
Link between History of Childhood Maltreatment and Emotion Dysregulation in Adults Suffering from Attention Deficit/Hyperactivity Disorder or Borderline Personality Disorder

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Assessment Instruments
2.3. Statistics
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Effect of Childhood Maltreatment on ERS Scores
3.3. Effect of Childhood Maltreatment on CERQ Scores
3.4. Effect of Childhood Maltreatment on RSQ Scores
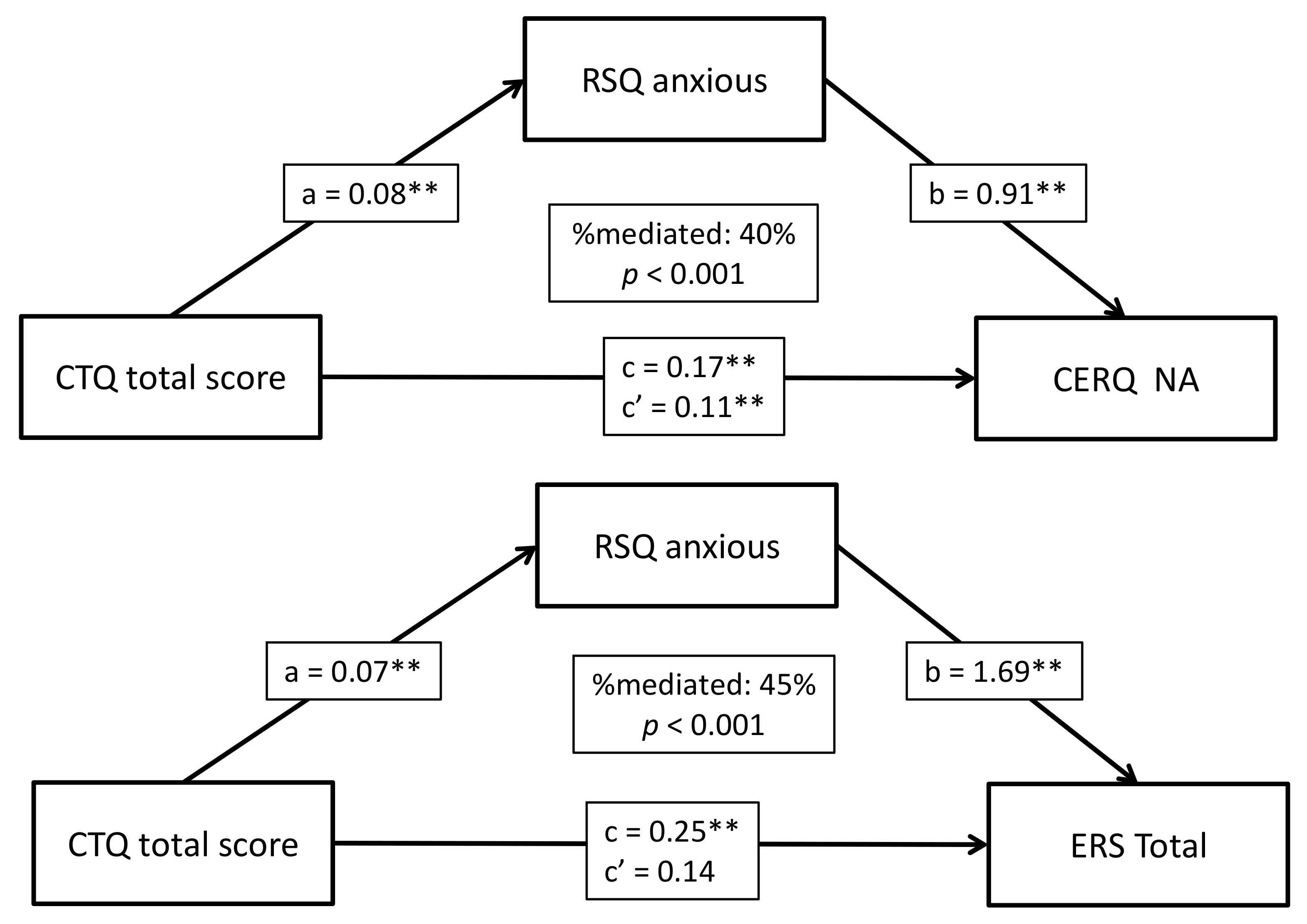
3.5. Mediation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dvir, Y.; Ford, J.D.; Hill, M.; Frazier, J.A. Childhood maltreatment, emotional dysregulation, and psychiatric comorbidities. Harv. Rev. Psychiatry 2014, 22, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Burns, E.E.; Jackson, J.L.; Harding, H.G. Child maltreatment, emotion regulation, and posttraumatic stress: The impact of emotional abuse. J. Aggress. Maltreat. Trauma 2010, 19, 801–819. [Google Scholar] [CrossRef]
- O’Mahen, H.A.; Karl, A.; Moberly, N.; Fedock, G. The association between childhood maltreatment and emotion regulation: Two different mechanisms contributing to depression? J. Affect. Disord. 2015, 174, 287–295. [Google Scholar] [CrossRef]
- Zanarini, M.C.; Frankenburg, F.R. Pathways to the development of borderline personality disorder. J. Pers. Disord. 1997, 11, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Bradley, R.; Jenei, J.; Westen, D. Etiology of borderline personality disorder: Disentangling the contributions of intercorrelated antecedents. J. Nerv. Ment. Dis. 2005, 193, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvo, N.; Lara, B.; Serrat, L.; Pérez-Rodríguez, V.; Andión, Ò.; Ramos-Quiroga, J.A.; Ferrer, M. The role of environmental influences in the complex relationship between borderline personality disorder and attention-deficit/hyperactivity disorder: Review of recent findings. Bord. Pers. Disord. Emot. Dysregul. 2020, 7, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Jennissen, S.; Holl, J.; Mai, H.; Wolff, S.; Barnow, S. Emotion dysregulation mediates the relationship between child maltreatment and psychopathology: A structural equation model. Child Abus. Negl. 2016, 62, 51–62. [Google Scholar] [CrossRef]
- Capusan, A.J.; Kuja-Halkola, R.; Bendtsen, P.; Viding, E.; McCrory, E.; Marteinsdottir, I.; Larsson, H. Childhood maltreatment and attention deficit hyperactivity disorder symptoms in adults: A large twin study. Psychol. Med. 2016, 46, 2637–2646. [Google Scholar] [CrossRef]
- Rucklidge, J.J.; Brown, D.L.; Crawford, S.; Kaplan, B.J. Retrospective reports of childhood trauma in adults with ADHD. J. Atten. Disord. 2006, 9, 631–641. [Google Scholar] [CrossRef]
- Ford, J.D.; Courtois, C.A. Treating Complex Traumatic Stress Disorders in Children and Adolescents: Scientific Foundations and Therapeutic Models; The Guilford Press: New York, NY, USA, 2013; 368p. [Google Scholar]
- Keyes, K.M.; Eaton, N.R.; Krueger, R.F.; McLaughlin, K.A.; Wall, M.M.; Grant, B.F.; Hasin, D.S. Childhood maltreatment and the structure of common psychiatric disorders. Br. J. Psychiatry 2012, 200, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.G.; Cohen, P.; Brown, J.; Smailes, E.M.; Bernstein, D.P. Childhood maltreatment increases risk for personality disorders during early adulthood. Arch. Gen. Psychiatry 1999, 56, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Kefeli, M.C.; Turow, R.G.; Yıldırım, A.; Boysan, M. Childhood maltreatment is associated with attachment insecurities, dissociation and alexithymia in bipolar disorder. Psychiatry Res. 2018, 260, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.D.; Courtois, C.A. Complex PTSD, affect dysregulation, and borderline personality disorder. Bord. Pers. Disord. Emot. Dysregul. 2014, 1, 9. [Google Scholar] [CrossRef] [Green Version]
- Golier, J.A.; Yehuda, R.; Bierer, L.M.; Mitropoulou, V.; New, A.S.; Schmeidler, J.; Silverman, J.M.; Siever, L.J. The relationship of borderline personality disorder to posttraumatic stress disorder and traumatic events. Am. J. Psychiatry 2003, 160, 2018–2024. [Google Scholar] [CrossRef] [PubMed]
- Euler, S.; Stalujanis, E.; Lindenmeyer, H.J.; Nicastro, R.; Kramer, U.; Perroud, N.; Weibel, S. Impact of childhood maltreatment in borderline personality disorder on treatment response to intensive dialectical behavior therapy. J. Pers. Disord. 2021, 35, 428–446. [Google Scholar] [CrossRef]
- Kaess, M.; Brunner, R.; Chanen, A. Borderline personality disorder in adolescence. Pediatrics 2014, 134, 782–793. [Google Scholar] [CrossRef] [Green Version]
- Russell, T.D.; Veith, A.; King, A.R. Childhood maltreatment predictors of trait impulsivity. In Advances in Psychology Research; NOVA: Hauppauge, NY, USA, 2015. [Google Scholar]
- Fossati, A.; Gratz, K.L.; Somma, A.; Maffei, C.; Borroni, S. The mediating role of emotion dysregulation in the relations between childhood trauma history and adult attachment and borderline personality disorder features: A study of Italian nonclinical participants. J. Pers. Disord. 2016, 30, 653–676. [Google Scholar] [CrossRef]
- Lobbestael, J.; Arntz, A.; Bernstein, D.P. Disentangling the relationship between different types of childhood maltreatment and personality disorders. J. Pers. Disord. 2010, 24, 285–295. [Google Scholar] [CrossRef]
- Martín-Blanco, A.; Soler, J.; Villalta, L.; Feliu-Soler, A.; Elices, M.; Pérez, V.; Arranz, M.J.; Ferraz, L.; Álvarez, E.; Pascual, J.C. Exploring the interaction between childhood maltreatment and temperamental traits on the severity of borderline personality disorder. Compr. Psychiatry 2014, 55, 311–318. [Google Scholar] [CrossRef]
- González, R.A.; Vélez-Pastrana, M.; McCrory, E.; Kallis, C.; Aguila, J.; Canino, G.; Bird, H. Evidence of concurrent and prospective associations between early maltreatment and ADHD through childhood and adolescence. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 671–682. [Google Scholar] [CrossRef] [Green Version]
- Sanderud, K.; Murphy, S.; Elklit, A. Child maltreatment and ADHD symptoms in a sample of young adults. Eur. J. Psychotraumatol. 2016, 7, 32061. [Google Scholar] [CrossRef] [Green Version]
- Becker-Blease, K.A.; Freyd, J.J. A preliminary study of ADHD symptoms and correlates: Do abused children differ from nonabused children? J. Aggress. Maltreat. Trauma 2008, 17, 133–140. [Google Scholar] [CrossRef]
- Briscoe-Smith, A.M.; Hinshaw, S.P. Linkages between child abuse and attention-deficit/hyperactivity disorder in girls: Behavioral and social correlates. Child Abus. Negl. 2006, 30, 1239–1255. [Google Scholar] [CrossRef] [Green Version]
- Stern, A.; Agnew-Blais, J.; Danese, A.; Fisher, H.L.; Jaffee, S.R.; Matthews, T.; Polanczyk, G.V.; Arseneault, L. Associations between abuse/neglect and ADHD from childhood to young adulthood: A prospective nationally-representative twin study. Child Abus. Negl. 2018, 81, 274–285. [Google Scholar] [CrossRef]
- Gokten, E.S.; Duman, N.S.; Soylu, N.; Uzun, M.E. Effects of attention-deficit/hyperactivity disorder on child abuse and neglect. Child Abus. Negl. 2016, 62, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Krause-Utz, A.; Erol, E.; Brousianou, A.V.; Cackowski, S.; Paret, C.; Ende, G.; Elzinga, B. Self-reported impulsivity in women with borderline personality disorder: The role of childhood maltreatment severity and emotion regulation difficulties. Bord. Pers. Disord. Emot. Dysregul. 2019, 6, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunford, N.; Wymbs, B.T.; Dawson, A.E.; Shorey, R.C. Childhood maltreatment, emotional lability, and alcohol problems in young adults at-risk for ADHD: Testing moderation and moderated moderation. J. Psychoact. Drugs 2017, 49, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Matthies, S.D.; Philipsen, A. Common ground in attention deficit hyperactivity disorder (ADHD) and borderline personality disorder (BPD)—Review of recent findings. Bord. Pers. Disord. Emot. Dysregul. 2014, 1, 3. [Google Scholar] [CrossRef] [Green Version]
- Clayton, K.; Lee, J.B.; Cheung, K.; Theule, J.; Henrikson, B. Quantifying the relationship between attention-deficit/hyperactivity disorder and experiences of child maltreatment: A meta-analysis. Child Abus. Rev. 2018, 27, 361–377. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef]
- Gaher, R.M.; Hofman, N.L.; Simons, J.S.; Hunsaker, R. Emotion regulation deficits as mediators between trauma exposure and borderline symptoms. Cogn. Ther. Res. 2013, 37, 466–475. [Google Scholar] [CrossRef]
- Corbisiero, S.; Mörstedt, B.; Bitto, H.; Stieglitz, R.-D. Emotional dysregulation in adults with attention-deficit/hyperactivity disorder-validity, predictability, severity, and comorbidity. J. Clin. Psychol. 2017, 73, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Beheshti, A.; Chavanon, M.-L.; Christiansen, H. Emotion dysregulation in adults with attention deficit hyperactivity disorder: A meta-analysis. BMC Psychiatry 2020, 20, 120. [Google Scholar] [CrossRef] [Green Version]
- Rüfenacht, E.; Euler, S.; Prada, P.; Nicastro, R.; Dieben, K.; Hasler, R.; Pham, E.; Perroud, N.; Weibel, S. Emotion dysregulation in adults suffering from attention deficit hyperactivity disorder (ADHD), a comparison with borderline personality disorder (BPD). Bord. Pers. Disord. Emot. Dysregul. 2019, 6, 11. [Google Scholar] [CrossRef] [Green Version]
- Pollak, S.D.; Cicchetti, D.; Hornung, K.; Reed, A. Recognizing emotion in faces: Developmental effects of child abuse and neglect. Dev. Psychol. 2000, 36, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Shipman, K.L.; Schneider, R.; Fitzgerald, M.M.; Sims, C.; Swisher, L.; Edwards, A. Maternal emotion socialization in maltreating and non-maltreating families: Implications for children’s emotion regulation. Soc. Dev. 2007, 16, 268–285. [Google Scholar] [CrossRef]
- Thompson, R.A. Emotion regulation: A theme in search of definition. Monogr. Soc. Res. Child. Dev. 1994, 59, 25–52. [Google Scholar] [CrossRef]
- Kim, J.; Cicchetti, D. Longitudinal pathways linking child maltreatment, emotion regulation, peer relations, and psychopathology. J. Child Psychol. Psychiatry 2009, 51, 706–716. [Google Scholar] [CrossRef] [Green Version]
- Shipman, K.; Zeman, J.; Penza, S.; Champion, K. Emotion management skills in sexually maltreated and nonmaltreated girls: A developmental psychopathology perspective. Dev. Psychopathol. 2000, 12, 47–62. [Google Scholar] [CrossRef]
- Shipman, K.L.; Zeman, J. Socialization of children’s emotion regulation in mother-child dyads: A developmental psychopathology perspective. Dev. Psychopathol. 2001, 13, 317–336. [Google Scholar] [CrossRef]
- Weissman, D.G.; Bitran, D.; Miller, A.B.; Schaefer, J.D.; Sheridan, M.A.; McLaughlin, K.A. Difficulties with emotion regulation as a transdiagnostic mechanism linking child maltreatment with the emergence of psychopathology. Dev. Psychopathol. 2019, 31, 899–915. [Google Scholar] [CrossRef]
- Fernando, S.C.; Beblo, T.; Schlosser, N.; Terfehr, K.; Otte, C.; Löwe, B.; Wolf, O.T.; Spitzer, C.; Driessen, M.; Wingenfeld, K. The impact of self-reported childhood trauma on emotion regulation in borderline personality disorder and major depression. J. Trauma Dissociation 2014, 15, 384–401. [Google Scholar] [CrossRef]
- Ehring, T.; Quack, D. Emotion regulation difficulties in trauma survivors: The role of trauma type and PTSD symptom severity. Behav. Ther. 2010, 41, 587–598. [Google Scholar] [CrossRef] [PubMed]
- Gruhn, M.A.; Compas, B.E. Effects of maltreatment on coping and emotion regulation in childhood and adolescence: A meta-analytic review. Child Abus. Negl. 2020, 103, 104446. [Google Scholar] [CrossRef]
- Fonagy, P.; Luyten, P. A developmental, mentalization-based approach to the understanding and treatment of borderline personality disorder. Dev. Psychopathol. 2009, 21, 1355–1381. [Google Scholar] [CrossRef] [PubMed]
- Fonagy, P.; Gergely, G.; Jurist, E.L.; Target, M. Affect Regulation, Mentalization, and the Development of the Self; Routledge: Millton, UK, 2018. [Google Scholar]
- Chiesa, M.; Fonagy, P. Reflective function as a mediator between childhood adversity, personality disorder and symptom distress. Pers. Ment. Health 2014, 8, 52–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Lacharité, C.; Muzik, M. The protective role of mentalizing: Reflective functioning as a mediator between child maltreatment, psychopathology and parental attitude in expecting parents. Child Abus. Negl. 2019, 95, 104065. [Google Scholar] [CrossRef]
- Bateman, A.; Fonagy, P. Mentalization based treatment for borderline personality disorder. World Psychiatry 2010, 9, 11–15. [Google Scholar] [CrossRef]
- Davila, J.; Ramsay, M.; Stroud, C.B.; Steinberg, S.J. Attachment as vulnerability to the development of psychopathology. In Development of Psychopathology: A Vulnerability-Stress Perspective; Sage Publications: Thousand Oaks, CA, USA, 2005; pp. 215–242. [Google Scholar]
- Pascuzzo, K.; Moss, E.; Cyr, C. Attachment and emotion regulation strategies in predicting adult psychopathology. SAGE Open 2015, 5, 2158244015604695. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R. An attachment perspective on psychopathology. World Psychiatry 2012, 11, 11–15. [Google Scholar] [CrossRef]
- Lyons-Ruth, K. Contributions of the mother-infant relationship to dissociative, borderline, and conduct symptoms in young adulthood. Child Adolesc. Soc. Work. J. 2008, 29, 203–218. [Google Scholar] [CrossRef] [Green Version]
- Baer, J.C.; Martinez, C.D. Child maltreatment and insecure attachment: A meta-analysis. J. Reprod. Infant Psychol. 2006, 24, 187–197. [Google Scholar] [CrossRef]
- Agrawal, H.R.; Gunderson, J.; Holmes, B.M.; Lyons-Ruth, K. Attachment studies with borderline patients: A review. Harv. Rev. Psychiatry 2004, 12, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Levy, K.N. The implications of attachment theory and research for understanding borderline personality disorder. Dev. Psychopathol. 2005, 17, 959–986. [Google Scholar] [CrossRef]
- Fonagy, P.; Target, M.; Gergely, G.; Allen, J.G.; Bateman, A.W. The developmental roots of borderline personality disorder in early attachment relationships: A theory and some evidence. Psychoanal. Inq. 2003, 23, 412–459. [Google Scholar] [CrossRef]
- Minzenberg, M.J.; Poole, J.H.; Vinogradov, S. Adult social attachment disturbance is related to childhood maltreatment and current symptoms in borderline personality disorder. J. Nerv. Ment. Dis. 2006, 194, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Liu, Z.; Liu, Q.; Chu, J.; Zheng, K.; Wang, J.; Wei, H.; Zhong, M.; Ling, Y.; Yi, J. Insecure attachment and maladaptive emotion regulation mediating the relationship between childhood trauma and borderline personality features. Depress. Anxiety 2021, 38, 28–39. [Google Scholar] [CrossRef]
- Godbout, N.; Daspe, M.È.; Runtz, M.; Cyr, G.; Briere, J. Childhood maltreatment, attachment, and borderline personality-related symptoms: Gender-specific structural equation models. Psychol. Trauma Theory Res. Pract. Policy 2019, 11, 90–98. [Google Scholar] [CrossRef]
- Crow, T.M.; Levy, K.N. Adult attachment anxiety moderates the relation between self-reported childhood maltreatment and borderline personality disorder features. Pers. Ment. Health 2019, 13, 239–249. [Google Scholar] [CrossRef]
- Scott, L.N.; Kim, Y.; Nolf, K.A.; Hallquist, M.N.; Wright, A.G.C.; Stepp, S.; Morse, J.Q.; Pilkonis, P.A. Preoccupied attachment and emotional dysregulation: Specific aspects of borderline personality disorder or general dimensions of personality pathology? J. Pers. Disord. 2013, 27, 473–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storebø, O.J.; Rasmussen, P.D.; Simonsen, E. Association between insecure attachment and ADHD: Environmental mediating factors. J. Atten. Disord. 2013, 20, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Kissgen, R.; Franke, S. An attachment research perspective on ADHD. Neuropsychiatrie 2016, 30, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentzler, A.L.; Kerns, K.A.; Keener, E. Emotional reactions and regulatory responses to negative and positive events: Associations with attachment and gender. Motiv. Emot. 2010, 34, 78–92. [Google Scholar] [CrossRef]
- Fraley, R.C.; Shaver, P.R. Adult attachment and the suppression of unwanted thoughts. J. Personal. Soc. Psychol. 1997, 73, 1080–1091. [Google Scholar] [CrossRef]
- Mikulincer, M.; Orbach, I. Attachment styles and repressive defensiveness: The accessibility and architecture of affective memories. J. Personal. Soc. Psychol. 1995, 68, 917–925. [Google Scholar] [CrossRef]
- Davis, D.; Shaver, P.R.; Vernon, M.L. Physical, emotional, and behavioral reactions to breaking up: The roles of gender, age, emotional involvement, and attachment style. Pers. Soc. Psychol. Bull. 2003, 29, 871–884. [Google Scholar] [CrossRef]
- Collins, N.L. Working models of attachment: Implications for explanation, emotion and behavior. J. Pers. Soc. Psychol. 1996, 71, 810–832. [Google Scholar] [CrossRef]
- Philipsen, A. Differential diagnosis and comorbidity of attention-deficit/hyperactivity disorder (ADHD) and borderline personality disorder (BPD) in adults. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, i42–i46. [Google Scholar] [CrossRef]
- Ramos-Quiroga, J.A.; Nasillo, V.; Richarte, V.; Corrales, M.; Palma, F.; Ibáñez, P.; Michelsen, M.; Van de Glind, G.; Casas, M.; Kooij, J.S. Criteria and concurrent validity of DIVA 2.0: A semi-structured diagnostic interview for adult ADHD. J. Atten. Disord. 2019, 23, 1126–1135. [Google Scholar] [CrossRef]
- First, M.B.; Gibbon, M. The structured clinical interview for DSM-IV axis I disorders (SCID-I) and the structured clinical interview for DSM-IV axis II disorders (SCID-II). In Comprehensive Handbook of Psychological Assessment; Vol. 2: Personality Assessment; John Wiley and Sons: Hoboken, NJ, USA, 2004; pp. 134–143. [Google Scholar]
- Caci, H.M.; Bouchez, J.; Baylé, F.J. An aid for diagnosing attention-deficit/hyperactivity disorder at adulthood: Psychometric properties of the French versions of two wender utah rating scales (WURS-25 and WURS-K). Compr. Psychiatry 2010, 51, 325–331. [Google Scholar] [CrossRef]
- Caci, H.; Morin, A.; Tran, A. Prevalence and correlates of attention deficit hyperactivity disorder in adults from a french community sample. J. Nerv. Ment. Dis. 2014, 202, 324–332. [Google Scholar] [CrossRef] [Green Version]
- Nicastro, R.; Prada, P.; Kung, A.-L.; Salamin, V.; Dayer, A.; Aubry, J.-M.; Guenot, F.; Perroud, N. Psychometric properties of the French borderline symptom list, short form (BSL-23). Bord. Pers. Disord. Emot. Dysregul. 2016, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Faraone, S.V.; Biederman, J.; Mick, E. The age-dependent decline of attention deficit hyperactivity disorder: A meta-analysis of follow-up studies. Psychol. Med. 2005, 36, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Moffitt, T.E.; Houts, R.; Asherson, P.; Belsky, D.W.; Corcoran, D.L.; Hammerle, M.; Harrington, H.; Hogan, S.; Meier, M.H.; Polanczyk, G.V.; et al. Is adult ADHD a childhood-onset neurodevelopmental disorder? Evidence from a four-decade longitudinal cohort study. Am. J. Psychiatry 2015, 172, 967–977. [Google Scholar] [CrossRef] [PubMed]
- Lannoy, S.; Heeren, A.; Rochat, L.; Rossignol, M.; Van der Linden, M.; Billieux, J. Is there an all-embracing construct of emotion reactivity? Adaptation and validation of the emotion reactivity scale among a French-speaking community sample. Compr. Psychiatry 2014, 55, 1960–1967. [Google Scholar] [CrossRef] [PubMed]
- Jermann, F.; Van Der Linden, M.; D’Acremont, M.; Zermatten, A. Cognitive emotion regulation questionnaire (CERQ). Eur. J. Psychol. Assess. 2006, 22, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, D.P.; Stein, J.A.; Newcomb, M.D.; Walker, E.; Pogge, D.; Ahluvalia, T.; Stokes, J.; Handelsman, L.; Medrano, M.; Desmond, D.; et al. Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abus. Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef]
- Griffin, D.W.; Bartholomew, K. Models of the self and other: Fundamental dimensions underlying measures of adult attachment. J. Personal. Soc. Psychol. 1994, 67, 430–445. [Google Scholar] [CrossRef]
- Simpson, J.A.; Rholes, W.S.; Nelligan, J.S. Support seeking and support giving within couples in an anxiety-provoking situation: The role of attachment styles. J. Personal. Soc. Psychol. 1992, 62, 434–446. [Google Scholar] [CrossRef]
- Hicks, R.; Tingley, D. Causal mediation analysis. Stata J. 2011, 11, 605–619. [Google Scholar] [CrossRef] [Green Version]
- Glaser, J.-P.; van Os, J.; Portegijs, P.J.; Myin-Germeys, I. Childhood trauma and emotional reactivity to daily life stress in adult frequent attenders of general practitioners. J. Psychosom. Res. 2006, 61, 229–236. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, K.A.; Kubzansky, L.D.; Dunn, E.; Waldinger, R.; Vaillant, G.; Koenen, K. Childhood social environment, emotional reactivity to stress, and mood and anxiety disorders across the life course. Depress. Anxiety 2010, 27, 1087–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poole, J.C.; Dobson, K.; Pusch, D. Do adverse childhood experiences predict adult interpersonal difficulties? The role of emotion dysregulation. Child Abus. Negl. 2018, 80, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Gratz, K.L.; Tull, M.T.; Baruch, D.E.; Bornovalova, M.A.; Lejuez, C. Factors associated with co-occurring borderline personality disorder among inner-city substance users: The roles of childhood maltreatment, negative affect intensity/reactivity, and emotion dysregulation. Compr. Psychiatry 2008, 49, 603–615. [Google Scholar] [CrossRef]
- Kuo, J.R.; Khoury, J.E.; Metcalfe, R.; Fitzpatrick, S.; Goodwill, A. An examination of the relationship between childhood emotional abuse and borderline personality disorder features: The role of difficulties with emotion regulation. Child Abus. Negl. 2015, 39, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Rosenstein, L.K.; Ellison, W.D.; Walsh, E.; Chelminski, I.; Dalrymple, K.; Zimmerman, M. The role of emotion regulation difficulties in the connection between childhood emotional abuse and borderline personality features. Pers. Disord. Theory Res. Treat. 2018, 9, 590–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heleniak, C.; Jenness, J.L.; Stoep, A.V.; McCauley, E.; McLaughlin, K.A. Childhood maltreatment exposure and disruptions in emotion regulation: A transdiagnostic pathway to adolescent internalizing and externalizing psychopathology. Cogn. Ther. Res. 2016, 40, 394–415. [Google Scholar] [CrossRef] [Green Version]
- Huh, H.J.; Kim, K.H.; Lee, H.-K.; Chae, J.-H. The relationship between childhood trauma and the severity of adulthood depression and anxiety symptoms in a clinical sample: The mediating role of cognitive emotion regulation strategies. J. Affect. Disord. 2017, 213, 44–50. [Google Scholar] [CrossRef]
- Seligowski, A.V.; Lee, D.; Bardeen, J.R.; Orcutt, H.K. Emotion regulation and posttraumatic stress symptoms: A meta-analysis. Cogn. Behav. Ther. 2014, 44, 87–102. [Google Scholar] [CrossRef]
- Krause, E.D.; Mendelson, T.; Lynch, T.R. Childhood emotional invalidation and adult psychological distress: The mediating role of emotional inhibition. Child Abus. Negl. 2003, 27, 199–213. [Google Scholar] [CrossRef]
- Ensink, K.; Borelli, J.L.; Normandin, L.; Target, M.; Fonagy, P. Childhood sexual abuse and attachment insecurity: Associations with child psychological difficulties. Am. J. Orthopsychiatry 2020, 90, 115–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Styron, T.; Janoff-Bulman, R. Childhood attachment and abuse: Long-term effects on adult attachment, depression, and conflict resolution. Child Abus. Negl. 1997, 21, 1015–1023. [Google Scholar] [CrossRef]
- Unger, J.A.M.; De Luca, R.V. The relationship between childhood physical abuse and adult attachment styles. J. Fam. Violence 2014, 29, 223–234. [Google Scholar] [CrossRef]
- Riggs, S.A.; Kaminski, P. Childhood emotional abuse, adult attachment, and depression as predictors of relational adjustment and psychological aggression. J. Aggress. Maltreat. Trauma 2010, 19, 75–104. [Google Scholar] [CrossRef]
- Widom, C.S.; Czaja, S.J.; Kozakowski, S.S.; Chauhan, P. Does adult attachment style mediate the relationship between childhood maltreatment and mental and physical health outcomes? Child Abus. Negl. 2018, 76, 533–545. [Google Scholar] [CrossRef]
- Hankin, B.L.; Kassel, J.D.; Abela, J.R.Z. Adult attachment dimensions and specificity of emotional distress symptoms: Prospective investigations of cognitive risk and interpersonal stress generation as mediating mechanisms. Pers. Soc. Psychol. Bull. 2005, 31, 136–151. [Google Scholar] [CrossRef]
- Illing, V.; Tasca, G.A.; Balfour, L.; Bissada, H. Attachment insecurity predicts eating disorder symptoms and treatment outcomes in a clinical sample of women. J. Nerv. Ment. Dis. 2010, 198, 653–659. [Google Scholar] [CrossRef]
- Lee, A.; Hankin, B.L. Insecure attachment, dysfunctional attitudes, and low self-esteem predicting prospective symptoms of depression and anxiety during adolescence. J. Clin. Child Adolesc. Psychol. 2009, 53, 219–231. [Google Scholar] [CrossRef]
- Kerns, K.A.; Brumariu, L.E. Is insecure parent-child attachment a risk factor for the development of anxiety in childhood or adolescence? Child Dev. Perspect. 2014, 8, 12–17. [Google Scholar] [CrossRef]
- Oshri, A.; Sutton, T.E.; Clay-Warner, J.; Miller, J.D. Child maltreatment types and risk behaviors: Associations with attachment style and emotion regulation dimensions. Pers. Individ. Differ. 2015, 73, 127–133. [Google Scholar] [CrossRef]
- Hankin, B.L. Childhood maltreatment and psychopathology: Prospective tests of attachment, cognitive vulnerability, and stress as mediating processes. Cogn. Ther. Res. 2005, 29, 645–671. [Google Scholar] [CrossRef]
- Thompson, K.N.; Jackson, H.; Cavelti, M.; Betts, J.; McCutcheon, L.; Jovev, M.; Chanen, A.M. The clinical significance of subthreshold borderline personality disorder features in outpatient youth. J. Pers. Disord. 2019, 33, 71–81. [Google Scholar] [CrossRef]
- Balázs, J.; Keresztény, Á. Subthreshold attention deficit hyperactivity in children and adolescents: A systematic review. Eur. Child Adolesc. Psychiatry 2014, 23, 393–408. [Google Scholar] [CrossRef] [PubMed]
- Pham, E.; Aouidad, A.; Edan, A.; Perroud, N.; Piguet, C. Diagnosing borderline personality disorder in adolescence: A French review. Neuropsychiatr. L’enfance L’adolescence 2021, 69, 185–189. [Google Scholar] [CrossRef]


{kind=link}
| ADHD | BPD | BPD + ADHD | Cont. | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N = 279 | N = 70 | N = 60 | N = 61 | |||||||
| Mean or N | SD or % | Mean or N | SD or % | Mean or N | SD or % | Mean or N | SD or % | p | ||
| Age | 35.49 | 12.86 | 31.66 | 9.08 | 30.29 | 8.64 | 35.24 | 12.29 | 0.005 | |
| Gender | Female | 122 | 43.73 | 66 | 94.29 | 55 | 91.67 | 34 | 55.74 | <0.001 |
| Civil status * | Single (vs. not single) | 130 | 49.24 | 36 | 51.43 | 33 | 57.89 | 31 | 52.54 | 0.84 |
| Children * | 0 | 163 | 61.74 | 46 | 65.71 | 43 | 74.14 | 39 | 66.1 | 0.11 |
| 1 | 28 | 10.61 | 13 | 18.57 | 7 | 12.07 | 6 | 10.17 | ||
| ≥2 | 73 | 27.65 | 11 | 15.71 | 8 | 13.79 | 14 | 23.73 | ||
| Job * | Yes (vs. no) | 157 | 61.33 | 30 | 42.86 | 26 | 48.15 | 27 | 45.76 | 0.026 |
| Years of education * | 15.52 | 2.86 | 15.23 | 3.18 | 14.87 | 2.69 | 15.76 | 3.2 | 0.236 | |
| Lifetime comorbidities | Major depressive disorder | 126 | 45.16 | 58 | 82.86 | 42 | 70 | 16 | 26.23 | <0.001 |
| Bipolar disorder | 6 | 2.15 | 7 | 10 | 6 | 10 | 0 | 0 | 0.001 | |
| Anxiety disorder ** | 57 | 20.43 | 58 | 82.86 | 33 | 55 | 9 | 14.75 | <0.001 | |
| Eating disorders | 10 | 3.58 | 15 | 21.43 | 11 | 18.33 | 4 | 6.56 | <0.001 | |
| Substance use disorder | 71 | 25.45 | 24 | 34.29 | 24 | 40 | 3 | 4.92 | <0.001 | |
| ERS | Sensitivity | 22.31 | 8.78 | 29.23 | 7.77 | 31.26 | 5.95 | 19.49 | 9.36 | <0.001 |
| Arousal/Intensity | 15.84 | 7.06 | 22.07 | 5.65 | 22.86 | 4.49 | 13.07 | 7.39 | <0.001 | |
| Persistence | 9.23 | 3.78 | 11.71 | 3.26 | 12.5 | 2.7 | 8.13 | 3.91 | <0.001 | |
| Total | 47.38 | 18.39 | 63.01 | 15.61 | 66.61 | 12.1 | 40.69 | 19.63 | <0.001 | |
| CERQ | Self-blame | 11.53 | 3.75 | 13.82 | 3.56 | 14.06 | 3.6 | 11.88 | 4.23 | <0.001 |
| Acceptance | 12.83 | 3.38 | 13.12 | 3.46 | 13.38 | 3.44 | 13.38 | 3.60 | 0.578 | |
| Rumination | 12.94 | 3.86 | 14.36 | 3.87 | 14.79 | 3.54 | 13.09 | 3.92 | 0.001 | |
| Positive refocusing | 9 | 3.68 | 7.71 | 3.63 | 7.39 | 3.17 | 8.75 | 4.10 | 0.004 | |
| Refocusing on planning | 12.94 | 3.63 | 10.82 | 3.93 | 11.65 | 3.53 | 13.42 | 3.72 | <0.001 | |
| Positive reappraisal | 12.45 | 3.89 | 10.07 | 4.12 | 10.53 | 3.56 | 12.17 | 4.27 | <0.001 | |
| Putting into perspective | 12.27 | 3.82 | 10.76 | 3.83 | 10.81 | 3.66 | 12.32 | 3.93 | 0.002 | |
| Catastrophizing | 8.66 | 3.6 | 10.27 | 3.86 | 10.79 | 3.93 | 8.88 | 3.47 | <0.001 | |
| Blaming others | 8.84 | 3.53 | 9.49 | 3.88 | 10.61 | 3.6 | 8.83 | 3.54 | 0.001 | |
| Total: Adaptive strategies | 59.49 | 13.29 | 52.58 | 14.02 | 53.76 | 11.86 | 60.03 | 15.60 | <0.001 | |
| Total: Non-adaptive strategies | 41.97 | 10.66 | 47.93 | 10.8 | 50.57 | 10.32 | 42.67 | 10.78 | <0.001 | |
| RSQ | Avoidant | 21.89 | 4.19 | 22.49 | 4.34 | 22.30 | 4.18 | 22.47 | 3.62 | 0.59 |
| Anxious | 13.80 | 4.13 | 17.37 | 4.23 | 16.96 | 3.13 | 13.95 | 4.18 | <0.001 | |
| Secure | 16.81 | 3.06 | 16.55 | 3.70 | 17.64 | 3.06 | 16.87 | 2.94 | 0.25 | |
| CTQ | Emotional abuse | 10.89 | 5.33 | 15.18 | 5.60 | 16.03 | 5.88 | 10.25 | 5.16 | <0.001 |
| Physical abuse | 7.03 | 3.38 | 8.57 | 4.92 | 9.01 | 5.25 | 6.20 | 2.04 | <0.001 | |
| Sexual abuse | 5.91 | 2.76 | 9.02 | 6.23 | 8.55 | 6.05 | 6.62 | 3.69 | <0.001 | |
| Emotional neglect | 12.79 | 4.94 | 15.30 | 4.63 | 15.43 | 5.33 | 12.03 | 5.09 | <0.001 | |
| Physical neglect | 7.82 | 3.03 | 9.20 | 3.92 | 9.08 | 4.30 | 7.84 | 3.10 | 0.003 | |
| Total | 44.20 | 14.73 | 56.16 | 20.75 | 58.09 | 20.13 | 42.95 | 14.49 | <0.001 | |
| ADHD | BPD | BPD + ADHD | Control | All | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| b | p | b | p | b | p | b | p | b | p | ||
| ERS | Sensitivity | 0.17 | 0.012 | 0.22 | 0.018 | 0.17 | 0.022 | 0.54 | <0.001 | 0.21 | <0.001 |
| Arousal/intensity | 0.19 | 0.004 | 0.21 | 0.013 | 0.15 | 0.032 | 0.53 | <0.001 | 0.21 | <0.001 | |
| Persistence | 0.11 | 0.108 | 0.16 | 0.075 | 0.19 | 0.014 | 0.57 | <0.001 | 0.17 | <0.001 | |
| Total | 0.18 | 0.001 | 0.21 | 0.014 | 0.17 | 0.013 | 0.57 | <0.001 | 0.23 | <0.001 | |
| CERQ | Self-blame | 0.05 | 0.445 | 0.24 | 0.012 | 0.07 | 0.494 | 0.43 | 0.023 | 0.13 | 0.007 |
| Acceptance | 0.1 | 0.158 | 0.37 | <0.001 | 0.19 | 0.07 | 0.05 | 0.798 | 0.18 | <0.001 | |
| Rumination | 0.03 | 0.379 | 0.25 | 0.021 | 0.08 | 0.428 | 0.5 | 0.002 | 0.14 | 0.005 | |
| Positive refocusing | −0.04 | 0.574 | −0.07 | 0.601 | −0.09 | 0.314 | −0.4 | 0.039 | −0.09 | 0.087 | |
| Refocusing on planning | −0.22 | 0.001 | 0.08 | 0.394 | 0.03 | 0.574 | −0.29 | 0.086 | −0.1 | 0.045 | |
| Positive reappraisal | −0.09 | 0.182 | 0.01 | 0.931 | 0.03 | 0.762 | −0.38 | 0.043 | −0.07 | 0.167 | |
| Putting into perspective | −0.11 | 0.11 | 0.12 | 0.235 | −0.01 | 0.997 | −0.17 | 0.329 | −0.04 | 0.451 | |
| Catastrophizing | 0.17 | 0.018 | 0.11 | 0.306 | 0.41 | <0.001 | 0.4 | 0.011 | 0.21 | <0.001 | |
| Blaming others | 0.14 | 0.04 | 0.29 | 0.009 | 0.33 | 0.024 | 0.33 | 0.04 | 0.23 | <0.001 | |
| Total: Adaptive strategies | −0.11 | 0.129 | 0.13 | 0.236 | 0.04 | 0.664 | −0.34 | 0.091 | −0.03 | 0.472 | |
| Total: Non-adaptive strategies | 0.14 | 0.05 | 0.31 | 0.003 | 0.31 | 0.002 | 0.58 | <0.001 | 0.25 | <0.001 | |
| RSQ | Avoidant | 0.17 | 0.025 | 0.16 | 0.161 | 0.01 | 0.932 | 0.37 | 0.014 | 0.16 | 0.002 |
| Anxious | 0.27 | <0.001 | 0.24 | 0.016 | 0.22 | 0.022 | 0.36 | 0.03 | 0.27 | <0.001 | |
| Secure | −0.09 | 0.192 | −0.16 | 0.19 | −0.15 | 0.25 | −0.12 | 0.464 | −0.11 | 0.029 | |
| Emotional Abuse | Emotional Neglect | Physical Abuse | Physical Neglect | Sexual Abuse | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| b | p | b | p | b | p | b | p | b | p | ||
| ERS | Total | 0.22 | <0.001 | 0.15 | 0.001 | 0.14 | 0.001 | 0.11 | 0.009 | 0.12 | 0.004 |
| CERQ | Total–Adaptive strategies | −0.02 | 0.673 | −0.17 | <0.001 | 0.03 | 0.519 | 0.02 | 0.597 | 0.08 | 0.081 |
| Total–Non-adaptive strategies | 0.3 | <0.001 | 0.16 | 0.001 | 0.18 | <0.001 | 0.13 | 0.005 | 0.16 | 0.001 | |
| RSQ | Avoidant | 0.18 | <0.001 | 0.17 | 0.001 | 0.06 | 0.191 | 0.16 | 0.001 | 0.1 | 0.038 |
| Anxious | 0.28 | <0.001 | 0.23 | <0.001 | 0.16 | 0.001 | 0.17 | <0.001 | 0.11 | 0.02 | |
| Secure | −0.01 | 0.706 | −0.13 | 0.009 | −0.03 | 0.533 | −0.12 | 0.012 | −0.05 | 0.271 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rüfenacht, E.; Pham, E.; Nicastro, R.; Dieben, K.; Hasler, R.; Weibel, S.; Perroud, N. Link between History of Childhood Maltreatment and Emotion Dysregulation in Adults Suffering from Attention Deficit/Hyperactivity Disorder or Borderline Personality Disorder. Biomedicines 2021, 9, 1469. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9101469
Rüfenacht E, Pham E, Nicastro R, Dieben K, Hasler R, Weibel S, Perroud N. Link between History of Childhood Maltreatment and Emotion Dysregulation in Adults Suffering from Attention Deficit/Hyperactivity Disorder or Borderline Personality Disorder. Biomedicines. 2021; 9(10):1469. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9101469
Chicago/Turabian StyleRüfenacht, Eva, Eléonore Pham, Rosetta Nicastro, Karen Dieben, Roland Hasler, Sébastien Weibel, and Nader Perroud. 2021. "Link between History of Childhood Maltreatment and Emotion Dysregulation in Adults Suffering from Attention Deficit/Hyperactivity Disorder or Borderline Personality Disorder" Biomedicines 9, no. 10: 1469. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9101469