
Influence of Nicotine from Diverse Delivery Tools on the Autonomic Nervous and Hormonal Systems

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Volunteers
2.2. ECG Measurements and HRV Analysis
2.3. Biochemical Analyses
2.4. Microbiological Analyses
2.5. Nicotine Delivery Tools
3. Results
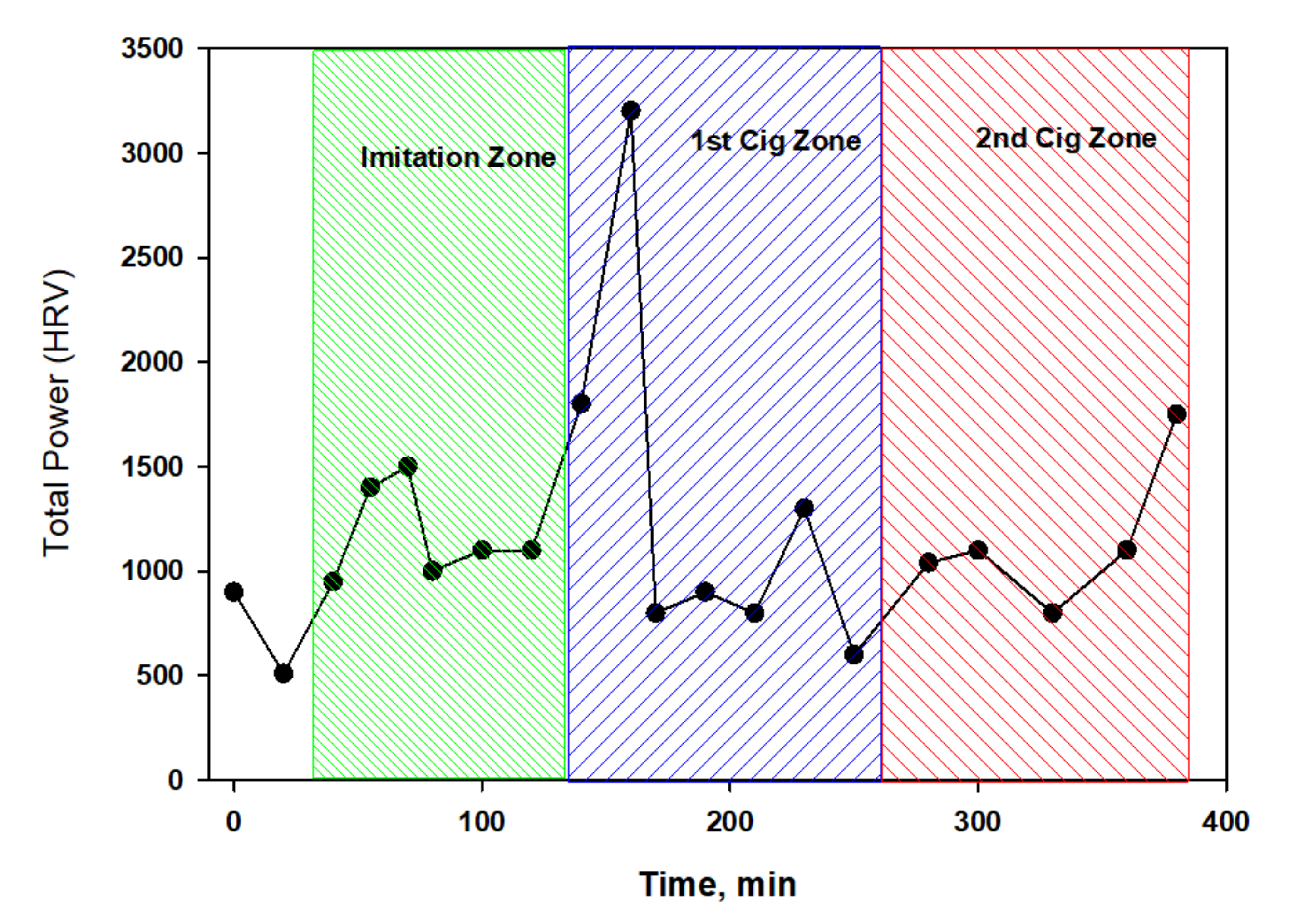
3.1. The Role of Smoke Components in Modulation of ANS Activity
3.2. Comparative Testing Nicotine-Containing Products with Analysis of HRV Changes
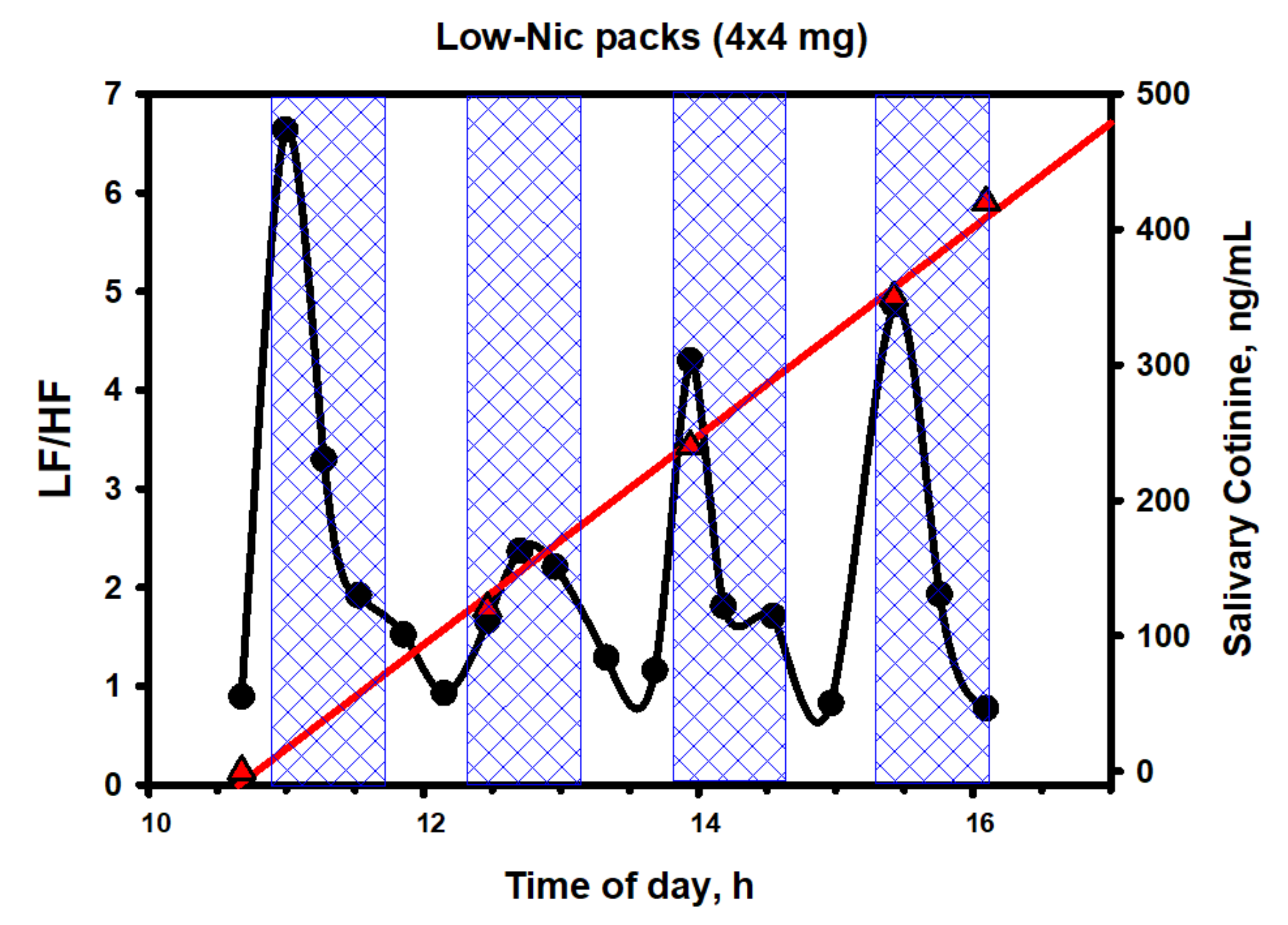
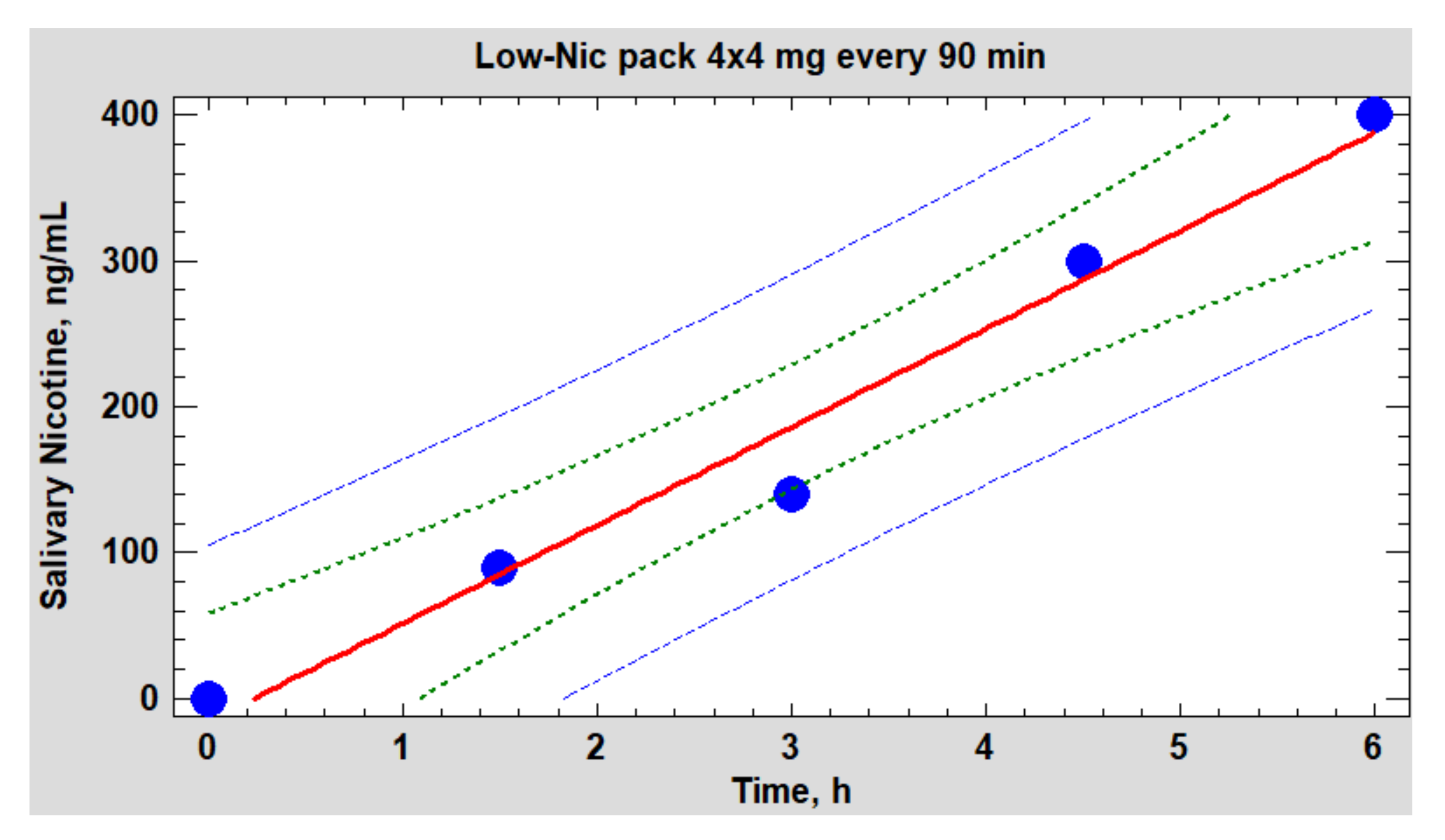
3.3. Testing Nicotine Packs with Systemic Use
4. Discussion
5. Practical Application
6. Conclusions
7. Outlook
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Biasi, M. Nicotinic mechanisms in the autonomic control of organ systems. J. Neurobiol. 2002, 53, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Dani, J.A.; De Biasi, M. Cellular mechanisms of nicotine addiction. Pharmacol. Biochem. Behav. 2001, 70, 439–446. [Google Scholar] [CrossRef]
- Jiloha, R.C. Biological basis of tobacco addiction: Implications for smoking-cessation treatment. Indian J. Psychiatry 2010, 52, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Task force of the European Society of Cardiology; The North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Hoyer, D.; Schmidt, A.; Pytlik, A.; Viehöfer, L.; Gonçalves, H.; Amorim-Costa, C.; Bernardes, J.; Ayres-de-Campos, D.; Lobmaier, S.M.; Schneider, U. Can fetal heart rate variability obtained from cardiotocography provide the same diagnostic value like from electrophysiological interbeat intervals? Physiol. Meas. 2021, 42, 015006. [Google Scholar] [CrossRef] [PubMed]
- Low, M.J. Neuroendocrinology. In Williams Textbook of Endocrinology; Elsevier: Amsterdam, The Netherlands, 2016; pp. 109–175. [Google Scholar] [CrossRef]
- Al-Wadei, H.A.; Plummer, H.K., 3rd; Ullah, M.F.; Unger, B.; Brody, J.R.; Schuller, H.M. Social stress promotes and γ-aminobutyric acid inhibits tumor growth in mouse models of non-small cell lung cancer. Cancer Prev. Res. 2012, 5, 189–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, M.B.; Le, X.; Heymach, J.V. β-Adrenergic signaling in lung cancer: A potential role for beta-blockers. J. Neuroimmune Pharmacol. 2020, 15, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Lang, K.; Bastian, P. Neurotransmitter effects on tumor cells and leukocytes. In Neuronal Activity in Tumor Tissue; Zänker, K.S., Entschladen, F., Eds.; Karger Publishers: Basel, Switzerland, 2002; Volume 39, pp. 99–121. [Google Scholar] [CrossRef]
- Barbieri, A.; Bimonte, S.; Palma, G.; Luciano, A.; Rea, D.; Giudice, A.; Scognamiglio, G.; La Mantia, E.; Franco, R.; Perdonà, S.; et al. The stress hormonehormone norepinephrine increases migration of prostate cancer cells in vitro and in vivo. Int. J. Oncol. 2015, 47, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borovikova, L.V.; Ivanova, S.; Zhang, M.; Yang, H.; Botchkina, G.I.; Watkins, L.R.; Wang, H.; Abumrad, N.; Eaton, J.W.; Tracey, K.J. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature 2000, 405, 458–462. [Google Scholar] [CrossRef] [PubMed]
- De Couck, M.; Gidron, Y. Norms of vagal nerve activity, indexed by Heart Rate Variability, in cancer patients. Cancer Epidemiol. 2013, 37, 737–741. [Google Scholar] [CrossRef]
- Walsh, D.; Nelson, K.A. Autonomic nervous system dysfunction in advanced cancer. Support. Care Cancer. 2002, 10, 523–528. [Google Scholar] [CrossRef]
- Hansen, M.V.; Rosenberg, J.; Gögenur, I. Lack of circadian variation and reduction of heart rate variability in women with breast cancer undergoing lumpectomy: A descriptive study. Breast Cancer. Res. Treat. 2013, 140, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Mouton, C.; Ronson, A.; Razavi, D.; Delhaye, F.; Kupper, N.; Paesmans, M.; Moreau, M.; Nogaret, J.M.; Hendlisz, A.; Gidron, Y. The relationship between heart rate variability and time-course of carcinoembryonic antigen in colorectal cancer. Auton. Neurosci. 2012, 166, 96–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, S.; Lou, J.; Zhang, Y.; Chen, P. Low heart rate variability relates to the progression of gastric cancer. World J. Surg. Oncol. 2018, 16, 49. [Google Scholar] [CrossRef] [Green Version]
- Drawz, P.; Babineau, D.; Brecklin, C.; He, J.; Kallem, R.; Soliman, E.; Xie, D.; Appleby, D.; Anderson, A.; Rahman, M.; et al. Heart rate variability is a predictor of mortality in chronic kidney disease: A report from the CRIC Study. Am. J. Nephrol. 2013, 38, 517–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murgia, F.; Melotti, R.; Foco, L.; Gögele, M.; Meraviglia, V.; Motta, B.; Steger, A.; Toifl, M.; Sinnecker, D.; Müller, A.; et al. Effects of smoking status, history and intensity on heart rate variability in the general population: The CHRIS study. PLoS ONE 2019, 14, e0215053. [Google Scholar] [CrossRef]
- Park, S.K.; O’Neill, M.S.; Vokonas, P.S.; Sparrow, D.; Schwartz, J. Effects of air pollution on heart rate variability: The VA normative aging study. Environ. Health Perspect. 2005, 113, 304–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utell, M.J.; Frampton, M.W.; Zareba, W.; Devlin, R.B.; Cascio, W.E. Cardiovascular effects associated with air pollution: Potential mechanisms and methods of testing. Inhal. Toxicol. 2002, 14, 1231–1247. [Google Scholar] [CrossRef]
- Stone, V.; Tuinman, M.; Vamvakopoulos, J.E.; Shaw, J.; Brown, D.; Petterson, S.; Faux, S.P.; Borm, P.; MacNee, W.; Michaelangeli, F.; et al. Increased calcium influx in a monocytic cell line on exposure to ultrafine carbon black. Eur. Respir. J. 2000, 15, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.D.; Zhang, W.; Victor, R.G. Impaired modulation of sympathetic vasoconstriction in contracting skeletal muscle of rats with chronic myocardial infarctions: Role of oxidative stress. Circ. Res. 2000, 88, 816–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronson, D.; Mittleman, M.A.; Burger, A.J. Interleukin-6 levels are inversely correlated with heart rate variability in patients with decompensated heart failure. J. Cardiovasc. Electrophysiol. 2001, 12, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Lutfi, M.F. Patterns of heart rate variability and cardiac autonomic modulations in controlled and uncontrolled asthmatic patients. BMC Pulm. Med. 2015, 15, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heusser, K.; Tank, J.; Holz, O.; May, M.; Brinkmann, J.; Engeli, S.; Diedrich, A.; Framke, T.; Koch, A.; Großhennig, A.; et al. Ultrafine particles and ozone perturb norepinephrine clearance rather than centrally generated sympathetic activity in humans. Sci. Rep. 2019, 9, 3641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pope, C.A., 3rd; Verrier, R.L.; Lovett, E.G.; Larson, A.C.; Raizenne, M.E.; Kanner, R.E.; Schwartz, J.; Villegas, G.M.; Gold, D.R.; Dockery, D.W. Heart rate variability associated with particulate air pollution. Am. Heart. J. 1999, 138, 890–899. [Google Scholar] [CrossRef]
- Godleski, J.J.; Verrier, R.L.; Koutrakis, P.; Catalano, P.; Coull, B.; Reinisch, U.; Lovett, E.G.; Lawrence, J.; Murthy, G.G.; Wolfson, J.M.; et al. Mechanisms of morbidity and mortality from exposure to ambient air particles. Res. Rep. Health Eff. Inst. 2000, 91, 5–88, discussion 89–103. [Google Scholar] [PubMed]
- Wang, J.B.; Olgin, J.E.; Nah, G.; Vittinghoff, E.; Cataldo, J.K.; Pletcher, M.J.; Marcus, G.M. Cigarette and e-cigarette dual use and risk of cardiopulmonary symptoms in the Health eHeart Study. PLoS ONE 2018, 13, e0198681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manohar, P.R.; Sorokin, O.; Chacko, J.; Nampoothiri, V. An exploratory clinical study to determine the utility of heart rate variability analysis in the assessment of dosha imbalance. J. Ayurveda Integr. Med. 2018, 9, 126–130. [Google Scholar] [CrossRef]
- Geisler, F.C.; Kubiak, T.; Siewert, K.; Weber, H. Cardiac vagal tone is associated with social engagement and self-regulation. Biol. Psychol. 2013, 93, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Teneggi, V.; Squassante, L.; Iavarone, L.; Milleri, S.; Bye, A.; Gomeni, R. Correlation and predictive performances of saliva and plasma nicotine concentration on tobacco withdrawal-induced craving. Br. J. Clin. Pharmacol. 2002, 54, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Osipov, G.A.; Boiko, N.B.; Fedosova, N.F.; Kasikhina, S.A.; Lyadov, K.V. Comparative gas chromatography-mass spectrometry study of the composition of microbial chemical markers in feces. Microb. Ecol. Health Dis. 2009, 21, 159–171. [Google Scholar] [CrossRef]
- Platonova, A.G.; Osipov, G.A.; Boiko, N.B.; Kirillova, N.V.; Rodionov, G.G. The chromatography-mass spectrometry analysis of microbial fatty acids in human biological fluids and their clinical significance. Klin. Lab. Diagn. 2015, 60, 46–55. (In Russian) [Google Scholar] [PubMed]
- Lee, S.; Lee, D.K. What is the proper way to apply the multiple comparison test? Korean J. Anesthesiol. 2018, 71, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Wang, Z.; Dong, J.; Pan, R.; Qiu, H.; Zhang, J.; Zhang, P.; Zheng, J.; Yu, W. Bilirubin modulates acetylcholine receptors in rat superior cervical ganglionic neurons in a bidirectional manner. Sci. Rep. 2014, 4, 7475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macmillanm, C.; Wildsmith, J.; Hamilton, W. Reversible increase in QT dispersion during carbon monoxide poisoning. Acta Anaesthesiol. Scand. 2001, 45, 396–397. [Google Scholar] [CrossRef] [PubMed]
- Dallas, M.L.; Yang, Z.; Boyle, J.P.; Boycott, H.E.; Scragg, J.L.; Milligan, C.J.; Elies, J.; Duke, A.; Thireau, J.; Reboul, C.; et al. Carbon monoxide induces cardiac arrhythmia via induction of the late Na+ current. Am. J. Respir. Crit. Care Med. 2012, 186, 648–656. [Google Scholar] [CrossRef] [Green Version]
- Andre, L.; Boissière, J.; Reboul, C.; Perrier, R.; Zalvidea, S.; Meyer, G.; Thireau, J.; Tanguy, S.; Bideaux, P.; Hayot, M.; et al. Carbon monoxide pollution promotes cardiac remodeling and ventricular arrhythmia in healthy rats. Am. J. Respir. Crit. Care Med. 2010, 181, 587–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reboul, C.; Thireau, J.; Meyer, G.; André, L.; Obert, P.; Cazorla, O.; Richard, S. Carbon monoxide exposure in the urban environment: An insidious foe for the heart? Respir. Physiol. Neurobiol. 2012, 184, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Schultz, H.D. The paradox of carbon monoxide and the heart. Am. J. Respir. Crit. Care Med. 2012, 186, 582–583. [Google Scholar] [CrossRef] [PubMed]
- Fowler, J.S.; Logan, J.; Wang, G.J.; Volkow, N.D. Monoamine oxidase and cigarette smoking. Neurotoxicol 2003, 24, 75–82. [Google Scholar] [CrossRef]
- Holschneider, D.P.; Scremin, O.U.; Chialvo, D.R.; Chen, K.; Shih, J.C. Heart rate dynamics in monoamine oxidase-A-and-B-deficient mice. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, H1751–H1759. [Google Scholar] [CrossRef] [Green Version]
- Dagnon, S.; Stoilova, A.; Ivanov, I.; Nikolova, S. The Effect of Cigarette Design on the Content of Phenols in Mainstream Tobacco Smoke. Beitr. Tabakforsch. Int./Contrib. Tob. Res. 2011, 24, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Youdim, K.A.; Shukitt-Hale, B.; Joseph, J.A. Flavonoids and the brain: Interactions at the blood–brain barrier and their physiological effects on the central nervous system. Free Radic. Biol. Med. 2004, 37, 1683–1693. [Google Scholar] [CrossRef]
- Aura, A.M. Microbial metabolism of dietary phenolic compounds in the colon. Phytochem. Rev. 2008, 7, 407–429. [Google Scholar] [CrossRef]
- Filosa, S.; Di Meo, F.; Crispi, S. Polyphenols-gut microbiota interplay and brain neuromodulation. Neural. Regen. Res. 2018, 13, 2055. [Google Scholar] [CrossRef] [PubMed]
- Duarte, A.A.; Mostarda, C.; Irigoyen, M.C.; Rigatto, K. A single dose of dark chocolate increases parasympathetic modulation and heart rate variability in healthy subjects. Rev. Nutr. 2016, 29, 765–773. [Google Scholar] [CrossRef] [Green Version]
- Cryer, P.; Haymond, M.; Santiago, J.; Shah, S. Norepinephrine and epinephrine release and adrenergic mediation of smoking-associated hemodynamic and metabolic events. N. Engl. J. Med. 1976, 295, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Shao, X.M.; Friedman, T.C. Pod-mod vs. conventional e-cigarettes: Nicotine chemistry, pH, and health effects. J. Appl. Physiol. 2020, 128, 1056–1058. [Google Scholar] [CrossRef] [PubMed]
- Salman, R.; Talih, S.; El-Hage, R.; Haddad, C.; Karaoghlanian, N.; El-Hellani, A.; Saliba, N.A.; Shihadeh, A. Free-base and total nicotine, reactive oxygen species, and carbonyl emissions from IQOS, a heated tobacco product. Nicotine Tob. Res. 2019, 21, 1285–1288. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.J.; Zhang, W.; Sarwinski, S. Presynaptic β2-adrenoceptors mediate nicotine-induced NOergic neurogenic dilation in porcine basilar arteries. Am. J. Physiol. Heart Circ. Physiol. 2000, 279, H808–H816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narkiewicz, K.; Van De Borne, P.J.; Hausberg, M.; Cooley, R.L.; Winniford, M.D.; Davison, D.E.; Somers, V.K. Cigarette smoking increases sympathetic outflow in humans. Circulation 1998, 98, 528–534. [Google Scholar] [CrossRef] [Green Version]
- Middlekauff, H.R.; Park, J.; Moheimani, R.S. Adverse effects of cigarette and noncigarette smoke exposure on the autonomic nervous system: Mechanisms and implications for cardiovascular risk. J. Am. Coll. Cardiol. 2014, 64, 1740–1750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassi, G.; Seravalle, G.; Calhoun, D.A.; Bolla, G.B.; Giannattasio, C.; Marabini, M.; Del Bo, A.; Mancia, G. Mechanisms responsible for sympathetic activation by cigarette smoking in humans. Circulation 1994, 90, 248–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hering, D.; Somers, V.K.; Kara, T.; Kucharska, W.; Jurak, P.; Bieniaszewski, L.; Narkiewicz, K. Sympathetic neural responses to smoking are age dependent. J. Hypertens. 2006, 24, 691–695. [Google Scholar] [CrossRef]
- Cachope, R.; Mateo, Y.; Mathur, B.N.; Irving, J.; Wang, H.L.; Morales, M.; Lovinger, D.M.; Cheer, J.F. Selective activation of cholinergic interneurons enhances accumbal phasic dopamine release: Setting the tone for reward processing. Cell. Rep. 2012, 2, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Prieto, J.C.; Quevedo, M.; Kutz, M.; Pérez Olea, J. Influencia vagal en las arritmias experimentales por dopamine. Arch. Inst. Cardiol. Méx. 1985, 55, 395–398. [Google Scholar]
- Mohebi, A.; Pettibone, J.; Hamid, A.; Wong, J.; Vinson, L.; Patriarchi, T.; Tian, L.; Kennedy, R.; Berke, J. Dissociable dopamine dynamics for learning and motivation. Nature 2019, 570, 65–70. [Google Scholar] [CrossRef]
- Bressan, R.A.; Crippa, J.A. The role of dopamine in reward and pleasure behaviour–review of data from preclinical research. Acta Psychiatr. Scand. 2005, 111, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.S.; Swoboda, K.J.; Miles, J.M.; Coppack, S.W.; Aneman, A.; Holmes, C.; Lamensdorf, I.; Eisenhofer, G. Sources and physiological significance of plasma dopamine sulfate. J. Clin. Endocrinol. Metab. 1999, 84, 2523–2531. [Google Scholar] [CrossRef]
- Eldrup, E.; Møller, S.E.; Andreasen, J.; Christensen, N.J. Effects of ordinary meals on plasma concentrations of 3,4-dihydroxyphenylalanine, dopamine sulphate and 3,4-dihydroxyphenylacetic acid. Clin. Sci. 1997, 92, 423–430. [Google Scholar] [CrossRef]
- Eisenhofer, G.; Aneman, A.; Friberg, P.; Hooper, D.; Fandriks, L.; Lonroth, H.; Hunyady, B.; Mezey, E. Substantial production of dopamine in the human gastrointestinal tract. J. Clin. Endocrinol. Metab. 1997, 82, 3864–3871. [Google Scholar] [CrossRef]
- Wolfovitz, E.; Grossman, E.; Folio, C.J.; Keiser, H.R.; Kopin, I.J.; Goldstein, D.S. Derivation of urinary dopamine from plasma dihydroxyphenylalanine in humans. Clin. Sci. 1993, 84, 549–557. [Google Scholar] [CrossRef]
- Goldstein, D.S.; Holmes, C. Neuronal source of plasma dopamine. Clin. Chem. 2008, 54, 1864–1871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannelli, M.; De Feo, M.L.; Maggi, M.; Salvetti, A.; Giusti, G.; Serio, M. Does endogenous dopamine modulate human sympathetic activity through DA2 receptors? Eur. J. Clin. Pharmacol. 1985, 29, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Mannelli, M.; Pupilli, C.; Fabbri, G.; Musante, R.; De Feo, M.L.; Franchi, F.; Giusti, G. Endogenous dopamine (DA) and DA2 receptors: A mechanism limiting excessive sympathetic-adrenal discharge in humans. J. Clin. Endocrinol. Metab. 1988, 66, 626–631. [Google Scholar] [CrossRef]
- Asano, Y.; Hiramoto, T.; Nishino, R.; Aiba, Y.; Kimura, T.; Yoshihara, K.; Koga, Y.; Sudo, N. Critical role of gut microbiota in the production of biologically active, free catecholamines in the gut lumen of mice. American journal of physiology. Gastrointest. Liver Physiol. 2012, 303, G1288–G1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cryan, J.F.; Dinan, T.G. Mind-altering microorganisms: The impact of the gut microbiota on brain and behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef]
- Xue, R.; Zhang, H.; Pan, J.; Du, Z.; Zhou, W.; Zhang, Z.; Tian, Z.; Zhou, R.; Bai, L. Peripheral dopamine controlled by gut microbes inhibits invariant natural killer T cell-mediated hepatitis. Front. Immunol. 2018, 9, 2398. [Google Scholar] [CrossRef] [Green Version]
- Yoneda, S.; Alexander, N.; Vlachakis, N.D. Enzymatic deconjugation of catecholamines in human and rat plasma and red blood cell lysate. Life Sci. 1983, 33, 935–942. [Google Scholar] [CrossRef]
- Kur’yanova, E.V.; Stupin, V.O.; Tryasuchev, A.V.; Teplyi, D.L. Effects of blockage of peripheral choline, serotonin, and dopamine receptors on heart rhythm variability in rats under conditions of stimulation of neurotransmitter systems. Bull. Exp. Biol. Med. 2019, 168, 193–198. [Google Scholar] [CrossRef]
- Bruce, E.N.; Bruce, M.C. A multicompartment model of carboxyhemoglobin and carboxymyoglobin responses to inhalation of carbon monoxide. J. Appl. Physiol. 2003, 95, 1235–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cronenberger, C.; Mould, D.R.; Roethig, H.J.; Sarkar, M. Population pharmacokinetic analysis of carboxyhaemoglobin concentrations in adult cigarette smokers. Br. J. Clin. Pharmacol. 2008, 65, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schober, W.; Szendrei, K.; Matzen, W.; Osiander-Fuchs, H.; Heitmann, D.; Schettgen, T.; JÖrres, R.A.; Fromme, H. Use of electronic cigarettes (e-cigarettes) impairs indoor air quality and increases FeNO levels of e-cigarette consumers. Int. J. Hyg. Environ. Health 2014, 217, 628–637. [Google Scholar] [CrossRef]
- Li, G.; Wang, H.; Wang, K.; Wang, W.; Dong, F.; Qian, Y.; Gong, H.; Hui, C.; Xu, G.; Li, Y.; et al. The association between smoking and blood pressure in men: A cross-sectional study. BMC Public Health 2017, 17, 797. [Google Scholar] [CrossRef] [PubMed]
- Nadel, J.A. Pathophysiology of asthma: Neural effects on airway smooth muscle, submucosal glands, breathing, and cough. Prog. Respir. Res. 1980, 14, 1–8. [Google Scholar] [CrossRef]
- Gold, W.M. Anticholinergic drugs. In Allergy: Principles and Practice; Middleton, E., Reed, C.E., Ellis, E.F., Eds.; CV Mosby Co.: St. Louis, MO, USA, 1978; pp. 499–530. [Google Scholar]
- Franco, O.S.; Júnior, A.; Signori, L.U.; Prietsch, S.O.; Zhang, L. Cardiac autonomic modulation assessed by heart rate variability in children with asthma. Pediatr. Pulmonol. 2020, 55, 1334–1339. [Google Scholar] [CrossRef]
- Antoniewicz, L.; Brynedal, A.; Hedman, L.; Lundbäck, M.; Bosson, J.A. Acute effects of electronic cigarette inhalation on the vasculature and the conducting airways. Cardiovasc. Toxicol. 2019, 19, 441–450. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Cooke, J.P. The role of nicotine in the pathogenesis of atherosclerosis. Atherosclerosis 2011, 215, 281–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansson, J.; Galanti, M.R.; Hergens, M.P.; Fredlund, P.; Ahlbom, A.; Alfredsson, L.; Bellocco, R.; Eriksson, M.; Hallqvist, J.; Hedblad, B.; et al. Use of snus and acute myocardial infarction: Pooled analysis of eight prospective observational studies. Eur. J. Epidemiol. 2012, 27, 771–779. [Google Scholar] [CrossRef]
- Joseph, A.M.; Norman, S.M.; Ferry, L.H.; Prochazka, A.V.; Westman, E.C.; Steele, B.G.; Sherman, S.E.; Cleveland, M.; Antonuccio, D.O.; Hartman, N.; et al. The safety of transdermal nicotine as an aid to smoking cessation in patients with cardiac disease. New Eng. J. Med. 1996, 335, 1792–1798. [Google Scholar] [CrossRef]
- Fedorova, G.F.; Kancheva, V.D.; Menshov, V.A.; Naumov, V.V.; Vasil’ev, R.F.; Veprintsev, T.L.; Trofimov, A.V.; Tsaplev, Y.B.; Yablonskaya, O.I. Exogenous and endogenous mediators of oxygen metabolism: Alternatives for chemical and biological activity. Stud. Nat. Prod. Chem. 2016, 47, 357–385. [Google Scholar] [CrossRef]
- Menshov, V.A.; Trofimov, A.V. Hydrogen peroxide derived from cigarette smoke: “Pardon impossible, to be sent to Siberia?”. Mini-Rev. Org. Chem. 2011, 8, 394–400. [Google Scholar] [CrossRef]
- Palmina, N.P.; Maltseva, E.L.; Chasovskaya, T.E.; Kasparov, V.V.; Bogdanova, N.G.; Menshov, V.A.; Trofimov, A.V. Effects of different phases of cigarette smoke on lipid peroxidation and membrane structure in liposomes. Aust. J. Chem. 2014, 67, 858–866. [Google Scholar] [CrossRef]
- Fedorova, G.F.; Menshov, V.A.; Trofimov, A.V.; Tsaplev, Y.B.; Vasil’ev, R.F.; Yablonskaya, O.I. Chemiluminescence of cigarette smoke: Salient features of the phenomenon. Photochem. Photobiol. 2017, 93, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Menshov, V.A.; Kancheva, V.D.; Yablonskaya, O.I.; Trofimov, A.V. Transformation of the antioxidant properties of tar from tobacco smoke in metabolic processes: Model chemiluminescence study. Russ. J. Phys. Chem. B 2021, 15, 108–111. [Google Scholar] [CrossRef]
- Balansky, R.; La Maestra, S.; Kancheva, V.D.; Trofimov, A.V.; Djongov, L.; De Flora, S. Clastogenic effects of cigarette smoke and urethane and their modulation by olive oil, curcumin and carotenoids in adult mice and fetuses. Food Chem. Toxicol. 2021, 155, 112383. [Google Scholar] [CrossRef] [PubMed]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hormone | 0 h (Control) | 1 h | 2 h | Norm Limits | |
|---|---|---|---|---|---|
| Min | Max | ||||
| Adrenaline, pg/mL | 42 | 47 | 46 | 0 | 110 |
| Noradrenaline, pg/mL | 308 | 344 | 395 | 70 | 750 |
| Dopamine b, pg/mL | 5 | 334 * | 530 * | 0 | 87 |
| Serotonin, ng/mL | 136 | 184 | 194 | 50 | 220 |
| ACTH c, pg/mL | 8.5 | 8.95 | 8 | 5 | 46 |
| STH d, ng/mL | 1.44 | 0.07 | 0.64 | 0 | 8.00 |
| Microorganisms | Before the Experiment | Norm | After the Experiment | % of Change |
|---|---|---|---|---|
| Residential (a sum) | 10,780 | 19,627 | 12,837 | +19.6 |
| Transitory (a sum) | 0 | 33 | 0 | 0 |
| Including | ||||
| Anaerobic bacteria | 10,476 | 17,687 | 12,085 | +15.3 |
| Firmicutes | 7504 | 12,085 | 9305 | +61.0 |
| Actinobacteria | 3251 | 7477 | 3441 | +5.8 |
| Bacteroidia, Flavobacteria | 0 | 35 | 0 | 0 |
| Proteobacteria | 26 | 63 | 86 | +231 |
| Fungi | 1328 | 2332 | 2974 | +124 |
| Viruses | 517 | 1444 | 2348 | +354 |
| Endotoxin, nmol/mL | 0.08 | 0.5 | 0.26 | +225 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menshov, V.A.; Trofimov, A.V.; Zagurskaya, A.V.; Berdnikova, N.G.; Yablonskaya, O.I.; Platonova, A.G. Influence of Nicotine from Diverse Delivery Tools on the Autonomic Nervous and Hormonal Systems. Biomedicines 2022, 10, 121. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10010121
Menshov VA, Trofimov AV, Zagurskaya AV, Berdnikova NG, Yablonskaya OI, Platonova AG. Influence of Nicotine from Diverse Delivery Tools on the Autonomic Nervous and Hormonal Systems. Biomedicines. 2022; 10(1):121. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10010121
Chicago/Turabian StyleMenshov, Valerii A., Aleksei V. Trofimov, Alla V. Zagurskaya, Nadezda G. Berdnikova, Olga I. Yablonskaya, and Anna G. Platonova. 2022. "Influence of Nicotine from Diverse Delivery Tools on the Autonomic Nervous and Hormonal Systems" Biomedicines 10, no. 1: 121. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10010121