Comparative Evaluation of Endotoxin Activity Level and Various Biomarkers for Infection and Outcome of ICU-Admitted Patients

Abstract
:1. Introduction
2. Experimental Section
2.1. Patient Characteristics
2.2. Endotoxin Activity Assay (EAA)
2.3. Laboratory Analyses
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
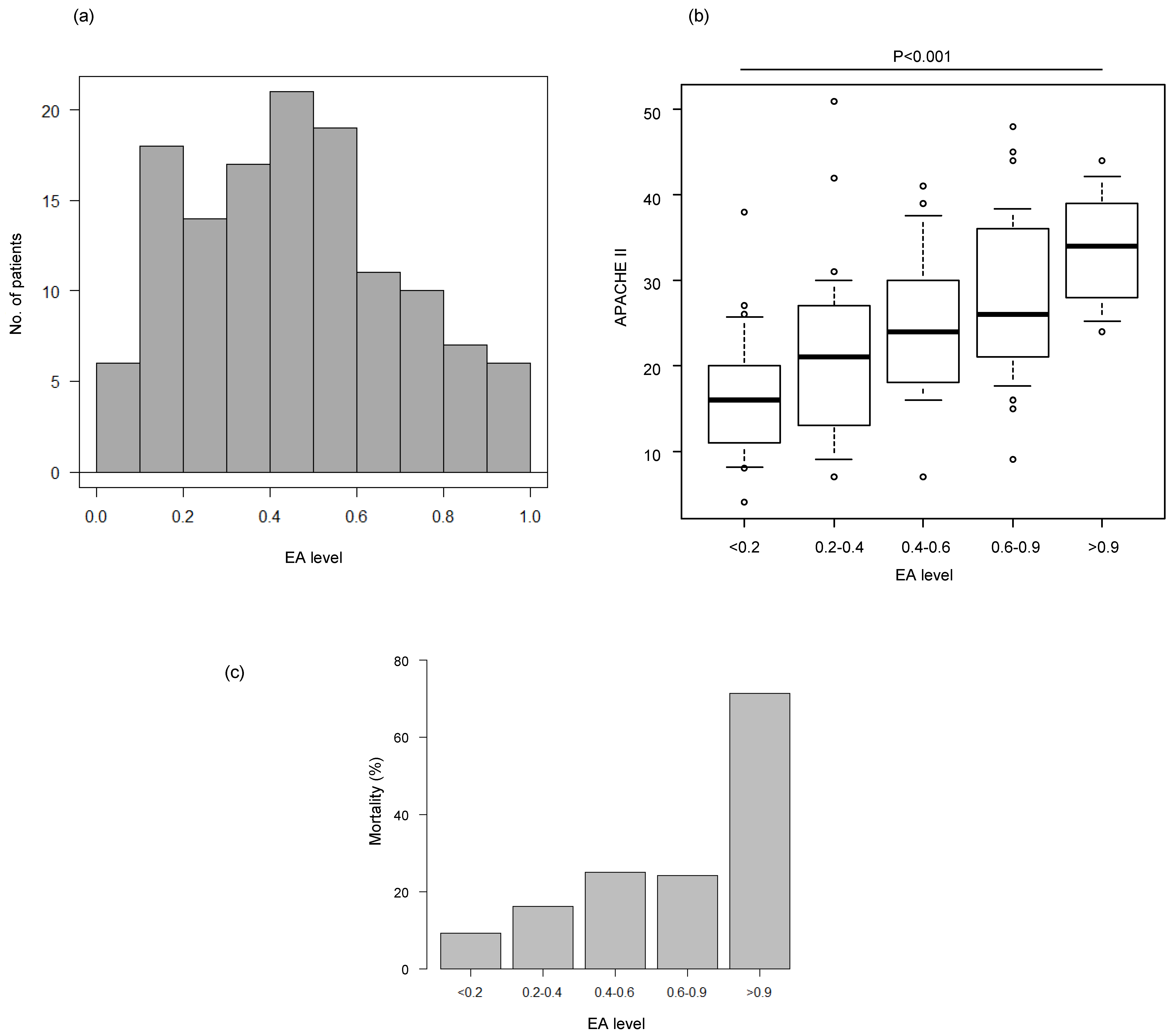
3.2. Comparison Between the EA Level and Disease Severity or Mortality
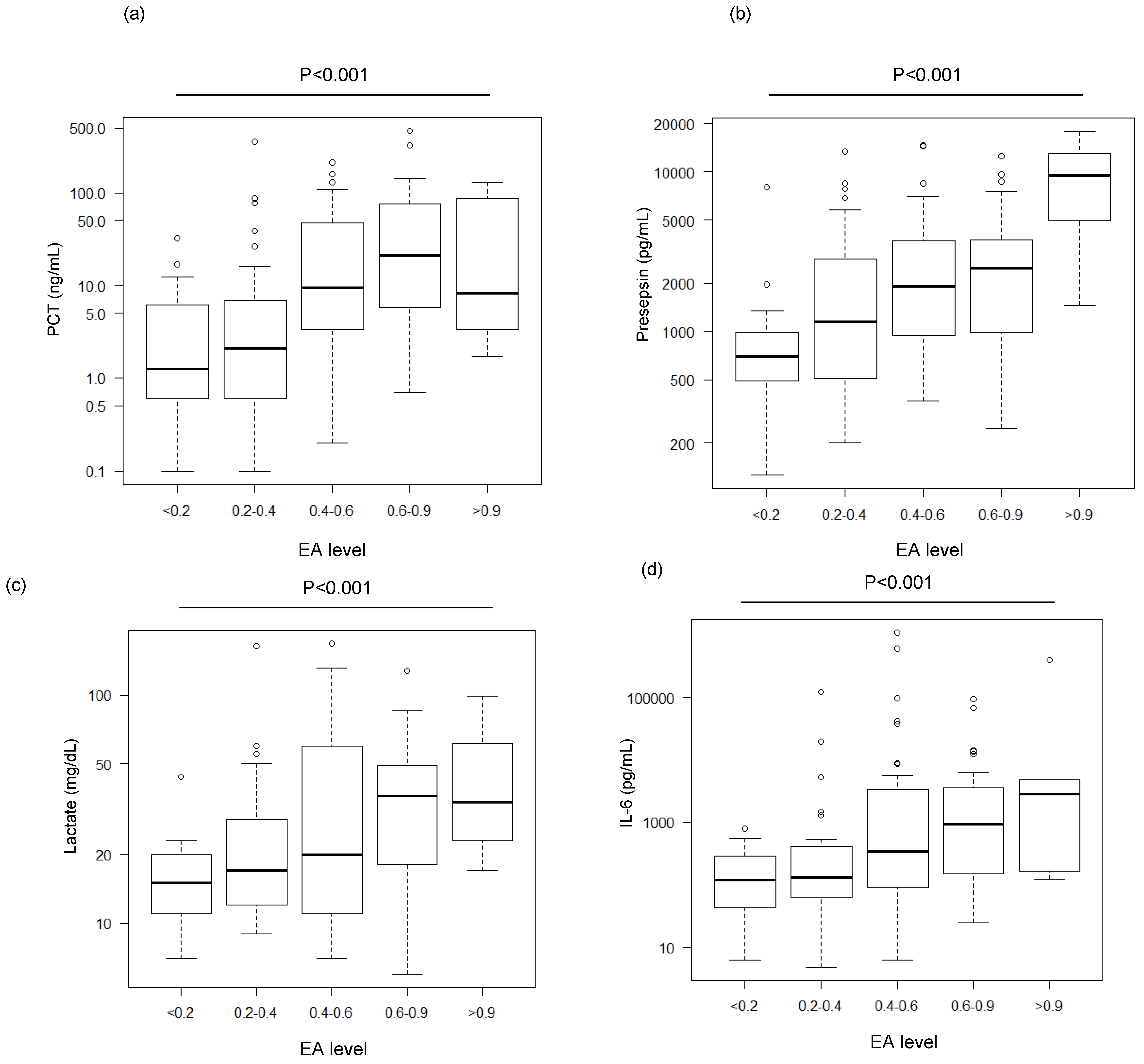
3.3. Comparison Between the EA Level and Various Biomarkers
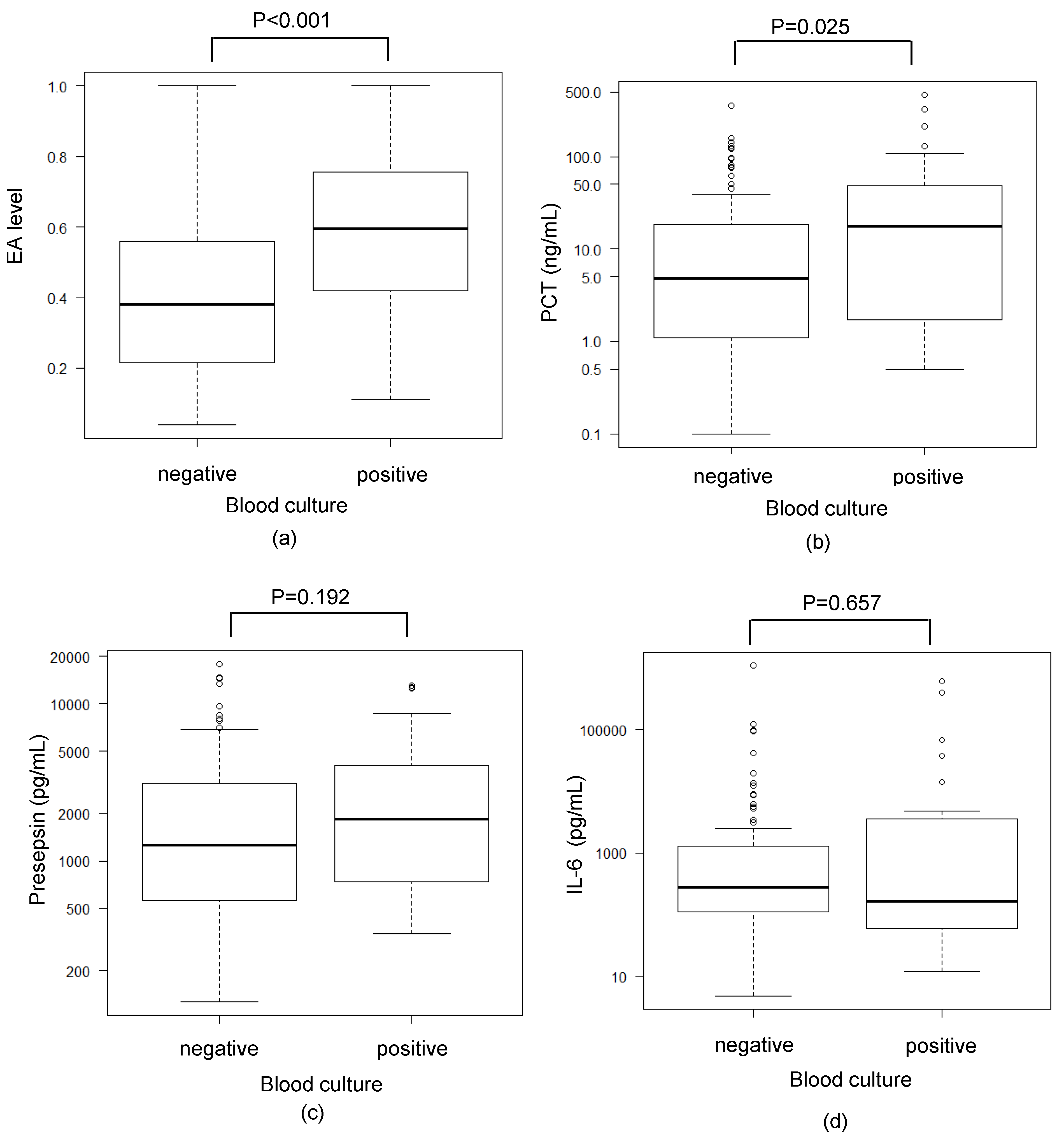
3.4. Comparison Between Blood Culture Results and Various Biomarkers
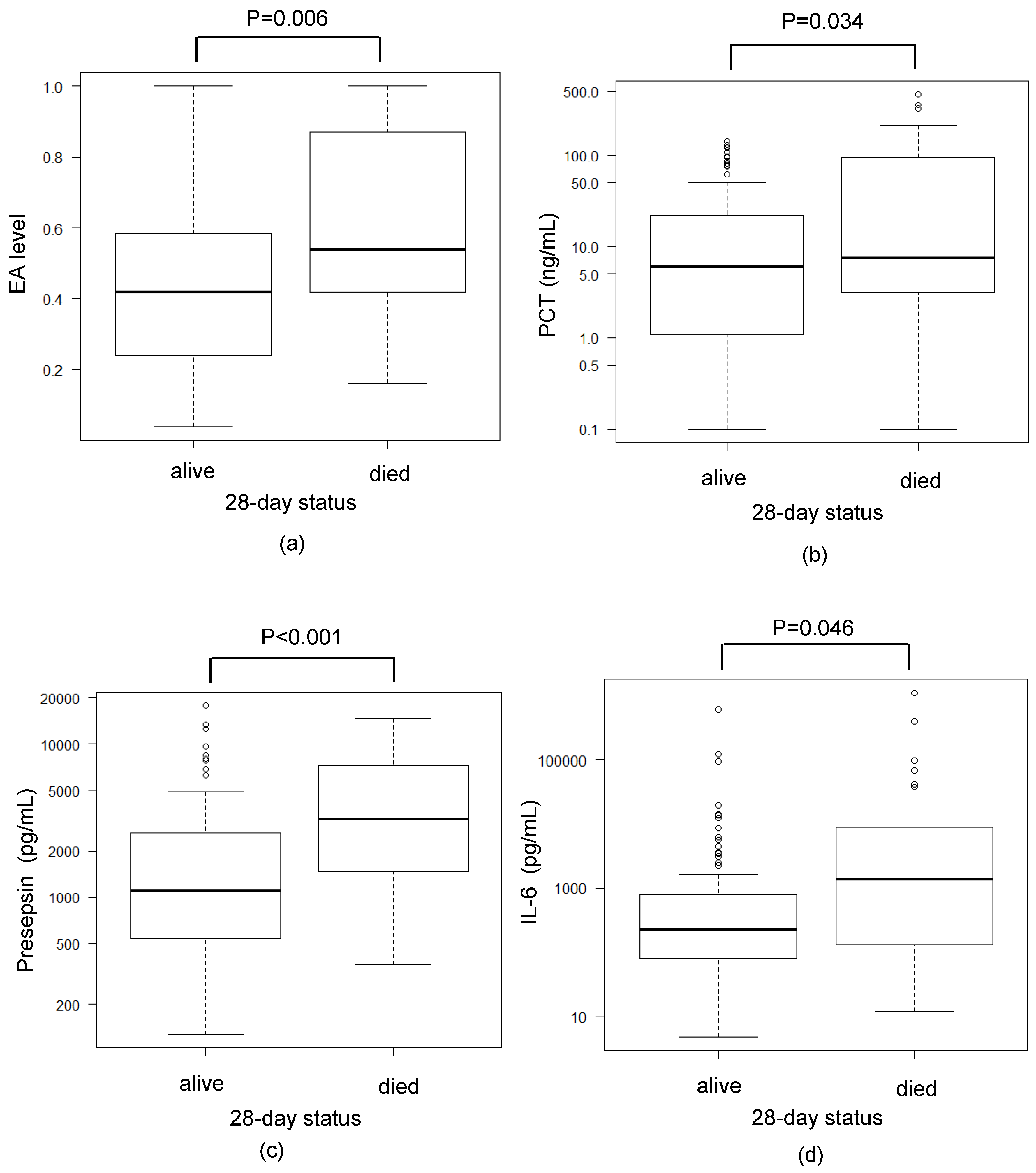
3.5. Comparison Between Mortality and Various Biomarkers
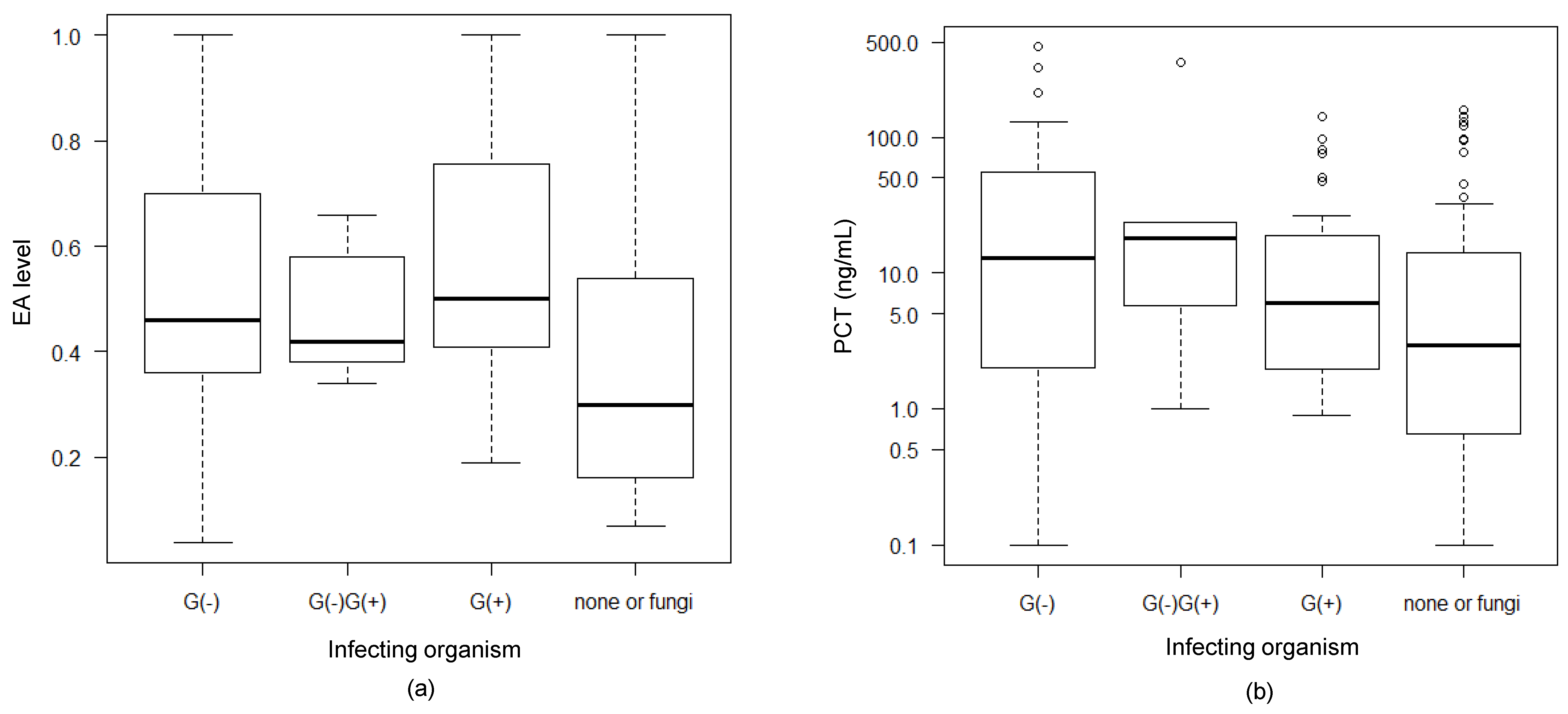
3.6. Association Between Infecting Organisms and EAA and PCT Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| EA level | endotoxin level |
| ICU | intensive care unit |
| EAA | endotoxin activity assay |
| PCT | procalcitonin |
| IL-6 | interleukin-6 |
| LAL | limulus amebocyte lysate |
| WBC | white blood cell count |
| CRP | C-reactive protein |
| FDA | Food and Drug Administration |
| EDTA | ethylenediaminetetraacetic acid |
| IQR | interquartile range |
| ECLIA | electrochemiluminescence immunoassay |
| CLEIA | chemiluminescent enzyme immunoassay |
| APACHE II | Acute Physiology and Chronic Health Evaluation II |
| SOFA | Sequential Organ Failure Assessment |
| SIRS | systemic inflammatory response syndrome |
References
- Carswell, E.A.; Old, L.J.; Kassel, R.L.; Green, S.; Fiore, N.; Williamson, B. An endotoxin-induced serum factor that causes necrosis of tumors. Proc. Nat. Acad. Sci. USA 1975, 72, 3666–3670. [Google Scholar] [CrossRef] [PubMed]
- Ulevitch, R.J.; Tobias, P.S. Recognition of Gram-negative bacteria and endotoxin by the innate immune system. Curr. Opin. Immunol. 1999, 11, 19–22. [Google Scholar] [CrossRef]
- Romaschin, A.D.; Klein, D.J.; Marshall, J.C. Bench-to-bedside review: Clinical experience with the endotoxin activity assay. Crit. Care 2012, 16, 248. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Assicot, M.; Gendrel, D.; Carsin, H.; Raymond, J.; Guilbaud, J.; Bohuon, C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet 1993, 341, 515–518. [Google Scholar] [CrossRef]
- Shozushima, T.; Takahashi, G.; Matsumoto, N.; Kojika, M.; Okamura, Y.; Endo, S. Usefulness of presepsin (sCD14-ST) measurements as a marker for the diagnosis and severity of sepsis that satisfied diagnostic criteria of systemic inflammatory response syndrome. J. Infect. Chemother. 2011, 17, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.P.; Chen, C.K.; Chung, K.; Tseng, J.C.; Hua, C.C.; Liu, Y.C.; Chuang, D.Y.; Yang, C.H. Serial cytokine levels in patients with severe sepsis. Inflamm. Res. 2009, 58, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Kong, L.; Fink, M.P.; Weissfeld, L.A.; Yearly, D.M.; Pinsky, M.R.; Fine, J.; Krichevsky, A.; Delude, R.L.; Angus, D.C. Understanding the inflammatory cytokine response in pneumonia and sepsis: Results of the genetic and inflammatory markers of sepsis (GenIMS) study. Arch. Intern. Med. 2007, 167, 1655–1663. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.T.; Sudhir, U.; Punith, K.; Kumar, R.; Ravi Kumar, V.N.; Rao, M.Y. Cytokine profile in elderly patients with sepsis. Ind. J. Crit. Care Med. 2009, 13, 74–78. [Google Scholar] [CrossRef] [Green Version]
- Ríos-Toro, J.J.; Márquez-Coello, M.; García-Álvarez, J.M.; Martín-Aspas, A.; Rivera-Fernández, R.; Sáez de Benito, A.; Girón-González, J.A. Soluble membrane receptors, interleukin 6, procalcitonin and C reactive protein as prognostic markers in patients with severe sepsis and septic shock. PLoS ONE 2017, 12, e0175254. [Google Scholar] [CrossRef]
- Romaschin, A.D.; Harris, D.M.; Ribeiro, M.B.; Paice, J.; Foster, D.M.; Walker, P.M.; Walker, P.M.; Marshall, J.C. A rapid assay of endotoxin in whole blood using autologous neutrophil dependent chemiluminescence. J. Immunol. Methods 1988, 212, 169–185. [Google Scholar] [CrossRef]
- Marshall, J.C.; Foster, D.; Vincent, J.L.; Cook, D.J.; Cohen, J.; Dellinger, R.P.; Opal, S.; Abraham, E.; Brett, S.J.; Smith, T.; et al. Diagnostic and prognostic implications of endotoxemia in critical illness: Results of the MEDIC study. J. Infect. Dis. 2004, 190, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Müller, B.; White, J.C.; Nylén, E.S.; Snider, R.H.; Becker, K.L.; Habener, J.F. Ubiquitous expression of the calcitonin-1 gene in multiple tissues in response to sepsis. J. Clin. Endocrinol. Metab. 2001, 86, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.M.; Eslick, G.D.; Craig, J.C.; McLean, A.S. Accuracy of procalcitonin for sepsis diagnosis in critically ill patients: Systematic review and meta-analysis. Lancet Infect. Dis. 2007, 7, 210–217. [Google Scholar] [CrossRef]
- Jensen, J.U.; Heslet, L.; Jensen, T.H.; Espersen, K.; Steffensen, P.; Tvede, M. Procalcitonin increase in early identification of critically ill patients at high risk of mortality. Crit. Care Med. 2006, 34, 2596–2602. [Google Scholar] [CrossRef] [PubMed]
- Bouadma, L.; Luyt, C.E.; Tubach, F.; Cracco, C.; Alvarez, A.; Schwebel, C.; Schortgen, F.; Lasocki, S.; Veber, B.; Dehoux, M.; et al. Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): A multicentre randomised controlled trial. Lancet 2010, 375, 463–474. [Google Scholar] [CrossRef]
- Maisel, A.; Neath, S.X.; Landsberg, J.; Mueller, C.; Nowak, R.M.; Peacock, W.F.; Ponikowski, P.; Möckel, M.; Hogan, C.; Wu, A.H.; et al. Use of procalcitonin for the diagnosis of pneumonia in patients presenting with a chief complaint of dyspnoea: Results from the BACH (Biomarkers in Acute Heart Failure) trial. Eur. J. Heart Fail. 2012, 14, 278–286. [Google Scholar] [CrossRef]
- Shirakawa, K.; Naitoh, K.; Hirose, J.; Nakamura, M.; Takeuchi, T.; Hosaka, Y.; Furusako, S. The new sepsis marker, sCD14-ST, induction mechanism in the rabbit sepsis models. Crit. Care 2010, 14, S5. [Google Scholar] [CrossRef]
- Hina, C.; Juhua, Z.; Yin, Z.; Mir, M.A.; Franklin, M.; Prakash, S.N.; Mitzi, N. Role of cytokines as a double-edged sword in sepsis. In Vivo 2013, 27, 669–684. [Google Scholar]
- Meisner, M. Procalcitonin—Biochemistry and Clinical Diagnosis, 1st ed.; UNI-MED: Bremen, Germany, 2010. [Google Scholar]
- Takahashi, W.; Nakada, T.A.; Yazaki, M.; Oda, S. Interleukin-6 levels act as a diagnostic marker for infection and a prognostic marker in patients with organ dysfunction in intensive care units. Shock 2016, 46, 254–260. [Google Scholar] [CrossRef]
- Koch, C.; Ruhrmann, S.; Pöhlmann, M.; Schneck, E.; Arneth, B.; Zajonz, T.; Sander, M.; Weigand, M.A.; Uhle, F. Longitudinal evaluation of plasma concentrations of presepsin in patients after severe trauma: A prospective observational study. Surg. Infect (Larchmt). 2018, 19, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Charbonney, E.; Tsang, J.Y.; Li, Y.; Klein, D.; Duque, P.; Romaschin, A.; Marshall, J.C. Endotoxemia Following Multiple Trauma: Risk Factors and Prognostic Implications. Crit. Care Med. 2016, 44, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, D.; Guivarch, E.; Neveux, N.; Fichet, J.; Pène, F.; Marx, J.S.; Chiche, J.D.; Cynober, L.; Mira, J.P.; Cariou, A. Markers of intestinal injury are associated with endotoxemia in successfully resuscitated patients. Resuscitation 2013, 84, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Thomas-Rüddel, D.O.; Poidinger, B.; Kott, M.; Weiss, M.; Reinhart, K. Influence of pathogen and focus of infection on procalcitonin values in sepsis patients with bacteremia or candidemia. Crit. Care 2018, 22, 128. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Klein, D.J. Polymyxin B hemoperfusion: A mechanistic perspective. Crit. Care 2014, 18, 309. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Bagshaw, S.M.; Antonelli, M.; Foster, D.M.; Klein, D.J.; Marshall, J.C.; Palevsky, P.M.; Weisberg, L.S.; Schorr, C.A.; Trzeciak, S.; et al. Effect of targeted polymyxin B hemoperfusion on 28-day mortality in patients with septic shock and elevated endotoxin level: The EUPHRATES randomized clinical trial. JAMA 2018, 20, 1455–1463. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, T.; Ikeda, K.; Suda, S.; Ueno, T. Usefulness of the endotoxin activity assay as a biomarker to assess the severity of endotoxemia in critically ill patients. Innate Immun. 2014, 20, 881–887. [Google Scholar] [CrossRef] [Green Version]
- Klein, D.J.; Foster, D.M.; Walker, P.M.; Bagshaw, S.M.; Mekonnen, H.; Antonelli, M. Polymyxin B hemoperfusion in endotoxemic septic shock patients without extreme endotoxemia: A post hoc analysis of the EUPHRATES trial. Intensive Care Med. 2018, 44, 2205–2212. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Age (median (IQR)) | 71 (66–77) |
| Male (n (%)) | 92 (71.3%) |
| Female (n (%)) | 37 (28.7%) |
| Severity (median (IQR)) | |
| APACHE II score | 23 (16–30) |
| SOFA score | 9 (5–12) |
| Blood culture (n (%)) | |
| Positive | 37 (28.7%) |
| Negative | 92 (71.3%) |
| Infecting organism (n (%)) | |
| Gram-negative | 41 (31.8%) |
| Gram-positive | 26 (20.2%) |
| Mixed infection | 5 (3.9%) |
| Other (None or fungi) | 57 (44.2%) |
| 28-day mortality (n (%)) | 29 (22.5%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikeda, T.; Kamohara, H.; Suda, S.; Nagura, T.; Tomino, M.; Sugi, M.; Wajima, Z. Comparative Evaluation of Endotoxin Activity Level and Various Biomarkers for Infection and Outcome of ICU-Admitted Patients. Biomedicines 2019, 7, 47. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines7030047
Ikeda T, Kamohara H, Suda S, Nagura T, Tomino M, Sugi M, Wajima Z. Comparative Evaluation of Endotoxin Activity Level and Various Biomarkers for Infection and Outcome of ICU-Admitted Patients. Biomedicines. 2019; 7(3):47. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines7030047
Chicago/Turabian StyleIkeda, Toshiaki, Hidenobu Kamohara, Shingo Suda, Takeo Nagura, Mikiko Tomino, Masatoshi Sugi, and Zen’ichiro Wajima. 2019. "Comparative Evaluation of Endotoxin Activity Level and Various Biomarkers for Infection and Outcome of ICU-Admitted Patients" Biomedicines 7, no. 3: 47. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines7030047