
Neoplastic Implications in Patients Suffering from Hidradenitis Suppurativa under Systemic Treatments

 , , , and
, , , and
Abstract
:1. Introduction
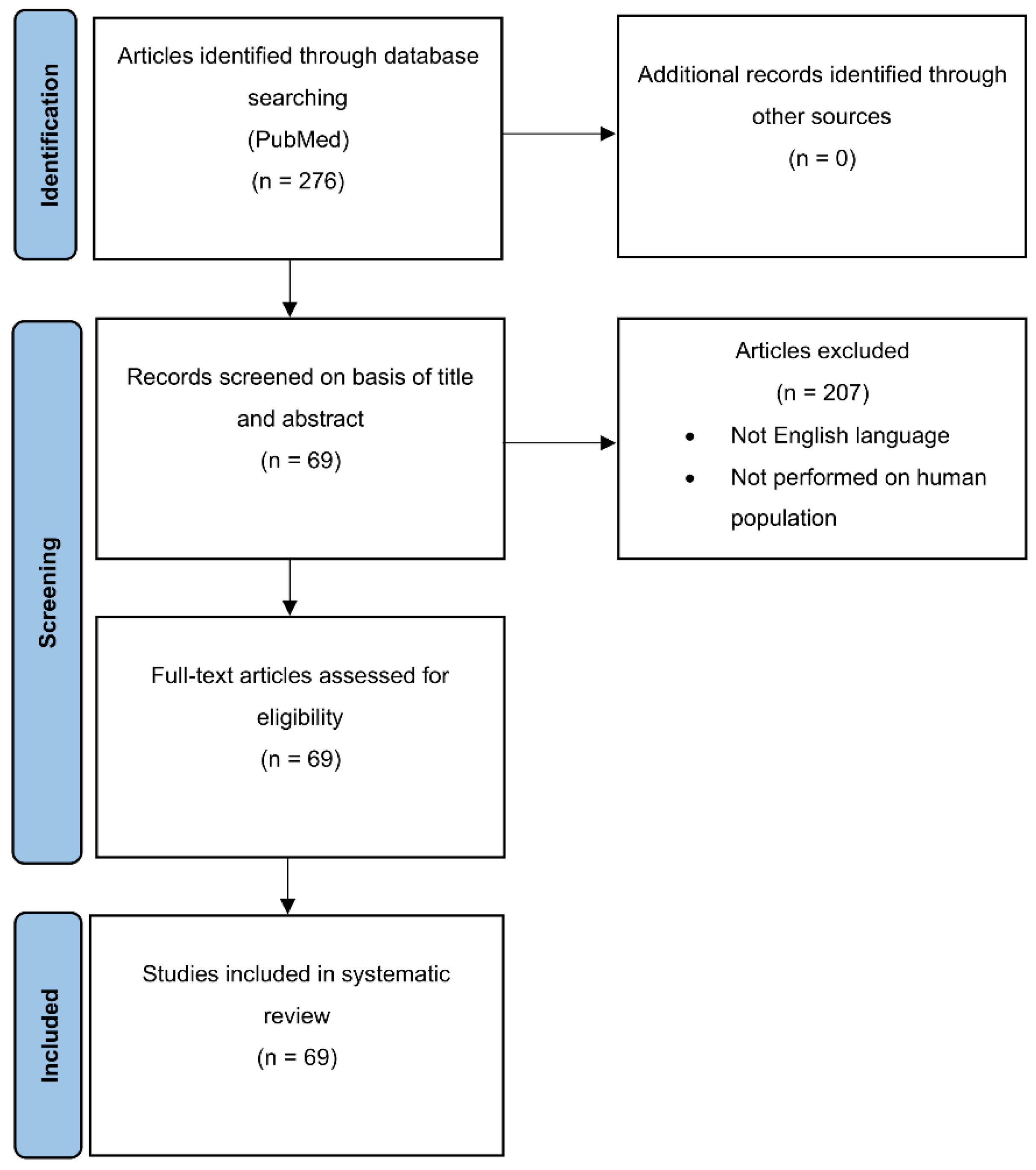
2. Materials and Methods
3. Results
4. Discussion
4.1. HS and NMSC
4.2. HS and Tumors beyond the Skin
4.3. HS and Hematological Malignancies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HS | Hidradenitis suppurativa |
| NMSC | Nonmelanoma skin cancer |
| SCC | Squamous cell carcinoma |
| IBD | Inflammatory bowel disease |
| CD | Crohn’s disease |
| HPV | Human papilloma virus |
| TNF | Tumor necrosis factor |
| MU | Marjolin ulcer |
| TNP | Topical negative pressure |
| PCR | Polymerase chain reaction |
| T1 | Primary tumor |
| DD | Dowling Degos |
| KID | Keratitis—Ichthyosis—Deafness |
| DMPM | Diffuse malignant peritoneal Mesothelioma |
| CT | Computed tomography |
| HR | Hazard Ratio |
| OCPC | Oral cavity and pharyngeal cancer |
| CNS | Central nervous system |
| HL | Hodgkin lymphoma |
| NHL | Non Hodgkin Lymphoma |
| CTCL | Cutaneous T-cell lymphoma |
| IPTCLB | Intralymphatic proliferation of T-cell lymphoid blasts |
| RTK | Receptor tyrosine kinase |
| IL | Interleukin |
| VEGF | Vascular endothelial grow factor |
| TLR | Toll-like receptor |
| CK | Cytokeratin |
References
- Peris, K.; Lo Schiavo, A.; Fabbrocini, G.; Dini, V.; Patrizi, A.; Fusano, M.; Bianchi, L.; Guanziroli, E.; Guarneri, C.; Parodi, A.; et al. HIDRAdisk: Validation of an innovative visual tool to assess the burden of hidradenitis suppurativa. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 766–773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campanati, A.; Orciani, M.; Sorgentoni, G.; Consales, V.; Offidani, A.; Di Primio, R. Pathogenetic Characteristics of Mesenchymal Stem Cells in Hidradenitis Suppurativa. JAMA Dermatol. 2018, 154, 1184–1190. [Google Scholar] [CrossRef]
- Makris, G.M.; Poulakaki, N.; Papanota, A.M.; Kotsifa, E.; Sergentanis, T.N.; Psaltopoulou, T. Vulvar, Perianal and Perineal Cancer After Hidradenitis Suppurativa: A Systematic Review and Pooled Analysis. Dermatol. Surg. 2017, 43, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.; Delgadillo, D., III; Barber, C.; Khachemoune, A. Cutaneous squamous cell carcinoma complicating hidradenitis suppurativa: A review of the prevalence, pathogenesis, and treatment of this dreaded complication. Acta Dermatovenerol. Alp. Pannonica Adriat. 2018, 27, 25–28. [Google Scholar] [CrossRef]
- Vekic, D.A.; Cains, G.D. Hidradenitis suppurativa, a review of pathogenesis, associations and management. Part 2. Australas. J. Dermatol. 2018, 59, 261–266. [Google Scholar] [CrossRef]
- Miller, I.M.; McAndrew, R.J.; Hamzavi, I. Prevalence, Risk Factors, and Comorbidities of Hidradenitis Suppurativa. Dermatol. Clin. 2016, 34, 7–16. [Google Scholar] [CrossRef]
- Dattilo, G.; Borgia, F.; Guarneri, C.; Casale, M.; Bitto, R.; Morabito, C.; Signorelli, S.; Katsiki, N.; Cannavò, S.P. Cardiovascular Risk in Psoriasis: Current State of the Art. Curr. Vasc. Pharmacol. 2019, 17, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Martina, E.; Campanati, A.; Giuliodori, K.; Offidani, A. Hidradenitis suppurativa in Crohn’s disease during adalimumab therapy: A paradox? Acta Dermatovenerol. Alp. Pannonica Adriat. 2017, 26, 21–23. [Google Scholar] [CrossRef]
- Lapins, J.; Ye, W.; Nyrén, O.; Emtestam, L. Incidence of cancer among patients with hidradenitis suppurativa. Arch. Dermatol. 2001, 137, 730–734. [Google Scholar] [PubMed]
- Crisafulli, S.; Bertino, L.; Fontana, A.; Calapai, F.; Ingrasciotta, Y.; Berretta, M.; Trifirò, G.; Guarneri, C. Incidence of Skin Cancer in Patients with Chronic Inflammatory Cutaneous Diseases on Targeted Therapies: A Systematic Review and Meta-Analysis of Observational Studies. Front. Oncol. 2021, 11, 687432. [Google Scholar] [CrossRef] [PubMed]
- Sidwell, K. Lucian A Selection. Ed. and trM.D. Macleod. Warminster: Aris and Phillips, 1991. Pp. Iv + 316. £35.00 (Bound), £12.50 (Paper). J. Hell. Stud. 1993, 113, 198–199. [Google Scholar] [CrossRef]
- Shlyankevich, J.; Chen, A.J.; Kim, G.E.; Kimball, A.B. Hidradenitis suppurativa is a systemic disease with substantial comorbidity burden: A chart-verified case-control analysis. J. Am. Acad. Dermatol. 2014, 71, 1144–1150. [Google Scholar] [CrossRef] [PubMed]
- Kohorst, J.J.; Shah, K.K.; Hallemeier, C.L.; Baum, C.L.; Davis, M.D.P. Squamous Cell Carcinoma in Perineal, Perianal, and Gluteal Hidradenitis Suppurativa: Experience in 12 Patients. Dermatol. Surg. 2019, 45, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, S.; Patel, K.R.; Singam, V.; Ali, Y.; Gao, J.; Amin, A.; Schlosser, B.J.; West, D.P.; Nardone, B. Vulvar cancer association with groin hidradenitis suppurativa: A large, urban, midwestern US patient population study. J. Am. Acad. Dermatol. 2019, 80, 808–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritz, J.P.; Runkel, N.; Haier, J.; Buhr, H.J. Extent of surgery and recurrence rate of hidradenitis suppurativa. Int. J. Colorectal. Dis. 1998, 13, 164–168. [Google Scholar] [CrossRef]
- Tannenbaum, R.; Strunk, A.; Garg, A. Association Between Hidradenitis Suppurativa and Lymphoma. JAMA Dermatol. 2019, 155, 624–625. [Google Scholar] [CrossRef] [PubMed]
- Gordon, S.W. Squamous cell carcinoma arising in hidradenitis suppurativa: Case report. Plast. Reconstr. Surg. 1977, 60, 800–802. [Google Scholar] [CrossRef] [PubMed]
- Black, S.B.; Woods, J.E. Squamous cell carcinoma complicating hidradenitis suppurativa. J. Surg. Oncol. 1982, 19, 25–26. [Google Scholar] [CrossRef]
- Rosen, T. Squamous cell carcinoma: Complication of chronic skin disorders in black patients. J. Natl. Med. Assoc. 1986, 78, 1203–1205. [Google Scholar] [PubMed]
- Zachary, L.S.; Robson, M.C.; Rachmaninoff, N. Squamous cell carcinoma occurring in hidradenitis suppurativa. Ann. Plast. Surg. 1987, 18, 71–73. [Google Scholar] [CrossRef]
- Anstey, A.V.; Wilkinson, J.D.; Lord, P. Squamous cell carcinoma complicating hidradenitis suppurativa. Br. J. Dermatol. 1990, 123, 527–531. [Google Scholar] [CrossRef]
- Mendonça, H.; Rebelo, C.; Fernandes, A.; Lino, A.; Garcia e Silva, L. Squamous cell carcinoma arising in hidradenitis suppurativa. J. Dermatol. Surg. Oncol. 1991, 7, 830–832. [Google Scholar] [CrossRef]
- Shukla, V.K.; Hughes, L.E. A case of squamous cell carcinoma complicating hidradenitis suppurativa. Eur. J. Surg. Oncol. 1995, 21, 106–109. [Google Scholar] [CrossRef]
- Pérez-Diaz, D.; Calvo-Serrano, M.; Mártinez-Hijosa, E.; Fuenmayor-Valera, L.; Muñoz-Jiménez, F.; Turégano-Fuentes, F.; Del Valle, E. Squamous cell carcinoma complicating perianal hidradenitis suppurativa. Int. J. Colorectal. Dis. 1995, 10, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Dufresne, R.G., Jr.; Ratz, J.L.; Bergfeld, W.F.; Roenigk, R.K. Squamous cell carcinoma arising from the follicular occlusion triad. J. Am. Acad. Dermatol. 1996, 35 Pt 1, 475–477. [Google Scholar] [CrossRef]
- Malaguarnera, M.; Pontillo, T.; Pistone, G.; Succi, L. Squamous-cell cancer in Verneuil’s disease (hidradenitis suppurativa). Lancet 1996, 348, 1449. [Google Scholar] [CrossRef]
- Gur, E.; Neligan, P.C.; Shafir, R.; Reznick, R.; Cohen, M.; Shpitzer, T. Squamous cell carcinoma in perineal inflammatory disease. Ann. Plast. Surg. 1997, 38, 653–657. [Google Scholar] [CrossRef]
- Alkeraye, S.; Nguyen, T.; Le Guern, A.; Alhaddad, M.; Mortier, L. Mucinous adenocarcinoma in association with hidradenitis suppurativa. Clin. Exp. Dermatol. 2017, 42, 550–551. [Google Scholar] [CrossRef]
- Manolitsas, T.; Biankin, S.; Jaworski, R.; Wain, G. Vulval squamous cell carcinoma arising in chronic hidradenitis suppurativa. Gynecol. Oncol. 1999, 75, 285–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosman, B.C.; O’Grady, T.C.; Pekarske, S. Verrucous carcinoma arising in hidradenitis suppurativa. Int. J. Colorectal. Dis. 2000, 15, 342–346. [Google Scholar] [CrossRef]
- Altunay, I.K.; Gökdemir, G.; Kurt, A.; Kayaoglu, S. Hidradenitis suppurativa and squamous cell carcinoma. Dermatol. Surg. 2002, 28, 88–90. [Google Scholar]
- Rosenzweig, L.B.; Brett, A.S.; Lefaivre, J.F.; Vandersteenhoven, J.J. Hidradenitis suppurativa complicated by squamous cell carcinoma and paraneoplastic neuropathy. Am. J. Med. Sci. 2005, 329, 150–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Short, K.A.; Kalu, G.; Mortimer, P.S.; Higgins, E.M. Vulval squamous cell carcinoma arising in chronic hidradenitis suppurativa. Clin. Exp. Dermatol. 2005, 30, 481–483. [Google Scholar] [CrossRef]
- Nyquist, G.G.; Mumm, C.; Grau, R.; Crowson, A.N.; Shurman, D.L.; Benedetto, P.; Allen, P.; Lovelace, K.; Smith, D.W.; Frieden, I.; et al. Malignant proliferating pilar tumors arising in KID syndrome: A report of two patients. Am. J. Med. Genet. A 2007, 143A, 734–741. [Google Scholar] [CrossRef]
- Kurokawa, I.; Nishimura, K.; Yamanaka, K.; Mizutani, H.; Tsubura, A.; Revuz, J. Cytokeratin expression in squamous cell carcinoma arising from hidradenitis suppurativa (acne inversa). J. Cutan. Pathol. 2007, 34, 675–678. [Google Scholar] [CrossRef]
- Maclean, G.M.; Coleman, D.J. Three fatal cases of squamous cell carcinoma arising in chronic perineal hidradenitis suppurativa. Ann. R. Coll. Surg. Engl. 2007, 89, 709–712. [Google Scholar] [CrossRef] [Green Version]
- Barresi, V.; Vitarelli, E.; Barresi, G. Acne inversa complicated by squamous cell carcinoma in association with diffuse malignant peritoneal mesothelioma arising in the absence of predisposing factors: A case report. J. Cutan. Pathol. 2008, 35, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Constantinou, C.; Widom, K.; Desantis, J.; Obmann, M. Hidradenitis suppurativa complicated by squamous cell carcinoma. Am. Surg. 2008, 74, 1177–1181. [Google Scholar] [CrossRef]
- Katz, R.D.; Goldberg, N.H. Marjolin ulcer arising within hidradenitis: A case report and literature review. Ann. Plast. Surg. 2009, 62, 173–174. [Google Scholar] [CrossRef] [PubMed]
- Chandramohan, K.; Mathews, A.; Kurian, A.; Thomas, S.; Ramachandran, K. Squamous cell carcinoma arising from perineal lesion in a familial case of Hidradenitis suppurativa. Int. Wound J. 2009, 6, 141–144. [Google Scholar] [CrossRef]
- Lavogiez, C.; Delaporte, E.; Darras-Vercambre, S.; De Lassalle, E.M.; Castillo, C.; Mirabel, X.; Laurent, F.; Patenotre, P.; Gheit, T.; Talmant, J.C.; et al. Clinicopathological study of 13 cases of squamous cell carcinoma complicating hidradenitis suppurativa. Dermatology 2010, 220, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Grewal, N.S.; Wan, D.C.; Roostaeian, J.; Rubayi, S.R. Marjolin ulcer in hidradenitis suppurativa: Case reports. Ann. Plast. Surg. 2010, 64, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Scheinfeld, N. A case of a patient with stage III familial hidradenitis suppurativa treated with 3 courses of infliximab and died of metastatic squamous cell carcinoma. Dermatol. Online J. 2014, 20. [Google Scholar]
- Chang, J.B.; Kung, T.A.; Cederna, P.S. Acute Marjolin’s ulcers: A nebulous diagnosis. Ann. Plast. Surg. 2014, 72, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Herschel, S.; Laske, J.; Stein, A. Squamous cell carcinoma arising in hidradenitis suppurativa. J. Dtsch. Dermatol. Ges. 2014, 12, 417–419. [Google Scholar] [CrossRef]
- Pena, Z.G.; Sivamani, R.K.; Konia, T.H.; Eisen, D.B. Squamous cell carcinoma in the setting of chronic hidradenitis suppurativa; report of a patient and update of the literature. Dermatol. Online J. 2015, 21. [Google Scholar] [CrossRef]
- Verdelli, A.; Antiga, E.; Bonciani, D.; Bonciolini, V.; Volpi, W.; Caproni, M. A fatal case of hidradenitis suppurativa associated with sepsis and squamous cell carcinoma. Int. J. Dermatol. 2016, 55, e52–e53. [Google Scholar] [CrossRef]
- Rekawek, P.; Mehta, S.; Andikyan, V.; Harmaty, M.; Zakashansky, K. Squamous cell carcinoma of the vulva arising in the setting of chronic hidradenitis suppurativa: A case report. Gynecol. Oncol. Rep. 2016, 16, 28–30. [Google Scholar] [CrossRef] [Green Version]
- Calamaro, P.; Cerroni, L. Intralymphatic Proliferation of T-cell Lymphoid Blasts in the Setting of Hidradenitis Suppurativa. Am. J. Dermatopathol. 2016, 38, 536–540. [Google Scholar] [CrossRef]
- Joglekar, K.; Jackson, C.; Kadaria, D.; Sodhi, A. Metastatic Squamous Cell Carcinoma of the Pleura: A Rare Complication of Hidradenitis Suppurativa. Am. J. Case Rep. 2016, 17, 989–992. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Lai, Z.; He, M.; Zhai, B.; Zhou, L.; Long, X. Successful surgical treatment for squamous cell carcinoma arising from hidradenitis suppurativa: A case report and literature review. Medicine 2017, 96, e5857. [Google Scholar] [CrossRef] [PubMed]
- Hessam, S.; Sand, M.; Bechara, F.G. When inflammation shifts to malignancy: Extensive squamous cell carcinoma in a female hidradenitis suppurativa/acne inversa patient. J. Dtsch. Dermatol. Ges. 2017, 15, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Yon, J.R.; Son, J.D.; Fredericks, C.; Morton, M.; Kingsley, S.; Gupta, S.; Poulakidas, S.; Bokhari, F. Marjolin’s Ulcer in Chronic Hidradenitis Suppurativa: A Rare Complication of an Often Neglected Disease. J. Burn Care Res. 2017, 38, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.Q.; Tan, C. Squamous cell carcinoma arising in chronic hidradenitis suppurativa: A lethal complication to be avoided. Acta Oncol. 2017, 56, 497–498. [Google Scholar] [CrossRef] [Green Version]
- Fabbrocini, G.; Ruocco, E.; De Vita, V.; Monfrecola, G. Squamous cell carcinoma arising in long-standing hidradenitis suppurativa: An overlooked facet of the immunocompromised district. Clin. Dermatol. 2017, 35, 225–227. [Google Scholar] [CrossRef]
- Sotoodian, B.; Abbas, M.; Brassard, A. Hidradenitis Suppurativa and the Association with Hematological Malignancies. J. Cutan. Med. Surg. 2017, 21, 158–161. [Google Scholar] [CrossRef]
- Jourabchi, N.; Fischer, A.H.; Cimino-Mathews, A.; Waters, K.M.; Okoye, G.A. Squamous cell carcinoma complicating a chronic lesion of hidradenitis suppurativa: A case report and review of the literature. Int. Wound J. 2017, 14, 435–438. [Google Scholar] [CrossRef] [PubMed]
- McArdle, D.J.T.; McArdle, J.P.; Lee, F.; Mignanelli, E.D. Rare “Inverted” Verrucous Carcinoma (Carcinoma Cuniculatum) of the Sacrogluteal Region: Case Report and Literature Review. Int. J. Surg. Pathol. 2017, 25, 438–442. [Google Scholar] [CrossRef]
- Dessinioti, C.; Plaka, M.; Zisimou, C.; Christofidou, E.; Antoniou, C.; Stratigos, A.J. Advanced squamous cell carcinoma of the axillae mimicking hidradenitis suppurativa. J. Eur. Acad. Dermatol. Venereol. 2017, 31, e421–e423. [Google Scholar] [CrossRef]
- Bessaleli, E.; Scheinfeld, N.; Kroumpouzos-, G. Squamous cell carcinoma of the cervix arising in a patient on adalimumab a need for cervical screenings in patients on tumor necrosis factor inhibitors. Dermatol. Online J. 2018, 24. [Google Scholar]
- Yen, C.F.; Chang, Y.Y.; Lee, Y.Y. Image Gallery: Squamous cell carcinoma arising in long-standing hidradenitis suppurativa. Br. J. Dermatol. 2018, 179, e226. [Google Scholar] [CrossRef] [Green Version]
- Beard, C.J.; Gathings, R.M.; Bandino, J.P. Exophytic Mass Arising Within Hidradenitis Suppurativa: Answer. Am. J. Dermatopathol. 2019, 41, 235–236. [Google Scholar] [CrossRef]
- Nielsen, V.W.; Jørgensen, A.R.; Thomsen, S.F. Fatal outcome of malignant transformation of hidradenitis suppurativa: A case report and literature review. Clin. Case Rep. 2020, 8, 504–507. [Google Scholar] [CrossRef] [Green Version]
- Ward, R.A.; Udechukwu, N.S.; Selim, M.A.; Jaleel, T. Vulvar and perineal verrucous changes complicating hidradenitis suppurativa after wide excision: A case and literature review. Dermatol. Online J. 2020, 26. [Google Scholar] [CrossRef]
- Kohorst, J.J.; Kimball, A.B.; Davis, M.D. Systemic associations of hidradenitis suppurativa. J. Am. Acad. Dermatol. 2015, 73 (Suppl. S1), S27–S35. [Google Scholar] [CrossRef]
- Caccavale, S.; Caccavale, T.; La Montagna, M. Hidradenitis suppurativa associated with squamous cell carcinoma: An example of an isoscartopic response. Int. J. Dermatol. 2016, 55, e629–e631. [Google Scholar] [CrossRef] [PubMed]
- Jackman, R.J. Hidradenitis suppurativa: Diagnosis and surgical management of perianal manifestations. Proc. R. Soc. Med. 1959, 52 (Suppl. S1), 110–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, J.T.; Naik, H.B. Complications of hidradenitis suppurativa. Semin. Cutan. Med. Surg. 2017, 36, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Asgeirsson, T.; Nunoo, R.; Luchtefeld, M.A. Hidradenitis suppurativa and pruritus ani. Clin. Colon Rectal Surg. 2011, 24, 71–80. [Google Scholar] [CrossRef] [Green Version]
- Radcliffe, K.W. Hidradenitis suppurativa. Genitourin. Med. 1991, 67, 58. [Google Scholar] [CrossRef] [Green Version]
- De Bree, E.; Zoetmulder, F.A.; Christodoulakis, M.; Aleman, B.M.; Tsiftsis, D.D. Treatment of malignancy arising in pilonidal disease. Ann. Surg. Oncol. 2001, 8, 60–64. [Google Scholar] [CrossRef]
- Stein, A.; Sebastian, G. Acne inversa. Hautarzt 2003, 54, 173–185. (In German) [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.J.; Doekerty, M.B. Perianal hidradenitis suppurativa. Dis. Colon Rectum 1958, I, 25–51. [Google Scholar] [CrossRef]
- Tchernev, G.; Guarneri, C.; Bevelacqua, V.; Wollina, U. Carcinoma cuniculatum in course of etanercept: Blocking autoimmunity but propagation of carcinogenesis? Int. J. Immunopathol. Pharmacol. 2014, 27, 261–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caccavale, S.; Caccavale, T.; La Montagna, M. Hidradenitis suppurativa complicated by squamous cell carcinoma: Isoscartopic response. Int. Wound J. 2017, 14, 1397–1398. [Google Scholar] [CrossRef]
- Nikkels, A.; Lebas, E. Should we provide anti-human papillomavirus vaccination for patients with genital hidradenitis suppurativa? Br. J. Dermatol. 2019, 180, 233. [Google Scholar] [CrossRef] [Green Version]
- Flores, R.; Lu, B.; Nielson, C.; Abrahamsen, M.; Wolf, K.; Lee, J.H.; Harris, R.B.; Giuliano, A.R. Correlates of human papillomavirus viral load with infection site in asymptomatic men. Cancer Epidemiol. Prev. Biomark. 2008, 17, 3573–3576. [Google Scholar] [CrossRef] [Green Version]
- Ceccarelli, M.; Venanzi Rullo, E.; Berretta, M.; Cacopardo, B.; Pellicanò, G.F.; Nunnari, G.; Guarneri, C. New generation biologics for the treatment of psoriasis and psoriatic arthritis. State of the art and considerations about the risk of infection. Dermatol. Ther. 2021, 34, e14660. [Google Scholar] [CrossRef]
- Di Lernia, V.; Guarneri, C.; Stingeni, L.; Gisondi, P.; Bonamonte, D.; Calzavara Pinton, P.G.; Offidani, A.; Hansel, K.; Girolomoni, G.; Filoni, A.; et al. Effectiveness of etanercept in children with plaque psoriasis in real practice: A one-year multicenter retrospective study. J. Dermatol. Treat. 2018, 29, 217–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molinelli, E.; Sapigni, C.; Campanati, A.; Brisigotti, V.; Offidani, A. Metabolic, pharmacokinetic, and toxicological issues of biologic therapies currently used in the treatment of hidradenitis suppurativa. Expert Opin. Drug Metab. Toxicol. 2020, 16, 1019–1037. [Google Scholar] [CrossRef]
- Ganzetti, G.; Campanati, A.; Molinelli, E.; Offidani, A. Biologic Therapy in Inflammatory and Immunomediated Skin Diseases: Safety Profile. Curr. Drug Saf. 2016, 11, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Kamangar, F.; Neuhaus, I.M.; Koo, J.Y. An evidence-based review of skin cancer rates on biologic therapies. J. Dermatol. Treat. 2012, 23, 305–315. [Google Scholar] [CrossRef]
- Cannavò, S.P.; Guarneri, F.; Giuffrida, R.; Aragona, E.; Guarneri, C. Evaluation of cutaneous surface parameters in psoriatic patients. Skin Res. Technol. 2017, 23, 41–47. [Google Scholar] [CrossRef]
- Askling, J.; Fahrbach, K.; Nordstrom, B.; Ross, S.; Schmid, C.H.; Symmons, D. Cancer risk with tumor necrosis factor alpha (TNF) inhibitors: Meta-analysis of randomized controlled trials of adalimumab, etanercept, and infliximab using patient level data. Pharmacoepidemiol. Drug Saf. 2011, 20, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Skarmoutsou, E.; Bevelacqua, V.; D’Amico, F.; Russo, A.; Spandidos, D.A.; Scalisi, A.; Malaponte, G.; Guarneri, C. FOXP3 expression is modulated by TGF-β1/NOTCH1 pathway in human melanoma. Int. J. Mol. Med. 2018, 42, 392–404. [Google Scholar] [CrossRef] [Green Version]
- Giuffrida, R.; Cannavò, S.P.; Coppola, M.; Guarneri, C. Novel Therapeutic Approaches and Targets for the Treatment of Hidradenitis Suppurativa. Curr. Pharm. Biotechnol. 2021, 22, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Hunt, M.J.; Commens, C.A. Hidradenitis suppurativa, Dowling Degos disease and perianal squamous cell carcinoma. Australas. J. Dermatol. 1997, 38, 209–211. [Google Scholar] [CrossRef]
- Jung, J.M.; Lee, K.H.; Kim, Y.J.; Chang, S.E.; Lee, M.W.; Choi, J.H.; Won, C.H.; Lee, W.J. Assessment of Overall and Specific Cancer Risks in Patients with Hidradenitis Suppurativa. JAMA Dermatol. 2020, 156, 844–853. [Google Scholar] [CrossRef]


{kind=link}
| Type of Article | Strength Level |
|---|---|
| Review | 1 |
| Retrospective cohort study | 2 |
| Case-control study | 3 |
| Cross sectional study | 4 |
| Case series | 5 |
| Case report | 6 |
| Authors, Reference Number and Year | Type of Study | Study Population | Strength Level |
|---|---|---|---|
| Gordon SW [17], 1977 | Case report | 38-year-old woman with HS and SCC of the sacral area | 6 |
| Black SB et al. [18], 1982 | Case report | 44-year-old man with HS and perianal SCC | 6 |
| Rosen T [19], 1986 | Case report | 55-year-old man with HS and perianal SCC | 6 |
| Zachary LS et al. [20], 1987 | Case report | 55-year-old man with HS and perineal SCC | 6 |
| Anstey AV et al. [21], 1990 | Case report | 67-year-old man with HS and SCC of the buttocks | 6 |
| Mendonça H et al. [22], 1991 | Case report | 57-year-old man with HS and SCC of the buttocks | 6 |
| Shukla VK et al. [23], 1995 | Case report | 71-year-old woman with HS and SCC of the buttocks | 6 |
| Pérez-Diaz D et al. [24], 1995 | Review | 27 cases described in literature presenting with HS and SCC. The buttocks were involved in 12 cases, perianal region in 11 cases, perineum in only one. The site of carcinoma was not specified in 3 cases. Four patients had lymph node metastasis, 1 lymph node, and liver metastatic disease | 1 |
| Dufresne RG Jr et al. [25], 1996 | Case report | 52-year-old woman with HS and follicular occlusion triad developing SCC of the buttocks | 6 |
| Malaguarnera M et al. [26], 1996 | Case report | 66-year-old man with perineal HS and metastatic SCC | 6 |
| Gur E et al. [27], 1997 | Case report | 1 case out of 4 with perineal SCC having also HS | 6 |
| Li M et al. [28], 1997 | Case report | 68-year-old man with HS and DD syndrome having perianal SCC | 6 |
| Ritz JP et al. [15], 1998 | Retrospective cohort study | 61-year-old man with gluteal SCC out of 31 patients that underwent surgery for HS | 2 |
| Manolitsas T et al. [29], 1999 | Case report | 52-year-old woman with HS and vulvar SCC | 6 |
| Cosman BC et al. [30], 2000 | Case report | 47-year-old man with HS and verrucous carcinoma (SCC) of the perianal area | 6 |
| Lapins J et al. [9], 2001 | Retrospective cohort study | 81 cases out of 2119 patients with HS. Significantly elevated relative risks for NMSC (5 cases), buccal cancer (5 cases), and primary liver cancer (3 cases) | 2 |
| Altunay IK et al. [31], 2002 | Case report | 54-year-old man with HS and SCC of the buttocks | 6 |
| Rosenzweig LB et al. [32], 2005 | Case report | 50-year-old man with HS and SCC of the perineum, complicated by paraneoplastic neuropathy | 6 |
| Short KA et al. [33], 2005 | Case report | 57-year-old woman with HS and SCC of the vulva | 6 |
| Nyquist GG et al. [34], 2007 | Case series | 31-year-old woman and 24-year-old man with HS and SCC of the groin in KID syndrome | 5 |
| Kurokawa I et al. [35], 2007 | Case series | 50-year-old man and 72-year-old man having HS and SCC of the buttocks, one with metastatic disease | 5 |
| Maclean GM et al. [36], 2007 | Review | Description of 3 fatal cases of SCC in HS patients and review of other cases in literature: 15 patients had SCC of the buttocks, 9 had the involvement of the perianal region, 4 of the perineum, 2 of the vulva and 1 had SCC of the groin region. 13 of these presented lymph node metastasis | 1 |
| Barresi V et al. [37], 2008 | Case report | 47-year-old man with sacral HS and diffuse malignant peritoneal mesothelioma | 6 |
| Constantinou C et al. [38], 2008 | Case series | One patient having diffuse abdominal carcinomatosis from perianal SCC arising on HS lesions; one patient with malignant hypercalcemia, as a complication of cutaneous SCC | 5 |
| Katz R [39], 2009 | Case report | 61-year-old man with HS and SCC (Marjolin Ulcer) of the buttocks | 6 |
| Chandramohan K et al. [40], 2009 | Case report | 40-year-old man with HS and perianal SCC | 6 |
| Lavogiez C et al. [41], 2010 | Review | 13 patients having HS and SCC of the buttocks, 2 with lymph node metastasis | 1 |
| Grewal NS et al. [42], 2010 | Case series | 2 cases with HS and gluteal SCC, 1 case with HS and SCC of the perineum | 5 |
| Scheinfeld N [43], 2014 | Case report | 47-year-old man with HS and perianal/anal SCC after starting infliximab | 6 |
| Chang JB et al. [44], 2014 | Case report | 50-year-old man with HS of the chest, axilla, thigh, buttocks, and groin and metastatic SCC (paraneoplastic syndrome: pancreatitis and deep venous thrombosis of the inferior vena cava and bilateral femoral veins) | 6 |
| Herschel S et al. [45], 2014 | Case report | 72-year-old man with HS and SCC of the sacral region with lymph nodes metastasis | 6 |
| Shlyankevich J et al. [12], 2014 | Case control study | 32 patients having HS and Lymphoma (9 healthy control), 9 patients having HS and SCC (0 healthy control) | 3 |
| Pena Z et al. [46], 2015 | Case report | 64-year-old woman having HS and metastatic vulvar SCC | 6 |
| Verdelli A et al. [47], 2016 | Case report | 78-year-old man with HS, treated with infliximab, and associated SCC | 6 |
| Rekawek P et al. [48], 2016 | Case report | 61-year-old woman with HS and SCC of the vulva | 6 |
| Calamaro P et al. [49], 2016 | Case report | 35-year-old man with inguinal HS and intralymphatic proliferation of T-cell lymphoid blasts | 6 |
| Joglekar K et al. [50], 2016 | Case report | 46-year-old man with gluteal HS and metastatic SCC | 6 |
| Makris GM et al. [3], 2017 | Review | 9 patients with HS and vulvar SCC (3 cases had nodal or metastatic disease); 6 patients with perineal/perianal SCC (2 cases had nodal or metastatic disease) and 1 with perianal mucinous adenocarcinoma | 1 |
| Huang C et al. [51], 2017 | Case report | 60-year-old man having HS and verrucous carcinoma (SCC) of the buttocks | 6 |
| Hessam S et al. [52], 2017 | Case report | 63-year-old man with inguinal, gluteal, and perianal HS and lymph node metastasis | 6 |
| Yon JR et al. [53], 2017 | Review | 2 cases out of 72 patients with HS, both having perineal SCC with lymph nodes metastasis | 1 |
| Zhang L et al. [54], 2017 | Case report | 59-year-old man with HS and SCC of the buttocks | 6 |
| Fabbrocini G et al. [55], 2017 | Review | Over 90 cases in literature of HS and SCC developing on the perineal or buttock area | 1 |
| Sotoodian B et al. [56], 2017 | Case series | a 60-year-old man with hairy cell leukemia and a 68 year-old man with chronic lymphocytic leukemia who developed HS later in life | 5 |
| Jourabchi N et al. [57], 2017 | Case report | 69-year-old man with HS and SCC of the buttocks | 6 |
| Alkeraye S et al. [28], 2017 | Case report | 61-year-old man with HS and perianal mucinous adenocarcinoma | 6 |
| McArdle DJT et al. [58], 2017 | Case report | 49-year-old woman with HS and anal SCC (carcinoma cuniculatum) | 6 |
| Dessinioti C et al. [59], 2017 | Case report | 56-year-old man with HS and SCC of the axillae | 6 |
| Chapman S et al. [4], 2018 | Review | 85 cases of SCC arising from HS found in English literature | 1 |
| Bessaleli E et al. [60], 2018 | Case report | 33-year-old woman treated with adalimumab who developed carcinoma of the cervix | 6 |
| Yen CF et al. [61], 2018 | Case report | 45-year-old man with HS and SCC of the buttock with metastatic disease | 6 |
| Beard C et al. [62], 2019 | Case report | 50-year-old man with MU arising in HS, having lymph node metastasis | 6 |
| Rastogi S et al. [14], 2019 | Case control study | 3 cases out of 716 patients with HS having vulvar SCC | 3 |
| Kohorst JJ et al. [13], 2019 | Retrospective cohort study | 12 cases with HS and gluteal, perianal, perineal and vulvo-vaginal SCC, 1 with lymph node metastasis | 2 |
| Tannenbaum R et al. [16], 2019 | Cross sectional cohort study | Prevalence of NHL, HL, and CTCL among patient with HS (n = 62 690) compared with patient without HS (n = 20 937 880) | 4 |
| Nielsen VW et al. [63], 2020 | Case report | 66-year-old woman having HS, vulvar SCC, and metastatic disease | 6 |
| Ward R et al. [64], 2020 | Case report | 54-year-old woman with HS and SCC of the vulva | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li Pomi, F.; Macca, L.; Motolese, A.; Ingrasciotta, Y.; Berretta, M.; Guarneri, C. Neoplastic Implications in Patients Suffering from Hidradenitis Suppurativa under Systemic Treatments. Biomedicines 2021, 9, 1594. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9111594
Li Pomi F, Macca L, Motolese A, Ingrasciotta Y, Berretta M, Guarneri C. Neoplastic Implications in Patients Suffering from Hidradenitis Suppurativa under Systemic Treatments. Biomedicines. 2021; 9(11):1594. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9111594
Chicago/Turabian StyleLi Pomi, Federica, Laura Macca, Alfonso Motolese, Ylenia Ingrasciotta, Massimiliano Berretta, and Claudio Guarneri. 2021. "Neoplastic Implications in Patients Suffering from Hidradenitis Suppurativa under Systemic Treatments" Biomedicines 9, no. 11: 1594. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9111594