
Ductal Carcinoma In Situ (DCIS) and Microinvasive DCIS: Role of Surgery in Early Diagnosis of Breast Cancer

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Method
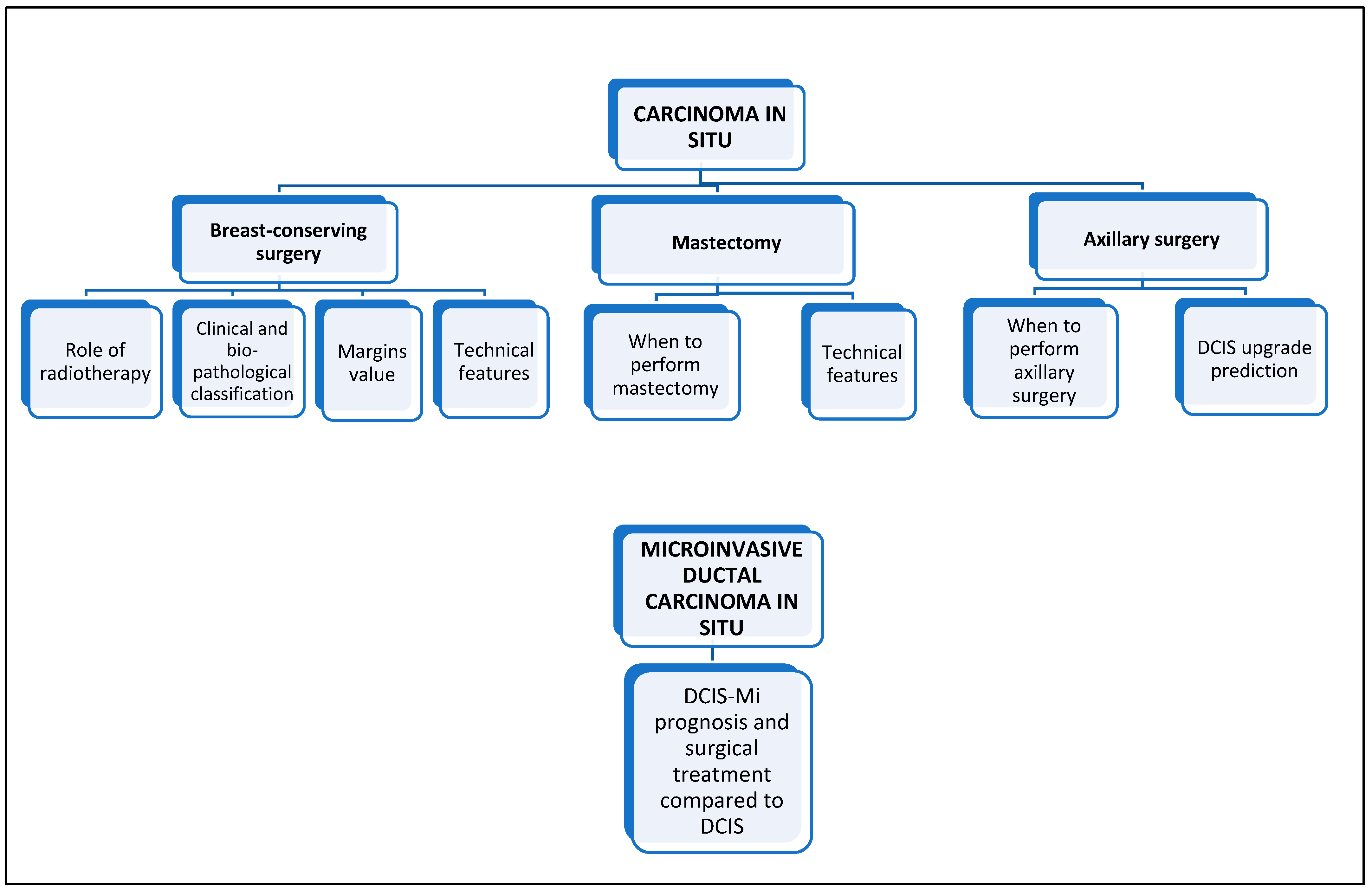
3. Ductal Carcinoma In Situ
3.1. Breast-Conserving Surgery
3.1.1. Role of Radiotherapy
3.1.2. Clinical and Bio-Pathological Classification
3.1.3. Margins Value
3.1.4. Technical Features
3.2. Mastectomy
3.2.1. When to Perform Mastectomy in Ductal Carcinoma In Situ
3.2.2. Technical Features
3.3. Axillary Surgery
3.3.1. When to Perform Axillary Surgery in Ductal Carcinoma In Situ
3.3.2. Ductal Carcinoma In Situ Upgrade Prediction
4. Microinvasive Ductal Carcinoma In Situ
DCIS-Mi Prognosis and Surgical Treatment Compared with Ductal Carcinoma In Situ
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). WHO Guide to Cancer Early Diagnosis. WHO. 2017. Available online: http://www.who.int/iris/handle/10665/254500 (accessed on 10 December 2022).
- Ginsburg, O.; Yip, C.H.; Brooks, A.; Cabanes, A.; Caleffi, M.; Dunstan Yataco, J.A.; Gyawali, B.; McCormack, V.; McLaughlin de Anderson, M.; Mehrotra, R.; et al. Breast cancer early detection: A phased approach to implementation. Cancer 2020, 126, 2379–2393. [Google Scholar] [CrossRef] [PubMed]
- Pashayan, N.; Antoniou, A.C.; Ivanus, U.; Esserman, L.J.; Easton, D.F.; French, D.; Sroczynski, G.; Hall, P.; Cuzick, J.; Evans, D.G.; et al. Publisher Correction: Personalized early detection and prevention of breast cancer: ENVISION consensus statement. Nat. Rev. Clin. Oncol. 2020, 17, 716. [Google Scholar] [CrossRef] [PubMed]
- La Vecchia, C.; Negri, E.; Carioli, G. Progress in cancer epidemiology: Avoided deaths in Europe over the last three decades. Eur. J. Cancer Prev. 2022, 31, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Ouédraogo, S.; Dabakuyo, T.S.; Gentil, J.; Poillot, M.L.; Dancourt, V.; Arveux, P. Attending breast cancer screening alone does not explain the detection of tumours at an early stage. Eur. J. Cancer Prev. 2013, 22, 103–111. [Google Scholar] [CrossRef]
- Trimboli, R.M.; Giorgi Rossi, P.; Battisti, N.M.L.; Cozzi, A.; Magni, V.; Zanardo, M.; Sardanelli, F. Do we still need breast cancer screening in the era of targeted therapies and precision medicine? Insights Imaging 2020, 11, 105. [Google Scholar] [CrossRef]
- Park, T.S.; Hwang, E.S. Current trends in management of Ductal Carcinoma In Situ. Oncology 2016, 30, 823–831. [Google Scholar]
- Neal, C.H.; Joe, A.I.; Patterson, S.K.; Pujara, A.C.; Helvie, M.A. Digital mammography has persistently increased high-grade and overall DCIS detection without altering upgrade rate. AJR Am. J. Roentgenol. 2021, 216, 912–918. [Google Scholar] [CrossRef]
- Van Bockstal, M.R.; Agahozo, M.C.; Koppert, L.B.; Deurzen, C.H. A retrospective alternative for active surveillance trials for ductal carcinoma in situ of the breast. Int. J. Cancer 2020, 146, 1189–1197. [Google Scholar] [CrossRef]
- Poiseuil, M.; Moutel, G.; Cosson, M.; Quertier, M.C.; Duchange, N.; Darquy, S. Participation in breast cancer screening and its influence on other cancer screening invitations: Study in women aged 56 years old in four French departments. Eur. J. Cancer Prev. 2023. ahead of print. [Google Scholar] [CrossRef]
- Bluekens, A.M.J.; Holland, R.; Karssemeijer, N.; Broeders, M.J.M.; den Heeten, G.J. Comparison of digital screening mammography and screen-film mammography in the early detection of clinically relevant cancers: A multicenter study. Radiology 2012, 265, 707–714. [Google Scholar] [CrossRef]
- Breast Cancer, Version 2.2023 © 2023 National Comprehensive Cancer Network© (NCCN©). Available online: https://www.nccn.org/ (accessed on 2 February 2023).
- van Seijen, M.; Lips, E.H.; Thompson, A.M.; Nik-Zainal, S.; Futreal, A.; Hwang, E.S.; Verschuur, E.; Lane, J.; Jonkers, J.; Rea, D.W.; et al. Ductal carcinoma in situ: To treat or not to treat, that is the question. Br. J. Cancer 2019, 121, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Fan, B.; Pardo, J.A.; Alapati, A.; Hopewood, P.; Mohammad Virk, Z.; James, T.A. Analysis of active surveillance as a treatment modality in ductal carcinoma in situ. Breast J. 2020, 26, 1221–1226. [Google Scholar] [CrossRef] [PubMed]
- Lynch, T.; Frank, E.S.; Collyar, D.E.; Pinto, D.; Basila, D.; Partridge, A.H.; Thompson, A.M.; Hwang, E.S.; Li, F.; Ren, Y.; et al. Comparing an operation to monitoring, with or without endocrine therapy (COMET), for low-risk ductal carcinoma in situ (DCIS). J. Clin. Oncol. 2022, 40, TPS616. [Google Scholar] [CrossRef]
- Hwang, E.S.; Hyslop, T.; Lynch, T.; Frank, E.; Pinto, D.; Basila, D.; Collyar, D.; Bennett, A.; Kaplan, C.; Rosenberg, S.; et al. The COMET (Comparison of Operative versus Monitoring and Endocrine Therapy) trial: A phase III randomised controlled clinical trial for low-risk ductal carcinoma in situ (DCIS). BMJ Open 2019, 9, e026797. [Google Scholar] [CrossRef]
- Francis, A.; Thomas, J.; Fallowfield, L.; Wallis, M.; Bartlett, J.M.; Brookes, C.; Roberts, T.; Pirrie, S.; Gaunt, C.; Young, J.; et al. Addressing overtreatment of screen detected DCIS; the LORIS trial. Eur. J. Cancer 2015, 51, 2296–2303. [Google Scholar] [CrossRef]
- Elshof, L.E.; Tryfonidis, K.; Slaets, L.; van Leeuwen-Stok, A.E.; Skinner, V.P.; Dif, N.; Pijnappel, R.M.; Bijker, N.; Rutgers, E.J.; Wesseling, J. Feasibility of a prospective, randomised, open-label, international multicentre, phase III, non-inferiority trial to assess the safety of active surveillance for low risk ductal carcinoma in situ—The LORD study. Eur. J. Cancer 2015, 51, 1497–1510. [Google Scholar] [CrossRef]
- Kanbayashi, C.; Thompson, A.M.; Hwang, E.-S.S.; Partridge, A.H.; Rea, D.W.; Wesseling, J.; Shien, T.; Mizutani, T.; Shibata, T.; Iwata, H. The international collaboration of active surveillance trials for low-risk DCIS (LORIS, LORD, COMET, LORETTA). J. Clin. Oncol. 2019, 37, TPS603. [Google Scholar] [CrossRef]
- Chavez de Paz Villanueva, C.; Bonev, V.; Senthil, M.; Solomon, N.; Reeves, M.E.; Garberoglio, C.A.; Namm, J.P.; Lum, S.S. Factors Associated With Underestimation of Invasive Cancer in Patients With Ductal Carcinoma In Situ: Precautions for Active Surveillance. JAMA Surg. 2017, 152, 1007–1014. [Google Scholar] [CrossRef]
- Doke, K.; Butler, S.; Mitchell, M.P. Current Therapeutic Approaches to DCIS. J. Mammary Gland. Biol. Neoplasia 2018, 23, 279–291. [Google Scholar] [CrossRef]
- Bijker, N.; Donker, M.; Wesseling, J.; den Heeten, G.J.; Rutgers, E.J. Is DCIS breast cancer, and how do I treat it? Curr. Treat. Opt. Oncol. 2013, 14, 75–87. [Google Scholar] [CrossRef]
- McCormick, B.; Winter, K.; Hudis, C.; Kuerer, H.M.; Rakovitch, E.; Smith, B.L.; Sneige, N.; Moughan, J.; Shah, A.; Germain, I.; et al. RTOG 9804: A prospective randomized trial for good-risk ductal carcinoma in situ comparing radiotherapy with observation. J. Clin. Oncol. 2015, 33, 709–715. [Google Scholar] [CrossRef]
- Burstein, H.J.; Curigliano, G.; Loibl, S.; Dubsky, P.; Gnant, M.; Poortmans, P.; Colleoni, M.; Denkert, C.; Piccart-Gebhart, M.; Regan, M.; et al. Estimating the benefits of therapy for early-stage breast cancer: The St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer. Ann. Oncol. 2019, 30, 1541–1557. [Google Scholar] [CrossRef] [PubMed]
- Bartram, A.; Gilbert, F.; Thompson, A.; Mann, G.B.; Agrawal, A. Breast MRI in DCIS size estimation, breast-conserving surgery and oncoplastic breast surgery. Cancer Treat. Rev. 2021, 94, 102158. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, C.K.; Schrading, S.; Bieling, H.B.; Wardelmann, E.; Leutner, C.C.; Koenig, R.; Kuhn, W.; Schild, H.H. MRI for diagnosis of pure ductal carcinoma in situ: A prospective observational study. Lancet 2007, 370, 485–492. [Google Scholar] [CrossRef]
- Allen, L.R.; Lago-Toro, C.E.; Hughes, J.H.; Careaga, E.; Brown, A.T.; Chernick, M.; Barrio, A.V.; Frazier, T.G. Is there a role for MRI in the preoperative assessment of patients with DCIS? Ann. Surg. Oncol. 2010, 17, 2395–2400. [Google Scholar] [CrossRef]
- Barrio, A.V.; Van Zee, K.J. Controversies in the Treatment of Ductal Carcinoma in Situ. Annu. Rev. Med. 2017, 68, 197–211. [Google Scholar] [CrossRef]
- Boyages, J.; Delaney, G.; Taylor, R. Predictors of local recurrence after treatment of ductal carcinoma in situ: A meta-analysis. Cancer 1999, 85, 616–628. [Google Scholar] [CrossRef]
- Toesca, A.; Botteri, E.; Lazzeroni, M.; Vila, J.; Manika, A.; Ballardini, B.; Bettarini, F.; Guerrieri-Gonzaga, A.; Bonanni, B.; Rotmensz, N.; et al. Breast conservative surgery for well-differentiated ductal intraepithelial neoplasia: Risk factors for ipsilateral breast tumor recurrence. Breast 2014, 23, 829–835. [Google Scholar] [CrossRef]
- Morrow, M.; Winograd, J.M.; Freer, P.E.; Eichhorn, J.H. Case 8-2013: A 48-year-old woman with carcinoma in situ of the breast. N. Engl. J. Med. 2013, 368, 1046–1053. [Google Scholar] [CrossRef]
- Magnoni, F.; Corso, G.; Maisonneuve, P.; Massari, G.; Alberti, L.; Castelnovo, G.; Leonardi, M.C.; Sacchini, V.; Galimberti, V.; Veronesi, P. A propensity score-matched analysis of breast-conserving surgery plus whole-breast irradiation versus mastectomy in breast cancer. J. Cancer Res. Clin. Oncol. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Magnoni, F.; Alessandrini, S.; Alberti, L.; Polizzi, A.; Rotili, A.; Veronesi, P.; Corso, G. Breast Cancer Surgery: New Issues. Curr. Oncol. 2021, 28, 4053–4066. [Google Scholar] [CrossRef]
- Goodwin, A.; Parker, S.; Ghersi, D.; Wilcken, N. Post-operative radiotherapy for ductal carcinoma in situ of the breast--a systematic review of the randomised trials. Breast 2009, 18, 143–149. [Google Scholar] [CrossRef]
- Wapnir, I.L.; Dignam, J.; Fisher, B.; Mamounas, E.P.; Anderson, S.J.; Julian, T.B.; Land, S.R.; Margolese, R.G.; Swain, S.M.; Costantino, J.P.; et al. Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCIS. J. Natl. Cancer Inst. 2011, 103, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Donker, M.; Litiere, S.; Werutsky, G.; Julien, J.P.; Fentiman, I.S.; Agresti, R.; Rouanet, P.; de Lara, C.T.; Bartelink, H.; Duez, N.; et al. Breast-conserving treatment with or without radiotherapy in ductal carcinoma In Situ: 15-year recurrence rates and outcome after a recurrence, from the EORTC 10853 randomized phase III trial. J. Clin. Oncol. 2013, 31, 4054–4059. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG); Darby, S.; McGale, P.; Correa, C.; Taylor, C.; Arriagada, R.; Clarke, M.; Cutter, D.; Davies, C.; Ewertz, M.; et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10, 801 women in 17 randomised trials. Lancet 2011, 378, 1707–1716. [Google Scholar] [CrossRef]
- Hickey, B.E.; Francis, D.P.; Lehman, M. Sequencing of chemotherapy and radiotherapy for early breast cancer. Cochrane Database Syst. Rev. 2013, 4, CD005212. [Google Scholar] [CrossRef]
- Correa, C.; Harris, E.E.; Leonardi, M.C.; Smith, B.D.; Taghian, A.G.; Thompson, A.M.; White, J.; Harris, J.R. Accelerated Partial Breast Irradiation: Executive summary for the update of an ASTRO Evidence-Based Consensus Statement. Pract. Radiat. Oncol. 2017, 7, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Burstein, H.J.; Curigliano, G.; Thürlimann, B.; Weber, W.P.; Poortmans, P.; Regan, M.M.; Senn, H.J.; Winer, E.P.; Gnant, M.; Panelists of the St Gallen Consensus Conference. Customizing local and systemic therapies for women with early breast cancer: The St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann. Oncol. 2021, 32, 1216–1235. [Google Scholar] [CrossRef]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Guideline Update. Arch. Pathol. Lab. Med. 2020, 144, 545–563. [Google Scholar] [CrossRef]
- Solin, L.J.; Gray, R.; Baehner, F.L.; Butler, S.M.; Hughes, L.L.; Yoshizawa, C.; Cherbavaz, D.B.; Shak, S.; Page, D.L.; Sledge, G.W., Jr.; et al. A multigene expression assay to predict local recurrence risk for ductal carcinoma in situ of the breast. J. Natl. Cancer Inst. 2013, 105, 701–710. [Google Scholar] [CrossRef]
- Nofech-Mozes, S.; Hanna, W.; Rakovitch, E. Molecular Evaluation of Breast Ductal Carcinoma in Situ with Oncotype DX DCIS. Am. J. Pathol. 2019, 189, 975–980. [Google Scholar] [CrossRef]
- Vicini, F.A.; Mann, G.B.; Shah, C.; Weinmann, S.; Leo, M.C.; Whitworth, P.; Rabinovitch, R.; Torres, M.A.; Margenthaler, J.A.; Dabbs, D.; et al. A Novel Biosignature Identifies Patients With DCIS With High Risk of Local Recurrence After Breast Conserving Surgery and Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2023, 115, 93–102. [Google Scholar] [CrossRef]
- Morrow, M.; Van Zee, K.J.; Solin, L.J.; Houssami, N.; Chavez-MacGregor, M.; Harris, J.R.; Horton, J.; Hwang, S.; Johnson, P.L.; Marinovich, M.L.; et al. Society of Surgical Oncology-American Society for Radiation Oncology-American Society of Clinical Oncology Consensus Guideline on Margins for Breast-Conserving Surgery with Whole-Breast Irradiation in Ductal Carcinoma In Situ. J. Clin. Oncol. 2016, 34, 4040–4046. [Google Scholar] [CrossRef]
- Kuerer, H.M.; Smith, B.D.; Chavez-MacGregor, M.; Albarracin, C.; Barcenas, C.H.; Santiago, L.; Edgerton, M.E.; Rauch, G.M.; Giordano, S.H.; Sahin, A.; et al. DCIS Margins and Breast Conservation: MD Anderson Cancer Center Multidisciplinary Practice Guidelines and Outcomes. J. Cancer 2017, 8, 2653–2662. [Google Scholar] [CrossRef] [PubMed]
- Van Zee, K.J.; Subhedar, P.; Olcese, C.; Patil, S.; Morrow, M. Relationship Between Margin Width and Recurrence of Ductal Carcinoma In situ: Analysis of 2996 Women Treated with Breast-conserving Surgery for 30 Years. Ann. Surg. 2015, 262, 623–631. [Google Scholar] [CrossRef]
- Galimberti, V.; Monti, S.; Mastropasqua, M.G. DCIS and LCIS are confusing and outdated terms. They should be abandoned in favor of ductal intraepithelial neoplasia (DIN) and lobular intraepithelial neoplasia (LIN). Breast 2013, 22, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Dai, H.; Liu, B.; Song, F.; Chen, K. Predictors for local invasive recurrence of ductal carcinoma in situ of the breast: A meta-analysis. Eur. J. Cancer Prev. 2016, 25, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Rodin, D.; Sutradhar, R.; Nofech-Mozes, S.; Gu, S.; Faught, N.; Hahn, E.; Fong, C.; Trebinjac, S.; Paszat, L.; Rakovitch, E. Long-term outcomes of women with large DCIS lesions treated with breast-conserving therapy. Breast Cancer Res. Treat. 2022, 192, 223–233. [Google Scholar] [CrossRef]
- De Lorenzi, F.; Di Bella, J.; Maisonneuve, P.; Rotmensz, N.; Corso, G.; Orecchia, R.; Colleoni, M.; Mazzarol, G.; Rietjens, M.; Loschi, P.; et al. Oncoplastic breast surgery for the management of ductal carcinoma in situ (DCIS): Is it oncologically safe? A retrospective cohort analysis. Eur. J. Surg. Oncol. 2018, 44, 957–962. [Google Scholar] [CrossRef]
- Galimberti, V.; Taffurelli, M.; Leonardi, M.C.; Aristei, C.; Trentin, C.; Cassano, E.; Pietribiasi, F.; Corso, G.; Munzone, E.; Tondini, C.; et al. Surgical resection margins after breast-conserving surgery: Senonetwork recommendations. Tumori 2016, 3, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Galimberti, V.; Vicini, E.; Corso, G.; Morigi, C.; Fontana, S.; Sacchini, V.; Veronesi, P. Nipple-sparing and skin-sparing mastectomy: Review of aims, oncological safety and contraindications. Breast 2017, 34, S82–S84. [Google Scholar] [CrossRef] [PubMed]
- Didier, F.; Radice, D.; Gandini, S.; Bedolis, R.; Rotmensz, N.; Maldifassi, A.; Santillo, B.; Luini, A.; Galimberti, V.; Scaffidi, E.; et al. Does nipple preservation in mastectomy improve satisfaction with cosmetic results, psychological adjustment, body image and sexuality? Breast Cancer Res. Treat. 2009, 118, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Timbrell, S.; Al-Himdani, S.; Shaw, O.; Tan, K.; Morris, J.; Bundred, N. Comparison of Local Recurrence After Simple and Skin-Sparing Mastectomy Performed in Patients with Ductal Carcinoma In Situ. Ann. Surg. Oncol. 2017, 24, 1071–1076. [Google Scholar] [CrossRef]
- Corso, G.; De Lorenzi, F.; Vicini, E.; Pagani, G.; Veronesi, P.; Sargenti, M.; Magnoni, F.; Naninato, P.; Maisonneuve, P.; Sangalli, C.; et al. Nipple-sparing mastectomy with different approaches: Surgical incisions, complications, and cosmetic results. Preliminary results of 100 consecutive patients at a single center. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 1751–1760. [Google Scholar] [CrossRef]
- Farante, G.; Galimberti, V.; Zurrida, S.; Veronesi, P.; Luini, A.; Veronesi, U. No more axillary dissection in patients with ductal intraepithelial neoplasia (DIN). Eur. J. Cancer 2010, 46, 476–478. [Google Scholar] [CrossRef]
- Intra, M.; Rotmensz, N.; Veronesi, P.; Colleoni, M.; Iodice, S.; Paganelli, G.; Viale, G.; Veronesi, U. Sentinel node biopsy is not a standard procedure in ductal carcinoma in situ of the breast: The experience of the European institute of oncology on 854 patients in 10 years. Ann. Surg. 2008, 247, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Magnoni, F.; Galimberti, V.; Corso, G.; Intra, M.; Sacchini, V.; Veronesi, P. Axillary surgery in breast cancer: An updated historical perspective. Semin. Oncol. 2020, 47, 341–352. [Google Scholar] [CrossRef]
- Lyman, G.H.; Somerfield, M.R.; Bosserman, L.D.; Perkins, C.L.; Weaver, D.L.; Giuliano, A.E. Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology clinical practice guideline update. J. Clin. Oncol. 2014, 32, 1365–1383. [Google Scholar] [CrossRef]
- Park, K.W.; Kim, S.W.; Han, H.; Park, M.; Han, B.-K.; Ko, E.Y.; Choi, J.S.; Cho, E.Y.; Cho, S.H.; Ko, E.S. Ductal carcinoma in situ: A risk prediction model for the underestimation of invasive breast cancer. NPJ Breast Cancer 2022, 8, 8. [Google Scholar] [CrossRef]
- Jia, H.; Zhao, P.; Chen, Z.; Wang, G.; Dong, X.; Xing, X.; Tan, X.; Wang, C. Clinicopathological characteristics and prognostic analysis of tumor-infiltrating lymphocytes (TILs) in ductal carcinoma in situ (DCIS) and DCIS with microinvasion (DCIS-Mi) of the breast. Breast Cancer Res. Treat. 2022, 193, 111–120. [Google Scholar] [CrossRef]
- Piltin, M.A.; Hoskin, T.L.; Day, C.N.; Habermann, E.B.; Boughey, J.C. Overuse of Axillary Surgery in Patients with Ductal Carcinoma In Situ: Opportunity for De-escalation. Ann. Surg. Oncol. 2022, 29, 7705–7712. [Google Scholar] [CrossRef] [PubMed]
- Davey, M.G.; O'Flaherty, C.; Cleere, E.F.; Nohilly, A.; Phelan, J.; Ronane, E.; Lowery, A.J.; Kerin, M.J. Sentinel lymph node biopsy in patients with ductal carcinoma in situ: Systematic review and meta-analysis. BJS Open 2022, 6, zrac022. [Google Scholar] [CrossRef] [PubMed]
- Karakatsanis, A.; Wärnberg, F.; Thompson, A.; Kwong, A.; Christenson, G.; Mohamed, I.; Nimeus, E.; Eriksson, S.; Nagy, G.; Patil, E.V. Sentinel Lymph Node Biopsy in Ductal Cancer In Situ or Unclear Lesions of the Breast and How to Not Do It. An Open-Label, Phase 3, Randomised Controlled Trial. (SentiNot 2.0). Available online: https://clinicaltrials.gov/ct2/show/NCT04722692 (accessed on 8 December 2022).
- Yu, K.-D.; Wu, L.-M.; Liu, G.-Y.; Wu, J.; Di, G.-H.; Shen, Z.-Z.; Shao, Z.-M. Different distribution of breast cancer subtypes in breast ductal carcinoma in situ (DCIS), DCIS with microinvasion, and DCIS with invasion component. Ann. Surg. Oncol. 2011, 18, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Connolly, J.L.; Edge, S.B.; Mittendorf, E.A.; Rugo, H.S.; Solin, L.J.; Weaver, D.L.; Winchester, D.J.; Hortobagyi, G.N. Breast cancer- major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin 2017, 67, 290–303. [Google Scholar] [CrossRef]
- Allison, K.H.; Brogi, E.; Ellis, I.O.; Fox, S.B.; Morris, E.A.; Sahin, A.; Salgado, R.; Sapino, A.; Sasano, H.; Schnitt, S.J.; et al. Microinvasive Carcinoma WHO Classification of Tumours of the Breast, 5th ed.; IARC Press: Lyon, France, 2019; pp. 110–113. [Google Scholar]
- Shaaban, A.M.; Hilton, B.; Clements, K.; Dodwell, D.; Sharma, N.; Kirwan, C.; Sawyer, E.; Maxwell, A.; Wallis, M.; Stobart, H.; et al. The presentation, management and outcome of patients with ductal carcinoma in situ (DCIS) with microinvasion (invasion ≤1 mm in size)-results from the UK Sloane Project. Br. J. Cancer 2022, 127, 2125–2132. [Google Scholar] [CrossRef]
- Sopik, V.; Sun, P.; Narod, S.A. Impact of microinvasion on breast cancer mortality in women with ductal carcinoma in situ. Breast Cancer Res. Treat. 2018, 167, 787–795. [Google Scholar] [CrossRef]
- Wang, W.; Zhu, W.; Du, F.; Luo, Y.; Xu, B. The Demographic Features, Clinicopathological Characteristics and Cancer-specific Outcomes for Patients with Microinvasive Breast Cancer: A SEER Database Analysis. Sci. Rep. 2017, 7, 42045. [Google Scholar] [CrossRef]
- Choi, B.; Jegatheeswaran, L.; Nakhoul, M.; Haria, P.; Srivastava, R.; Karki, S.; Lupi, M.; Patel, V.; Chakravorty, A.; Babu, E. Axillary staging in ductal carcinoma in situ with microinvasion: A meta-analysis. Surg. Oncol. 2021, 37, 101557. [Google Scholar] [CrossRef]
- Kim, M.; Kim, H.J.; Chung, Y.R.; Kang, E.; Kim, E.K.; Kim, S.H.; Kim, Y.J.; Kim, J.H.; Kim, I.A.; Park, S.Y. Microinvasive carcinoma versus ductal carcinoma in situ: A comparison of clinicopathological features and clinical outcomes. J. Breast Cancer 2018, 21, 197–205. [Google Scholar] [CrossRef]
- Magnoni, F.; Massari, G.; Santomauro, G.; Bagnardi, V.; Pagan, E.; Peruzzotti, G.; Galimberti, V.; Veronesi, P.; Sacchini, V.S. Sentinel lymph node biopsy in microinvasive ductal carcinoma in situ. Br. J. Surg. 2019, 106, 375–383. [Google Scholar] [CrossRef]
- Margalit, D.N.; Sreedhara, M.; Chen, Y.H.; Catalano, P.J.; Nguyen, P.L.; Golshan, M.; Overmoyer, B.A.; Harris, J.R.; Brock, J.E. Microinvasive breast cancer: ER, PR, and HER-2/neu status and clinical outcomes after breast-conserving therapy or mastectomy. Ann. Surg. Oncol. 2013, 20, 811–818. [Google Scholar] [CrossRef]
- Liu, B.-T.; Ding, J.-N.; Wang, J.-L.; Li, Z.-S.; Ding, Y.-L.; Ma, R. Differences in pathologic characteristics between ductal carcinoma in situ (DCIS), DCIS with microinvasion and DCIS with invasive ductal carcinoma. Int. J. Clin. Exp. Pathol. 2020, 13, 1066–1072. [Google Scholar] [PubMed]
- Champion, C.D.; Ren, Y.; Thomas, S.M.; Fayanju, O.M.; Rosenberger, L.H.; Greenup, R.A.; Menendez, C.S.; Hwang, E.S.; Plichta, J.K. DCIS with Microinvasion: Is It In Situ or Invasive Disease? Ann. Surg. Oncol. 2019, 26, 3124–3132. [Google Scholar] [CrossRef]
- Shiino, S.; Quinn, C.; Ball, G.; Syed, B.M.; Kurozumi, S.; Tsuda, H.; Rakha, E.A. Prognostic significance of microinvasion with ductal carcinoma in situ of the breast: A meta-analysis. Breast Cancer Res. Treat 2023, 197, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Hacking, S.M.; Leonard, K.L.; Wu, D.; Banks, M.; Graves, T.; Wang, L.; Yakirevich, E.; Wang, Y. Microinvasive breast cancer and the role of sentinel lymph node biopsy. Sci. Rep. 2022, 12, 12391. [Google Scholar] [CrossRef] [PubMed]
- Pfob, A.; Mehrara, B.J.; Nelson, J.A.; Wilkins, E.G.; Pusic, A.L.; Sidey-Gibbons, C. Towards Patient-Centered Decision-Making in Breast Cancer Surgery: Machine Learning to Predict Individual Patient-Reported Outcomes at 1-Year Follow-up. Ann. Surg 2021, 277, e144–e152. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magnoni, F.; Bianchi, B.; Corso, G.; Alloggio, E.A.; Di Silvestre, S.; Abruzzese, G.; Sacchini, V.; Galimberti, V.; Veronesi, P. Ductal Carcinoma In Situ (DCIS) and Microinvasive DCIS: Role of Surgery in Early Diagnosis of Breast Cancer. Healthcare 2023, 11, 1324. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11091324
Magnoni F, Bianchi B, Corso G, Alloggio EA, Di Silvestre S, Abruzzese G, Sacchini V, Galimberti V, Veronesi P. Ductal Carcinoma In Situ (DCIS) and Microinvasive DCIS: Role of Surgery in Early Diagnosis of Breast Cancer. Healthcare. 2023; 11(9):1324. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11091324
Chicago/Turabian StyleMagnoni, Francesca, Beatrice Bianchi, Giovanni Corso, Erica Anna Alloggio, Susanna Di Silvestre, Giuliarianna Abruzzese, Virgilio Sacchini, Viviana Galimberti, and Paolo Veronesi. 2023. "Ductal Carcinoma In Situ (DCIS) and Microinvasive DCIS: Role of Surgery in Early Diagnosis of Breast Cancer" Healthcare 11, no. 9: 1324. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare11091324