
Association between Kinesiophobia and Knee Pain Intensity, Joint Position Sense, and Functional Performance in Individuals with Bilateral Knee Osteoarthritis

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Methodology
2.1. Study Design and Participants
2.2. Outcome Measures
2.2.1. Kinesiophobia
2.2.2. Knee Pain Intensity-Visual Analogue Scale (VAS)
2.2.3. Knee Joint Position Sense
2.2.4. Functional Performance
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yoo, J.J.; Kim, D.H.; Kim, H.A. Risk factors for progression of radiographic knee osteoarthritis in elderly community residents in Korea. BMC Musculoskelet. Disord. 2018, 19, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Alahmari, K.A.; Silvian, P.S.; Reddy, R.S.; Ahmad, I.; Kakaraparthi, V.N.; Alam, M.M. Mediating role of body mass index in knee osteoarthritis. J. Taibah Univ. Med. Sci. 2017, 12, 150. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Schmid, C.H.; Kent, D.M.; Vaysbrot, E.E.; Wong, J.B.; McAlindon, T.E. Comparative effectiveness of pharmacologic interventions for knee osteoarthritis: A systematic review and network meta-analysis. Ann. Intern. Med. 2015, 162, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; Schwartz, T.A.; Abbate, L.M.; Callahan, L.F. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2007, 34, 172–180. [Google Scholar] [PubMed]
- Ferreira, R.M.; Duarte, J.A.; Gonçalves, R.S. Non-pharmacological and non-surgical interventions to manage patients with knee osteoarthritis: An umbrella review. Acta Reum. Port 2018, 43, 182–200. [Google Scholar]
- O’Reilly, S.; Doherty, M. Lifestyle changes in the management of osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2001, 15, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Vincent, K.R.; Vincent, H.K. Resistance exercise for knee osteoarthritis. Pm&r 2012, 4, S45–S52. [Google Scholar]
- Cherian, J.J.; Kapadia, B.H.; Bhave, A.; McElroy, M.J.; Cherian, C.; Harwin, S.F.; Mont, M.A. Use of transcutaneous electrical nerve stimulation device in early osteoarthritis of the knee. J. Knee Surg. 2015, 28, 321–328. [Google Scholar] [CrossRef]
- Cudejko, T.; Van Der Esch, M.; Schrijvers, J.; Richards, R.; Van Den Noort, J.C.; Wrigley, T.; Van Der Leeden, M.; Roorda, L.D.; Lems, W.; Harlaar, J. The immediate effect of a soft knee brace on dynamic knee instability in persons with knee osteoarthritis. Rheumatology 2018, 57, 1735–1742. [Google Scholar] [CrossRef] [Green Version]
- Kamel, S.R.; Ibrahim, R.S.; Moens, H.M.; Mohammed, R.M. Neuropathic pain in primary knee osteoarthritis patients: Correlation with physical function, quality of life, disease severity, and serum beta nerve growth factor levels. Egypt. Rheumatol. Rehabil. 2021, 48, 1–9. [Google Scholar] [CrossRef]
- van der Straaten, R.; Wesseling, M.; Jonkers, I.; Vanwanseele, B.; Bruijnes, A.K.; Malcorps, J.; Bellemans, J.; Truijen, J.; De Baets, L.; Timmermans, A. Functional movement assessment by means of inertial sensor technology to discriminate between movement behaviour of healthy controls and persons with knee osteoarthritis. J. Neuroeng. Rehabil. 2020, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Meulders, A.; Karsdorp, P.A.; Claes, N.; Vlaeyen, J.W. Comparing counterconditioning and extinction as methods to reduce fear of movement-related pain. J. Pain 2015, 16, 1353–1365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neelapala, Y.R.; Reddy, Y.R.S.; Danait, R. Effect of mulligan’s posterolateral glide on shoulder rotator strength, scapular upward rotation in shoulder pain subjects–A randomized controlled trial. J. Musculoskelet. Res. 2016, 19, 1650014. [Google Scholar] [CrossRef]
- Fisher, N.M.; Pendergast, D.R.; Gresham, G.E.; Calkins, E. Muscle rehabilitation: Its effect on muscular and functional performance of patients with knee osteoarthritis. Arch. Phys. Med. Rehabil. 1991, 72, 367–374. [Google Scholar] [PubMed]
- Fisher, N.; Pendergast, D. Reduced muscle function in patients with osteoarthritis. Scand. J. Rehabil. Med. 1997, 29, 213–221. [Google Scholar]
- Burgess, L.C.; Taylor, P.; Wainwright, T.W.; Swain, I.D. Strength and endurance deficits in adults with moderate-to-severe hip osteoarthritis, compared to healthy, older adults. Disabil. Rehabil. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ferlinc, A.; Fabiani, E.; Velnar, T.; Gradisnik, L. The importance and role of proprioception in the elderly: A short review. Mater. Socio-Med. 2019, 31, 219. [Google Scholar] [CrossRef]
- Cuevas-Trisan, R. Balance problems and fall risks in the elderly. Clin. Geriatr. Med. 2019, 35, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Cuevas-Trisan, R. Balance problems and fall risks in the elderly. Phys. Med. Rehabil. Clin. 2017, 28, 727–737. [Google Scholar] [CrossRef]
- Asiri, F.; Reddy, R.S.; Tedla, J.S.; ALMohiza, M.A.; Alshahrani, M.S.; Govindappa, S.C.; Sangadala, D.R. Kinesiophobia and its correlations with pain, proprioception, and functional performance among individuals with chronic neck pain. PLoS ONE 2021, 16, e0254262. [Google Scholar]
- Ishak, N.A.; Zahari, Z.; Justine, M. Kinesiophobia, pain, muscle functions, and functional performances among older persons with low back pain. Pain Res. Treat. 2017, 2017, 489617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.; Nagao, M.; Arita, H.; Shiozawa, J.; Nishio, H.; Kobayashi, Y.; Kaneko, H.; Nagayama, M.; Saita, Y.; Ishijima, M. Reproducibility, responsiveness and validation of the Tampa Scale for Kinesiophobia in patients with ACL injuries. Health Qual. Life Outcomes 2019, 17, 1–8. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test–retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J. Pain Res. 2018, 11, 851. [Google Scholar] [CrossRef] [Green Version]
- Romero-Franco, N.; Montaño-Munuera, J.A.; Jiménez-Reyes, P. Validity and reliability of a digital inclinometer to assess knee joint-position sense in a closed kinetic chain. J. Sport Rehabil. 2017, 26, 26. [Google Scholar] [CrossRef] [Green Version]
- Reddy, R.S.; Alahmari, K.A.; Samuel, P.S.; Tedla, J.S.; Kakaraparthi, V.N.; Rengaramanujam, K. Intra-rater and inter-rater reliability of neutral and target lumbar positioning tests in subjects with and without non-specific lower back pain. J. Back Musculoskelet. Rehabil. 2021, 34, 289–299. [Google Scholar] [CrossRef]
- Alahmari, K.; Reddy, R.S.; Silvian, P.; Ahmad, I.; Nagaraj, V.; Mahtab, M. Intra-and inter-rater reliability of neutral head position and target head position tests in patients with and without neck pain. Braz. J. Phys. Ther. 2017, 21, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Medina-Mirapeix, F.; Vivo-Fernández, I.; López-Cañizares, J.; García-Vidal, J.A.; Benítez-Martínez, J.C.; del Baño-Aledo, M.E. Five times sit-to-stand test in subjects with total knee replacement: Reliability and relationship with functional mobility tests. Gait Posture 2018, 59, 258–260. [Google Scholar] [CrossRef]
- Goldberg, A.; Chavis, M.; Watkins, J.; Wilson, T. The five-times-sit-to-stand test: Validity, reliability and detectable change in older females. Aging Clin. Exp. Res. 2012, 24, 339–344. [Google Scholar] [CrossRef]
- Luque-Suarez, A.; Martinez-Calderon, J.; Falla, D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: A systematic review. Br. J. Sports Med. 2019, 53, 554–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domenech, J.; Sanchis-Alfonso, V.; López, L.; Espejo, B. Influence of kinesiophobia and catastrophizing on pain and disability in anterior knee pain patients. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1562–1568. [Google Scholar] [CrossRef] [PubMed]
- Gracely, R.; Geisser, M.; Giesecke, T.; Grant, M.; Petzke, F.; Williams, D.; Clauw, D. Pain catastrophizing and neural responses to pain among persons with fibromyalgia. Brain 2004, 127, 835–843. [Google Scholar] [CrossRef] [Green Version]
- Trinderup, J.S.; Fisker, A.; Juhl, C.B.; Petersen, T. Fear avoidance beliefs as a predictor for long-term sick leave, disability and pain in patients with chronic low back pain. BMC Musculoskelet. Disord. 2018, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nordstoga, A.L.; Meisingset, I.; Vasseljen, O.; Nilsen, T.I.; Unsgaard-Tøndel, M. Longitudinal associations of kinematics and fear-avoidance beliefs with disability, work ability and pain intensity in persons with low back pain. Musculoskelet. Sci. Pract. 2019, 41, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Shim, E.-J.; Hahm, B.-J.; Go, D.J.; Lee, K.-M.; Noh, H.L.; Park, S.-H.; Song, Y.W. Modeling quality of life in patients with rheumatic diseases: The role of pain catastrophizing, fear-avoidance beliefs, physical disability, and depression. Disability and rehabilitation 2018, 40, 1509–1516. [Google Scholar] [CrossRef]
- Ghordadekar, D.R.; Kapoor, A. Assessing Fear-Avoidance Belief Questionnaire and Quality of Life in Housewives with Knee Osteoarthritis: A Research Protocol. Indian J. Forensic Med. Toxicol. 2021, 15, 44–49. [Google Scholar]
- Peters, M.L.; Vlaeyen, J.W.; Weber, W.E. The joint contribution of physical pathology, pain-related fear and catastrophizing to chronic back pain disability. Pain 2005, 113, 45–50. [Google Scholar] [CrossRef]
- Baez, S.; Hoch, M.C.; Hoch, J.M. Evaluation of cognitive behavioral interventions and psychoeducation implemented by rehabilitation specialists to treat fear-avoidance beliefs in patients with low back pain: A systematic review. Arch. Phys. Med. Rehabil. 2018, 99, 2287–2298. [Google Scholar] [CrossRef] [PubMed]
- Clark, N.C. In Predictors of Knee Functional Joint Stability in Uninjured Physically Active Adults; University of Pittsburgh: Pittsburgh, PA, USA; 2014.
- Pakzad, M.; Fung, J.; Preuss, R. Pain catastrophizing and trunk muscle activation during walking in patients with chronic low back pain. Gait Posture 2016, 49, 73–77. [Google Scholar] [CrossRef]
- Aydoğdu, O.; Zübeyir, S. The association between kinesiophobia and proprioception, postural stability, activity level, knee function, and quality of life following anterior cruciate ligament reconstruction. J. Exerc. Ther. Rehabil. 2020, 7, 247–252. [Google Scholar]
- Desai, D.; SuroshreeMitra, D.R. Fear of Movement: Kinesiophobia in Knee Arthroplasty Cases-A Cross-Sectional Study. J. Orthop. Rehabil. 2016, 3, 9–11. [Google Scholar]
- Bailey, K.M.; Carleton, R.N.; Vlaeyen, J.W.; Asmundson, G.J. Treatments addressing pain-related fear and anxiety in patients with chronic musculoskeletal pain: A preliminary review. Cogn. Behav. Ther. 2010, 39, 46–63. [Google Scholar] [CrossRef] [PubMed]
- Vincent, H.K.; Omli, M.R.; Day, T.; Hodges, M.; Vincent, K.R.; George, S.Z. Fear of movement, quality of life, and self-reported disability in obese patients with chronic lumbar pain. Pain Med. 2011, 12, 154–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alahmari, K.A.; Reddy, R.S.; Silvian, P.S.; Ahmad, I.; Kakaraparthi, V.N.; Alam, M.M. Association of age on cervical joint position error. J. Adv. Res. 2017, 8, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Reddy, R.S.; Meziat-Filho, N.; Ferreira, A.S.; Tedla, J.S.; Kandakurti, P.K.; Kakaraparthi, V.N. Comparison of neck extensor muscle endurance and cervical proprioception between asymptomatic individuals and patients with chronic neck pain. J. Bodyw. Mov. Ther. 2021, 26, 180–186. [Google Scholar] [CrossRef]
- Kandakurti, P.K.; Reddy, R.S.; Kakarparthy, V.N.; Rengaramanujam, K.; Tedla, J.S.; Dixit, S.; Gautam, A.P.; Silvian, P.; Gular, K.; Eapen, C. Comparison and Association of Neck Extensor Muscles’ Endurance and Postural Function in Subjects with and without Chronic Neck Pain—A Cross-Sectional Study. Phys. Med. Rehabil. Kurortmed. 2021. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Mean ± SD |
|---|---|
| Age (years) | 67.10 ± 4.36 |
| BMI (kg/m2) | 29.59 ± 4.52 |
| VAS (cm) | 06.00 ± 1.34 |
| TSK total score | 48.68 ± 4.38 |
| Knee JPS angles | |
| 15° of knee flexion—left | 4.08 ± 1.74 |
| 15° of knee flexion—right | 5.14 ± 1.70 |
| 30° of knee flexion—left | 6.04 ± 1.73 |
| 30° of knee flexion—right | 4.22 ± 1.59 |
| 60° of knee flexion—left | 5.54 ± 1.67 |
| 60° of knee flexion—right | 6.56 ± 1.68 |
| Functional performance—five times sit-to-stand test (s) | 15.30 ± 3.76 |
| Correlation Variables | Kinesiophobia–TSK Score | |
|---|---|---|
| r | p Value | |
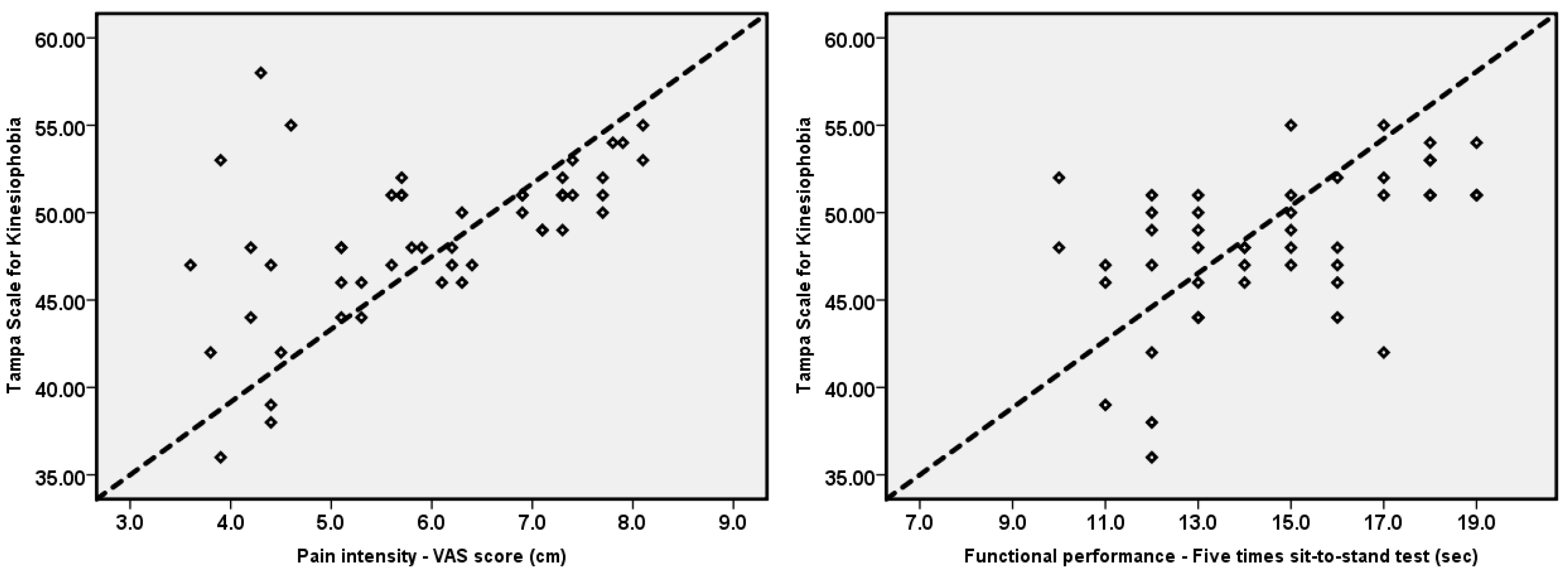
| Knee pain intensity-VAS (mm) | 0.55 | <0.001 |
| Knee JPS angles | ||
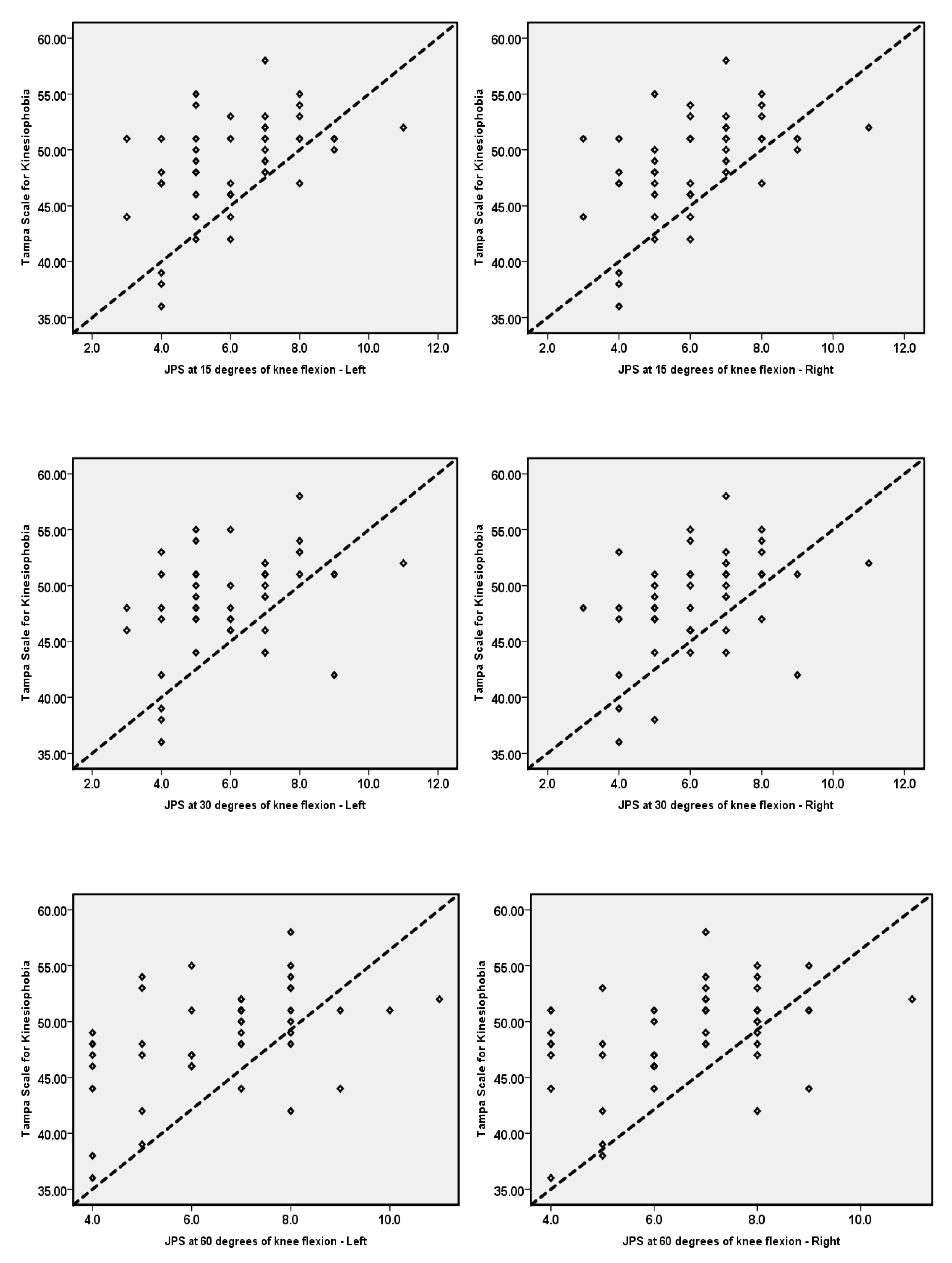
| 15° of knee flexion—left | 0.48 | <0.001 |
| 15° of knee flexion—right | 0.50 | <0.001 |
| 30 ° of knee flexion—left | 0.38 | <0.001 |
| 30 ° of knee flexion—right | 0.42 | 0.003 |
| 60 ° of knee flexion—left | 0.46 | 0.001 |
| 60 ° of knee flexion—right | 0.42 | 0.002 |
| Functional performance—five times sit-to-stand test (s) | 0.49 | <0.001 |
| Variable | B | SE | t-Value | p Value |
|---|---|---|---|---|
| Knee pain intensity-VAS (mm) | 1.80 | 0.39 | 4.58 | <0.001 |
| Knee JPS angles | ||||
| 15° of knee flexion—left | 1.21 | 0.32 | 3.77 | <0.001 |
| 15° of knee flexion—right | 1.30 | 0.32 | 4.04 | <0.001 |
| 30° of knee flexion—left | 0.96 | 0.34 | 2.84 | 0.007 |
| 30° of knee flexion—right | 1.14 | 0.36 | 3.17 | 0.003 |
| 60° of knee flexion—left | 1.20 | 0.34 | 3.58 | 0.001 |
| 60° of knee flexion—right | 1.10 | 0.34 | 3.22 | 0.002 |
| Functional performance—five times sit-to-stand test (s) | 0.57 | 0.15 | 3.87 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshahrani, M.S.; Reddy, R.S.; Tedla, J.S.; Asiri, F.; Alshahrani, A. Association between Kinesiophobia and Knee Pain Intensity, Joint Position Sense, and Functional Performance in Individuals with Bilateral Knee Osteoarthritis. Healthcare 2022, 10, 120. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010120
Alshahrani MS, Reddy RS, Tedla JS, Asiri F, Alshahrani A. Association between Kinesiophobia and Knee Pain Intensity, Joint Position Sense, and Functional Performance in Individuals with Bilateral Knee Osteoarthritis. Healthcare. 2022; 10(1):120. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010120
Chicago/Turabian StyleAlshahrani, Mastour Saeed, Ravi Shankar Reddy, Jaya Shanker Tedla, Faisal Asiri, and Adel Alshahrani. 2022. "Association between Kinesiophobia and Knee Pain Intensity, Joint Position Sense, and Functional Performance in Individuals with Bilateral Knee Osteoarthritis" Healthcare 10, no. 1: 120. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010120