognitive Impairment. Phys. Medica 2017, 38, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Mehmood, A.; Maqsood, M.; Bashir, M.; Shuyuan, Y. A Deep Siamese Convolution Neural Network for Multi-Class Classification of Alzheimer Disease. Brain Sci. 2020, 10, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, A.; Mohan, S.; Tarolli, C.; Schneider, R.B.; Adams, J.L.; Sharma, S.; Elson, M.J.; Spear, K.L.; Glidden, A.M.; Little, M.A.; et al. Using smartphones and machine learning to quantify Parkinson disease severity: The mobile Parkinson disease score. JAMA Neurol. 2018, 75, 876–880. [Google Scholar] [CrossRef]
- Yang, H.; Liu, J.; Sui, J.; Pearlson, G.; Calhoun, V.D. A hybrid machine learning method for fusing fMRI and genetic data: Combining both improves classification of schizophrenia. Front. Hum. Neurosci. 2010, 4, 192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, L.G.; Eshlaghy, A.T.; Poorebrahimi, A.; Ebrahimi, M.; Razavi, A.R. Using three machine learning techniques for predicting breast cancer recurrence. J. Health Med. Inform. 2013, 4, 3. [Google Scholar]
- Libbrecht, M.W.; Noble, W.S. Machine learning applications in genetics and genomics. Nat. Rev. Genet. 2015, 16, 321–332. [Google Scholar] [CrossRef] [Green Version]
- Monaco, A.; Monda, A.; Amoroso, N.; Bertolino, A.; Blasi, G.; Di Carlo, P.; Papalino, M.; Pergola, G.; Tangaro, S.; Bellotti, R. A complex network approach reveals a pivotal substructure of genes linked to schizophrenia. PLoS ONE 2018, 13, e0190110. [Google Scholar] [CrossRef] [Green Version]
- Caravagna, G.; Heide, T.; Williams, M.J.; Zapata, L.; Nichol, D.; Chkhaidze, K.; Cross, W.; Cresswell, G.D.; Werner, B.; Acar, A.; et al. Subclonal reconstruction of tumors by using machine learning and population genetics. Nat. Genet. 2020, 52, 898–907. [Google Scholar] [CrossRef]
- Kopczyk, D. Quantum machine learning for data scientists. arXiv 2018, arXiv:1804.10068. [Google Scholar]
- Aïmeur, E.; Brassard, G.; Gambs, S. Quantum clustering algorithms. In Proceedings of the 24th International Conference on Machine Learning, Corvallis, OR, USA, 20–24 June 2007; pp. 1–8. [Google Scholar]
- Rebentrost, P.; Mohseni, M.; Lloyd, S. Quantum Support Vector Machine for Big Data Classification. Phys. Rev. Lett. 2014, 113, 130503. [Google Scholar] [CrossRef]
- Lloyd, S.; Mohseni, M.; Rebentrost, P. Quantum principal component analysis. Nat. Phys. 2014, 10, 631–633. [Google Scholar] [CrossRef] [Green Version]
- Schuld, M.; Killoran, N. Quantum Machine Learning in Feature Hilbert Spaces. Phys. Rev. Lett. 2019, 122, 040504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tacchino, F.; Barkoutsos, P.; Macchiavello, C.; Tavernelli, I.; Gerace, D.; Bajoni, D. Quantum implementation of an artificial feed-forward neural network. Quantum Sci. Technol. 2020, 5, 044010. [Google Scholar] [CrossRef]
- Grant, E.; Benedetti, M.; Cao, S.; Hallam, A.; Lockhart, J.; Stojevic, V.; Green, A.G.; Severini, S. Hierarchical quantum classifiers. npj Quantum Inf. 2018, 65. [Google Scholar] [CrossRef] [Green Version]
- Stoudenmire, E.M. Learning relevant features of data with multi-scale tensor networks. Quantum Sci. Technol. 2018, 3, 034003. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Ran, S.-J.; Wittek, P.; Peng, C.; Blázquez García, R.; Su, G.; Lewenstein, M. Machine learning by unitary tensor network of hierarchical tree structure. New J. Phys. 2019, 21, 073059. [Google Scholar] [CrossRef]
- Borujeni, S.E.; Nguyen, N.H.; Nannapaneni, S.; Behrman, E.C.; Steck, J.E. Experimental evaluation of quantum Bayesian networks on IBM QX hardware. In Proceedings of the IEEE International Conference on Quantum Computing and Engineering, Los Alamitos, CA, USA, 12–16 October 2020. [Google Scholar]
- Glasser, I.; Pancotti, N.; Cirac, J.I. From Probabilistic Graphical Models to Generalized Tensor Networks for Supervised Learning. IEEE Access 2020, 8, 68169–68182. [Google Scholar] [CrossRef]
- Facchi, P.; Ligabò, M. Classical and quantum aspects of tomography. AIP Conf. Proc. 2010, 3, 1260. [Google Scholar]
- Kiani, B.T.; Villanyi, A.; Lloyd, S. Quantum Medical Imaging Algorithms. arXiv 2020, arXiv:2004.02036. [Google Scholar]
- Outeiral, C.; Strahm, M.; Shi, J.; Morris, G.M.; Benjamin, S.C.; Deane, C.M. The prospects of quantum computing in computational molecular biology. WIREs Comput. Mol. Sci. 2020, 11. [Google Scholar] [CrossRef]
- Farnsworth, R.H.; Achen, M.G.; Stacker, S.A. The evolving role of lymphatics in cancer metastasis. Curr. Opin. Immunol. 2018, 53, 64–73. [Google Scholar] [CrossRef]
- Land, S.R.; Kopec, J.A.; Julian, T.B.; Brown, A.M.; Anderson, S.J.; Krag, D.N.; Christian, N.J.; Costantino, J.P.; Wolmark, N.; Ganz, P.A. Patient-reported outcomes in sentinel node-negative adjuvant breast cancer patients receiving sentinel-node biopsy or axillary dissection: National Surgical Adjuvant Breast and Bowel Project phase III protocol B-32. J. Clin. Oncol. 2010, 28, 3929–3936. [Google Scholar] [CrossRef] [PubMed]
- DiSipio, T.; Rye, S.; Newman, B.; Hayes, S. Incidence of unilateral lymphedema after breast cancer: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 500–515. [Google Scholar] [CrossRef]
- Giuliano, A.E.; Hunt, K.K.; Ballman, K.V.; Beitsch, P.D.; Whitworth, P.W.; Blumencranz, P.W.; Leitch, A.M.; Saha, S.; McCall, L.M.; Morrow, M. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: A randomized clinical trial. JAMA 2011, 305, 569–575. [Google Scholar] [CrossRef] [Green Version]
- Mazo, C.; Kearns, C.; Mooney, C.; Gallagher, W.M. Clinical Decision Support Systems in Breast Cancer: A Systematic Review. Cancers 2020, 12, 369. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.L.; Nolan, M.E.; Silverstein, M.J.; Mihm, M.C.; Sober, A.J.; Tanabe, K.K.; Smith, B.L.; Younger, J.; Michaelson, J.S. The impact of primary tumor size, lymph node status, and other prognostic factors on the risk of cancer death. Cancer 2009, 115, 5071–5083. [Google Scholar] [CrossRef] [PubMed]
- Michaelson, J.S.; Chen, L.L.; Silverstein, M.J.; Mihm, M.C.; Sober, A.J.; Tanabe, K.K.; Smith, B.L.; Younger, J. How cancer at the primary site and in the lymph nodes contributes to the risk of cancer death. Cancer 2009, 115, 5095–5107. [Google Scholar] [CrossRef] [PubMed]
- Cancer Web-Calculators for Medical Professionals. Available online: http://www.lifemath.net/cancer/ (accessed on 20 December 2020).
- Chatterjee, S. Multivariate stratified surveys. J. Am. Stat. Assoc. 1968, 63, 530–534. [Google Scholar]
- Dyson, F. General Theory of Spin-Wave Interactions. Phys. Rev. 1956, 102, 1217–1230. [Google Scholar] [CrossRef]
- Tüysüz, C.; Carminati, F.; Demirköz, B.; Dobos, D.; Fracas, F.; Novotny, K.; Potamianos, K.; Vallecorsa, S.; Vlimant, J.-R. A Quantum Graph Neural Network Approach to Particle Track Reconstruction. In Proceedings of the Connecting the Dots, Princeton, NJ, USA, 10–18 September 2020; Volume 34. [Google Scholar]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Flach, P.A. The Geometry of ROC Space: Understanding Machine Learning Metrics through ROC Isometrics. In Proceedings of the Twentieth International Conference on Machine Learning, Washington, DC, USA, 21–24 August 2003. [Google Scholar]
- Kim, Y.Y.; Oh, S.J.; Chun, Y.S.; Lee, W.K.; Park, H.K. Gene expression assay and Watson for Oncology for optimization of treatment in ER-positive, HER2-negative breast cancer. PLoS ONE 2018, 13, e0200100. [Google Scholar] [CrossRef]
- Park, C.; Ahn, J.; Kim, H.; Park, S. Integrative Gene Network Construction to Analyze Cancer Recurrence Using Semi-Supervised Learning. PLoS ONE 2014, 9, e86309. [Google Scholar] [CrossRef] [Green Version]
- Madekivi, V.; Boström, P.; Karlsson, A.; Aaltonen, R.; Salminen, E. Can a machine-learning model improve the prediction of nodal stage after a positive sentinel lymph node biopsy in breast cancer? Acta Oncol. 2020, 59, 689–695. [Google Scholar] [CrossRef]
- Banerjee, S.M.; Michalopoulos, N.V.; Williams, N.R.; Davidson, T.; El Sheikh, S.; McDermott, N.; Tran-Dang, M.-A.; Davison, S.; Keshtgar, M.R. Detailed evaluation of one step nucleic acid (OSNA) molecular assay for intra-operative diagnosis of sentinel lymph node metastasis and prediction of non-sentinel nodal involvement: Experience from a London Teaching Hospital. Breast 2014, 23, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Szychta, P.; Westfal, B.; Maciejczyk, R.; Smolarz, B.; Romanowicz, H.; Krawczyk, T.; Zadrozny, M. Intraoperative diagnosis of sentinel lymph node metastases in breast cancer treatment with onestep nucleic acid amplification assay (OSNA). Arch. Med. Sci. 2016, 12, 1239–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanfani, F.; Monterossi, G.; Ghizzoni, V.; Rossi, E.D.; Dinoi, G.; Inzani, F.; Fagotti, A.; Gueli Alletti, S.; Scarpellini, F.; Nero, C.; et al. One-Step Nucleic Acid Amplification (OSNA): A fast molecular test based on CK19 mRNA concentration for assessment of lymph-nodes metastases in early stage endometrial cancer. PLoS ONE 2018, 13, e0195877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanizzi, A.; Pomarico, D.; Paradiso, A.; Bove, S.; Diotaiuti, S.; Didonna, V.; Giotta, F.; La Forgia, D.; Latorre, A.; Pastena, M.I.; et al. Predicting of Sentinel Lymph Node Status in Breast Cancer Patients with Clinically Negative Nodes: A Validation Study. Cancers 2021, 13, 352. [Google Scholar] [CrossRef] [PubMed]
- Okuno, J.; Miyake, T.; Sota, Y.; Tanei, T.; Kagara, N.; Naoi, Y.; Shimoda, M.; Shimazu, K.; Kim, S.J.; Noguchi, S. Development of prediction model including microRNA expression for sentinel lymph node metastasis in ER-positive and HER2-negative breast cancer. Ann. Surg. Oncol. 2021, 28, 310–319. [Google Scholar] [CrossRef]
- Bevilacqua, J.L.B.; Kattan, M.W.; Fey, J.V.; Cody, H.S., III; Borgen, P.I.; Van Zee, K.J. Doctor, what are my chances of having a positive sentinel node? A validated nomogram for risk estimation. J. Clin. Oncol. 2007, 25, 3670–3679. [Google Scholar] [CrossRef]
- Dong, Y.; Feng, Q.; Yang, W.; Lu, Z.; Deng, C.; Zhang, L.; Lian, Z.; Liu, J.; Luo, X.; Pei, S.; et al. Preoperative prediction of sentinel lymph node metastasis in breast cancer based on radiomics of T2-weighted fat-suppression and diffusion-weighted MRI. Eur. Radiol. 2018, 28, 582–591. [Google Scholar] [CrossRef]
- Luo, J.; Ning, Z.; Zhang, S.; Feng, Q.; Zhang, Y. Bag of deep features for preoperative prediction of sentinel lymph node metastasis in breast cancer. Phys. Med. Biol. 2018, 63, 245014. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Mao, N.; Ma, H.; Dong, J.; Zhang, K.; Che, K.; Duan, S.; Zhang, X.; Shi, Y.; Xie, H. Pharmacokinetic parameters and radiomics model based on dynamic contrast enhanced MRI for the preoperative prediction of sentinel lymph node metastasis in breast cancer. Cancer Imaging 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Sun, D.; Chen, L.; Fang, Z.; Song, W.; Guo, D.; Ni, T.; Liu, C.; Feng, L.; Xia, Y.; et al. Radiomics analysis of dynamic contrast-enhanced magnetic resonance imaging for the prediction of sentinel lymph node metastasis in breast cancer. Front. Oncol. 2019, 9, 980. [Google Scholar] [CrossRef]
- Qiu, S.-Q.; Zeng, H.-C.; Zhang, F.; Chen, C.; Huang, W.-H.; Pleijhuis, R.G.; Wu, J.-D.; van Dam, G.M.; Zhang, G.-J. A nomogram to predict the probability of axillary lymph node metastasis in early breast cancer patients with positive axillary ultrasound. Sci. Rep. 2016, 6, 21196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Wang, T.; Yang, L.; Wang, Y.; Li, H.; Zhou, X.; Zhao, W.; Ren, J.; Li, X.; Tian, J.; et al. Preoperative prediction of axillary lymph node metastasis in breast cancer using mammography-based radiomics method. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanizzi, A.; Basile, T.M.A.; Losurdo, L.; Bellotti, R.; Bottigli, U.; Dentamaro, R.; Didonna, V.; Fausto, A.; Massafra, R.; Moschetta, M.; et al. A Machine Learning Approach on Multiscale Texture Analysis for Breast Microcalcification Diagnosis. BMC Bioinform. 2020, 21 Suppl. (S2), 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanizzi, A.; Basile, T.M.A.; Losurdo, L.; Bellotti, R.; Bottigli, U.; Campobasso, F.; Didonna, V.; Fausto, A.; Massafra, R.; Tagliafico, A.; et al. Ensemble Discrete Wavelet Transform and Gray-Level Co-Occurrence Matrix for Microcalcification Cluster Classification in Digital Mammography. Appl. Sci. 2019, 9, 5388. [Google Scholar] [CrossRef]
- Losurdo, L.; Fanizzi, A.; Basile, T.M.A.; Bellotti, R.; Bottigli, U.; Dentamaro, R.; Didonna, V.; Lorusso, V.; Massafra, R.; Tamborra, P.; et al. Radiomics Analysis on Contrast-Enhanced Spectral Mammography Images for Breast Cancer Diagnosis: A Pilot Study. Entropy 2019, 21, 1110. [Google Scholar] [CrossRef] [Green Version]
- Fanizzi, A.; Losurdo, L.; Basile, T.M.A.; Bellotti, R.; Bottigli, U.; Delogu, P.; Diacono, D.; Didonna, V.; Fausto, A.; Lombardi, A.; et al. Fully Automated Support System for Diagnosis of Breast Cancer in Contrast-Enhanced Spectral Mammography Images. J. Clin. Med. 2019, 8, 891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basile, T.M.A.; Fanizzi, A.; Losurdo, L.; Bellotti, R.; Bottigli, U.; Dentamaro, R.; Didonna, V.; Fausto, A.; Massafra, R.; Moschetta, M.; et al. Microcalcification Detection in Full-Field Digital Mammograms: A Fully Automated Computer-Aided System. Phys. Medica 2019, 64, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fanizzi, A.; Basile, T.M.A.; Losurdo, L.; Amoroso, N.; Bellotti, R.; Bottigli, U.; Dentamaro, R.; Didonna, V.; Fausto, A.; Massafra, R.; et al. Hough transform for microcalcification detection in digital mammograms. Appl. Digit. Image Process. XL 2017, 10396, 41. [Google Scholar]
- Losurdo, L.; Fanizzi, A.; Basile, T.M.A.; Bellotti, R.; Bottigli, U.; Dentamaro, R.; Didonna, V.; Fausto, A.; Massafra, R.; Monaco, A.; et al. A combined approach of multiscale texture analysis and interest point/corner detectors for microcalcifications diagnosis. Appl. Evol. Comput. 2018, 1, 302–313. [Google Scholar]
- La Forgia, D.; Fanizzi, A.; Campobasso, F.; Bellotti, R.; Didonna, V.; Lorusso, V.; Moschetta, M.; Massafra, R.; Tamborra, P.; Tangaro, S.; et al. Radiomic Analysis in Contrast-Enhanced Spectral Mammography for Predicting Breast Cancer Histologicalal Outcome. Diagnostics 2020, 10, 708. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. of Patients | No. of Positive | No. of Patients | No. of Positive | ||
|---|---|---|---|---|---|
| Overall | ER | ||||
| 634 | 214 | negative | 64 | 21 | |
| Age | positive | 570 | 193 | ||
| <40 | 33 | 14 | PgR | ||
| 41–50 | 128 | 46 | negative | 146 | 49 |
| 51–60 | 151 | 50 | positive | 488 | 165 |
| 61–70 | 163 | 54 | Ki67 | ||
| 71–80 | 114 | 33 | negative | 397 | 116 |
| >80 | 45 | 17 | positive | 237 | 98 |
| Diameter (mm) | Her2/neu | ||||
| T1a (>1, ≤5) | 31 | 3 | 0 | 471 | 161 |
| T1b (>5, ≤10) | 125 | 18 | 78 | 23 | |
| T1c (>10, ≤20) | 281 | 88 | 46 | 21 | |
| T2 (>20, ≤50) | 197 | 105 | 39 | 9 | |
| Histological type | Grading | ||||
| ductal | 511 | 185 | G1 | 175 | 35 |
| lobular | 67 | 20 | G2 | 286 | 111 |
| special type | 56 | 9 | G3 | 173 | 68 |
| Multiple tumors | In situ component | ||||
| negative | 492 | 153 | negative | 265 | 100 |
| positive | 142 | 61 | positive | 369 | 114 |
| Age | ER-PgR-Ki67 | Histological Subtype | |
|---|---|---|---|
| CM | 6 strata | binary | 3 strata |
| Q’ | continuous | binary | 2 binary features |
| Q | continuous | continuous | 2 binary features |
| AUC | Accuracy | Specificity | Sensitivity | |
| 63.1 (62.7–63.3) | 65.5 (65.1–65.8) | 68.7 (67.6–70.0) | 59.3 (57.0–60.3) | |
| 64.7 (64.1–65.1) | 69.5 (61.8–70.2) | 84.9 (59.3–87.9) | 39.5 (36.0–66.8) | |
| 67.4 (67.4–67.5) | 61.7 (60.6–62.8) | 55.6 (51.9–59.5) | 73.6 (69.6–77.1) | |
| 59.5 (59.1–59.8) | 65.3 (64.7–65.9) | 76.0 (75.5–78.3) | 43.2 (41.1–44.4) | |
| 65.6 (65.4–65.8) | 65.8 (65.1–65.8) | 69.1 (67.6–69.1) | 59.3 (59.3–59.8) | |
| AUC | Accuracy | Specificity | Sensitivity | |
| 62.2 (62.0–62.2) | 68.3 (65.5–69.1) | 83.2 (75.0–84.8) | 39.5 (38.8–46.7) | |
| 65.5 (65.3–65.7) | 64.3 (63.7–65.0) | 65.7 (62.9–68.6) | 61.7 (58.4–65.0) | |
| 68.1 (67.8–68.5) | 62.0 (61.8–62.5) | 54.1 (53.6–55.7) | 77.8 (76.6–78.5) | |
| 61.8 (60.3–62.8) | 69.2 (67.7–70.2) | 85.6 (84.8–86.7) | 37.6 (36.0–37.9) | |
| 66.1 (65.7–66.2) | 57.4 (57.1–58.0) | 44.3 (42.9–46.2) | 83.2 (81.8–85.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomarico, D.; Fanizzi, A.; Amoroso, N.; Bellotti, R.; Biafora, A.; Bove, S.; Didonna, V.; Forgia, D.L.; Pastena, M.I.; Tamborra, P.; et al. A Proposal of Quantum-Inspired Machine Learning for Medical Purposes: An Application Case. Mathematics 2021, 9, 410. https://0-doi-org.brum.beds.ac.uk/10.3390/math9040410
Pomarico D, Fanizzi A, Amoroso N, Bellotti R, Biafora A, Bove S, Didonna V, Forgia DL, Pastena MI, Tamborra P, et al. A Proposal of Quantum-Inspired Machine Learning for Medical Purposes: An Application Case. Mathematics. 2021; 9(4):410. https://0-doi-org.brum.beds.ac.uk/10.3390/math9040410
Chicago/Turabian StylePomarico, Domenico, Annarita Fanizzi, Nicola Amoroso, Roberto Bellotti, Albino Biafora, Samantha Bove, Vittorio Didonna, Daniele La Forgia, Maria Irene Pastena, Pasquale Tamborra, and et al. 2021. "A Proposal of Quantum-Inspired Machine Learning for Medical Purposes: An Application Case" Mathematics 9, no. 4: 410. https://0-doi-org.brum.beds.ac.uk/10.3390/math9040410