Disorders of Dental Hard Tissues Induced by Radioiodine-131 (I-131) Therapy Used in Differentiated Thyroid Cancer: An In Vitro Study

 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Preparation and Distribution in Groups
2.2. Radioiodine Irradiation Basics and Measurements of the Radioactive Isotopes
2.3. Atomic Force Microscopy on Enamel and Dentin
2.4. Statistical Analysis
3. Results
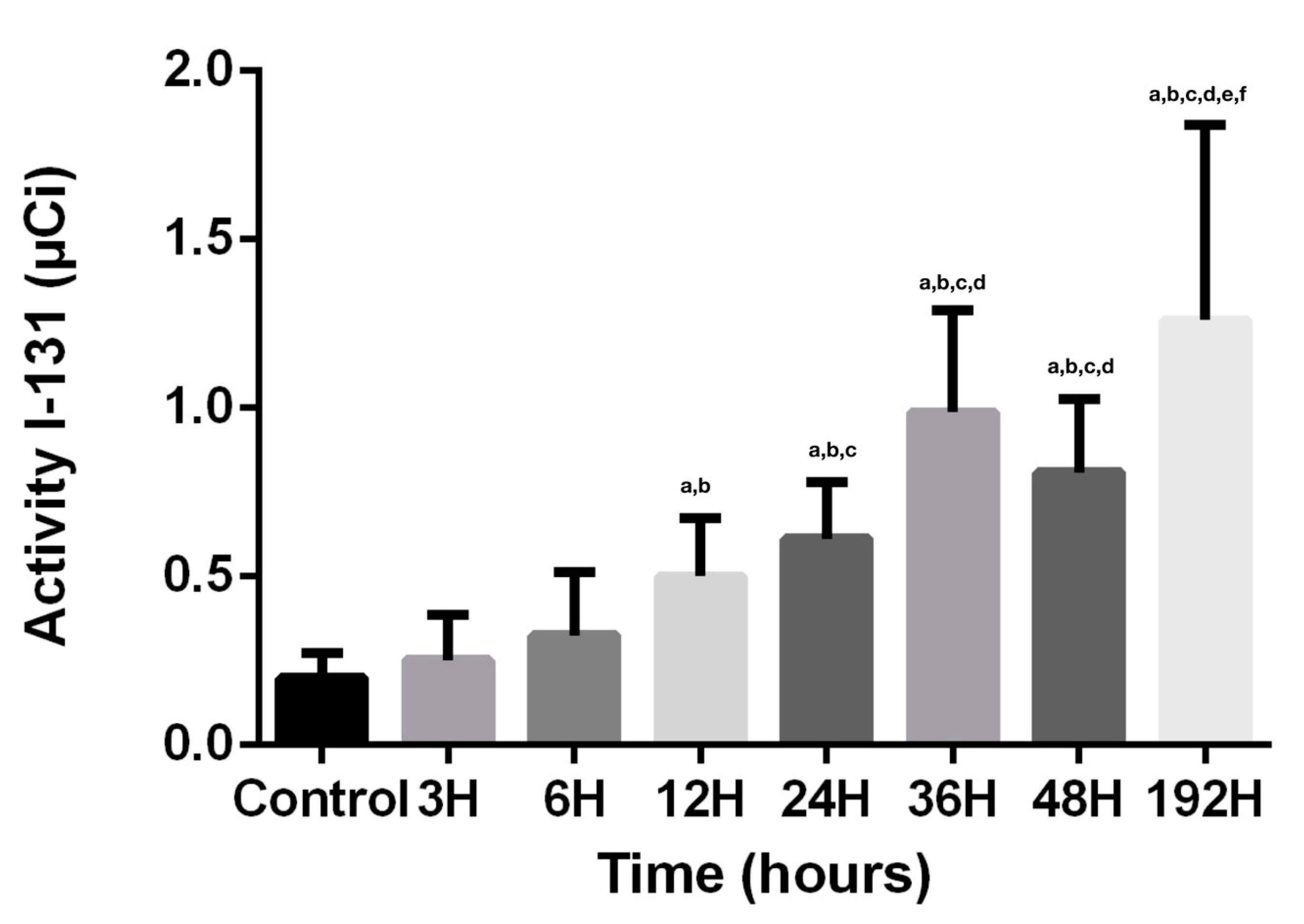
3.1. Radioiodine Activity
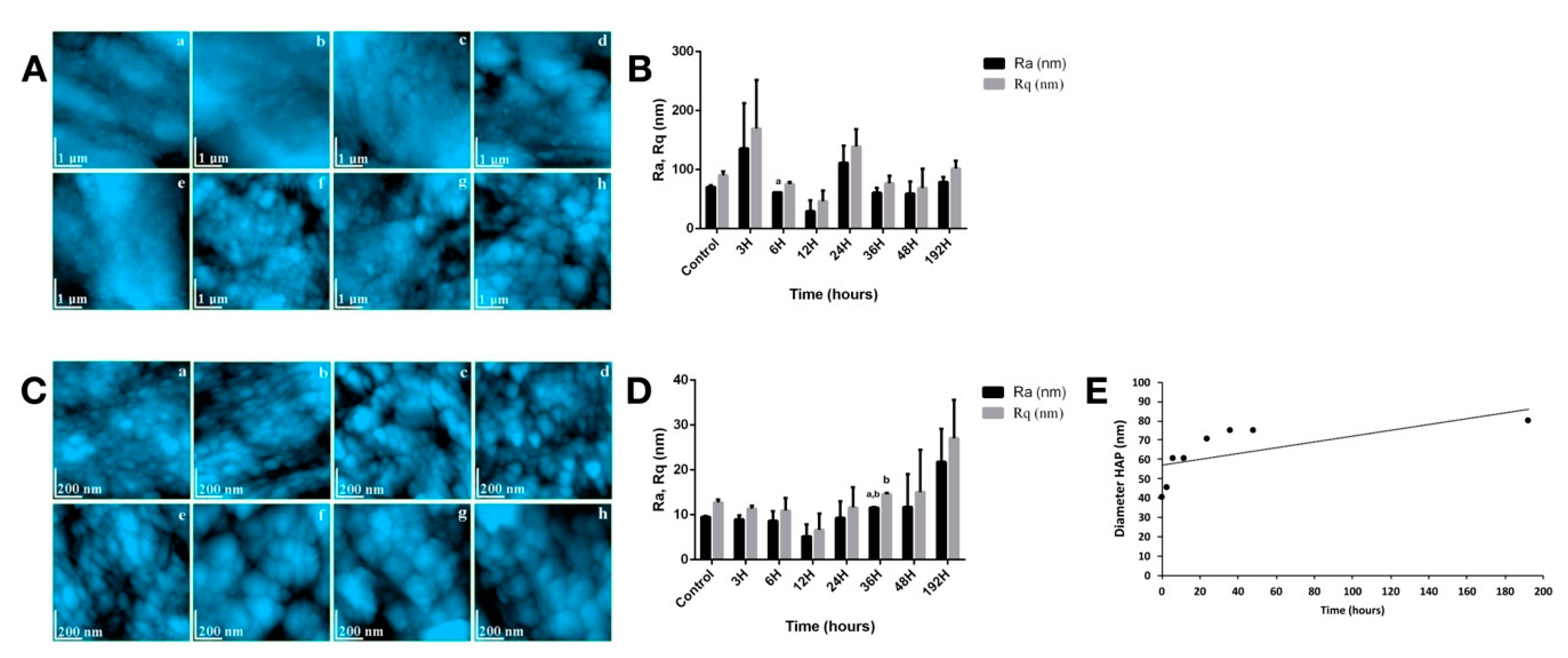
3.2. Enamel Assessment
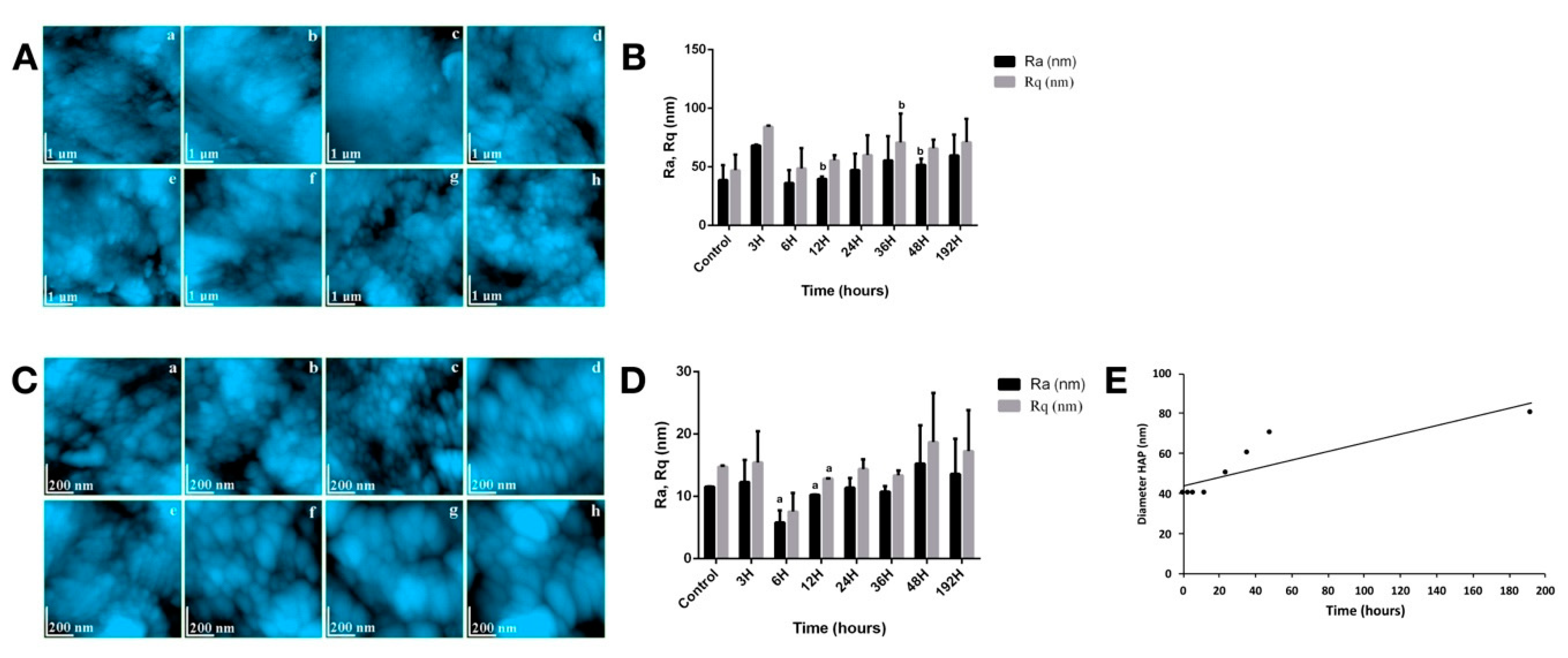
3.3. Dentin Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- NIH Cancer Stat Facts: Thyroid Cancer. Available online: https://seer.cancer.gov/statfacts/html/thyro.html (accessed on 4 November 2020).
- Piciu, D. Thyroid cancer incidence 25 years after Chernobyl, in a Romanian cancer center: Is it a public health problem? Curr. Radiopharm. 2013, 6, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Piciu, D. Nuclear Endocrinology, 2nd ed.; Springer: New York, NY, USA, 2017; ISBN 978-3319565811. [Google Scholar]
- Newkirk, K.A.; Ringel, M.D.; Wartofsky, L.; Burman, K.D. The role of radioactive iodine in salivary gland dysfunction. Ear Nose Throat J. 2000, 79, 460–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, S.Y.; Kim, H.W.; Lee, S.-W.; Ahn, B.-C.; Lee, J. Salivary gland function 5 years after radioactive iodine ablation in patients with differentiated thyroid cancer: Direct comparison of pre- and postablation scintigraphies and their relation to xerostomia symptoms. Thyroid 2013, 23, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Mandel, S.J.; Mandel, L. Radioactive iodine and the salivary glands. Thyroid 2003, 13, 265–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jo, K.S.; An, Y.-S.; Lee, S.J.; Soh, E.-Y.; Lee, J.; Chung, Y.-S.; Kim, D.J.; Yoon, S.-H.; Lee, D.H.; Yoon, J.-K. Significance of Salivary Gland Radioiodine Retention on Post-ablation (131)I Scintigraphy as a Predictor of Salivary Gland Dysfunction in Patients with Differentiated Thyroid Carcinoma. Nucl. Med. Mol. Imaging 2014, 48, 203–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kielbassa, A.M.; Hinkelbein, W.; Hellwig, E.; Meyer-Luckel, H. Radiation-related damage to dentition. Lancet Oncol. 2006, 7, 326–335. [Google Scholar] [CrossRef]
- Vissink, A.; Jansma, J.; Spijkervet, F.K.L.; Burlage, F.R.; Coppes, R.P. Oral sequelae of head and neck radiotherapy. Crit. Rev. Oral Biol. Med. 2003, 14, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.R.S.; Alves, F.A.; Berger, S.B.; Giannini, M.; Goes, M.F.; Lopes, M.A. Radiation-related caries and early restoration failure in head and neck cancer patients. A polarized light microscopy and scanning electron microscopy study. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2010, 18, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, L.M.N.; Palma-Dibb, R.G.; Paula-Silva, F.W.G.; de Oliveira, H.F.; Nelson-Filho, P.; da Silva, L.A.B.; de Queiroz, A.M. Radiation therapy alters microhardness and microstructure of enamel and dentin of permanent human teeth. J. Dent. 2014, 42, 986–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seyedmahmoud, R.; Wang, Y.; Thiagarajan, G.; Gorski, J.P.; Reed Edwards, R.; McGuire, J.D.; Walker, M.P. Oral cancer radiotherapy affects enamel microhardness and associated indentation pattern morphology. Clin. Oral Investig. 2018, 22, 1795–1803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Siqueira Mellara, T.; Palma-Dibb, R.G.; de Oliveira, H.F.; Garcia Paula-Silva, F.W.; Nelson-Filho, P.; da Silva, R.A.B.; da Silva, L.A.B.; de Queiroz, A.M. The effect of radiation therapy on the mechanical and morphological properties of the enamel and dentin of deciduous teeth—An in vitro study. Radiat. Oncol. 2014, 9, 30. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Zhao, Q.; Guo, J.; Zeng, B.; Yu, X.; Yu, D.; Zhao, W. Direct radiation-induced effects on dental hard tissue. Radiat. Oncol. 2019, 14, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benua, R.S.; Cicale, N.R.; Sonenberg, M.; Rawson, R.W. The relation of radioiodine dosimetry to results and complications in the treatment of metastatic thyroid cancer. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1962, 87, 171–182. [Google Scholar] [PubMed]
- Maxon, H.R.; Thomas, S.R.; Hertzberg, V.S.; Kereiakes, J.G.; Chen, I.W.; Sperling, M.I.; Saenger, E.L. Relation between effective radiation dose and outcome of radioiodine therapy for thyroid cancer. N. Engl. J. Med. 1983, 309, 937–941. [Google Scholar] [CrossRef] [PubMed]
- Alan Selcuk, N.; Toklu, T.; Beykan, S.; Karaaslan, S.I. Evaluation of the dosimetry approaches in ablation treatment of thyroid cancer. J. Appl. Clin. Med. Phys. 2018, 19, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Giovanella, L. Nuclear Medicine Therapy: Side Effects and Complications, 1st ed.; Springer Nature Switzerland AG: Cham, Switzerland, 2019; ISBN 978-2-030-17493-4. [Google Scholar]
- International Atomic Energy Agency IAEA-TECDOC-1340 Manual for Reactor Produced Radioisotopes; IAEA: Vienna, Austria, 2003; pp. 1–254.
- Kudkuli, J.; Abdulla, R.; Rekha, P.D.; Sharma, S.D.; Gurjar, O. Spectroscopic analyses reveal radiotherapy-induced variations in elemental composition and crystallite properties of human permanent teeth enamel. J. Oral Biosci. 2019, 61, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Bakr, M.A.; Saafan, A.M.; El Maghraby, E.M.F.; El Rouby, D.H.; Ahmed, S.F. Microhardness and Ultrastructure of Demineralized Gamma-Irradiated Human Enamel after Diode Laser (980 nm) and Fluoride Surface Treatment. Braz. Arch. Biol. Technol. 2019, 62. [Google Scholar] [CrossRef] [Green Version]
- Lechner, B.-D.; Roper, S.; Messerschmidt, J.; Blume, A.; Magerle, R. Monitoring Demineralization and Subsequent Remineralization of Human Teeth at the Dentin-Enamel Junction with Atomic Force Microscopy. ACS Appl. Mater. Interfaces 2015, 7, 18937–18943. [Google Scholar] [CrossRef] [PubMed]
- De Souza, M.R.; Watanabe, I.-S.; Azevedo, L.H.; Tanji, E.Y. Morphological Alterations of the Surfaces of Enamel and Dentin of Deciduous Teeth Irradiated with Nd:YAG, CO2 and Diode Lasers. Int. J. Morphol. 2009, 27, 441–446. [Google Scholar] [CrossRef] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mester, A.; Piciu, A.; Piciu, D.; Petean, I.; Lucaciu, P.O.; Apostu, D.; Moisescu-Goia, C.; Voina-Tonea, A.; Moldovan, M. Disorders of Dental Hard Tissues Induced by Radioiodine-131 (I-131) Therapy Used in Differentiated Thyroid Cancer: An In Vitro Study. Biomedicines 2020, 8, 475. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8110475
Mester A, Piciu A, Piciu D, Petean I, Lucaciu PO, Apostu D, Moisescu-Goia C, Voina-Tonea A, Moldovan M. Disorders of Dental Hard Tissues Induced by Radioiodine-131 (I-131) Therapy Used in Differentiated Thyroid Cancer: An In Vitro Study. Biomedicines. 2020; 8(11):475. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8110475
Chicago/Turabian StyleMester, Alexandru, Andra Piciu, Doina Piciu, Ioan Petean, Patricia Ondine Lucaciu, Dragos Apostu, Cristina Moisescu-Goia, Andrada Voina-Tonea, and Marioara Moldovan. 2020. "Disorders of Dental Hard Tissues Induced by Radioiodine-131 (I-131) Therapy Used in Differentiated Thyroid Cancer: An In Vitro Study" Biomedicines 8, no. 11: 475. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8110475