
Acute Pulmonary Embolism in COVID-19: A Potential Connection between Venous Congestion and Thrombus Distribution

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
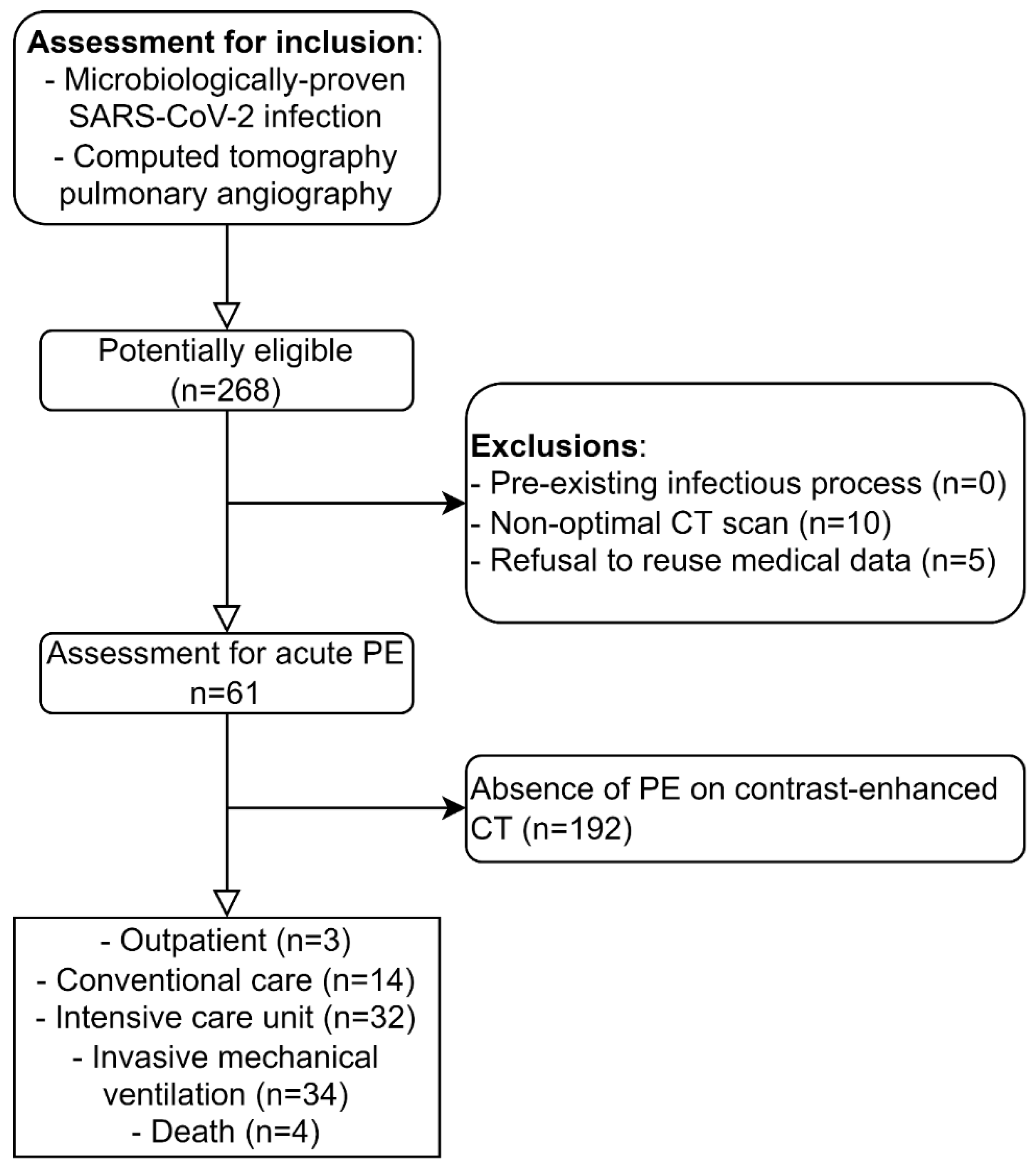
2.1. Study Design and Cohort
2.2. Data Analysis
2.2.1. Clinical Data
2.2.2. Imaging Data
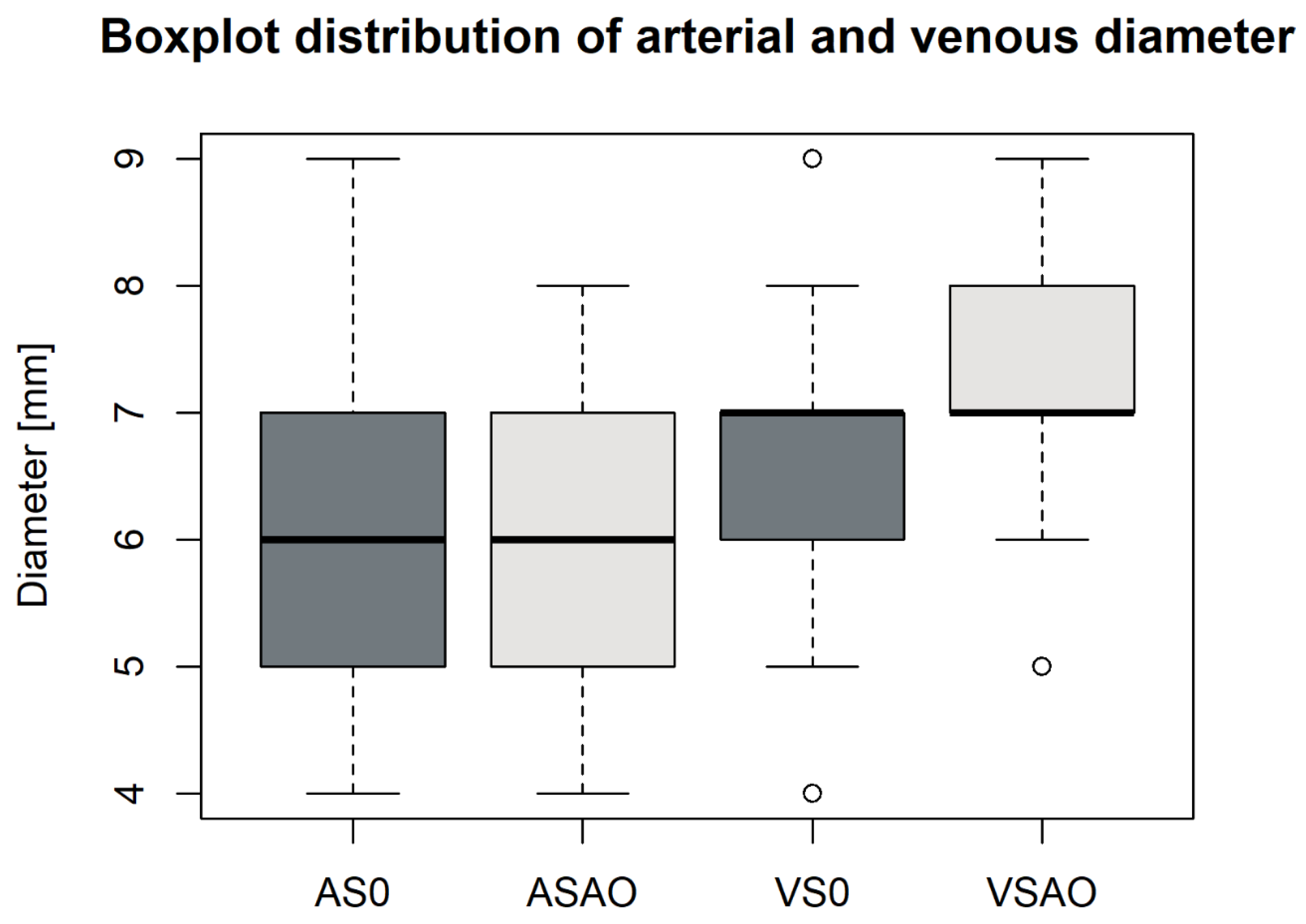
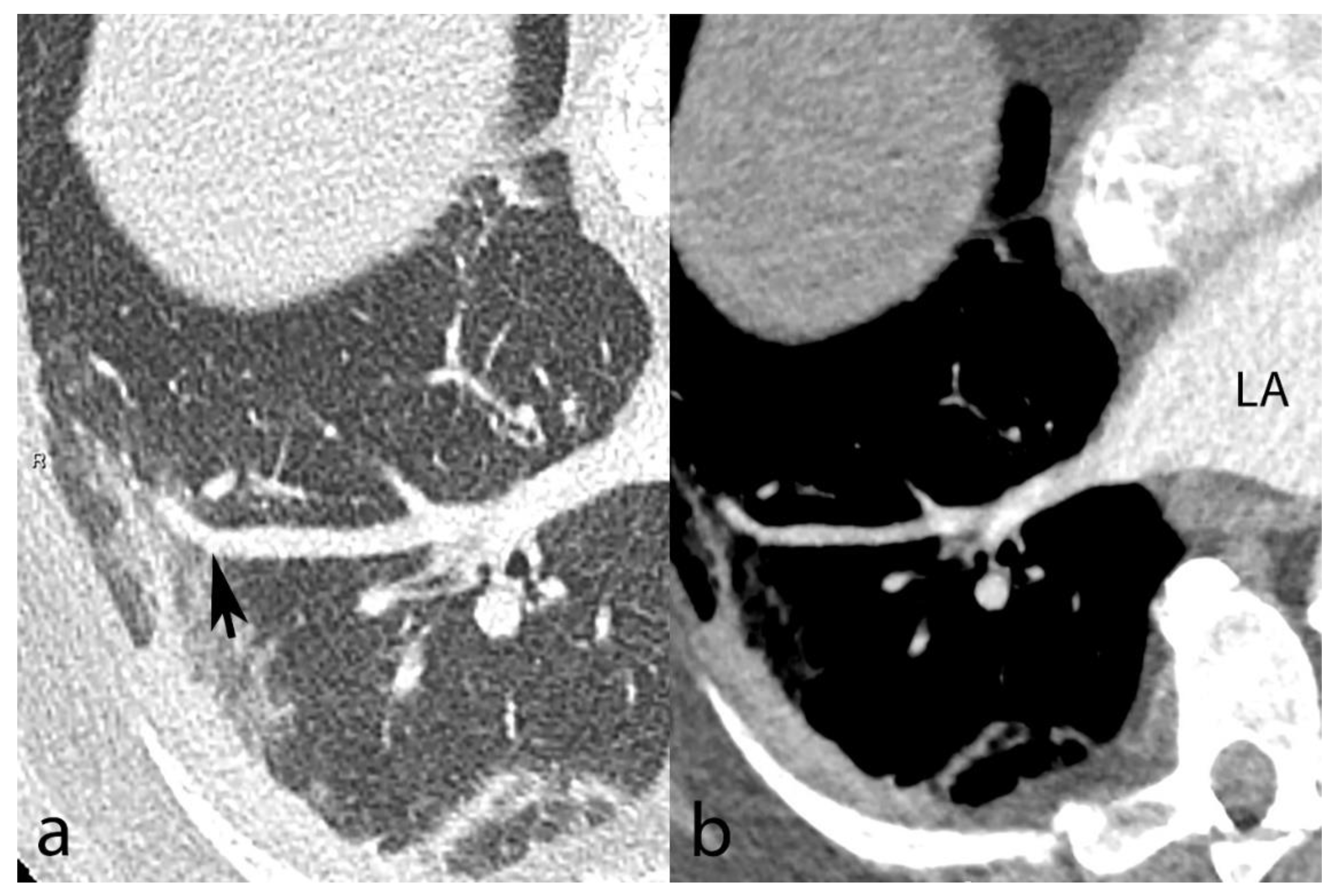
2.2.3. Vascular Dilatation
2.2.4. Degree of Pulmonary Artery Obstruction
2.2.5. Alveolar Opacity
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Vascular Changes
3.3. Anatomic Distribution of Pulmonary Emboli
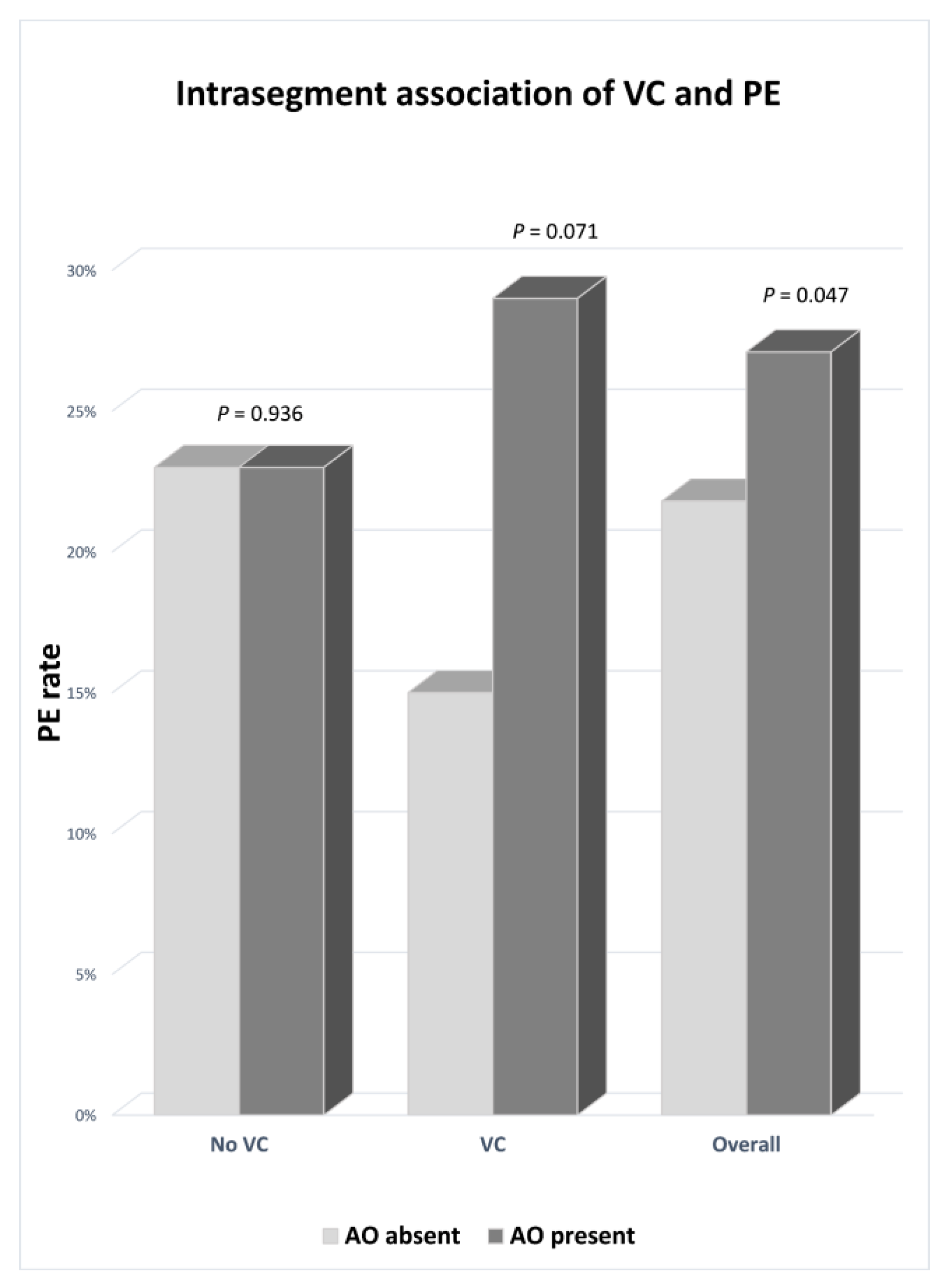
3.4. Relationship between Pulmonary Embolism, Venous Congestion, and Alveolar Opacity
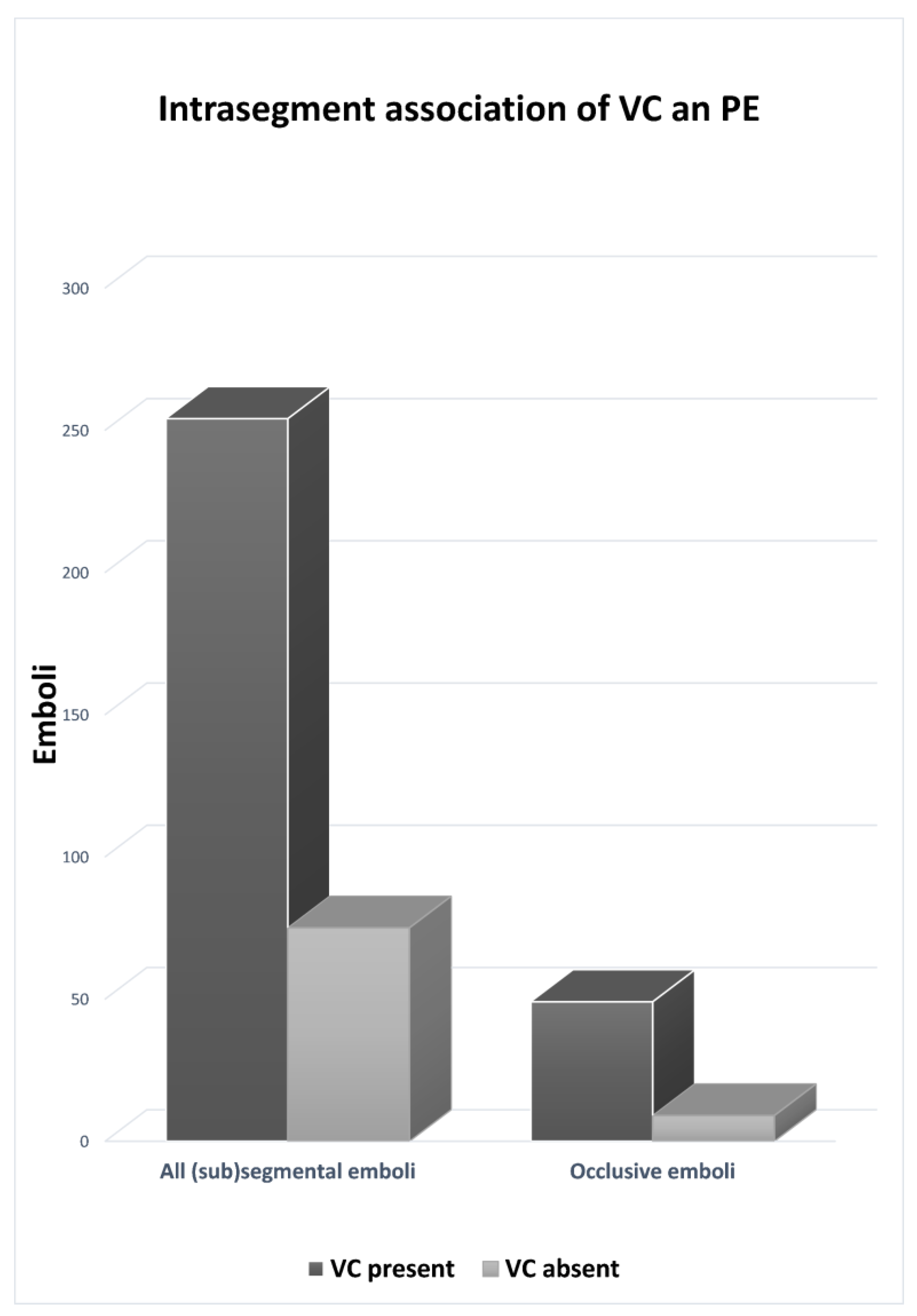
3.4.1. Distribution of Pulmonary Embolism in Segments with Venous Congestion
3.4.2. Distribution of Pulmonary Embolism Related to Alveolar Opacity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: An updated analysis. Thromb. Res. 2020, 191, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Pavon, A.G.; Meier, D.; Samim, D.; Rotzinger, D.C.; Fournier, S.; Marquis, P.; Monney, P.; Muller, O.; Schwitter, J. First Documentation of Persistent SARS-CoV-2 Infection Presenting With Late Acute Severe Myocarditis. Can. J. Cardiol. 2020, 36, 1326.e5–1326.e7. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Wang, D.W.; Zhao, C. Cardiovascular Involvement in Patients with 2019 Novel Coronavirus Disease. J. Transl. Int. Med. 2021, 9, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Qanadli, S.D.; Rocha, A.C.; Rotzinger, D.C. Case Report: Intrapulmonary Arteriovenous Anastomoses in COVID-19-Related Pulmonary Vascular Changes: A New Player in the Arena? Front. Med. 2021, 8, 639152. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.S.; Lee, A.G.; Renz, J.; DeSantis, K.; Liang, J.; Powell, C.A.; Ventetuolo, C.E.; Poor, H.D. Pulmonary Vascular Dilatation Detected by Automated Transcranial Doppler in COVID-19 Pneumonia. Am. J. Respir. Crit Care Med. 2020, 202, 1037–1039. [Google Scholar] [CrossRef]
- Von der Thüsen, J.H.; Ghariq, E.; Overbeek, M.J.; Leyten, E.; Drijkoningen, T.; Gietema, H.A.; Prokop, M.; Quarles van Ufford, H.M.E. Spectrum of Vascular Involvement in Coronavirus Disease 2019 Pneumonia-Findings on CT Perfusion. Crit. Care Explor. 2020, 2, e0266. [Google Scholar] [CrossRef]
- Narasimhan, B.; Lorente-Ros, M.; Aguilar-Gallardo, J.S.; Lizardo, C.P.; Narasimhan, H.; Morton, C.; Donahue, K.R.; Aronow, W.S. Anticoagulation in COVID-19: A review of current literature and guidelines. Hosp. Pract. 2021, 49, 307–324. [Google Scholar] [CrossRef]
- Deshpande, C. Thromboembolic Findings in COVID-19 Autopsies: Pulmonary Thrombosis or Embolism? Ann. Intern Med. 2020, 173, 394–395. [Google Scholar] [CrossRef]
- Jorda, A.; Siller-Matula, J.M.; Zeitlinger, M.; Jilma, B.; Gelbenegger, G. Anticoagulant treatment regimens in patients with COVID-19: A meta-analysis. Clin. Pharmacol. Ther. 2021, 111, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, H.; Townsend, L.; Ni Cheallaigh, C.; Bergin, C.; Martin-Loeches, I.; Browne, P.; Bacon, C.L.; Gaule, R.; Gillett, A.; Byrne, M.; et al. COVID19 coagulopathy in Caucasian patients. Br. J. Haematol. 2020, 189, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Tal, S.; Spectre, G.; Kornowski, R.; Perl, L. Venous Thromboembolism Complicated with COVID-19: What Do We Know So Far? Acta Haematol 2020, 143, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Tang, R.; Chen, H.; Huang, Y.; Yi, S.; Bai, Q.; Zhu, Y.; Hong, C.; Liu, C.; Zhang, N.; et al. Pulmonary Vasculature: A Target for COVID-19. Am. J. Respir. Crit Care Med. 2021, 203, 260–261. [Google Scholar] [CrossRef]
- Lang, M.; Som, A.; Carey, D.; Reid, N.; Mendoza, D.P.; Flores, E.J.; Li, M.D.; Shepard, J.O.; Little, B.P. Pulmonary Vascular Manifestations of COVID-19 Pneumonia. Radiol. Cardiothorac. Imaging 2020, 2, e200277. [Google Scholar] [CrossRef]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.J.; Martin, I.B.K.; et al. The Role of Chest Imaging in Patient Management during the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Radiology 2020, 296, 172–180. [Google Scholar] [CrossRef] [Green Version]
- Si-Mohamed, S.; Chebib, N.; Sigovan, M.; Zumbihl, L.; Turquier, S.; Boccalini, S.; Boussel, L.; Mornex, J.F.; Cottin, V.; Douek, P. In vivo demonstration of pulmonary microvascular involvement in COVID-19 using dual-energy computed tomography. Eur. Respir. J. 2020, 56, 2002608. [Google Scholar] [CrossRef]
- Lv, H.; Chen, T.; Pan, Y.; Wang, H.; Chen, L.; Lu, Y. Pulmonary vascular enlargement on thoracic CT for diagnosis and differential diagnosis of COVID-19: A systematic review and meta-analysis. Ann. Transl. Med. 2020, 8, 878. [Google Scholar] [CrossRef]
- Qanadli, S.D.; Sauter, A.W.; Alkadhi, H.; Christe, A.; Poletti, P.A.; Ebner, L.; Rotzinger, D.C. Vascular Abnormalities Detected with Chest CT in COVID-19: Spectrum, Association with Parenchymal Lesions, Cardiac Changes, and Correlation with Clinical Severity (COVID-CAVA Study). Diagnostics 2021, 11, 606. [Google Scholar] [CrossRef]
- Rotzinger, D.C.; Knebel, J.F.; Jouannic, A.M.; Adler, G.; Qanadli, S.D. CT Pulmonary Angiography for Risk Stratification of Patients with Nonmassive Acute Pulmonary Embolism. Radiol. Cardiothorac. Imaging 2020, 2, e190188. [Google Scholar] [CrossRef]
- Elmokadem, A.H.; Mounir, A.M.; Ramadan, Z.A.; Elsedeiq, M.; Saleh, G.A. Comparison of chest CT severity scoring systems for COVID-19. Eur. Radiol. 2022, 32, 3501–3512. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Li, X.; Liu, H.; Zhen, Y.; Zhang, X.; Xiong, Q.; Luo, Y.; Gao, C.; Zeng, W. Chest CT Severity Score: An Imaging Tool for Assessing Severe COVID-19. Radiol. Cardiothorac. Imaging 2020, 2, e200047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, L.; Wang, J.G.; Liu, M.; Guo, X.J.; Guo, Y.L.; Zhai, X.H.; Guo, Y.M.; Wang, C. Anatomic distribution of embolus at CT pulmonary angiography in patients suspected acute pulmonary embolism. Zhonghua Jie He He Hu Xi Za Zhi 2012, 35, 833–836. [Google Scholar] [PubMed]
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology 2020, 77, 198–209. [Google Scholar] [CrossRef]
- Li, Y.; Xia, L. Coronavirus Disease 2019 (COVID-19): Role of Chest CT in Diagnosis and Management. AJR Am. J. Roentgenol. 2020, 214, 1280–1286. [Google Scholar] [CrossRef]
- Zhao, W.; Zhong, Z.; Xie, X.; Yu, Q.; Liu, J. Relation Between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. AJR Am. J. Roentgenol. 2020, 214, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Tekcan Şanlı, D.E.; Yıldırım, D. A new imaging sign in COVID-19 pneumonia: Vascular changes and their correlation with clinical severity of the disease. Diagn. Interv. Radiol. 2021, 27, 172–180. [Google Scholar] [CrossRef]
- Zhou, S.; Wang, Y.; Zhu, T.; Xia, L. CT Features of Coronavirus Disease 2019 (COVID-19) Pneumonia in 62 Patients in Wuhan, China. AJR Am. J. Roentgenol. 2020, 214, 1287–1294. [Google Scholar] [CrossRef]
- Henkel, M.; Weikert, T.; Marston, K.; Schwab, N.; Sommer, G.; Haslbauer, J.; Franzeck, F.; Anastasopoulos, C.; Stieltjes, B.; Michel, A.; et al. Lethal COVID-19: Radiologic-Pathologic Correlation of the Lungs. Radiol. Cardiothorac. Imaging 2020, 2, e200406. [Google Scholar] [CrossRef]
- Piciucchi, S.; Ravaglia, C.; Vizzuso, A.; Bertocco, M.; Poletti, V. Reversibility of venous dilatation and parenchymal changes density in SARS-CoV-2 pneumonia: Toward the definition of a peculiar pattern. Pulmonology 2021, 27, 353–357. [Google Scholar] [CrossRef]
- Aoki, R.; Iwasawa, T.; Hagiwara, E.; Komatsu, S.; Utsunomiya, D.; Ogura, T. Pulmonary vascular enlargement and lesion extent on computed tomography are correlated with COVID-19 disease severity. Jpn. J. Radiol. 2021, 39, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Garg, M.; Gupta, P.; Maralakunte, M.; Kumar, M.P.; Sinha, A.; Kang, M.; Agarwal, R.; Sandhu, M.S. Diagnostic accuracy of CT and radiographic findings for novel coronavirus 2019 pneumonia: Systematic review and meta-analysis. Clin. Imaging 2021, 72, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Loffi, M.; Regazzoni, V.; Toselli, M.; Cereda, A.; Palmisano, A.; Vignale, D.; Moroni, F.; Pontone, G.; Andreini, D.; Mancini, E.M.; et al. Incidence and characterization of acute pulmonary embolism in patients with SARS-CoV-2 pneumonia: A multicenter Italian experience. PLoS ONE 2021, 16, e0245565. [Google Scholar] [CrossRef]
- Masselli, G.; Almberger, M.; Tortora, A.; Capoccia, L.; Dolciami, M.; D’Aprile, M.R.; Valentini, C.; Avventurieri, G.; Bracci, S.; Ricci, P. Role of CT angiography in detecting acute pulmonary embolism associated with COVID-19 pneumonia. Radiol. Med. 2021, 126, 1553–1560. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Coppola, S.; Cressoni, M.; Busana, M.; Rossi, S.; Chiumello, D. COVID-19 Does Not Lead to a "Typical" Acute Respiratory Distress Syndrome. Am. J. Respir. Crit Care Med. 2020, 201, 1299–1300. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, M.; Kanno, H.; Zhou, Y.; Xiao, T.H.; Suzuki, T.; Ibayashi, Y.; Harmon, J.; Takizawa, S.; Hiramatsu, K.; Nitta, N.; et al. Massive image-based single-cell profiling reveals high levels of circulating platelet aggregates in patients with COVID-19. Nat. Commun. 2021, 12, 7135. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Patients (n = 61) |
|---|---|
| Mean age ± SD (y) | 61.7 ± 14.2 |
| Sex, n (%) | |
| Male | 44 (72) |
| Female | 17 (28) |
| Comorbidities, n (%) 1 | |
| Heart failure | 2 (4) |
| Hypertension | 13 (27) |
| Obesity | 5 (10) |
| Diabetes | 4 (8) |
| History of PE | 2 (4) |
| History of malignancy | 3 (6) |
| Laboratory mean, ± SD | |
| D-Dimer (ng/mL) 2 | 8516 ± 11175 |
| Troponin (μg/L) 3 | 46 ± 94 |
| PaO2 (mmHg) 4 | 70 ± 29 |
| CRP (mg/L) 5 | 150 ± 113 |
| Type of care, n (%) 1 | |
| Ambulatory | 3 (6) |
| Conventional care | 14(29) |
| Critical care (ICU) | 32 (65) |
| Invasive mechanical ventilation | 24 (49) |
| Anticoagulationthromboprophylaxis, n (%) 6 | 14 (32) |
| Death, n (%) 1 | 4 (8) |
| Anatomical Level | Number of Emboli |
|---|---|
| Troncular | 23 (6%) |
| Lobar | 59 (14%) |
| Segmental/sub-segmental | 329 (80%) |
| * Upper lobes | 65 (16%) |
| # Middle lobe/Lingula | 34 (8%) |
| ° Lower lobes | 230 (56%) |
| Emboli/Segments | VC + | VC − | Total |
|---|---|---|---|
| No AO | 5/34 (15%) | 46/200 (23%) | 51/234 (21.8%) |
| AO < 50% | 115/413 (28%) | 24/100 (24%) | 139/513 (27.1%) |
| AO > 50% | 134/449 (30%) | 5/24 (21%) | 139/473 (29.4%) |
| Total | 254/896 (28.3%) | 75/324 (23.1%) | 329/1220 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nevesny, F.; Rotzinger, D.C.; Sauter, A.W.; Loebelenz, L.I.; Schmuelling, L.; Alkadhi, H.; Ebner, L.; Christe, A.; Platon, A.; Poletti, P.-A.; et al. Acute Pulmonary Embolism in COVID-19: A Potential Connection between Venous Congestion and Thrombus Distribution. Biomedicines 2022, 10, 1300. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061300
Nevesny F, Rotzinger DC, Sauter AW, Loebelenz LI, Schmuelling L, Alkadhi H, Ebner L, Christe A, Platon A, Poletti P-A, et al. Acute Pulmonary Embolism in COVID-19: A Potential Connection between Venous Congestion and Thrombus Distribution. Biomedicines. 2022; 10(6):1300. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061300
Chicago/Turabian StyleNevesny, Franck, David C. Rotzinger, Alexander W. Sauter, Laura I. Loebelenz, Lena Schmuelling, Hatem Alkadhi, Lukas Ebner, Andreas Christe, Alexandra Platon, Pierre-Alexandre Poletti, and et al. 2022. "Acute Pulmonary Embolism in COVID-19: A Potential Connection between Venous Congestion and Thrombus Distribution" Biomedicines 10, no. 6: 1300. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061300