
Air Pollution: A Silent Key Driver of Dementia

1
Military Institute of Hygiene and Epidemiology, 01-163 Warsaw, Poland
2
Department of Experimental and Clinical Pharmacology, Centre for Preclinical Research (CBP), Medical University of Warsaw, 02-097 Warsaw, Poland
3
Department of Experimental Pharmacology, Mossakowski Medical Research Institute, Polish Academy of Sciences, 5 Pawinskiego Str., 02-106 Warsaw, Poland
4
Maria Sklodowska-Curie, Medical Academy in Warsaw, Solidarnosci 12 Str., 03-411 Warsaw, Poland
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Biomedicines 2023, 11(5), 1477; https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines11051477
Submission received: 27 April 2023
/
Revised: 13 May 2023
/
Accepted: 16 May 2023
/
Published: 18 May 2023
(This article belongs to the Special Issue Feature Reviews in Neurodegenerative Diseases and Environmental Factors)
Abstract
:In 2017, the Lancet Commission on Dementia Prevention, Intervention, and Care included air pollution in its list of potential risk factors for dementia; in 2018, the Lancet Commission on Pollution concluded that the evidence for a causal relationship between fine particulate matter (PM) and dementia is encouraging. However, few interventions exist to delay or prevent the onset of dementia. Air quality data are becoming increasingly available, and the science underlying the associated health effects is also evolving rapidly. Recent interest in this area has led to the publication of population-based cohort studies, but these studies have used different approaches to identify cases of dementia. The purpose of this article is to review recent evidence describing the association between exposure to air pollution and dementia with special emphasis on fine particulate matter of 2.5 microns or less. We also summarize here the proposed detailed mechanisms by which air pollutants reach the brain and activate the innate immune response. In addition, the article also provides a short overview of existing limitations in the treatment of dementia.
1. Introduction
Dementia, and the cognitive impairment that precedes it, is a common multifactorial disease with no singular cause, and its likelihood of occurrence increases with age. The globally aging population means that the absolute numbers of those living with dementia continue to increase with an estimated new case every three seconds [1].
There are currently more than 57 million people worldwide living with dementia, and it is one of the biggest global public health and social care challenges that people face now and will continue to face in the future [2]. By 2050, it is estimated that this number will rise to 131.5 million. Dementia also has a huge economic impact. It is estimated that the total global cost of dementia will reach USD 2 trillion by 2030 [1]. The fact that dementia is being diagnosed at an increasingly young age seems alarming. According to a new report by the Blue Cross Blue Shield Association (BCBSA), the number of commercially insured Americans between the ages of 30 and 64 diagnosed with early-onset dementia or Alzheimer’s disease (AD) jumped 200% from 2013 to 2017, from 4.2 to 12.6 per 10,000 [3].
There are several types of dementia, the most common of which is AD, a progressive neurodegenerative disorder that accounts for 60% to 80% of all dementia cases [4]. The key processes underlying AD include the accumulation of amyloid beta peptides into plaques, the formation of neurofibrillary tangles containing the tau protein, and neuronal degeneration. Other types of dementia include vascular dementia, dementia with Lewy bodies, dementia in Parkinson’s disease (PD), frontotemporal dementia (FTD), dementia in Huntington’s disease, and dementia in Creutzfeldt–Jakob disease [5]. Although each of these types is different, there are some standard features including the loss of basic brain features and capabilities. All types of dementia cause significantly impaired intellectual functioning. People with dementia lose their ability to solve problems, have an impaired ability to think abstractly and to plan and maintain emotional control, and may experience personality changes and behavioral problems such as agitation, delusions, and hallucinations. Over time, patients develop a severe phase, become totally dependent on their caregivers, and eventually die. Advances in understanding the role of the immune system, inflammation, and synapse degradation in dementia neuropathology are contributing to broad approaches to drug discovery and bringing hope for a clinical breakthrough in the causal treatment of neurodegenerative disease.
There are a huge number of potential risk factors for the development of dementia, including modifiable risk factors such as lifestyle, occupation, diabetes, physical inactivity, smoking, and obesity with a special place for genetic background (i.e., APOE4 gene variant, APP, and PSEN1/2 gene mutations) [6,7,8,9,10,11,12,13]. There are also plausible links between exposure to certain air pollutants and dementia.
2. Current and Future Pharmacological Treatment Options for Dementia
Developing treatments for dementia is a challenge. The main drugs available for symptomatic treatment have only minimal and transient efficacy (Figure 1). None of them have been shown to slow the progression of the disease, and all carry the risk of life-threatening side effects and numerous interactions with other drugs [14,15,16,17]. The cholinesterase inhibitors donepezil, galantamine, and rivastigmine can cause side effects, including sometimes severe vomiting; cardiac symptoms, such as arrhythmia and conduction disturbances; bradycardia; collapse; and syncope. In addition, donepezil can cause compulsive sexual behavior [18,19]. Memantine, an NMDA glutamate receptor antagonist, can cause neuropsychiatric symptoms such as hallucinations and confusion, sometimes leading to violent behavior, seizures, psychotic disorders, and heart failure or bradyarrhythmia [20]. Nevertheless, until recently, AD treatment research has focused almost exclusively on amyloid plaques. A new category, aducanumab, which is an anti-amyloid-beta (Aβ) monoclonal antibody, received accelerated approval from the FDA in June 2021, a decision that marks the first approval of a new drug for AD since 2003. Aducanumab appears to have limited evidence for clinical benefit, pending the results of an ongoing Phase 4 trial. The newly registered drug is ineffective in treating individuals with advanced disease and seems to work better as a preventative treatment for people with mild cognitive impairment or mild stages of dementia (Figure 1). It is supposed to remove Aβ plaques that accumulate in the brain, although removing the plaques does not appear to dramatically slow the progression of the disease [21,22,23,24].
Lecanemab is the second Aβ monoclonal antibody approved in January 2023 by the FDA under the accelerated approval pathway for the treatment of mild cognitive impairment or mild stages of dementia.
Thus, current Aβ antibody-based immunotherapies have an inherent risk of causing more harm than good due to the inflammatory side effects of amyloid-related imaging abnormalities (ARIA) and have numerous limitations, including the high cost of treatment. Aβ monoclonal antibodies may carry the risk of causing amyloid-related edema (ARIA-E) or hemosiderin deposition-related microhemorrhage (ARIA-H), which are known to occur with antibodies. ARIA most often manifests as temporary swelling and may be accompanied by small spots of bleeding in or on the brain, although serious and life-threatening events are rare [25]. Patients may experience symptoms such as headache, confusion, dizziness, vision changes, nausea, and seizures. Remarkably, in clinical trials, aducanumab was associated with encephalitis and bleeding in one-third of those who received the FDA-approved dose. Two patients in the treatment arm of the lecanemab clinical trials died from the side effect of strokes leading to brain hemorrhages [26]. In addition, warnings about lecanemab include a risk of infusion-related reactions, with flu-like symptoms, nausea, vomiting, and changes in blood pressure [27]. There remains an unmet need for other safe disease-modifying therapies for AD due to all the controversy surrounding the approval of aducanumab and the significant risks and limitations for both antibodies.
Given that the dysbiosis of the gut microbiota and the abnormal increase in intestinal flora metabolites can cause inflammation, the first marine-derived oligosaccharide to recondition the gut microbiota, oligomannate (GV-971), was approved in China in 2020 for mild-to-moderate AD (Figure 1). This oral drug reduces amyloid protein deposition and tau hyperphosphorylation via the peripheral and central modulation of dysbiosis-related inflammation, reducing the contribution of altered peripheral immunity to AD pathogenesis. GV-971 was also found to be safe and well tolerated without side effects typical of Aβ monoclonal antibodies [28,29]. Marketing applications in selected countries are planned. A multicenter global Phase III clinical trial (GREEN MEMORY) with sites in the USA, Europe, and Asia was conducted to support the global regulatory filing of oligomannate. Recently, GV-971 was given the green light from the FDA and has entered Phase III, with an expected registration date in other countries in 2025.
Gene therapy using neurotrophins called nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF), which support the survival of existing neurons and promote the growth and differentiation of new neurons and synapses, may be the future method for treating AD. Animal trials from 2001–2012 using AAV2 and NGF have provided promising features in this regard [30]. The main drawback of such neurotrophins is their limited crossing of the blood–brain barrier; thus, researchers have resorted to gene therapy, in which a modified adeno-associated virus (AAV2) more efficiently delivers and distributes the protein gene to key structures in dementia (entorhinal cortex and hippocampus). Based on the ongoing first-in-human Phase I clinical trial with AAV2-BDNF, this gene therapy represents an advancement over previous studies with NGF completed in 2010 [31]; thus, it appears to be a more potent growth factor than NGF for the neuronal circuits that are affected in AD the earliest [32]. It should be noted that BDNF injections must be precisely controlled to avoid side effects as freely circulating BDNF can cause seizures. The estimated completion date of the study is scheduled for the end of 2027.
Another ongoing Phase 2 study aims to evaluate the safety and toxicity of AAV gene transfer vector expressing the cDNA coding for human APOE2 (AAVrh.10hAPOE2) (LX1001) for the treatment of patients who are APOE4 homozygotes with mild cognitive impairment due to AD, and mild dementia [33]. Direct intrathecal administration of LX1001 to the CNS of these AD patients will lead to the conversion of APOE protein isoforms in the CSF of APOE4 homozygotes from APOE4 to APOE2-APOE4. The estimated completion date of the study is expected soon at the end of 2024.
It should be noted that there are currently no therapies that can effectively act on tau, so a gene-silencing drug is urgently needed to slow down—and perhaps even reverse—the course of Alzheimer’s disease and other diseases caused by tau accumulation. A significant step forward in this field is an ongoing world-first Phase I clinical trial published in Nature Medicine—with results from 46 patients—testing the safety of a drug called BIIB080 (/IONIS-MAPTRx), which is an antisense oligonucleotide (used to stop RNA producing the protein), to “silence” the gene encoding the tau protein, known as the tau microtubule-associated protein (MAPT) gene [34,35]. This prevents the gene from being translated into a protein in a dose–response and reversible manner. It also lowers the production of this protein and alters the course of the disease. The study looked at three doses of the drug, administered by intrathecal injection (injection into the nervous system via the spinal canal), compared to placebo. No serious adverse events occurred in patients who received the drug. The study found a greater than 50% reduction in CNS levels of total tau and tau phosphorus after 24 weeks in the two treatment groups that received the highest dose of the drug. There is a need for further studies evaluating the drug in older and larger groups of subjects and in more diverse populations. The estimated completion date of the study is scheduled for the end of 2026.
In summary, drug development for AD faces challenges due to an incomplete understanding of the disease’s pathological mechanisms. Focusing solely on amyloids was simply a case of tunnel vision. Combination therapies targeting multiple pathological alterations would likely be more effective than single-target anti-amyloid therapies currently approved on the market.
3. The Non-Pharmacological Treatment Options for Dementia
Given that the medications still have strong limitations, non-pharmacological interventions (i.e., reassurance, increased activities, etc.) are commonly proposed, which are mainly aimed at improving patients’ cognitive function and learning to cope with psychological and behavioral symptoms of dementia such as depression, delusions, aggression, and others [36]. These activities can, in turn, significantly improve the quality of life and well-being of people living with dementia, including their families [37]. Based on suggestions made by Cammusuli et al. [37], these interventions can be divided into the following groups: (i) holistic techniques, (ii) primary psychotherapy, (iii) cognitive methods, and (iv) alternative methods. Holistic approaches have continuously been shown to benefit both dementia patients and their caregivers. Similarly, the aforementioned cognitive training, cognitive stimulation, and combinations of these interventions have been suggested to positively affect cognitive function in patients with dementia [38,39,40]. Aerobic and resistance exercises are great examples of activities that have beneficial effects on cognition [41]. However, some studies have shown it to be moderate and limited to a specific activity (e.g., dance, Tai Chi, cycling, and stretching), while others have found no significant differences between experimental and control groups [42,43,44].
Therefore, while both pharmacological and non-pharmacological treatments remain a challenge, it is better to prevent dementia than to treat the already existing disease. Before embarking on preventive strategies, however, it is important to consider the knowledge of factors that can either induce or increase the risk of dementia development.
4. Environmental Risk Factors for Dementia
The world is undergoing constant change, which is mainly observed in global climate change as a response to several elements, such as solar radiation and an increase in solar input to the earth, the burning of fossil fuels, electromagnetic fields, and others. As a result of human activity and the rapid development of industry and transportation, several pollutants are generated, including those that pollute the aquatic ecosystem, which, paradoxically, can threaten human health and life in the long term. Indeed, all these factors, referred to as environmental factors, have been found to play a major role in the risk of dementia development and progression [45].
For instance, the presence of various toxic heavy metals and other chemical elements can be detected during water quality analysis. These include aluminum, cobalt, iron, lead, iron, zinc, and copper. Each of these has been linked to the risk of dementia. Iron, for example, is known as an essential component for the efficient delivery of oxygen to every cell in the human body. However, excessive amounts of it can cause several undesirable pathways, including ferroptosis, defined as iron-dependent cell death driven by lipid peroxidation [46]. This process is now widely described as a risk factor for dementia associated with AD [46,47,48]. Moreover, the effect of iron-induced ferroptosis on the onset of cognitive impairment has been confirmed in various animal models [49,50,51]. In contrast, only one case–control study by Emard and colleagues on the role of cobalt in dementia has been suggested [52]. Importantly, this was true not only when cobalt is present in the environment but also when it is implanted in the body (such as in the case of a hip implant) [52,53]. Emard also revealed that several people living in areas with high concentrations of lead suffered from AD [52]. Most papers describe aluminum exposure as the major risk factor for dementia, however, studies show no association or conflicting results [54,55]. This discrepancy in results is related to the different forms of aluminum studied. Aluminum from drinking water accounts for only about 5% of total intake; thus, there is little work on this source of the element. In contrast, information on the role of aluminum present in cosmetics and personal care products is more extensive [56]. Nevertheless, the role of aluminum in the development of dementia is indisputable, especially given the work published in 2008 by Rondeau et al. [57]. Aluminum was shown to double the risk of dementia and triple the risk of AD in water drinkers, especially at a concentration above 0.1 mg/day. Another recently published study confirmed such a relationship as the aluminum residue was found in post-mortem brain samples of patients diagnosed with familial AD [58]. In addition, dialysis dementia, also known as dialysis encephalopathy syndrome (DES), has been characterized in patients with renal failure undergoing hemodialysis who used aluminum-containing tap water for dialysis fluids [59,60].
Air Pollutants
Air pollution is contamination that sometimes results from natural processes in the world (e.g., biological processes, volcanic eruptions, and the chemical weathering of rocks or forest fires), but it can also be the result of direct human activity (e.g., chemicals, refining, metallurgy, or the chemical conversion of fuels). Currently, air pollution is the largest environmental risk factor for multiple complex mental and physical diseases with serious economic consequences in the form of increased medical costs and reduced productivity. According to World Health Organization (WHO) estimates, air pollution causes 4.3 million deaths annually [61]. Notably, outdoor exposure to PM with an aerodynamic diameter <2.5 µm (PM2.5) is the fifth leading risk factor for mortality worldwide [62]. Major factors that have been linked to the disease include ozone (O3); components of tobacco smoke (i.e., benzene, toluene, and formaldehyde); the PM present in motor vehicle exhaust fumes, which contains various compositions of black carbon, SO42−, NH4+, and NO3− and metallic components (K, Ca, Zn, Fe, Al, and Mg), as well as nitrogen dioxide (NO2) and other oxides of nitrogen, carbon monoxide (CO), sulfur dioxide (SO2), or polycyclic aromatic hydrocarbons (PAH), such as phenanthrene, benzo (a)pyrene, benzo (b)fluoranthene, benzo (a)anthracene, fluorene, fluoranthene, pyrene, chrysene, benzo (k)fluoranthene, dibenzo (a,h)anthracene, indene (1,2,3-cd)pyrene, and benzo (ghi)perylene [63,64,65,66,67].
In 2017, the Lancet Commission on Dementia Prevention, Intervention, and Care included air pollution in its list of potential risk factors for dementia [68]; in 2018, the Lancet Commission on Pollution concluded that the evidence for a causal relationship between fine particulate matter and dementia is encouraging [69]. Currently, the most widespread human air pollution is PM, which is produced by so-called low emissions (i.e., any exhaust fumes entering the air at low altitudes). Particulate matter is a mixture of molecules for which harmful effects depend on the size of the particles [70]. In fact, three classes of PM can be distinguished: a particle with a diameter less than 10 µm (PM10), a particle with a diameter of less than 2.5 µm (PM2.5), and ultrafine particles (UFPs) with a diameter less than 0.1 µm (PM0.1) [70,71,72]. These are extremely fine particles: 2.5 μm, for example, is about one-thirtieth of the diameter of a human hair. It is known that the size and the fineness (dispersion) state of a particle have a key effect on its absorption mainly by the respiratory and gastrointestinal systems (Figure 2). While large particles settle in the nasopharynx and larynx, from where they can be easily removed, smaller particles, especially those below 5 µm, penetrate deeper into the body and accumulate in the lung bronchi; hence, they have easy access to the blood and have observed toxic effects [73] (Figure 2). However, the most health-damaging particles are even smaller. Given the above, PM0.1 is known to be responsible for inflammatory reactions in the airways, which can exacerbate the course of asthma or COPD (chronic pulmonary obstructive disease) [74]. In the case of PM, cytotoxicity is associated with increased levels of oxidative stress and the (neuro)inflammatory process [75,76,77]; however, each fraction may be characterized by its ability to induce its specific toxic effect [78,79].
The World Health Organization has estimated that more than four million deaths per year can be attributed to particles smaller than 2.5 μm in diameter [80]. The WHO offers guidelines (Air Quality Guidelines—AQG) for reducing the health effects of air pollution. Although the WHO AQGs state that annual average concentrations should not exceed 10 μg/m, almost ¾ of European countries still exceed the annual concentrations set by the WHO AQGs for PM2.5 pollution [81,82]. Boldo et al. found that in 23 European cities life expectancy at age 30 would increase from one month to more than two years if long-term exposure to PM2.5 levels were reduced to 15 μg/m [83].
5. Insights from Experimental and Clinical Studies
5.1. Animal Studies
With regard to dementia, recently, Herr and colleagues reported that PM, particularly UFPs, increased tau phosphorylation in the hippocampus and enhanced microglial activity in a genetic 3xTgAD mouse model [84]. Tau phosphorylation has also been observed in other studies describing toxicity induced by higher PM2.5 [85,86,87]. Interestingly, neuronal loss, a common pathological phenomenon of neurodegeneration, has been observed in brain areas both in adult animals exposed to PM2.5 and in offspring after prenatal exposure during pregnancy [88].
5.2. Clinical Studies
A prospective birth cohort study involving children found that black carbon was one of the PM components associated with cognitive decline, including memory impairment [89]. Consistently with these studies, Calderón-Garcidueñas [90] and other research groups [91,92] report that children who are chronically exposed to outdoor air pollution are characterized by early hallmarks of AD such as a significant increase in tau [92,93].
This seems significant considering the current Chinese diagnosis of the world’s youngest person with probable AD (age 19), who was found to have no genetic mutations [94]. Age currently remains the largest risk factor for AD, but this study aims to encourage more attention to exogenous, environmental risk factors for dementia of young onset.
Long-term PM exposure can also affect neurodevelopmental outcomes in children. However, it should be noted that most of the studies have been conducted in areas with a low level of PM. To the best of our knowledge, the NeuroSmog study will be the first to assess whether long-term outdoor exposure to PM affects brain structure, function, and connectivity in both healthy children (aged between 10 and 13 years) and those diagnosed with attention deficit hyperactivity disorder (ADHD) [95]. The study covers an area including 18 cities in Poland with the highest concentration of air pollution [95]. The planned use of an fMRI can provide detailed information on the functioning of neural systems with a particular focus on cognitive flexibility [96]. The authors hypothesized that children diagnosed with ADHD would be more vulnerable to increased exposure to air pollution. There is emerging evidence that greater exposure to air pollution is associated with an increased risk of dementia. Kioumourtzoglou et al. [97] found that exposure to PM2.5 increases the hospitalization of patients with AD. Similar findings were reported by Carey et al. [98] and in a newly published paper by Shi and colleagues [99], who provided information on the existing correlation between increased PM2.5 concentrations and higher levels of dementia. A large-scale cohort study that followed older adults for 10 years found that the risk of developing dementia associated with AD increases by nearly 140% as PM2.5 concentrations increase by 4.34 μg/m3 [100]. In contrast, Abolhasani et al. [101] found, based on 12 studies, that the risk of dementia increases by 3% for every 1 μg/m3 increase in PM2.5 concentrations. Similarly, three other cohort studies (NHS, WHIMS, and the Whitehall II longitudinal study) found a higher risk of cognitive decline associated with higher PM2.5 exposure [102,103,104]. In the NHS study, the rate of cognitive decline was significant in women with the highest level of PM2.5 exposure compared to the lowest level [104]. In one similar study, Cacciottolo et al. additionally noted a dose-dependent relationship between the apolipoprotein E4 (APOE4) allele and PM2.5, such that the smallest decline in cognitive function was in those with the lowest exposure and without an APOE4 allele [101]. Cleary et al. [105] also reported a dose–response relationship for the interaction between the presence of APOE4 and PM2.5 and and cognitive decline. Interestingly, Chen et al. [106] noted that the location of residence (near the road) appears to be another causal factor of cognitive decline. Based on their analysis, they analyzed the following parameters: a place of residence’s distance from the roadway, the level of both PM2.5 and NO2, and the risk of PD-related dementia. They found that living closer to a roadway was associated with an increased risk of PD-related dementia for all distance categories (1–100 m and 101–200 m) except for the distance of 201–300 m. In another population-based cohort study, the Betula Study, Oudin et al. [107] found an association between higher PM2.5 levels from traffic exhaust and incidence of dementia. Overall, these results showed a potential link to dementia and revealed PM as an agent with high toxicological potential in all age groups. It should be stated that there is no clear consensus as to what period of exposure is most informative for assessing the neurological effects of air pollution.
The results for nitric oxides, particularly NO and NO2, are inconclusive, and their involvement in dementia is not as proven as for PMs. For instance, one study found that NO is positively involved in learning and memory, while its inhibitors (i.e., L-arginine methyl analogs) have been linked to cognitive impairment in older adults [108,109]. On the other hand, some authors have suggested that elevated NO levels may result in abnormal protein modification and, thus, may be involved in the pathogenesis of some neurodegenerative diseases, including AD. Similarly, endothelial NO deficiency also leads to vascular endothelial dysfunction and cerebral hypoperfusion, which, in turn, may result in greater β-amyloid-induced damage [110,111,112,113]. Amyloids are self-aggregating proteins that can induce cellular dysfunction in patients at risk for neurodegenerative disorders. Nevertheless, a population-based retrospective cohort study of 1720 Taiwanese individuals exposed to various levels of NO2 between 1998 and 2010, found that increased NO2 exposure was associated with a higher risk of dementia in both sexes [114]. Moreover, a similar risk was widely observed in younger patients living in highly urbanized residential areas. In another cohort study, the authors reported that a higher risk of dementia was associated with a combination of air pollutants, such as NO2 and PM2.5 [115]. Abolhasani et al., in a systematic review and meta-analysis, suggested a nonsignificant association between dementia and nitrogen oxides, including NO2. This was mainly explained by the lack of a significant number of studies [101]. An interesting study was conducted by Wang and colleagues, who showed that improving air quality reduces the risk of dementia in older women [116,117].
Carbon monoxide is another important risk factor drawing attention. This poisonous gas, although non-irritating, is mainly found in car exhaust, but it is also in fumes produced by grills, heaters, or even fireplaces. Its main toxic effect is cerebral hypoxia and ischemia, as well as neurological defects, including dementia, parkinsonism, etc., which were observed in 10–30% of intoxicated patients [118,119,120,121]. In examining the potential link between dementia and CO, it has been suggested that the risk factor for dementia increases with age and the severity of intoxication [114,122]. Some studies have also reported a strong association between CO and dementia with additional noise exposure [123]. In fact, CO and noise co-intoxication were found to magnify the risk level. This was demonstrated by an increase in oxidative stress and ROS production. Another study showed a link between CO and dementia as CO was found to have the ability to induce APOE e4 (a genetic risk factor for dementia) in carriers of the gene with increased morbidity compared to non-carriers [124].
6. Mechanisms Leading to Dementia after Exposure to Air Pollution
The fine PM and UFPs of air pollution described above are particularly hazardous to health. Due to their small size, they can reach and deposit in both the respiratory tract, the lungs (Figure 2) and the gastrointestinal tract. From there, they can enter the blood vessels [125]. Munzel and colleagues [126] showed that PM2.5 can damage vascular endothelial cells and lead to vascular dysfunction. Interestingly, UFPs can enter the brain directly through the olfactory nerve; thus, the human nose may be a port for the entry of air pollutants into the brain [127,128,129] (Figure 3). The penetration of even a few particles into the brain parenchyma triggers several defensive phenomena, including the induction and activation of microglia and then astroglia cells, and leads to the development of inflammation (Figure 3). Microglia are reprogrammed to a heightened proinflammatory state (priming) to produce more cytokine and become deleterious. The toxic activation of microglia might lead to aberrant synapse elimination in older age, which is part of the pathway to dementia [130]. The over- and under-expression of pro- and anti-inflammatory cytokines alter the homeostasis of the central nervous system (CNS) and may contribute to progressive neuronal dysfunction [131]. Two recent studies in mice and rats showed that astrocyte function and mitochondrial activity in the cortex were severely impaired by PM, with greater effects observed with the exposure to smaller particle sizes [132,133].
Recently, a clear link has been shown between the presence of UFPs and damage to the neurovascular unit in various brain structures [134,135]. The neurovascular unit is a complex morphological and functional structure that includes neuronal (neurons and interneurons), vascular (endothelial cells and pericytes) and glial cells (astrocytes), the basal lamina, and components of the extracellular matrix. It is the smallest functional unit of the brain responsible for the integrity of the BBB and the regulation of cerebral blood flow, thus ensuring proper brain function [136]. Damage within the neurovascular unit is known to lead to inflammation and neurodegeneration. Additionally, the vascular effects and red blood cell damage caused by UFPs can lead to neuronal degeneration and the development of dementia by causing brain inflammation or thrombosis, among other conditions [137,138]. Remarkably, a robust link between PM2.5 and vascular dysfunction has been noted [128]. Particles of this size can cause damage to endothelial cells in the brain; thus, such pathways may promote various types of dementia [137]. Direct cellular damage caused by air pollutants is high as they induce oxidative stress in the cell and damage mitochondria (Figure 3). The latter increases the intensity and overload of autophagy and mitophagy processes. This can lead to fragmentation and the inability to remove damaged mitochondria, as well as the degeneration of synapses and whole neurons [139] (Figure 3). However, the main mechanism of cell damage by fine PM and UFPs is based on the induction of free radicals, which destroy cellular structures and lead to the development of neuroinflammation and protein aggregation [140] (Figure 3). Air pollutants also induce abnormal neovascularization and the excessive autophagy of nerve cells [140]. Different types of proteins can bind to the surface of UFP, which can help air pollutants enter the body’s cells and interact with cell organelles [141]. Inside the cell, the particle matter can damage cellular proteins, interfere with protein folding and assembly processes leading to the formation of abnormal protein deposits [142], and damage the endoplasmic reticulum necessary for protein production [143]. An additional problem is magnetic particles, which become highly concentrated in the cell’s endosomes. They exhibit strong magnetic interactions and are sensitive to external magnetic fields, which can lead to the strong heating of the particles [144]. Many data show a strong link between exposure to air pollution and the development of cardiovascular diseases and events such as myocardial infarctions, transient ischemic attacks, and strokes [145,146,147,148,149,150,151]. All these pathologies, if the patient survives, can lead to the induction or worsening of dementia.
Air pollution can also affect the gut microbiome [152]. A normal gut microbial flora has a beneficial effect on digestive processes and immune function and is important for the proper functioning of the entire body, including the brain [137,153,154,155]. Fine and ultrafine particles damage not only the gut microbiome but also the neurons that make up the enteric nervous system, and through the vague nerves causing toxic effects on the CNS [156,157].
Air pollution particles may also cause local damage to body organs, leading to inflammation and oxidative stress [156,157]. Such local and, especially, systemic inflammation and oxidative stress can, in turn, lead to the progression of neurodegenerative diseases and dementia [125] (Figure 3).
Selected air pollutants and their potential effects on dementia onset are summarized in Table 1.
7. Limitations
The review presented here does not provide the full context of air pollution and dementia due to the numerous limitations of the included studies listed below. First, for the current study, this is not a systematic review, due to methodological diversity in the assessment of air pollution exposure in the included articles, which made the data too inconsistent to be combined into a single metanalysis. The evidence from the toxicological studies in animal and cellular models is limited and inconclusive. While there are a growing number of neuroimaging studies on the effects of air pollution exposure on dementia in the brain, they remain elusive. Moreover, data on measures linking air pollution exposure to other forms of dementia, i.e., vascular and frontotemporal dementia, are too limited. In fact, there is only one study devoted to dementia associated with Parkinson’s disease [106]. Therefore, dementia related to Alzheimer’s disease was the focus of this review. In addition, the measure of cognitive decline used in the study’s methodology does not in itself necessarily indicate an ongoing degenerative process and dementia. In addition, some studies considered multiple pollutants at the same time; thus, this does not allow for a direct causal relationship between dementia risk and air pollution. Finally, the data are mainly from population-based cohort studies of low quality and reliability, and the risk of moderate bias means that the results obtained in this way should be interpreted with caution. There is a need for more high-quality data with a larger number of study groups.
8. Conclusions and Future Directions
The causality of dementia is multifactorial, but air pollution may be a modifiable key factor in increasing individual risk by accelerating age-related changes observed in the brain. The impact on the CNS is chronic, beginning in childhood, and the pathology can take time (years) to accumulate. Intensive global efforts to improve air quality, in the form of long-term policies to reduce air pollution, have been successful in many regions, but half of the world’s population is still exposed daily to particulate pollution above the recommended standards. Given the global scale of dementia, and an aging population, only the increased control of fine particulate emissions and the implementation of innovative public health initiatives can minimize this risk and prevent dementia from reaching epidemic status in the future.
There is an urgent need to characterize the link between the chronic exposure to air pollutants and the risk of developing dementia and its implications for public health worldwide. In addition, understanding the precise mechanisms by which PM affects the body’s organs will allow for the better treatment of patients who develop symptoms related to its exposure. More neuroimaging and molecular data are needed to determine the cellular event that triggers the pathological brain response.
Author Contributions
Conceptualization, M.Z. and P.K.; writing—original draft preparation, P.S., M.Z., D.S. and P.K.; writing—review and editing, M.Z. and P.K.; supervision, P.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.-C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015. The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends. Available online: https://www.alzint.org/u/WorldAlzheimerReport2015.pdf (accessed on 12 February 2023).
- GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Brooks, M. Concerning Jump in Dementia Diagnoses in Younger Americans. Available online: https://www.medscape.com/viewarticle/926297 (accessed on 12 February 2023).
- Cummings, J.; Lee, G.; Nahed, P.; Kambar, M.E.Z.N.; Zhong, K.; Fonseca, J.; Taghva, K. Alzheimer’s disease drug development pipeline: 2022. Alzheimers Dement. 2022, 8, e12295. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Török, N.; Vécsei, L. Novel pharmaceutical approaches in dementia. In NeuroPsychopharmacotherapy; Riederer, P., Laux, G., Nagatsu, T., Le, W., Riederer, C., Eds.; Springer: Cham, Switzerland, 2022. [Google Scholar] [CrossRef]
- Balogh, L.; Tanaka, M.; Török, N.; Vécsei, L.; Taguchi, S. Crosstalk between existential phenomenological psychotherapy and neurological sciences in mood and anxiety disorders. Biomedicines 2021, 9, 340. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Vécsei, L. Editorial of Special Issue ‘Dissecting Neurological and Neuropsychiatric Diseases: Neurodegeneration and Neuroprotection’. Int. J. Mol. Sci. 2022, 23, 6991. [Google Scholar] [CrossRef]
- Slomski, A. Obesity is now the top modifiable dementia risk factor in the US. JAMA 2022, 328, 10. [Google Scholar] [CrossRef]
- Licher, S.; Ahmad, S.; Karamujić-Čomić, H.; Voortman, T.; Leening, M.J.G.; Arfan Ikram, M.; Kamran Ikram, M. Genetic predisposition, modifiable-risk-factor profile and long-term dementia risk in the general population. Nat. Med 2019, 25, 1364–1369. [Google Scholar] [CrossRef]
- Paulson, H.L.; Igo, I. Genetics of dementia. Semin. Neurol. 2011, 31, 449–460. [Google Scholar] [CrossRef]
- Barnes, D.E.; Yaffe, K. The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurol. 2011, 10, 819–828. [Google Scholar] [CrossRef]
- Fenoglio, C.; Scarpini, E.; Serpente, M.; Galimberti, D. Role of genetics and epigenetics in the pathogenesis of Alzheimer’s disease and frontotemporal dementia. J. Alzheimers Dis. 2018, 62, 913–932. [Google Scholar] [CrossRef]
- Yamazaki, Y.; Zhao, N.; Caulfield, T.R.; Liu, C.C.; Bu, G. Apolipoprotein E and Alzheimer disease, pathobiology and targeting strategies. Nat. Rev. Neurosci. 2019, 15, 501–518. [Google Scholar] [CrossRef]
- Wang, H.; Yang, F.; Zhang, S.; Xin, R.; Sun, Y. Genetic and environmental factors in Alzheimer’s and Parkinson’s diseases and promising therapeutic intervention via fecal microbiota transplantation. NPJ Parkinsons Dis. 2021, 7, 70. [Google Scholar] [CrossRef]
- Gerlach, L.B.; Kales, H.C. Managing behavioral and psychological symptoms of dementia. Psychiatr. Clin. N. Am. 2018, 41, 127–139. [Google Scholar] [CrossRef]
- Katz, I.R.; Jeste, D.V.; Mintzer, J.E.; Clyde, C.; Napolitano, J.; Brecher, M. Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: A randomized, double-blind trial. Risperidone Study Group. J. Clin. Psychiatry 1999, 60, 107–115. [Google Scholar] [CrossRef]
- Schneider, L.S.; Pollock, V.E.; Lyness, S.A. A metaanalysis of controlled trials of neuroleptic treatment in dementia. J. Am. Geriatr. Soc. 1990, 38, 553–563. [Google Scholar] [CrossRef]
- Yury, C.A.; Fisher, J.E. Meta-analysis of the effectiveness of atypical antipsychotics for the treatment of behavioural problems in persons with dementia. Psychother. Psychosom. 2007, 76, 213–218. [Google Scholar] [CrossRef]
- Corey-Bloom, J.; Anand, R.; Veach, J. A randomized trial evaluating the efficacy and safety of ENA 713 (rivastigmine tartrate), a new acetylcholinesterase inhibitor, in patients with mild to moderately severe Alzheimer’s disease. Int. J. Geriatr. Psychopharmacol. 1998, 1, 55–65. [Google Scholar]
- Tanaka, M.; Bohár, Z.; Vécsei, L. Are kynurenines accomplices or principal villains in dementia? Maintenance of Kynurenine Metabolism. Molecules 2020, 25, 564. [Google Scholar] [CrossRef]
- Mehta, M.; Adem, A.; Sabbagh, M. New acetylcholinesterase inhibitors for Alzheimer’s disease. Int. J. Alzheimers Dis. 2012, 2012, 728983. [Google Scholar] [CrossRef]
- Barenholtz Levy, H. Accelerated approval of aducanumab: Where do we stand now? Ann. Pharmacother. 2021, 56, 736–739. [Google Scholar] [CrossRef]
- Sturchio, A.; Dwivedi, A.K.; Young, C.B.; Malm, T.; Marsili, L.; Sharma, J.S.; Mahajan, A.; Hill, E.J.; Andaloussi, S.E.; Poston, K.L.; et al. High cerebrospinal amyloid-β 42 is associated with normal cognition in individuals with brain amyloidosis. EClinicalMedicine 2021, 38, 100988. [Google Scholar] [CrossRef]
- Woloshin, S.; Kesselheim, A. What to know about the Alzheimer drug aducanumab (Aduhelm). JAMA Intern. Med. 2022, 182, 892. [Google Scholar] [CrossRef] [PubMed]
- Product Information. Aduhelm (Aducanumab). Biogen Idec Inc. 2021. Available online: https://investors.biogen.com/news-releases/news-release-details/fda-approves-updated-aduhelmtm-prescribing-information-emphasize (accessed on 26 February 2023).
- Piller, C. Second Death Linked to Potential Antibody Treatment for Alzheimer’s Disease. Available online: https://www.science.org/content/article/second-death-linked-potential-antibody-treatment-alzheimer-s-disease (accessed on 3 March 2023).
- The Lancet. Lecanemab for Alzheimer’s disease: Tempering hype and hope. Lancet 2022, 400, 1899. [Google Scholar] [CrossRef] [PubMed]
- Seo, D.O.; Boros, B.D.; Holtzman, D.M. The microbiome: A target for Alzheimer disease? Cell Res. 2019, 29, 779–780. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Sun, G.; Feng, T.; Zhang, J.; Huang, X.; Wang, T.; Xie, Z.; Chu, X.; Wang, H.; Chang, S.; et al. Sodium oligomannate therapeutically remodels gut microbiota and suppresses gut bacterial amino acids-shaped neuroinflammation to inhibit Alzheimer’s disease progression. Cell Res. 2019, 29, 787–803. [Google Scholar] [CrossRef]
- Berg-Weger, M.; Stewart, D.B. Non-pharmacological interventions for persons with dementia. Missouri Med. 2017, 114, 116–119. [Google Scholar]
- Nagahara, A.H.; Wilson, B.R.; Ivasyk, I.; Kovacs, I.; Rawalji, S.; Bringas, J.R.; Pivirotto, P.J.; Sebastian, W.S.; Samaranch, L.; Bankiewicz, K.S.; et al. MR-guided delivery of AAV2-BDNF into the entorhinal cortex of non-human primates. Gene Ther. 2018, 25, 104–114. [Google Scholar] [CrossRef]
- A Phase I, Dose-Escalating Study to Assess the Safety and Tolerability of CERE-110 [Adeno-Associated Virus (AAV)-Based Vector-Mediated Delivery of Beta-Nerve Growth Factor (NGF)] in Subjects with Mild to Moderate Alzheimer’s Disease. ClinicalTrials.gov Identifier: NCT00087789. Available online: https://clinicaltrials.gov/ct2/show/NCT00087789 (accessed on 9 May 2023).
- A Phase I Study to Assess the Safety, Tolerability and Preliminary Efficacy of AAV2-BDNF [Adeno-Associated Virus (AAV)-Based, Vector-Mediated Delivery of Human Brain Derived Neurotrophic Factor] in Subjects with Early Alzheimer’s Disease and Mild Cognitive Impairment. ClinicalTrials.gov Identifier: NCT05040217. Available online: https://www.clinicaltrials.gov/ct2/show/NCT05040217 (accessed on 9 May 2023).
- A 52-Week, Multicenter, Phase 1/2 Open-label Study to Evaluate the Safety of LX1001 in Participants with APOE4 Homozygote Alzheimer’s Disease. ClinicalTrials.gov Identifier: NCT03634007. Available online: https://clinicaltrials.gov/ct2/show/NCT03634007 (accessed on 9 May 2023).
- Mummery, C.J.; Borjesson-Hanson, A.; Blackburn, D.J.; Vijverberg, E.G.B.; De Deyn, P.P.; Ducharme, S.; Jonsson, M.; Schneider, A.; Rinne, J.O.; Ludolph, A.C.; et al. Tau-targeting antisense oligonucleotide MAPTRx in mild Alzheimer’s disease: A phase 1b, randomized, placebo-controlled trial. Nat. Med. 2023. [Google Scholar] [CrossRef]
- A Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study to Assess the Efficacy, Safety, and Tolerability of BIIB080 in Subjects with Mild Cognitive Impairment Due to Alzheimer’s Disease or Mild Alzheimer’s Disease Dementia ClinicalTrials.gov Identifier: NCT05399888. Available online: https://clinicaltrials.gov/ct2/show/NCT05399888 (accessed on 9 May 2023).
- Cammisuli, D.M.; Danit, S.; Bosinelli, F.; Cipriani, G. Non-pharmacological interventions for people with Alzheimer’s disease: A critical review of the scientific literature from the last ten years. Eur. Geriatr. Med. 2016, 7, 57–64. [Google Scholar] [CrossRef]
- Liang, J.H.; Lin, L.; Wang, Y.Q.; Jia, R.X.; Qu, X.Y.; Li, J.; Li, J.Y.; Qian, S.; Qian, Y.X.; Wang, S.; et al. Non-pharmacological therapeutic strategy options for patients with dementia based on cognitive function-A Bayesian network meta-analysis of randomized controlled trials. Ageing Res. Rev. 2019, 56, 100965. [Google Scholar] [CrossRef]
- Liang, J.H.; Li, J.Y.; Jia, R.X.; Wang, Y.Q.; Wu, R.K.; Zhang, H.B.; Hang, L.; Xu, Y.; Pan, C.W. Comparison of cognitive intervention strategies for older adults with mild to moderate Alzheimer’s disease: A Bayesian meta-analytic review. J. Am. Med. Dir. Assoc. 2019, 20, 347–355. [Google Scholar] [CrossRef]
- Woods, B.; Aguirre, E.; Spector, A.E.; Orrell, M. Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst. Rev. 2012, 2, CD005562. [Google Scholar] [CrossRef]
- Antunes, H.K.; De Mello, M.T.; de Aquino Lemos, V.; Ferreira Santos-Galduroz, R.; Galdieri, L.C.; Bueno, O.F.A.; Tufik, S.; D’Almeida, V. Aerobic physical exercise improved the cognitive function of elderly males but did not modify their blood homocysteine levels. Dement. Geriatr. Cogn. Dis. Extra 2015, 5, 13–24. [Google Scholar] [CrossRef]
- Barnes, D.E.; Santos-Modesitt, W.; Poelke, G.; Kramer, A.F.; Castro, C.; Middleton, L.E.; Yaffe, K. The Mental Activity and eXercise (MAX) trial: A randomized controlled trial to enhance cognitive function in older adults. JAMA Intern. Med. 2013, 173, 797–804. [Google Scholar] [CrossRef]
- Toots, A.; Littbrand, H.; Boström, G.; Hörnsten, C.; Holmberg, H.; Lundin-Olsson, L.; Lindelöf, N.; Nordström, P.; Gustafson, Y.; Rosendahl, E. Effects of exercise on cognitive function in older people with dementia: A Randomized Controlled Trial. J. Alzheimers Dis. 2017, 60, 323–332. [Google Scholar] [CrossRef]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef]
- Sini, P.; Dang, T.B.C.; Fais, M.; Galioto, M.; Padedda, B.M.; Lugliè, A.; Iaccarino, C.; Crosio, C. Cyanobacteria, cyanotoxins, and neurodegenerative diseases: Dangerous liaisons. Int. J. Mol. Sci. 2021, 22, 8726. [Google Scholar] [CrossRef]
- Chen, K.; Jiang, X.; Wu, M.; Cao, X.; Bao, W.; Zhu, L.Q. Ferroptosis, a potential therapeutic target in Alzheimer’s disease. Front. Cell Dev. Biol. 2021, 9, 704298. [Google Scholar] [CrossRef]
- Gleason, A.; Bush, A.I. Iron and ferroptosis as therapeutic targets in Alzheimer’s disease. Neurotherapeutics 2021, 18, 252–264. [Google Scholar] [CrossRef]
- Masaldan, S.; Bush, A.I.; Devos, D.; Rolland, A.S.; Moreau, C. Striking while the iron is hot: Iron metabolism and ferroptosis in neurodegeneration. Free Radic. Biol. Med. 2019, 133, 221–233. [Google Scholar] [CrossRef]
- Ayton, S.; Faux, N.G.; Bush, A.I. Association of cerebrospinal fluid ferritin level with preclinical cognitive decline in APOE-epsilon4 carriers. JAMA Neurol. 2017, 74, 122–125. [Google Scholar] [CrossRef]
- Weiland, A.; Wang, Y.; Wu, W.; Lan, X.; Han, X.; Li, Q.; Wang, J. Ferroptosis and its role in diverse brain diseases. Mol. Neurobiol. 2018, 56, 4880–4893. [Google Scholar] [CrossRef] [PubMed]
- Yan, N.; Zhang, J.J. The emerging roles of ferroptosis in vascular cognitive impairment. Front. Neurosci. 2019, 13, 811. [Google Scholar] [CrossRef] [PubMed]
- Emard, J.F.; Andre, P.; Thouez, J.P.; Mathieu, J.; Boily, C.; Beaudry, M.; Cholette, A.; Robitaille, Y.; Bouchard, R.; Daoud, N.; et al. Geographical distribution of Alzheimer’s disease cases at birth and the geochemical profile of Saguenay-Lac-Saint-Jean Quebec, Canada (IMAGE Project). Water Air Soil Pollut. 1994, 72, 251–264. [Google Scholar] [CrossRef]
- Green, B.; Griffiths, E.; Almond, S. Neuropsychiatric symptoms following metal-on-metal implant failure with cobalt and chromium toxicity. BMC Psychiatry 2017, 17, 33. [Google Scholar] [CrossRef] [PubMed]
- Munoz, D.G. Is exposure to aluminum a risk factor for the development of Alzheimer’s disease? Arch. Neurol. 1998, 55, 737–739. [Google Scholar] [CrossRef]
- Tomljenovic, L. Aluminum and Alzheimer’s disease: After a century of controversy, is there a plausible link? J. Alzheimers Dis. 2011, 23, 567–598. [Google Scholar] [CrossRef]
- Sanajou, S.; Şahin, G.; Baydar, T. Aluminium in cosmetics and personal care products. J. Appl. Toxicol. 2021, 41, 1704–1718. [Google Scholar] [CrossRef]
- Rondeau, V.; Jacqmin-Gadda, H.; Commenges, D.; Helmer, C.; Dartigues, J.-F. Aluminum and silica in drinking water and the risk of Alzheimer’s disease or cognitive decline: Findings from 15-year follow-up of the PAQUID cohort. Am. J. Epidemiol. 2008, 169, 489–496. [Google Scholar] [CrossRef]
- Mold, M.J.; O’Farrell, A.; Morris, B.; Exley, C. Aluminum and Tau in neurofibrillary tangles in familial Alzheimer’s disease. J. Alzheimers Dis. Rep. 2021, 5, 283–294. [Google Scholar] [CrossRef]
- Rob, P.M.; Niederstadt, C.; Reusche, E. Dementia in patients undergoing long-term dialysis: Aetiology, differential diagnoses, epidemiology and management. CNS Drugs 2001, 15, 691–699. [Google Scholar] [CrossRef]
- Schreeder, M.T.; Favero, M.S.; Hughes, J.R.; Petersen, N.J.; Bennett, P.H.; Maynard, J.E. Dialysis encephalopathy and aluminium exposure: An epidemiologic analysis. J. Chronic Dis. 1983, 36, 581–593. [Google Scholar] [CrossRef]
- World Health Organization. Preventing Disease through Health Environments: A Global Assessment of the Burden of Disease from Environmental Risks; Prüss-Üstün, A., Wolf, J., Corvalán, C., Bos, R., Neira, M., Eds.; World Health Organization: Paris, France, 2016; Available online: https://www.who.int/publications/i/item/9789241565196 (accessed on 23 December 2021).
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of diseases study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Nitrogen Dioxide (NO2) Pollution. Available online: https://www.epa.gov/no2-pollution (accessed on 4 January 2023).
- Låg, M.; Øvrevik, J.; Refsnes, M.; Holme, J.A. Potential role of polycyclic aromatic hydrocarbons in air pollution-induced non-malignant respiratory diseases. Respir. Res. 2020, 21, 299. [Google Scholar] [CrossRef]
- Abdel-Shafy, H.I.; Mansour, M.S.M. A review on polycyclic aromatic hydrocarbons: Source, environmental impact, effect on human health and remediation. Egypt. J. Pet. 2016, 25, 107–123. [Google Scholar] [CrossRef]
- Cakmak, S.; Dales, R.; Kauri, L.M.; Mahmud, M.; Van Ryswyk, K.; Vanos, J.; Liu, L.; Kumarathasa, P.; Thomson, E.; Vincent, R.; et al. Metal composition of fine particulate air pollution and acute changes in cardiorespiratory physiology. Environ. Pollut. 2014, 189, 208–214. [Google Scholar] [CrossRef]
- Kunt, F.; Ayturan, Z.C.; Yumun, F.; Karagonen, I.; Semerci, M.; Akgun, M. Modeling and assessment of PM10 and atmospheric metal pollution in Kayseri Province, Turkey. Atmosphere 2023, 14, 356. [Google Scholar] [CrossRef]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Balde, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef]
- Choi, H.; Kim, S.H. Air pollution and dementia. Dement. Neurocogn. Disord. 2019, 18, 109–112. [Google Scholar] [CrossRef]
- de Jesus, A.L.; Rahmn, M.M.; Mazaheri, M.; Thompson, H.; Knibbs, L.D.; Jeong, C.; Evans, G.; Nei, W.; Ding, A.; Qiao, L.; et al. Ultrafine particles and PM2.5 in the air of cities around the world: Are they representative of each other? Environ. Int. 2019, 129, 118–135. [Google Scholar] [CrossRef]
- Kwon, H.S.; Ryu, M.H.; Carlsten, C. Ultrafine particles: Unique physicochemical properties relevant to health and disease. Exp. Mol. Med. 2020, 52, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Jurowski, K.; Madej, K.; Piekoszewski, W. An Outline of Food Toxicology; Krakowska Wyzsza Szkola Promocji Zdrowia: Krakow, Poland, 2016; ISBN 978-83-65545-03-9. [Google Scholar]
- Schraufnagel, D.E. The health effects of ultrafine particles. Exp. Mol. Med. 2020, 52, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.B.; Coburn, J.; Dao, K.; Roque, P.; Chang, Y.C.; Kalia, V.; Guilarte, T.R.; Dziedzic, J.; Costa, L.G. Sex and genetic differences in the effects of acute diesel exhaust exposure on inflammation and oxidative stress in mouse brain. Toxicology 2016, 374, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hajipour, S.; Farbood, Y.; Gharib-Naseri, M.K.; Goudarzi, G.; Rashno, M.; Maleki, H.; Bakhtiari, N.; Nesari, A.; Khoshnam, S.E.; Dianat, M.; et al. Exposure to ambient dusty particulate matter impairs spatial memory and hippocampal LTP by increasing brain inflammation and oxidative stress in rats. Life Sci. 2020, 242, 117210. [Google Scholar] [CrossRef]
- Lee, S.H.; Chen, Y.H.; Chien, C.C.; Yan, Y.H.; Chen, H.C.; Chuang, H.C.; Hsieh, H.I.; Cho, K.H.; Kuo, L.W.; Chou, C.C.; et al. Three month inhalation exposure to low-level PM2.5 induced brain toxicity in an Alzheimer’s disease mouse model. PLoS ONE 2021, 16, e0254587. [Google Scholar] [CrossRef]
- Ferin, J.; Oberdörster, G.; Penney, D.P. Pulmonary retention of ultrafine and fine particles in rats. Am. J. Respir. Cell Mol. Biol. 1992, 6, 535–542. [Google Scholar] [CrossRef]
- Lodovici, M.; Bigagli, E. Oxidative stress and air pollution exposure. J. Toxicol. 2011, 2011, 487074. [Google Scholar] [CrossRef]
- State of Global Air 2020; Special Report; Health Effects Institute: Boston, MA, USA, 2020. Available online: https://www.stateofglobalair.org/ (accessed on 4 January 2023).
- Juginović, A.; Vuković, M.; Aranza, I.; Biloš, V. Health impacts of air pollution exposure from 1990 to 2019 in 43 European countries. Sci. Rep. 2021, 11, 22516. [Google Scholar] [CrossRef]
- Krzyzanowski, M.; Cohen, A. Update of WHO air quality guidelines. Air Qual. Atmos. Health 2008, 1, 7–13. [Google Scholar] [CrossRef]
- Boldo, E.; Medina, S.; Letertre, A.; Hurley, F.; Mucke, H.G.; Ballester, F.; Aguilera, I.; Eilstein, D.; Aphesis Group. Apheis: Health impact assessment of long-term exposure to PM 2.5 in 23 European cities. Eur. J. Epidemiol. 2006, 21, 449–458. [Google Scholar] [CrossRef]
- Herr, D.; Jew, K.; Wong, C.; Kennell, A.; Gelein, R.; Chalupa, D.; Raab, A.; Oberdörster, G.; Olschowka, J.; O’Banion, M.K.; et al. Effects of concentrated ambient ultrafine particulate matter on hallmarks of Alzheimer’s disease in the 3xTgAD mouse model. Neurotoxicology 2021, 84, 172–183. [Google Scholar] [CrossRef]
- Chuang, H.-C.; Chen, H.-C.; Chai, P.-J.; Liao, H.-T.; Wu, C.-F.; Chen, C.-L.; Jhan, M.K.; Hsieh, H.I.; Wu, K.Y.; Chen, T.F.; et al. Neuropathology changed by 3- and 6-months low-level PM2.5 inhalation exposure in spontaneously hypertensive rats. Part. Fibre Toxicol. 2020, 17, 59. [Google Scholar] [CrossRef]
- Shih, C.-H.; Chen, J.-K.; Kuo, L.-W.; Cho, K.-H.; Hsiao, T.-C.; Lin, Z.-W.; Lin, Y.S.; Kang, J.H.; Lo, Y.C.; Chuang, K.J.; et al. Chronic pulmonary exposure to traffic-related fine particulate matter causes brain impairment in adult rats. Part. Fibre Toxicol. 2018, 15, 44. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wei, L.Y.; Ding, R.; Feng, Y.; Li, D.; Li, C.; Malko, P.; Mortadza, S.A.S.; Wu, W.; Yin, Y.; et al. Predisposition to Alzheimer’s and age-related brain pathologies by PM2.5 exposure: Perspective on the roles of oxidative stress and TRPM2 channel. Front. Physiol. 2020, 11, 155. [Google Scholar] [CrossRef]
- Zhang, T.; Zheng, X.; Wang, X.; Zhao, H.; Wang, T.; Zhang, H.; Li, W.; Shen, H.; Yu, L. Maternal exposure to PM(2.5) during pregnancy induces impaired development of cerebral cortex in mice offspring. Int. J. Mol. Sci. 2018, 19, 257. [Google Scholar] [CrossRef]
- Suglia, S.F.; Gryparis, A.; Wright, R.O.; Schwartz, J.; Wright, R.J. Association of black carbon with cognition among children in a prospective birth cohort study. Am. J. Epidemiol. 2008, 167, 280–286. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; Leray, E.; Heydarpour, P.; Torres-Jardón, R.; Reis, J. Air pollution, a rising environmental risk factor for cognition, neuroinflammation and neurodegeneration: The clinical impact on children and beyond. Rev. Neurol. 2016, 172, 69–80. [Google Scholar] [CrossRef]
- Braak, H.; Del Tredici, K. Where, when, and in what form does sporadic Alzheimer’s disease begin? Curr. Opin. Neurol. 2012, 25, 708–714. [Google Scholar] [CrossRef]
- Braak, H.; Thal, D.R.; Ghebremedhin, E.; Del Tredici, K. Stages of the pathologic process in Alzheimer disease: Age categories from 1 to 100 years. J. Neuropathol. Exp. Neurol. 2011, 70, 960–969. [Google Scholar] [CrossRef]
- Wang, J.Z.; Xia, Y.Y.; Grundke-Iqbal, I.; Iqbal, K. Abnormal hyperphosphorylation of tau: Sites, regulation, and molecular mechanism of neurofibrillary degeneration. J. Alzheimers Dis. 2013, 33 (Suppl. S1), S123–S139. [Google Scholar] [CrossRef]
- Jia, J.; Zhang, Y.; Shi, Y.; Yin, X.; Wang, S.; Li, Y.; Zhao, T.; Liu, W.; Zhou, A.; Jia, L. A 19-Year-Old adolescent with probable Alzheimer’s disease. J. Alzheimer Dis. 2023, 91, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Orlov, N.; Grellier, J.; Kaczmarek-Majer, K.; Lipowska, M.; Sitnik-Warchulska, K.; Mysak, Y.; Baumbach, C.; Wierzba-Łukaszyk, M.; Soomro, M.H.; et al. NeuroSmog: Determining the impact of air pollution on the developing brain: Project Protocol. Int. J. Environ. Res. Public Health 2022, 19, 310. [Google Scholar] [CrossRef] [PubMed]
- Nyatega, C.O.; Qiang, L.; Jajere, M.A.; Kawuwa, H.B. Atypical functional connectivity of limbic network in attention deficit/hyperactivity disorder. Clin. Schizophr. Relat. Psychoses 2022, 16, 1–16. [Google Scholar]
- Kioumourtzoglou, M.A.; Schwartz, J.D.; Weisskopf, M.G.; Melly, S.J.; Wang, Y.; Dominici, F.; Zanobetti, A. Long-term PM2.5 Exposure and Neurological Hospital Admissions in the Northeastern United States. Environ. Health Perspect. 2016, 124, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Carey, I.M.; Anderson, H.R.; Atkinson, R.W.; Beevers, S.D.; Cook, D.G.; Strachan, D.P.; Dajnak, D.; Gulliver, J.; Kelly, F.J. Are noise and air pollution related to the incidence of dementia? A cohort study in London, England. BMJ Open 2018, 8, e022404. [Google Scholar] [CrossRef]
- Shi, L.; Zhu, Q.; Wang, Y.; Liu, P. Incident dementia and long-term exposure to constituents of fine particle air pollution: A national cohort study in the United States. Proc. Natl. Acad. Sci. USA 2022, 120, e2211282119. [Google Scholar] [CrossRef]
- Jung, C.R.; Lin, Y.T.; Hwang, B.F. Ozone, particulate matter, and newly diagnosed Alzheimer’s disease: A population-based cohort study in Taiwan. J. Alzheimers Dis. 2015, 44, 573–584. [Google Scholar] [CrossRef]
- Abolhasani, E.; Hachinski, V.; Ghazaleh, N.; Azarpazhooh, M.R.; Mokhber, N.; Martin, J. Air pollution and incidence of dementia: A systematic review and meta-analysis. Neurology 2023, 100, e242–e254. [Google Scholar] [CrossRef]
- Cacciottolo, M.; Wang, X.; Driscoll, I.; Woodward, N.; Saffari, A.; Reyes, J.; Serre, M.L.; Vizuete, W.; Sioutas, C.; Morgan, T.E.; et al. Particulate air pollutants, APOE alleles and their contributions to cognitive impairment in older women and to amyloidogenesis in experimental models. Transl. Psychiatry 2017, 7, e1022. [Google Scholar] [CrossRef]
- Tonne, C.; Elbaz, A.; Beevers, S.; Singh-Manoux, A. Traffic-related air pollution in relation to cognitive function in older adults. Epidemiology 2014, 25, 674–681. [Google Scholar] [CrossRef]
- Weuve, J.; Puett, R.C.; Schwartz, J.; Yanosky, J.D.; Laden, F.; Grodstein, F. Exposure to particulate air pollution and cognitive decline in older women. Arch. Intern. Med. 2012, 172, 219–227. [Google Scholar] [CrossRef]
- Cleary, E.G.; Cifuentes, M.; Grinstein, G.; Brugge, D.; Shea, T.B. Association of low-level ozone with cognitive decline in older adults. J. Alzheimers Dis. 2018, 61, 67–78. [Google Scholar] [CrossRef]
- Chen, H.; Kwong, J.C.; Copes, R.; Tu, K.; Villeneuve, P.J.; van Donkelaar, A.; Hystad, P.; Martin, R.V.; Murray, B.J.; Jessiman, B.; et al. Living near major roads and the incidence of dementia, Parkinson’s disease, and multiple sclerosis: A population-based cohort study. Lancet 2017, 389, 718–726. [Google Scholar] [CrossRef]
- Oudin, A.; Segersson, D.; Adolfsson, R.; Forsberg, B. Association between air pollution from residential wood burning and dementia incidence in a longitudinal study in Northern Sweden. PLoS ONE 2018, 13, e0198283. [Google Scholar] [CrossRef]
- Asif, M.; Soiza, R.L.; McEvoy, M.; Mangoni, A.A. Asymmetric dimethylarginine: A possible link between vascular disease and dementia. Curr. Alzheimer Res. 2013, 10, 347–356. [Google Scholar] [CrossRef]
- Paul, V.; Ekambaram, P. Involvement of nitric oxide in learning & memory processes. Indian J. Med. Res. 2011, 133, 471–478. [Google Scholar]
- Daulatzai, M.A. Cerebral hypoperfusion and glucose hypometabolism: Key pathophysiological modulators promote neurodegeneration, cognitive impairment, and Alzheimer’s disease. J. Neurosci. Res. 2017, 95, 943–972. [Google Scholar] [CrossRef]
- Kelleher, R.J.; Soiza, R.L. Evidence of endothelial dysfunction in the development of Alzheimer’s disease: Is Alzheimer’s a vascular disorder? Am. J. Cardiovasc. Dis. 2013, 3, 197–226. [Google Scholar]
- Manukhina, E.B.; Pshennikova, M.G.; Goryacheva, A.V.; Khomenko, I.P.; Mashina, S.Y.; Pokidyshev, D.A.; Malyshev, I.Y. Role of nitric oxide in prevention of cognitive disorders in neurodegenerative brain injuries in rats. Bull. Exp. Biol. Med. 2008, 146, 391–395. [Google Scholar] [CrossRef]
- Toda, N.; Okamura, T. Cerebral blood flow regulation by nitric oxide in Alzheimer’s disease. J. Alzheimers Dis. 2012, 32, 569–578. [Google Scholar] [CrossRef]
- Chang, K.H.; Chang, M.Y.; Muo, C.H.; Wu, T.N.; Chen, C.Y.; Kao, C.H. Increased risk of dementia in patients exposed to nitrogen dioxide and carbon monoxide: A population-based retrospective cohort study. PLoS ONE 2014, 9, e103078. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Li, X.; Zhou, T.; Wang, M.; Heianza, Y.; Qi, L. Long-term exposure to low-level air pollution, genetic susceptibility and risk of dementia. Int. J. Epidemiol. 2022, dyac146. [Google Scholar] [CrossRef] [PubMed]
- Younan, D.; Wang, X.; Millstein, J.; Petkus, A.J.; Beavers, D.P.; Espeland, M.A.; Chui, H.C.; Resnick, S.M.; Gatz, M.; Kaufman, J.D.; et al. Air quality improvement and cognitive decline in community-dwelling older women in the United States: A longitudinal cohort study. PLoS Med. 2022, 19, e1003893. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Younan, D.; Millstein, J.; Petkus, A.J.; Garcia, E.; Beavers, D.P.; Espeland, M.A.; Chui, H.C.; Resnick, S.M.; Gatz, M.; et al. Association of improved air quality with lower dementia risk in older women. Proc. Natl. Acad. Sci. USA 2022, 119, e2107833119. [Google Scholar] [CrossRef] [PubMed]
- Hullmann, M.; Albrecht, C.; van Berlo, D.; Gerlofs_Nijland, M.E.; Wahle, T.; Boots, A.W.; Krutmann, J.; Cassee, F.R. Diesel engine exhaust accelerates plaque formation in a mouse model of Alzheimer’s disease. Part. Fibre Toxicol. 2017, 14, 35. [Google Scholar] [CrossRef]
- Kara, H.; Bayir, A.; Ak, A.; Degirmenci, S. Cerebrovascular ischaemia after carbon monoxide intoxication. Singap. Med. J. 2015, 56, e26–e28. [Google Scholar] [CrossRef]
- Sekiya, K.; Nishihara, T.; Abe, N.; Konishi, A.; Nandate, H.; Hamada, T.; Ikemune, K.; Takasaki, Y.; Tanaka, J.; Asano, M.; et al. Carbon monoxide poisoning-induced delayed encephalopathy accompanies decreased microglial cell numbers: Distinctive pathophysiological features from hypoxemia-induced brain damage. Brain Res. 2019, 1710, 22–32. [Google Scholar] [CrossRef]
- Webb, C.J., 2nd; Vaitkevicius, P.V. Dementia with a seasonal onset secondary to carbon monoxide poisoning. J. Am. Geriatr. Soc. 1997, 45, 1281–12822. [Google Scholar] [CrossRef]
- Lai, C.Y.; Huang, Y.W.; Tseng, C.H.; Lin, C.L.; Sung, F.C.; Kao, C.H. Patients with carbon monoxide poisoning and subsequent dementia: A Population-Based Cohort Study. Medicine 2016, 95, e2418. [Google Scholar] [CrossRef]
- Bagheri, F.; Rashedi, V. Simultaneous exposure to noise and carbon monoxide increases the risk of Alzheimer’s disease: A literature review. Med. Gas Res. 2020, 10, 85–90. [Google Scholar]
- Hopkins, R.O.; Weaver, L.K.; Valentine, K.J.; Mower, C.; Churchill, S.; Carlquist, J. Apolipoprotein E genotype and response of carbon monoxide poisoning to hyperbaric oxygen treatment. Am. J. Respir. Crit. Care Med. 2007, 176, 1001–1006. [Google Scholar] [CrossRef]
- Peters, A. Ambient air pollution and Alzheimer’s disease: The role of the composition of fine particles. Proc. Natl. Acad. Sci. USA 2023, 120, e2220028120. [Google Scholar] [CrossRef]
- Munzel, T.; Gori, T.; Al-Kindi, S.; Deadfield, J.; Leliveld, J.; Daiber, A.; Rajagopalan, S. Effects of gaseous and solid constituents of air pollution on endothelial function. Eur. Heart J. 2018, 39, 3543–3550. [Google Scholar] [CrossRef]
- Heusinkveld, H.J.; Wahle, T.; Campbell, A.; Westerink, R.H.S.; Tran, L.; Johnston, H.; Stone, V.; Cassee, F.R.; Schins, R.P.F. Neurodegenerative and neurological disorders by small inhaled particles. Neurotoxicol. 2016, 56, 94–106. [Google Scholar] [CrossRef]
- Peters, A.; Veronesi, B.; Calderon-Garciduenas, L.; Gehr, P.; Chen, L.C.; Geiser, M.; Reed, W.; Rothen-Rutishauser, B.; Schurch, S.; Schulz, H. Translocation and potential neurological effects of fine and ultrafine particles a critical update. Part. Fibre Toxicol. 2006, 3, 13. [Google Scholar] [CrossRef]
- Stone, V.; Miller, M.R.; Clift, M.J.D.; Elder, A.; Mills, N.L.; Moller, P.; Schins, R.P.F.; Vogel, U.; Kreyling, W.G.; Jensen, K.A.; et al. Nanomaterials versus ambient ultrafine particles: An opportunity to exchange toxicology knowledge. Environ. Health Perspect. 2017, 125, 106002. [Google Scholar] [CrossRef]
- Wilker, E.H.; Osman, M.; Weisskopf, M.G. Ambient air pollution and clinical dementia: Systematic review and meta-analysis. BMJ 2023, 381, e071620. [Google Scholar] [CrossRef]
- Nicholson, S.; Baccarelli, A.; Prada, D. Role of brain extracellular vesicles in air pollution-related cognitive impairment and neurodegeneration. Environ. Res. 2022, 204, 112316. [Google Scholar] [CrossRef]
- Araújo, J.E.; Jorge, S.; Santos, H.M.; Chiechi, A.; Galstyan, A.; Lodeiro, C.; Diniz, M.; Kleinman, M.T.; Ljubimova, J.Y.; Capelo, J.L. Proteomic changes driven by urban pollution suggest particulate matter as a deregulator of energy metabolism, mitochondrial activity, and oxidative pathways in the rat brain. Sci. Total Environ. 2019, 687, 839–848. [Google Scholar] [CrossRef]
- Di Domenico, M.; Benevenuto, S.G.D.M.; Tomasini, P.P.; Yariwake, V.Y.; Alves, N.D.O.; Rahmeier, F.L.; Fernandes, M.D.C.; Moura, D.J.; Saldiva, P.H.N.; Veras, M.M. Concentrated ambient fine particulate matter (PM2.5) exposure induce brain damage in pre and postnatal exposed mice. Neurotoxicology 2020, 79, 127–141. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; González-Maciel, A.; Reynoso-Robles, R.; Delgado-Chávez, R.; Mukherjee, P.S.; Kulesza, R.J.; Torres-Jardón, R.; Ávila-Ramírez, J.; Villarreal-Ríos, R. Hallmarks of Alzheimer disease are evolving relentlessly in Metropolitan Mexico City infants, children and young adults. APOE4 carriers have higher suicide risk and higher odds of reaching NFT stage V at ≤40 years of age. Environ. Res. 2018, 164, 475–487. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Garcidueñas, L.; González-Maciel, A.; Reynoso-Robles, R.; Silva-Pereyra, H.G.; Torres-Jardón, R.; Brito-Aguilar, R.; Ayala, A.; Stommel, E.W.; Delgado-Chavez, R. Environmentally toxic solid nanoparticles in noradrenergic and dopaminergic nuclei and cerebellum of metropolitan Mexico City children and young adults with neural quadruple misfolded protein pathologies and high exposures to nano particulate matter. Toxics 2022, 10, 164. [Google Scholar] [CrossRef] [PubMed]
- Iadecola, C. The neurovascular unit coming of age: A journey through neurovascular coupling in health and disease. Neuron 2017, 96, 17–42. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Garcidueñas, L.; Stommel, E.W.; Rajkumar, R.P.; Mukherjee, P.S.; Ayala, A. Particulate air pollution and risk of neuropsychiatric outcomes. What we breathe, swallow, and put on our skin matters. Int. J. Environ. Res. Public Health 2021, 18, 11568. [Google Scholar] [CrossRef] [PubMed]
- Pretini, V.; Koenen, M.H.; Kaestner, L.; Fens, M.H.A.M.; Schiffelers, R.M.; Bartels, M.; Van Wijk, R. Red blood cells: Chasing interactions. Front. Physiol. 2019, 10, 945. [Google Scholar] [CrossRef]
- Morton, H.; Kshirsagar, S.; Orlov, E.; Bunquin, L.E.; Sawant, N.; Boleng, L.; George, M.; Basu, T.; Ramasubramanian, B.; Pradeepkiran, J.A.; et al. Defective mitophagy and synaptic degeneration in Alzheimer’s disease: Focus on aging, mitochondria and synapse. Free Radic. Biol. Med. 2021, 172, 652–667. [Google Scholar] [CrossRef]
- Yarjanli, Z.; Ghaedi, K.; Esmaeili, A.; Rahgozar, S.; Zarrabi, A. Iron oxide nanoparticles may damage to the neural tissue through iron accumulation, oxidative stress, and protein aggregation. BMC Neurosci. 2017, 18, 51. [Google Scholar] [CrossRef]
- Parveen, R.; Shamsi, T.N.; Fatima, S. Nanoparticles-protein interaction: Role in protein aggregation and clinical implications. Int. J. Biol. Macromol. 2017, 94 Pt A, 386–395. [Google Scholar] [CrossRef]
- Hartl, F.U. Protein Misfolding Diseases. Annu. Rev. Biochem. 2017, 86, 21–26. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; González-Maciel, A.; Reynoso-Robles, R.; Hammond, J.; Kulesza, R.; Lachmann, I.; Torres-Jardón, R.; Mukherjee, P.S.; Maher, B.A. Quadruple abnormal protein aggregates in brainstem pathology and exogenous metal-rich magnetic nanoparticles (and engineered Ti-rich nanorods). The substantia nigrae is a very early target in young urbanites and the gastrointestinal tract a key brainstem portal. Environ. Res. 2020, 191, 110139. [Google Scholar]
- Gutiérrez, L.; de la Cueva, L.; Moros, M.; Mazarío, E.; de Bernardo, S.; de la Fuente, J.M.; Morales, M.P.; Salas, G. Aggregation effects on the magnetic properties of iron oxide colloids. Nanotechnology 2019, 30, 112001. [Google Scholar] [CrossRef]
- Boot, E.; Ekker, M.S.; Putaala, J.; Kittner, S.; De Leeuw, F.E.; Tuladhar, A.M. Ischaemic stroke in young adults: A global perspective. J. Neurol. Neurosurg. Psychiatry 2020, 91, 411–417. [Google Scholar] [CrossRef]
- Byrne, C.P.; Bennett, K.E.; Hickey, P.; Broderick, B.; O’Mahony, M.; Williams, D.J. Short-term air pollution as a risk for stroke admission: A Time-Series Analysis. Cerebrovasc. Dis. 2020, 49, 404–411. [Google Scholar] [CrossRef]
- Feigin, V.L.; Roth, G.A.; Naghavi, M.; Parmar, P.; Krishnamurthi, R.; Chugh, S.; Mensah, G.A.; Norrving, B.; Shiue, I.; Ng, M.; et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: A systematic analysis for the global burden of disease study 2013. Lancet Neurol. 2016, 15, 913–924. [Google Scholar] [CrossRef]
- Gu, J.; Shi, Y.; Chen, N.; Wang, H.; Chen, T. Ambient fine particulate matter and hospital admissions for ischemic and hemorrhagic strokes and transient ischemic attack in 248 Chinese cities. Sci. Total Environ. 2020, 715, 136896. [Google Scholar] [CrossRef]
- Hahad, O.; Lelieveld, J.; Birklein, F.; Lieb, K.; Daiber, A.; Münzel, T. Ambient air pollution increases the risk of cerebrovascular and neuropsychiatric disorders through induction of inflammation and oxidative stress. Int. J. Mol. Sci. 2020, 21, 4306. [Google Scholar] [CrossRef]
- Ljungman, P.L.S.; Andersson, N.; Stockfelt, L.; Andersson, E.M.; Sommar, J.N.; Eneroth, K.; Gidhagen, L.; Johansson, C.; Lager, A.; Leander, K.; et al. Long-term exposure to particulate air pollution, black carbon, and their source components in relation to ischemic heart disease and stroke. Environ. Health Perspect. 2019, 127, 107012. [Google Scholar] [CrossRef]
- Rajagopalan, S.; Brauer, M.; Bhatnagar, A.; Deepak, L.B.; Brook, J.R.; Huang, W.; Münzel, T.; Newby, D.; Siegel, J.; Brook, R.D.; et al. Personal-level protective actions against particulate matter air pollution exposure: A scientific statement from the American Heart Association. Circulation 2020, 142, e411–e431. [Google Scholar] [CrossRef]
- Sommer, A.J.; Peters, A.; Rommel, M.; Cyrys, J.; Grallert, H.; Haller, D.; Muller, C.L.; Bind, M.A.C. A randomization-based causal inference framework for uncovering environmental exposure effects on human gut microbiota. PLoS Comput. Biol. 2022, 18, e1010044. [Google Scholar] [CrossRef]
- Belkaid, Y.; Hand, T. Role of the microbiota in immunity and inflammation. Cell 2014, 157, 121–141. [Google Scholar] [CrossRef]
- Visconti, A.; Le Roy, C.I.; Rosa, F.; Rossi, N.; Martin, T.C.; Mohney, R.P.; Weizhong, L.; de Rinaldis, E.; Bell, J.T.; Venter, J.C.; et al. Interplay between the human gut microbiome and host metabolism. Nat. Commun. 2019, 10, 4505. [Google Scholar] [CrossRef] [PubMed]
- Wikoff, W.R.; Anfora, A.T.; Liu, J.; Schultz, P.G.; Lesley, S.A.; Peters, E.C.; Siuzdak, G. Metabolomics analysis reveals large effects of gut microflora on mammalian blood metabolites. Proc. Natl. Acad. Sci. USA 2009, 106, 3698–3703. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Garcidueñas, L.; Reynoso-Robles, R.; Pérez-Guillé, B.; Mukherjee, P.S.; Gónzalez-Maciel, A. Combustion-derived nanoparticles, the neuroenteric system, cervical vagus, hyperphosphorylated alpha synuclein and tau in young Mexico City residents. Environ. Res. 2017, 159, 186–201. [Google Scholar] [CrossRef] [PubMed]
- Diao, J.; Xia, Y.; Jiang, X.; Qiu, J.; Cheng, S.; Su, J.; Duan, X.; Gao, M.; Qin, X.; Zhang, J.; et al. Silicon dioxide nanoparticles induced neurobehavioral impairments by disrupting microbiota-gut-brain axis. J. Nanobiotechnol. 2021, 19, 174. [Google Scholar] [CrossRef]
- You, R.; Ho, Y.S.; Chang, R.C.C. The pathogenic effects of particulate matter on neurodegeneration: A review. J. Biomed. Sci. 2022, 29, 15. [Google Scholar] [CrossRef]
- Humpreys, J.; Valdes Hernandez, M.d.C. Impact of polycyclic aromatic hydrocarbon exposure on cognitive function and neurodegeneration in humans: A systemic review and meta-analysis. Front. Neurol. 2023, 13, 1052333. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; Herrera-Soto, A.; Jury, N.; Maher, B.A.; González-Maciel, A.; Reynoso-Robles, R.; Ruiz-Rudolph, P.; van Zundert, B.; Varela-Nallar, L. Reduced repressive epigenetic marks, increased DNA damage and Alzheimer’s disease hallmarks in the brain of humans and mice exposed to particulate urban air pollution. Environ. Res. 2020, 183, 109226. [Google Scholar] [CrossRef]
- Li, Y.; Liu, Y.; Hu, C.; Chang, Q.; Deng, Q.; Yang, X.; Wu, Y. Study of the neurotoxicity of indoor airborne nanoparticles based on a 3D human blood-brain barrier chip. Environ. Int. 2020, 143, 105598. [Google Scholar] [CrossRef]
- Jayaraj, R.L.; Rodriguez, E.A.; Wang, Y.; Block, M.L. Outdoor ambient air pollution and neurodegenerative diseases: The neuroinflammation hypothesis. Curr. Environ. Health Rep. 2017, 4, 166–179. [Google Scholar] [CrossRef]
- Ku, T.; Li, B.; Gao, R.; Zhang, Y.; Yan, W.; Ji, X.; Li, G.; Sang, N. NF-kappaB-regulated microRNA-574–5p underlies synaptic and cognitive impairment in response to atmospheric PM2.5 aspiration. Part. Fibre Toxicol. 2017, 14, 34. [Google Scholar] [CrossRef]
- Li, J.; Dong, Y.; Song, Y.; Dong, B.; van Donkelaar, A.; Martin, R.V.; Shi, L.; Ma, Y.; Zou, Z.; Ma, J. Long-term effects of PM2.5 components on blood pressure and hypertension in Chinese children and adolescents. Environ. Int. 2022, 161, 107134. [Google Scholar] [CrossRef]
- Knopman, D.S. Cerebrovascular disease and dementia. Br. J. Radiol. 2014, 80, S121–S127. [Google Scholar] [CrossRef]
- Chen, J.C.; Wang, X.; Wellenius, G.A.; Serre, M.L.; Driscoll, I.; Casanova, R.; McArdle, J.J.; Manson, J.E.; Chui, H.C.; Espeland, M.A. Ambient air pollution and neurotoxicity on brain structure: Evidence from women’s health initiative memory study. Ann. Neurol. 2015, 78, 466–476. [Google Scholar] [CrossRef]
- Younan, D.; Petkus, A.J.; Widaman, K.F.; Wang, X.; Casanova, R.; Espeland, M.A.; Gatz, M.; Henderson, V.W.; Manson, J.E.; Rapp, S.R.; et al. Particulate matter and episodic memory decline mediated by early neuroanatomic biomarkers of Alzheimer’s disease. Brain 2020, 143, 289–302. [Google Scholar] [CrossRef]
- Allen, J.L.; Liu, X.; Pelkowski, S.; Palmer, B.; Conrad, K.; Oberdorster, G.; Weston, D.; Mayer-Proschel, M.; Cory-Slechta, D.A. Early postnatal exposure to ultrafine particulate matter air pollution: Persistent ventriculomegaly, neurochemical disruption, and glial activation preferentially in male mice. Environ. Health Perspect. 2014, 122, 939–945. [Google Scholar] [CrossRef]
- Koivisto, A.M.; Kurki, M.I.; Alafuzoff, I.; Sutela, A.; Rummukainen, J.; Savolainen, S.; Vanninen, R.; Jääskeläinen, J.E.; Soininen, H.; Leinonen, V. High risk of dementia in ventricular enlargement with normal pressure hydrocephalus related symptoms1. J. Alzheimers Dis. 2016, 52, 497–507. [Google Scholar] [CrossRef]
- Rodriguez-Martinez, E.; Martinez, F.; Espinosa-Garcia, M.T.; Maldonado, P.; Rivas-Arancibia, S. Mitochondrial dysfunction in the hippocampus of rats caused by chronic oxidative stress. Neuroscience 2013, 252, 384–395. [Google Scholar] [CrossRef]
- Erickson, M.A.; Jude, J.; Zhao, H.; Rhea, E.M.; Salameh, T.S.; Jester, W.; Pu, S.; Harrowitz, J.; Nguyen, N.; Banks, W.A.; et al. Serum amyloid A: An ozone-induced circulating factor with potentially important functions in the lung-brain axis. FASEB J. 2017, 31, 3950–3965, Erratum in FASEB J. 2018, 31, 535. [Google Scholar] [CrossRef]
- Martinez-Canabal, A.; Angoa-Perez, M.; Rugerio-Vargas, C.; Borgonio-Perez, G.; Rivas-Arancibia, S. Effect of growth hormone on Cyclooxygenase-2 expression in the hippocampus of rats chronically exposed to ozone. Int. J. Neurosci. 2008, 118, 455–469. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; Solt, A.C.; Henriquez-Roldan, C.; Torres-Jardon, R.; Nuse, B.; Herritt, L.; Villarreal-Calderon, R.; Osnaya, N.; Stone, I.; Garcia, R.; et al. Long-term air pollution exposure is associated with neuroinflammation, an altered innate immune response, disruption of the blood-brain barrier, ultrafine particulate deposition, and accumulation of amyloid beta-42 and alpha-synuclein in children and young adults. Toxicol. Pathol. 2008, 36, 289–310. [Google Scholar]
- Kummer, M.P.; Hermes, M.; Delekarte, A.; Hammerschmidt, T.; Kumar, S.; Terwel, D.; Walter, J.; Pape, H.C.; Konig, S.; Roeber, S.; et al. Nitration of tyrosine 10 critically enhances amyloid β aggregation and plaque formation. Neuron 2011, 71, 833–844. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Xin, X. Nitrogen dioxide (NO (2)) pollution as a potential risk factor for developing vascular dementia and its synaptic mechanisms. Chemosphere 2013, 92, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Saunders, C.R.; Das, S.K.; Ramesh, A.; Shockley, D.C.; Mukherjee, S. Benzo(a)pyrene-induced acute neurotoxicity in the F-344rat: Role of oxidative stress. J. Appl. Toxic. 2006, 26, 427–438. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Current drugs approved for the treatment of cognitive impairment and AD-related dementia (registration and indication for oral and i.v. therapy). Abbreviations: AD—Alzheimer’s disease; i.v.—intravenous administration; Aβ—amyloid beta; NMDA—N-methyl-D-aspartate receptor; FDA—Food and Drug Administration (USA); EMA—European Medicines Agency (EMA); NMPA—National Medical Products Administration (China). * Continued approval will be based on further trials confirming a clinical benefit over currently available therapy.
Figure 1.
Current drugs approved for the treatment of cognitive impairment and AD-related dementia (registration and indication for oral and i.v. therapy). Abbreviations: AD—Alzheimer’s disease; i.v.—intravenous administration; Aβ—amyloid beta; NMDA—N-methyl-D-aspartate receptor; FDA—Food and Drug Administration (USA); EMA—European Medicines Agency (EMA); NMPA—National Medical Products Administration (China). * Continued approval will be based on further trials confirming a clinical benefit over currently available therapy.

Figure 2.
Size-dependent regional deposition of inhaled particulate matters. The deposition sites of various inhaled particles of differing size (PM10, PM2.5, and PM1), which are located in specific regions of the respiratory tract. Created with BioRender.com (accessed on 3 February 2023).
Figure 2.
Size-dependent regional deposition of inhaled particulate matters. The deposition sites of various inhaled particles of differing size (PM10, PM2.5, and PM1), which are located in specific regions of the respiratory tract. Created with BioRender.com (accessed on 3 February 2023).

Figure 3.
Environmental exposures to air pollutants in the etiology and pathogenesis of dementia. Sources of air pollution (fine and ultrafine particles—UFPM) include particles smaller than 2.5 μm in diameter, for which annual average concentrations should not exceed 10 μg/m. Air pollution is a common environmental factor that affects the brain through multiple pathways (i.e., through the olfactory tract and blood vessels via the respiratory system). Particles affect the brain by accelerating (priming) microglia and astroglia and, thus, initiating neuroinflammation, production of reactive oxygen species (ROS), deposition of amyloid beta (Aβ) peptides, and tau phosphorylation. Aβ causes synaptic impairment, neuronal death, and progressive neurodegeneration, ultimately leading to Ad-related dementia and cognitive impairment. Created with BioRender.com (accessed on 12 May 2023).
Figure 3.
Environmental exposures to air pollutants in the etiology and pathogenesis of dementia. Sources of air pollution (fine and ultrafine particles—UFPM) include particles smaller than 2.5 μm in diameter, for which annual average concentrations should not exceed 10 μg/m. Air pollution is a common environmental factor that affects the brain through multiple pathways (i.e., through the olfactory tract and blood vessels via the respiratory system). Particles affect the brain by accelerating (priming) microglia and astroglia and, thus, initiating neuroinflammation, production of reactive oxygen species (ROS), deposition of amyloid beta (Aβ) peptides, and tau phosphorylation. Aβ causes synaptic impairment, neuronal death, and progressive neurodegeneration, ultimately leading to Ad-related dementia and cognitive impairment. Created with BioRender.com (accessed on 12 May 2023).


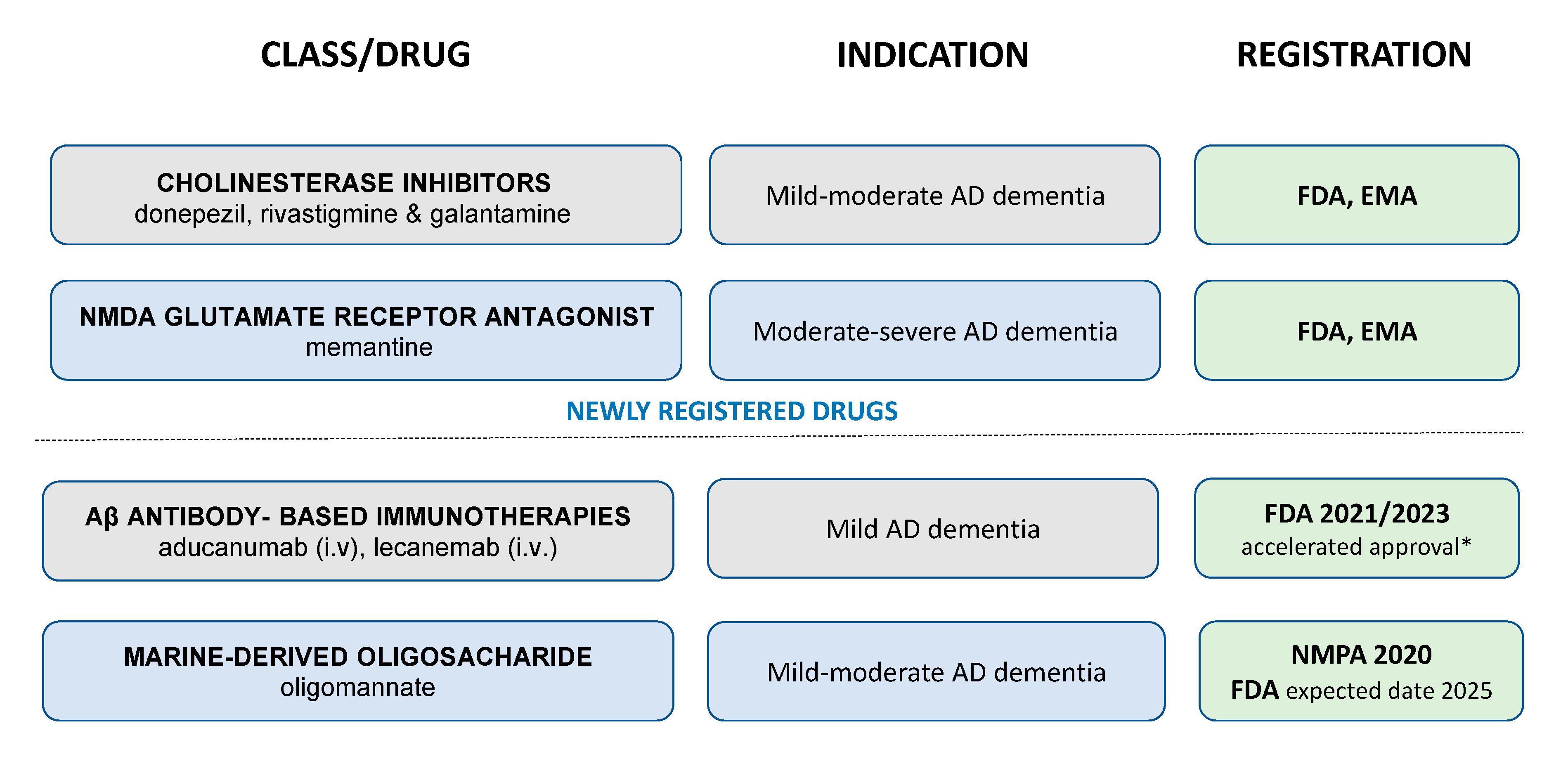{kind=link}
{kind=link}
{kind=link}
Table 1.
Major air pollutants and the type of their effects on the development and progress of dementia.
Table 1.
Major air pollutants and the type of their effects on the development and progress of dementia.
| Air Pollutant | Effect | References |
|---|---|---|
| PM10 |
| |
| PM2.5 |
| [75,76,77,137,158,159,160,161,162,163,164,165,166,167] |
| UFPs (e.g., PM0.1) |
| [84,118,125,131,158,159,168,169] |
| Ozone |
| [170,171,172,173] |
| Nitrogen dioxide |
| [174,175] |
| Polycyclic aromatic hydrocarbons (PAH) | Since PAHs are associated with particulate matter of an aerodynamic diameter ≤2.5 μm (PM2.5), it is not obvious whether PAHs solely can be associated with the development and/or progression of dementia. However, a body of evidence confirmed such a relationship, and this includes the following:
| [175,176] |
The effects summarized for PMs, including UFPMs, were not categorized based on PM’s composition (such as sulfate, nitrate, ammonium, organic carbon, elemental carbon, and heavy metals), surface properties, and concentration. ↑ = increase; ↓ decrease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Serafin, P.; Zaremba, M.; Sulejczak, D.; Kleczkowska, P. Air Pollution: A Silent Key Driver of Dementia. Biomedicines 2023, 11, 1477. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines11051477
AMA Style
Serafin P, Zaremba M, Sulejczak D, Kleczkowska P. Air Pollution: A Silent Key Driver of Dementia. Biomedicines. 2023; 11(5):1477. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines11051477
Chicago/Turabian StyleSerafin, Pawel, Malgorzata Zaremba, Dorota Sulejczak, and Patrycja Kleczkowska. 2023. "Air Pollution: A Silent Key Driver of Dementia" Biomedicines 11, no. 5: 1477. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines11051477
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.