
lnc-IL7R Expression Reflects Physiological Pulmonary Function and Its Aberration Is a Putative Indicator of COPD

 , , , , , , ,
, , , , , , ,
Abstract
:1. Clinical Relevance
- (i)
- Protracted ‘smoldering’ inflammation, repeated lung injury, and accelerated lung aging are implicated in the enhanced predisposition to or progression of COPD;
- (ii)
- Altered lnc-IL7R expression in the human airway epithelium and blood is clinically relevant in pulmonary pathophysiology;
- (iii)
- The lnc-IL7R level is significantly downregulated in patients with COPD and is correlated with disease progression;
- (iv)
- The correlation of circulating lnc-IL7R with improved pulmonary function, and anti-correlation with PM2.5, PM10, and SO2 provide some mechanistic insights into pulmonary dysfunction and COPD, as well as suggest potential actionable novel biotherapeutics/biologics for the treatment of COPD.
2. Introduction
3. Methods
Statistical Analysis
4. Results
4.1. Baseline Characteristics of Our COPD Cohort
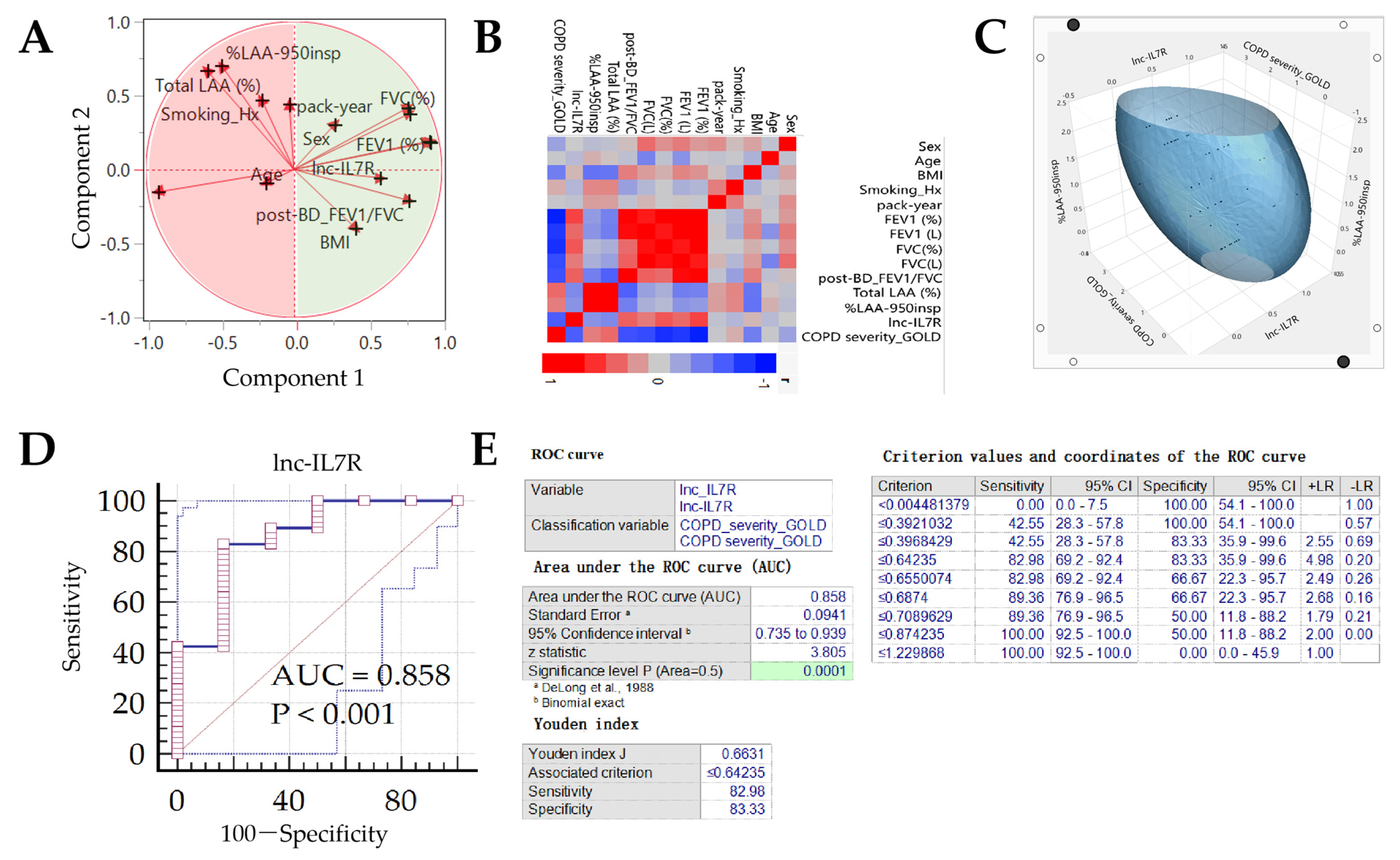
4.2. lnc-IL7R Expression Is Associated with Physiological Pulmonary Function and Exhibits Diagnostic Relevance for COPD-Based Patient Stratification
4.3. lnc-IL7R Level Correlates with COPD Status and Emphysematous Phenotype, and Its Differential Expression Reflects Disease Course
4.4. lnc-IL7R, a Probable Biological Response Modifier, Exhibits Strong Anti-COPD Therapeutic Potential
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Negewo, N.A.; Gibson, P.G.; McDonald, V.M. COPD and its comorbidities: Impact, measurement and mechanisms. Respirology 2015, 20, 1160–1171. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Estimates. 2020. Available online: https://www.who.int/data/global-health-estimates (accessed on 21 February 2022).
- Wu, S.M.; Sun, W.L.; Lee, K.Y.; Lin, C.W.; Feng, P.H.; Chuang, H.C.; Ho, S.C.; Chen, K.Y.; Chen, T.T.; Liu, W.T.; et al. Determinants of Pulmonary Emphysema Severity in Taiwanese Patients with Chronic Obstructive Pulmonary Disease: An Integrated Epigenomic and Air Pollutant Analysis. Biomedicines 2021, 9, 1833. [Google Scholar] [CrossRef] [PubMed]
- Sinden, N.J.; Stockley, R.A. Systemic inflammation and comorbidity in COPD: A result of ‘overspill’ of inflammatory mediators from the lungs? Review of the evidence. Thorax 2010, 65, 930–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, P.T. Inflammation in chronic obstructive pulmonary disease and its role in cardiovascular disease and lung cancer. Clin. Transl. Med. 2015, 4, 68. [Google Scholar] [CrossRef] [Green Version]
- Barnes, P.J. Cellular and molecular mechanisms of asthma and COPD. Clin. Sci. 2017, 131, 1541–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, P.J. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2016, 138, 16–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, P.; Celli, B.; Agustí, A.; Boje Jensen, G.; Divo, M.; Faner, R.; Guerra, S.; Marott, J.L.; Martinez, F.D.; Martinez-Camblor, P.; et al. Lung-Function Trajectories Leading to Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2015, 373, 111–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercado, N.; Ito, K.; Barnes, P.J. Accelerated ageing of the lung in COPD: New concepts. Thorax 2015, 70, 482–489. [Google Scholar] [CrossRef] [Green Version]
- Penkala, I.J.; Liberti, D.C.; Pankin, J.; Sivakumar, A.; Kremp, M.M.; Jayachandran, S.; Katzen, J.; Leach, J.P.; Windmueller, R.; Stolz, K.; et al. Age-dependent alveolar epithelial plasticity orchestrates lung homeostasis and regeneration. Cell Stem Cell 2021, 28, 1775–1789.e5. [Google Scholar] [CrossRef]
- Zacharias, W.J.; Frank, D.B.; Zepp, J.A.; Morley, M.P.; Alkhaleel, F.A.; Kong, J.; Zhou, S.; Cantu, E.; Morrisey, E.E. Regeneration of the lung alveolus by an evolutionarily conserved epithelial progenitor. Nature 2018, 555, 251–255. [Google Scholar] [CrossRef]
- Johnson, J.D.; Theurer, W.M. A stepwise approach to the interpretation of pulmonary function tests. Am. Fam. Physician. 2014, 89, 359–366. [Google Scholar] [PubMed]
- Devadoss, D.; Long, C.; Langley, R.J.; Manevski, M.; Nair, M.; Campos, M.A.; Borchert, G.; Rahman, I.; Chand, H.S. Long Noncoding Transcriptome in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Cell Mol. Biol. 2019, 61, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.M.; Feng, P.H.; Chuang, H.C.; Ho, S.C.; Fan Chung, K.; Chen, K.Y.; Wu, G.S.; Chen, T.T.; Tseng, C.H.; Liu, W.T.; et al. Impaired lnc-IL7R modulatory mechanism of Toll-like receptors is associated with an exacerbator phenotype of chronic obstructive pulmonary disease. FASEB J. 2020, 34, 13317–13332. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease Global Initiative for Chronic Obstructive Lung Disease. 2020. Available online: http://www.goldcopd.org/ (accessed on 22 October 2021).
- Occhipinti, M.; Paoletti, M.; Bartholmai, B.J.; Rajagopalan, S.; Karwoski, R.A.; Nardi, C.; Inchingolo, R.; Larici, A.R.; Camiciottoli, G.; Lavorini, F.; et al. Spirometric assessment of emphysema presence and severity as measured by quantitative CT and CT-based radiomics in COPD. Respir. Res. 2019, 20, 101. [Google Scholar] [CrossRef] [Green Version]
- Hastie, A.T.; Martinez, F.J.; Curtis, J.L.; Doerschuk, C.M.; Hansel, N.N.; Christenson, S.; Putcha, N.; Ortega, V.E.; Li, X.; Barr, R.G.; et al. Association of sputum and blood eosinophil concentrations with clinical measures of COPD severity: An analysis of the SPIROMICS cohort. Lancet Respir. Med. 2017, 5, 956–967. [Google Scholar] [CrossRef]
- Ernst, P.; Saad, N.; Suissa, S. Inhaled corticosteroids in COPD: The clinical evidence. Eur. Respir. J. 2015, 45, 525–537. [Google Scholar] [CrossRef] [Green Version]
- Leung, J.M.; Obeidat, M.; Sadatsafavi, M.; Sin, D.D. Introduction to precision medicine in COPD. Eur. Respir. J. 2019, 53, 1802460. [Google Scholar] [CrossRef]
- Drucker, E.; Krapfenbauer, K. Pitfalls and limitations in translation from biomarker discovery to clinical utility in predictive and personalised medicine. EPMA J. 2013, 4, 7. [Google Scholar] [CrossRef] [Green Version]
- Mannino, D.M. Biomarkers for chronic obstructive pulmonary disease diagnosis and progression: Insights, disappointments and promise. Curr. Opin. Pulm. Med. 2019, 25, 144–149. [Google Scholar] [CrossRef]
- Topalovic, M.; Exadaktylos, V.; Decramer, M.; Berckmans, D.; Troosters, T.; Janssens, W. Using dynamics of forced expiration to identify COPD where conventional criteria for the FEV₁ /FVC ratio do not match. Respirology 2015, 20, 925–931. [Google Scholar] [CrossRef] [Green Version]
- Lowe, K.E.; Regan, E.A.; Anzueto, A.; Austin, E.; Austin, J.H.M.; Beaty, T.H.; Benos, P.V.; Benway, C.J.; Bhatt, S.P.; Bleecker, E.R.; et al. COPDGene® 2019: Redefining the Diagnosis of Chronic Obstructive Pulmonary Disease. Chronic Obstr. Pulm. Dis. 2019, 6, 384–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, K.A.; Strand, M.; Ragland, M.F.; Kinney, G.L.; Austin, E.E.; Regan, E.A.; Lowe, K.E.; Make, B.J.; Silverman, E.K.; Crapo, J.D.; et al. Pulmonary Subtypes Exhibit Differential Global Initiative for Chronic Obstructive Lung Disease Spirometry Stage Progression: The COPDGene® Study. Chronic Obstr. Pulm. Dis. 2019, 6, 414–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Patients with COPD (GOLD Stage, n = 125) | |||
|---|---|---|---|---|
| I (n = 18) | II (n = 58) | III (n = 38) | IV (n = 11) | |
| Age (years) | ||||
| Median (IQR) | 68.00 (65.25–71.50) | 68.50 (62.25–73.00) | 70.50 (67.00–77.25) | 66.00 (63.00–69.00) |
| Sex, n (%) | ||||
| Male | 17 (94.44) | 55 (94.83) | 31 (81.58) | 9 (81.82) |
| Female | 1 (5.56) | 3 (5.17) | 7 (18.42) | 2 (18.18) |
| BMI, Kg/m2 | ||||
| Median (IQR) | 23.90 (21.63–26.29) | 24.14 (21.16–26.60) | 22.30 (20.00–24.50) | 20.60 (19.90–22.98) |
| Tobacco smoking, n (%) | ||||
| Current smoker | 5 (27.78) | 31 (53.44) | 11 (28.95) | 2 (18.18) |
| Ex-smoker | 13 (72.22) | 23 (39.66) | 22 (57.89) | 8 (72.73) |
| Never-smoker | 0 (0.00) | 4 (6.90) | 5 (13.16) | 1 (9.09) |
| Smoking pack-years | ||||
| Mean ± SD (Min-Max) | 48.89 ± 35.19 (5.00–150.00) | 49.02 ± 36.34 (0.00–180.00) | 49.30 ± 35.66 (0.00–156.00) | 56.73 ± 37.65 (0.00–123.00) |
| Median (IQR) | 42.50 (20.50–60.00) | 40.00 (23.00–60.00) | 40.00 (25.00–75.00) | 46.00 (35.00–85.00) |
| Pulmonary function indices | ||||
| FEV1 (L) Median (IQR) | 1.90 (1.74–2.11) | 1.61 b’ (1.38–1.90 | 0.99 a’b’c’d’ (0.74–1.12) | 0.58 a’b’c’d’ (0.52–0.66) |
| FEV1 % Median (IQR) | 84.55 (81.3–86.68) | 65.00 ab’c (57.38–72.00) | 39.05 a’b’c’d’ (35.00–45.00) | 25.00 a’b’c’d’ (22.10–27.95) |
| FEV1/FVC % Median (IQR) | 63.68 (61.25–66.87) | 59.25 a’b’ (54.12–65.50) | 46.50 a’b’c’d’ (42.11–55.25) | 41.41 a’b’c’d’ (30.93–45.67) |
| Emphysema severity | ||||
| Null/Mild (%) | 66.67 | 19.05 | 0.00 | 0.00 |
| Moderate (%) | 33.33 | 66.67 | 69.23 | 20.00 |
| Severe (%) | 0.00 | 14.28 | 30.77 | 80.00 |
| Lnc-IL7R expression | ||||
| Median (IQR) | 0.88 (0.79–0.94) | 0.59 (0.50–0.69) | 0.29 (0.19–0.41) | 0.18 (0.14–0.43) |
| COPD exacerbation in previous year | ||||
| 1.21 ± 1.03 | 1.09 ± 1.01 | 3.59 ± 2.10 | 3.74 ± 1.35 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bamodu, O.A.; Wu, S.-M.; Feng, P.-H.; Sun, W.-L.; Lin, C.-W.; Chuang, H.-C.; Ho, S.-C.; Chen, K.-Y.; Chen, T.-T.; Tseng, C.-H.; et al. lnc-IL7R Expression Reflects Physiological Pulmonary Function and Its Aberration Is a Putative Indicator of COPD. Biomedicines 2022, 10, 786. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040786
Bamodu OA, Wu S-M, Feng P-H, Sun W-L, Lin C-W, Chuang H-C, Ho S-C, Chen K-Y, Chen T-T, Tseng C-H, et al. lnc-IL7R Expression Reflects Physiological Pulmonary Function and Its Aberration Is a Putative Indicator of COPD. Biomedicines. 2022; 10(4):786. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040786
Chicago/Turabian StyleBamodu, Oluwaseun Adebayo, Sheng-Ming Wu, Po-Hao Feng, Wei-Lun Sun, Cheng-Wei Lin, Hsiao-Chi Chuang, Shu-Chuan Ho, Kuan-Yuan Chen, Tzu-Tao Chen, Chien-Hua Tseng, and et al. 2022. "lnc-IL7R Expression Reflects Physiological Pulmonary Function and Its Aberration Is a Putative Indicator of COPD" Biomedicines 10, no. 4: 786. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040786