
Anatomy, Pathophysiology, Molecular Mechanisms, and Clinical Management of Erectile Dysfunction in Patients Affected by Coronary Artery Disease: A Review

 , ,
, ,
Abstract
:1. Introduction
2. Anatomy of Erection
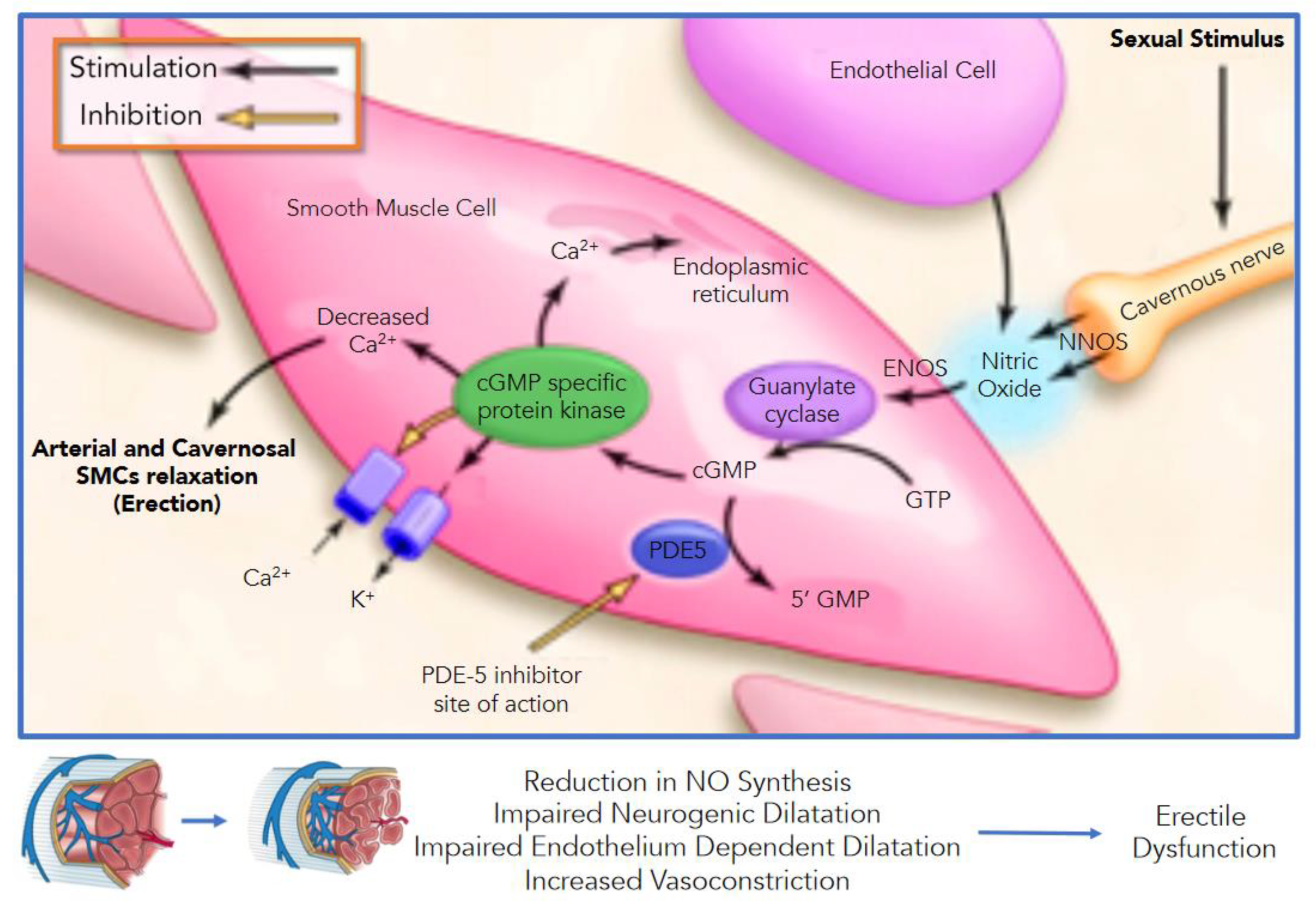
3. Vascular Events of Erection
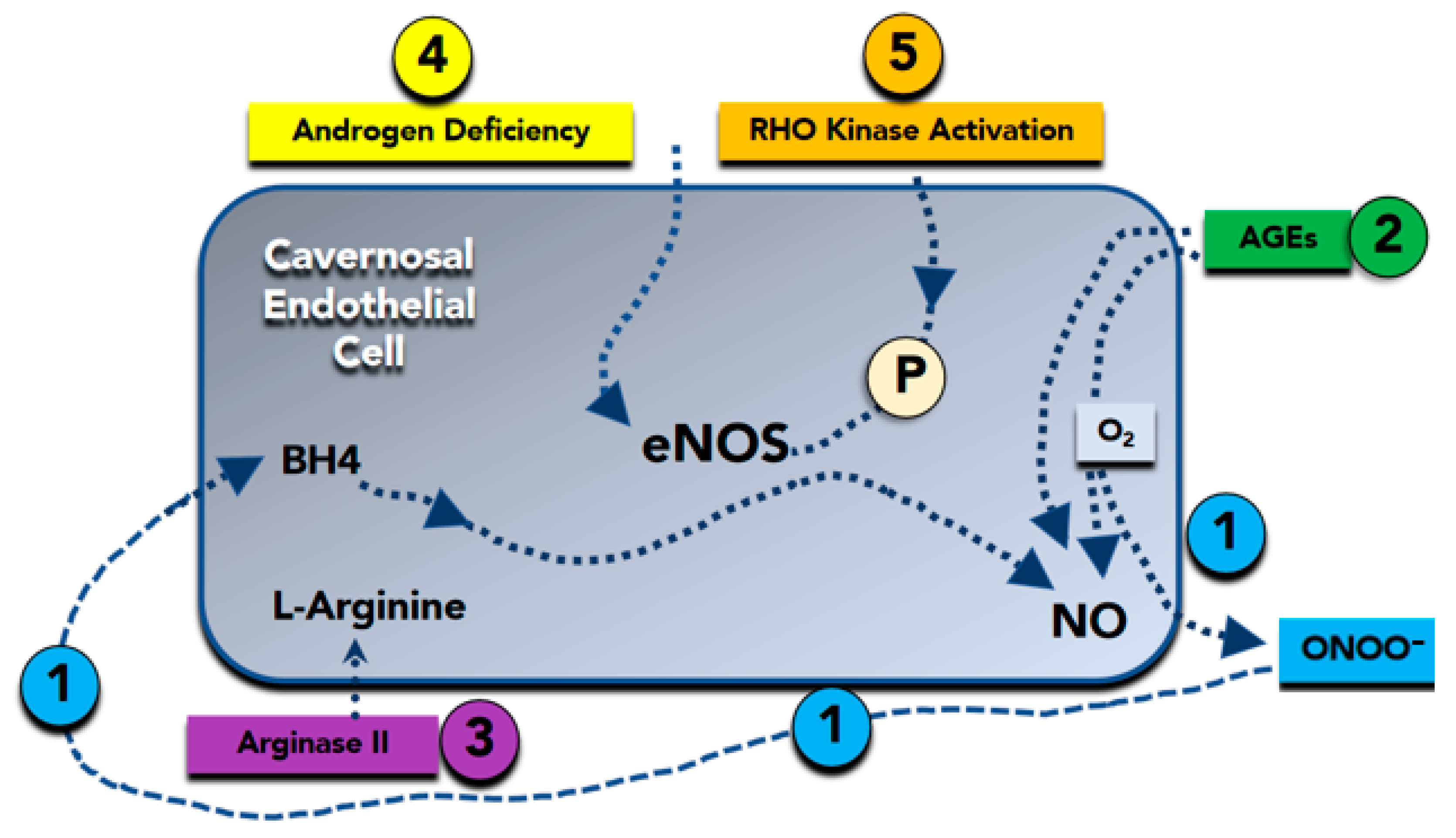
4. Molecular Basis of Erectile Dysfunction
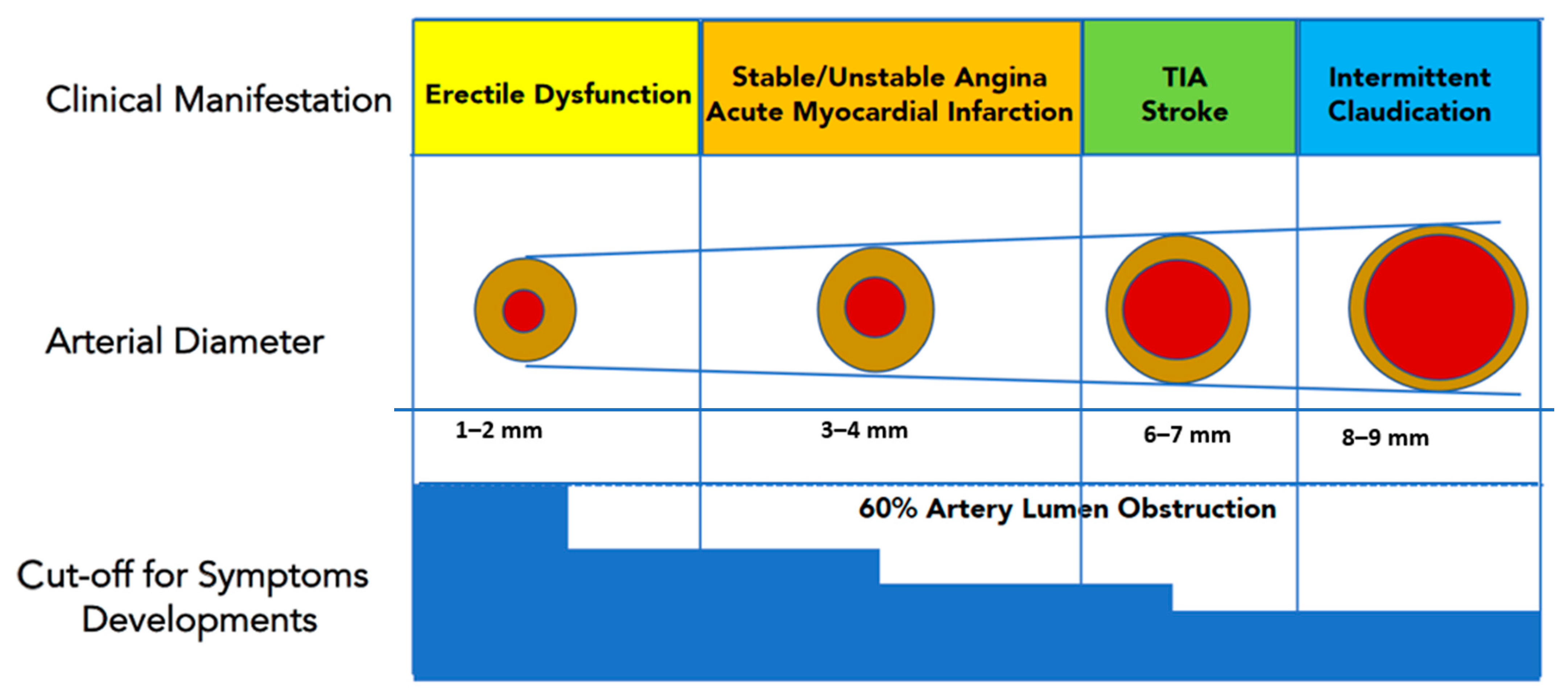
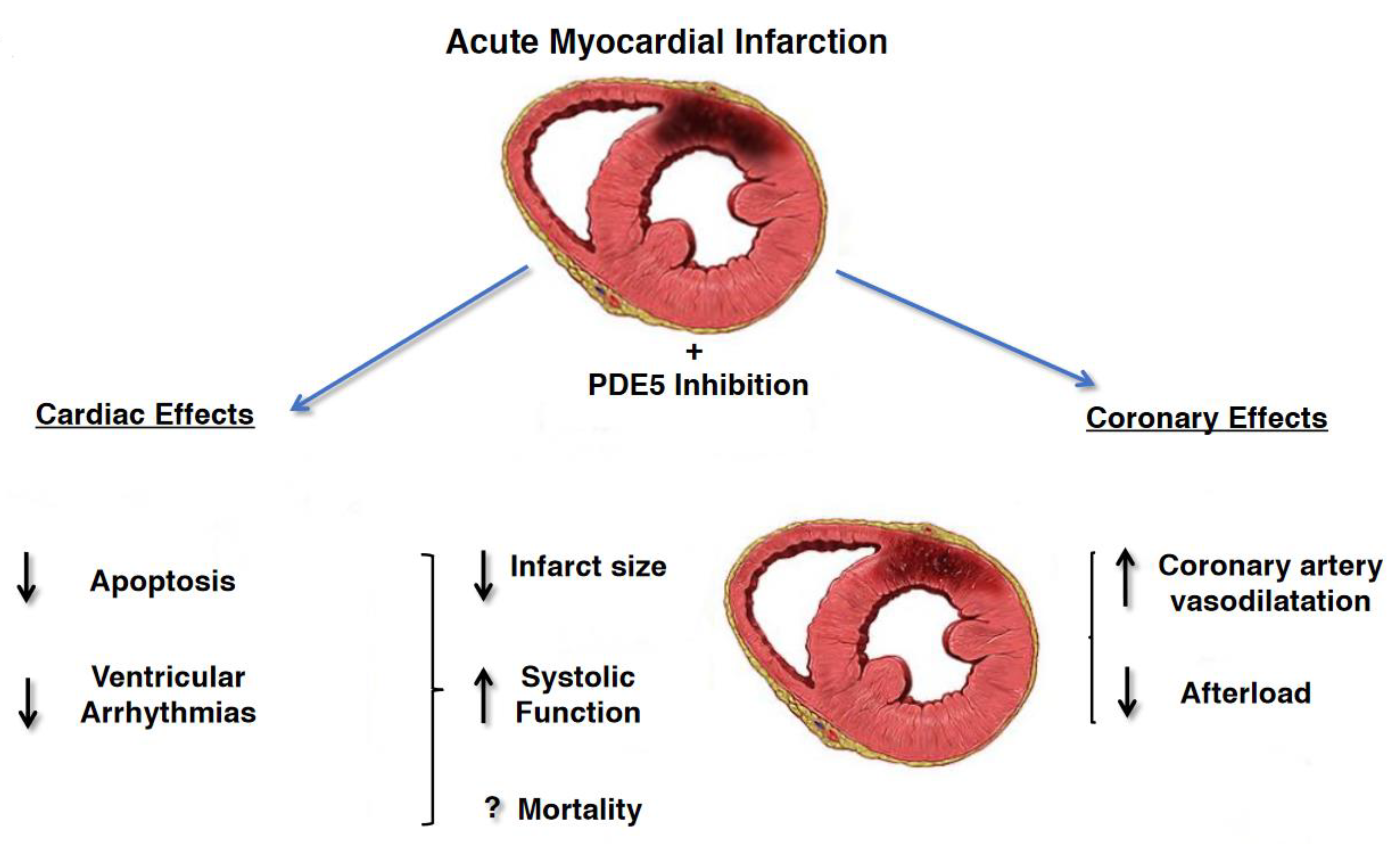
5. Erectile Dysfunction and Cardiovascular Diseases
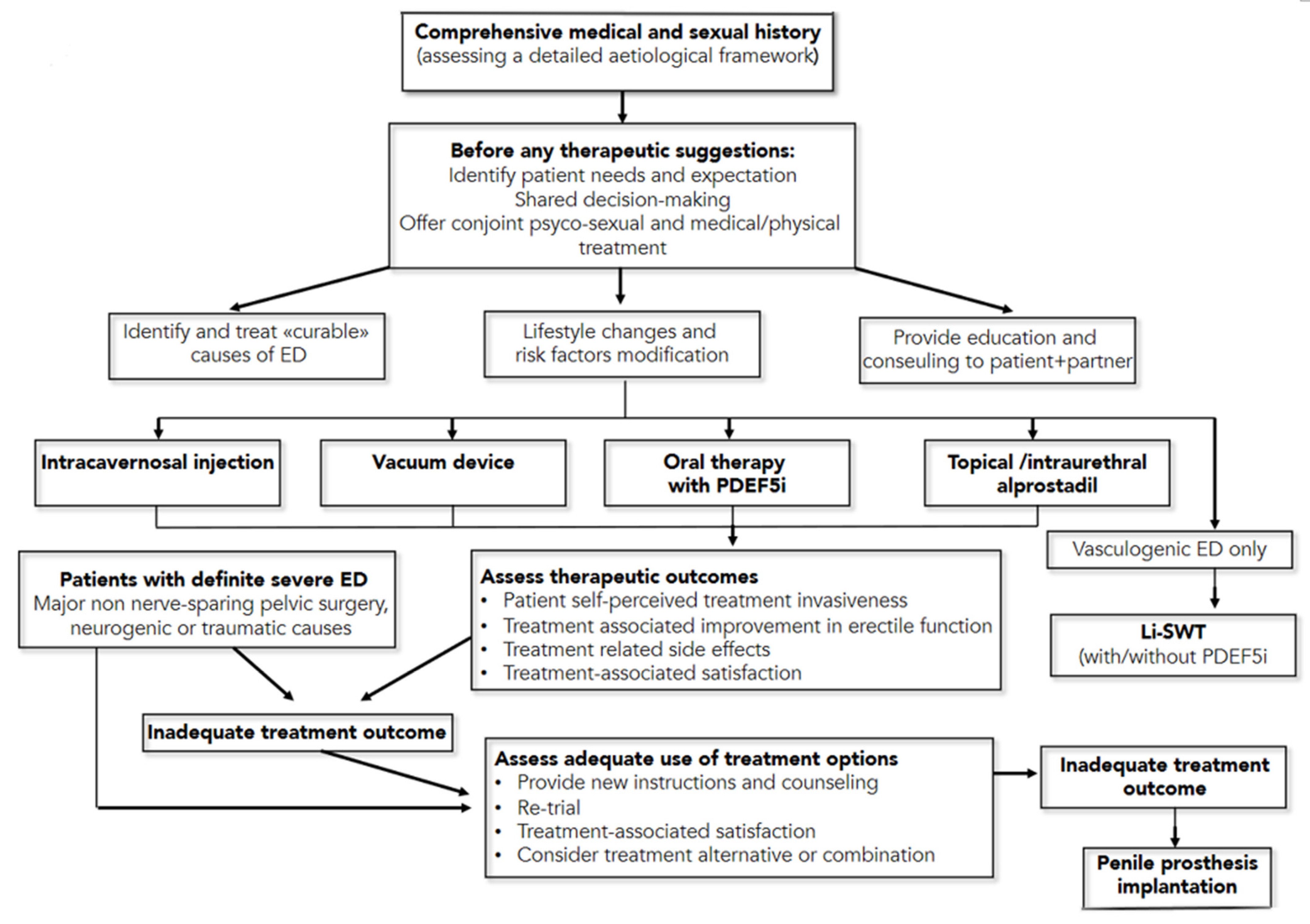
6. Guidelines for Therapeutic Management of Erectile Dysfunction
7. New on the Horizon: Regeneration Strategies for ED
7.1. Platelet-Rich Plasma and ED
7.2. Stem Cell Therapy and ED
8. Conclusions
Author Contributions
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCabe, M.P.; Sharlip, I.D.; Atalla, E.; Balon, R.; Fisher, A.D.; Laumann, E.; Lee, S.W.; Lewis, R.; Segraves, R.T. Definitions of Sexual Dysfunctions in Women and Men: A Consensus Statement From the Fourth International Consultation on Sexual Medicine 2015. J. Sex. Med. 2016, 13, 135–143. [Google Scholar] [CrossRef]
- Grover, S.A.; Lowensteyn, I.; Kaouache, M.; Marchand, S.; Coupal, L.; Decarolis, E.; Zoccoli, J.; Defoy, I. The Prevalence of Erectile Dysfunction in the Primary Care Setting. Arch. Intern. Med. 2006, 166, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Schouten, B.W.V.; Bosch, J.L.H.R.; Bernsen, R.M.D.; Blanker, M.H.; Thomas, S.; Bohnen, A.M. Incidence rates of erectile dysfunction in the Dutch general population. Effects of definition, clinical relevance and duration of follow-up in the Krimpen Study. Int. J. Impot. Res. 2004, 17, 58–62. [Google Scholar] [CrossRef]
- Corona, G.; Lee, D.M.; Forti, G.; O’Connor, D.B.; Maggi, M.; O’Neill, T.W.; Pendleton, N.; Bartfai, G.; Boonen, S.; Casanueva, F.F.; et al. Age-Related Changes in General and Sexual Health in Middle-Aged and Older Men: Results from the European Male Ageing Study (EMAS). J. Sex. Med. 2010, 7, 1362–1380. [Google Scholar] [CrossRef] [PubMed]
- Parazzini, F.; Fabris, F.M.; Bortolotti, A.; Calabrò, A.; Chatenoud, L.; Colli, E.; Landoni, M.; Lavezzari, M.; Turchi, P.; Sessa, A.; et al. Frequency and Determinants of Erectile Dysfunction in Italy. Eur. Urol. 2000, 37, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Ayta, I.A.; McKinlay, J.B.; Krane, R.J. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 1999, 84, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Alberti, L.; Torlasco, C.; Lauretta, L.; Loffi, M.; Maranta, F.; Salonia, A.; Margonato, A.; Montorsi, F.; Fragasso, G. Erectile dysfunction in heart failure patients: A critical reappraisal. Andrology 2013, 1, 177–191. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Liao, C.; Zou, Y.; Li, F.; Li, T.; Zhou, Q.; Cao, Y.; Mao, X. Erectile Dysfunction and Risk of Clinical Cardiovascular Events: A Meta-Analysis of Seven Cohort Studies. J. Sex. Med. 2010, 7, 2805–2816. [Google Scholar] [CrossRef] [PubMed]
- Montorsi, P.P.; Montorsi, F.; Schulman, C.C. Is Erectile Dysfunction the “Tip of the Iceberg” of a Systemic Vascular Disorder? Eur. Urol. 2003, 44, 352–354. [Google Scholar] [CrossRef]
- Feldman, H.A.; Goldstein, I.; Hatzichristou, D.G.; Krane, R.J.; McKinlay, J.B. Impotence and Its Medical and Psychosocial Correlates: Results of the Massachusetts Male Aging Study. J. Urol. 1994, 151, 54–61. [Google Scholar] [CrossRef]
- Nehra, A.; Azadzoi, K.M.; Moreland, R.B.; Pabby, A.; Siroky, M.B.; Krane, R.J.; Goldstein, I.; Udelson, D. cavernosal expandability is an erectile tissue mechanical property which predicts trabecular histology in an animal model of vasculogenic erectile dysfunction. J. Urol. 1998, 159, 2229–2236. [Google Scholar] [CrossRef]
- Nehra, A.; Goldstein, I.; Pabby, A.; Nugent, M.; Huang, Y.-H.; Morenas, A.D.L.; Krane, R.J.; Udelson, D.; De Tejada, I.S.; Moreland, R.B. Mechanisms of Venous Leakage: A Prospective Clinicopathological Correlation of Corporeal Function and Structure. J. Urol. 1996, 156, 1320–1329. [Google Scholar] [CrossRef]
- Bossart, M.I.; Spjut, H.J.; Scott, F.B. Ultrastructural analysis of human penile corpus cavernosum Its significance in tumescence and detumescence. Urology 1980, 15, 448–456. [Google Scholar] [CrossRef]
- Raviv, G.; Kiss, R.; Vanegas, J.P.; Petein, M.; Danguy, A.; Schulman, C.; Wespes, E. Objective measurement of the different collagen types in the corpus cavernosum of potent and impotent men: An immunohistochemical staining with computerized-image analysis. World J. Urol. 1997, 15, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Podlasek, C.A.; Zelner, D.J.; Bin Jiang, H.; Tang, Y.; Houston, J.; McKenna, K.E.; McVary, K.T. Sonic hedgehog cascade is required for penile postnatal morphogenesis, differentiation, and adult homeostasis. Biol. Reprod. 2003, 68, 423–438. [Google Scholar] [CrossRef]
- Sattar, A.A.; Salpigides, G.; Vanderhaeghen, J.-J.; Schulman, C.C.; Wespes, E. Cavernous Oxygen Tension and Smooth Muscle Fibers: Relation and Function. J. Urol. 1995, 154, 1736–1739. [Google Scholar] [CrossRef]
- Breza, J.; Aboseif, S.R.; Orvis, B.R.; Lue, T.F.; Tanagho, E.A. Detailed Anatomy of Penile Neurovascular Structures: Surgical Significance. J. Urol. 1989, 141, 437–443. [Google Scholar] [CrossRef]
- Hsu, G.-L. Hypothesis of human penile anatomy, erection hemodynamics and their clinical applications. Asian J. Androl. 2006, 8, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Gratzke, C.; Angulo, J.; Chitaley, K.; Dai, Y.-T.; Kim, N.N.; Paick, J.-S.; Simonsen, U.; Ückert, S.; Wespes, E.; Andersson, K.E.; et al. Anatomy, Physiology, and Pathophysiology of Erectile Dysfunction. J. Sex. Med. 2010, 7, 445–475. [Google Scholar] [CrossRef]
- Lue, T.F.; Tanagho, E.A. Physiology of Erection and Pharmacological Management of Impotence. J. Urol. 1987, 137, 829–836. [Google Scholar] [CrossRef]
- Lue, T.F. Physiology of penile erection and pathophysiology of erectile dysfunction. In Campbell-Walsh Urology; Saunders, W., Ed.; Saunders: Philadelphia, PA, USA, 2012. [Google Scholar]
- Elesber, A.A.; Solomon, H.; Lennon, R.J.; Mathew, V.; Prasad, A.; Pumper, G.; Nelson, R.E.; McConnell, J.P.; Lerman, L.O.; Lerman, A. Coronary endothelial dysfunction is associated with erectile dysfunction and elevated asymmetric dimethylarginine in patients with early atherosclerosis. Eur. Heart J. 2006, 27, 824–831. [Google Scholar] [CrossRef] [Green Version]
- Ganz, P.; Vita, J.A. Testing Endothelial Vasomotor Function. Circulation 2003, 108, 2049–2053. [Google Scholar] [CrossRef] [PubMed]
- Lue, T.F. Erectile Dysfunction. N. Engl. J. Med. 2000, 342, 1802–1813. [Google Scholar] [CrossRef]
- Holmquist, F.; Andersson, K.-E.; Hedlund, H. Actions of endothelin on isolated corpus cavernosum from rabbit and man. Acta Physiol. Scand. 1990, 139, 113–122. [Google Scholar] [CrossRef]
- De Tejada, I.S.; Goldstein, I.; Azadzoi, K.; Krane, R.J.; Cohen, R.A. Impaired Neurogenic and Endothelium-Mediated Relaxation of Penile Smooth Muscle from Diabetic Men with Impotence. N. Engl. J. Med. 1989, 320, 1025–1030. [Google Scholar] [CrossRef]
- Kim, N.; Azadzoi, K.M.; Goldstein, I.; De Tejada, I.S. A nitric oxide-like factor mediates nonadrenergic-noncholinergic neurogenic relaxation of penile corpus cavernosum smooth muscle. J. Clin. Investig. 1991, 88, 112–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, L.J.; Murad, F. Nitric Oxide and Cyclic GMP Signaling. Exp. Biol. Med. 1996, 211, 1–6. [Google Scholar] [CrossRef]
- Rajfer, J.; Aronson, W.J.; Bush, P.A.; Dorey, F.J.; Ignarro, L.J. Nitric Oxide as a Mediator of Relaxation of the Corpus Cavernosum in Response to Nonadrenergic, Noncholinergic Neurotransmission. N. Engl. J. Med. 1992, 326, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Wegner, H.E.; Knispel, H.H. Effect of nitric oxide-donor, linsidomine chlorhydrate, in treatment of human erectile dysfunction caused by venous leakage. Urology 1993, 42, 409–411. [Google Scholar] [CrossRef]
- Lorrain, D.S.; Matuszewich, L.; Howard, R.V.; Du, J.; Hull, E.M. Nitric oxide promotes medial preoptic dopamine release during male rat copulation. Neuroreport 1996, 8, 31–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melis, M.R.; Argiolas, A. Role op central nitric oxide in the control of penile erection and yawning. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 1997, 21, 899–922. [Google Scholar] [CrossRef]
- Förstermann, U.; Closs, E.I.; Pollock, J.S.; Nakane, M.; Schwarz, P.; Gath, I.; Kleinert, H. Nitric oxide synthase isozymes. Characterization, purification, molecular cloning, and functions. Hypertension 1994, 23, 1121–1131. [Google Scholar] [CrossRef] [Green Version]
- Vergoni, A.V.; Bertolini, A.; Mutulis, F.; Wikberg, J.E.; Schiöth, H.B. Differential influence of a selective melanocortin MC4 receptor antagonist (HS014) on melanocortin-induced behavioral effects in rats. Eur. J. Pharmacol. 1998, 362, 95–101. [Google Scholar] [CrossRef]
- Naylor, A.M. Endogenous neurotransmitters mediating penile erection. BJU Int. 1998, 81, 424–431. [Google Scholar] [CrossRef]
- Hedlund, P.; Aszódi, A.; Pfeifer, A.; Alm, P.; Hofmann, F.; Ahmad, M.; Fässler, R.; Andersson, K.-E. Erectile dysfunction in cyclic GMP-dependent kinase I-deficient mice. Proc. Natl. Acad. Sci. USA 2000, 97, 2349–2354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangiorgi, G.; Colantonio, R.; Antonini, G.; Savino, A.; Sperandio, M. [Percutaneous intervention therapy for vascular erectile dysfunction]. G. Ital. Cardiol. 2016, 17, 12S-21. [Google Scholar]
- Moriel, E.Z.; Mehringer, C.M.; Schwartz, M.; Rajfer, J. Pulmonary Migration of Coils Inserted for Treatment of Erectile Dysfunction Caused by Venous Leakage. J. Urol. 1993, 149, 1316–1318. [Google Scholar] [CrossRef]
- Beavo, J.A. Cyclic nucleotide phosphodiesterases: Functional implications of multiple isoforms. Physiol. Rev. 1995, 75, 725–748. [Google Scholar] [CrossRef]
- Furchgott, R.F.; Zawadzki, J.V. The obligatory role of endothelial cells in the relaxation of arterial smooth muscle by acetylcholine. Nat. Cell Biol. 1980, 288, 373–376. [Google Scholar] [CrossRef]
- Vita, J.A.; Keaney, J.F. Endothelial Function. Circulation 2002, 106, 640–642. [Google Scholar] [CrossRef] [Green Version]
- Sangiorgi, G.; Pizzuto, A.; Diehm, N.; Greco, F.; Fusco, F.; Chiricolo, G.; Vismara, A.; Altieri, V.; Cereda, A. Sante Bongoet al. Endovascular therapy for erectile dysfunction: A state of the art re-view. Minerva Cardioangiol. 2020, 10. [Google Scholar] [CrossRef]
- Brotons, F.B.; Campos, J.C.; Gonzalez-Correales, R.; Martin-Morales, A.; Moncada, I.; Pomerol, J.M. Core document on erectile dysfunction: Key aspects in the care of a patient with erectile dysfunction. Int. J. Impot. Res. 2004, 16, S26–S39. [Google Scholar] [CrossRef] [Green Version]
- De Angelis, L.; Marfella, M.A.; Siniscalchi, M.; Marino, L.; Nappo, F.; Giugliano, F.; De Lucia, D. Erectile and endothelial dysfunction in Type II diabetes: A possible link. Diabetologia 2001, 44, 1155–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gazzaruso, C.; Giordanetti, S.; De Amici, E.; Bertone, G.; Falcone, C.; Geroldi, D.; Fratino, P.; Solerte, S.B.; Garzaniti, A. Relationship between Erectile Dysfunction and Silent Myocardial Ischemia in Apparently Uncomplicated Type 2 Diabetic Patients. Circulation 2004, 110, 22–26. [Google Scholar] [CrossRef] [Green Version]
- Gupta, B.P.; Murad, M.H.; Clifton, M.M.; Prokop, L.; Nehra, A.; Kopecky, S.L. The Effect of Lifestyle Modification and Cardiovascular Risk Factor Reduction on Erectile Dysfunction. Arch. Intern. Med. 2011, 171, 1797–1803. [Google Scholar] [CrossRef] [Green Version]
- Rosen, M.P.; Greenfield, A.J.; Walker, T.G.; Grant, P.; Dubrow, J.; Bettmann, M.A.; Fried, L.E.; Goldstein, I. Cigarette Smoking: An Independent Risk Factor for Atherosclerosis in the Hypogastric-Cavernous Arterial Bed of Men with Arteriogenic Impotence. J. Urol. 1991, 145, 759–763. [Google Scholar] [CrossRef]
- Gandaglia, G.; Briganti, A.; Jackson, G.; Kloner, R.A.; Montorsi, F.; Montorsi, P.; Vlachopoulos, C. A Systematic Review of the Association Between Erectile Dysfunction and Cardiovascular Disease. Eur. Urol. 2014, 65, 968–978. [Google Scholar] [CrossRef]
- Thompson, I.M.; Tangen, C.M.; Goodman, P.J.; Probstfield, J.L.; Moinpour, C.M.; Coltman, C.A. Erectile Dysfunction and Subsequent Cardiovascular Disease. JAMA 2005, 294, 2996–3002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osondu, C.U.; Vo, B.; Oni, E.T.; Blaha, M.J.; Veledar, E.; Feldman, T.; Agatston, A.S.; Nasir, K.; Aneni, E.C. The relationship of erectile dysfunction and subclinical cardiovascular disease: A systematic review and meta-analysis. Vasc. Med. 2018, 23, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Uddin, S.M.I.; Mirbolouk, M.; Dardari, Z.; Feldman, D.I.; Cainzos-Achirica, M.; DeFilippis, A.P.; Greenland, P.; Blankstein, R.; Billups, K.L.; Miner, M.M.; et al. Erectile Dysfunction as an Independent Predictor of Future Cardiovascular Events. Circulation 2018, 138, 540–542. [Google Scholar] [CrossRef]
- Montorsi, F.; Briganti, A.; Salonia, A.; Rigatti, P.; Margonato, A.; Macchi, A.; Galli, S.; Ravagnani, P.M.; Montorsi, P. Erectile Dysfunction Prevalence, Time of Onset and Association with Risk Factors in 300 Consecutive Patients with Acute Chest Pain and Angiographically Documented Coronary Artery Disease. Eur. Urol. 2003, 44, 360–365. [Google Scholar] [CrossRef]
- Watts, G.F.; Chew, K.-K.; Stuckey, B.G. The erectile–endothelial dysfunction nexus: New opportunities for cardiovascular risk prevention. Nat. Clin. Pr. Neurol. 2007, 4, 263–273. [Google Scholar] [CrossRef]
- Rosen, M.P.; Greenfield, A.J.; Walker, T.G.; Grant, P.; Guben, J.K.; Dubrow, J.; Bettmann, M.A.; Goldstein, I. Arteriogenic Impotence: Findings in 195 Impotent Men Examined with Selective Internal Pudendal Angiography. Radiology 1990, 174, 1043–1048. [Google Scholar] [CrossRef]
- Montorsi, P.; Ravagnani, P.M.; Galli, S.; Rotatori, F.; Veglia, F.; Briganti, A.; Salonia, A.; Dehò, F.; Rigatti, P.; Montorsi, F.; et al. Association between erectile dysfunction and coronary artery disease. Role of coronary clinical presentation and extent of coronary vessels involvement: The COBRA trial. Eur. Heart J. 2006, 27, 2632–2639. [Google Scholar] [CrossRef]
- Lehman, T.P.; Jacobs, J.A. Etiology of Diabetic Impotence. J. Urol. 1983, 129, 291–294. [Google Scholar] [CrossRef]
- Whitehead, E.D.; Klyde, B.J. Diabetes-Related Impotence in the Elderly. Clin. Geriatr. Med. 1990, 6, 771–795. [Google Scholar] [CrossRef]
- Koncz, L.; Balodimos, M. Impotence in diabetes mellitus. Med. Times 1970, 98, 159–170. [Google Scholar]
- Gazzaruso, C.; Solerte, S.B.; Pujia, A.; Coppola, A.; Vezzoli, M.; Salvucci, F.; Valenti, C.; Giustina, A.; Garzaniti, A. Erectile Dysfunction as a Predictor of Cardiovascular Events and Death in Diabetic Patients With Angiographically Proven Asymptomatic Coronary Artery Disease. J. Am. Coll. Cardiol. 2008, 51, 2040–2044. [Google Scholar] [CrossRef] [Green Version]
- Seftel, A.D.; Sun, P.; Swindle, R. The prevalence of hypertension, hyperlipidemia, diabetes mellitus and de-pression in men with erectile dysfunction. J. Urol. 2004, 171, 2341–2345. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, F.A.; Leriche, A.; Jaudinot, E.O.; De Gendre, A.S. Prevalence of erectile dysfunction among 7689 patients with diabetes or hypertension, or both. Urology 2004, 64, 1196–1201. [Google Scholar] [CrossRef] [PubMed]
- Behr-Roussel, D.; Gorny, D.; Mevel, K.; Compagnie, S.; Kern, P.; Sivan, V.; Bernabé, J.; Bedigian, M.P.; Alexandre, L.; Giuliano, F. Erectile dysfunction: An early marker for hypertension? A longitudinal study in spontaneously hypertensive rats. Am. J. Physiol. Integr. Comp. Physiol. 2005, 288, R276–R283. [Google Scholar] [CrossRef]
- Gandaglia, G.; Briganti, A.; Montorsi, P.; Mottrie, A.; Salonia, A.; Montorsi, F. Diagnostic and Therapeutic Implications of Erectile Dysfunction in Patients with Cardiovascular Disease. Eur. Urol. 2016, 70, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Inman, B.A.; Sauver, J.L.S.; Jacobson, D.J.; McGree, M.E.; Nehra, A.; Lieber, M.M.; Roger, V.L.; Jacobsen, S.J. A Population-Based, Longitudinal Study of Erectile Dysfunction and Future Coronary Artery Disease. Mayo Clin. Proc. 2009, 84, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Araujo, A.B.; Travison, T.G.; Ganz, P.; Chiu, G.R.; Kupelian, V.; Rosen, R.C.; Hall, S.A.; McKinlay, J.B. Erectile Dysfunction and Mortality. J. Sex. Med. 2009, 6, 2445–2454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, B.G.; Levine, L.A.; Comstock, G.; Stecher, V.J.; Kloner, R.A. Cardiac Uses of Phosphodiesterase-5 Inhibitors. J. Am. Coll. Cardiol. 2012, 59, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Andersson, D.P.; Lagerros, Y.T.; Grotta, A.; Bellocco, R.; Lehtihet, M.; Holzmann, M.J. Association between treatment for erectile dysfunction and death or cardiovascular outcomes after myocardial infarction. Heart 2017, 103, 1264–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, S.G.; Hutchings, D.C.; Woodward, M.; Rahimi, K.; Rutter, M.K.; Kirby, M.; Hackett, G.; Trafford, A.W.; Heald, A.H. Phosphodiesterase type-5 inhibitor use in type 2 diabetes is associated with a reduction in all-cause mortality. Heart 2016, 102, 1750–1756. [Google Scholar] [CrossRef] [Green Version]
- Andersson, D.P.; Landucci, L.; Lagerros, Y.T.; Grotta, A.; Bellocco, R.; Lehtihet, M.; Holzmann, M.J. Association of Phosphodiesterase-5 Inhibitors Versus Alprostadil With Survival in Men With Coronary Artery Disease. J. Am. Coll. Cardiol. 2021, 77, 1535–1550. [Google Scholar] [CrossRef]
- Hutchings, D.C.; Anderson, S.G.; Caldwell, J.L.; Trafford, A.W. Phosphodiesterase-5 inhibitors and the heart: Compound cardioprotection? Heart 2018, 104, 1244–1250. [Google Scholar] [CrossRef]
- Burnett, A.L.; Nehra, A.; Breau, R.H.; Culkin, D.J.; Faraday, M.M.; Hakim, L.S.; Heidelbaugh, J.; Khera, M.; McVary, K.T.; Miner, M.M.; et al. Erectile Dysfunction: AUA Guideline. J. Urol. 2018, 200, 633–641. [Google Scholar] [CrossRef]
- Ahmed, K.; Hatzimouratidis, K.; Muneer, A. Male Sexual Dysfunction and Hypogonadism Guidelines for the Aging Male. Eur. Urol. Focus 2017, 3, 514–516. [Google Scholar] [CrossRef]
- Hoeben, A.; Landuyt, B.; Highley, M.S.; Wildiers, H.; Van Oosterom, A.T.; De Bruijn, E.A. Vascular Endothelial Growth Factor and Angiogenesis. Pharmacol. Rev. 2004, 56, 549–580. [Google Scholar] [CrossRef]
- Raica, M.; Cimpean, A.M. Platelet-Derived Growth Factor (PDGF)/PDGF Receptors (PDGFR) Axis as Target for Antitumor and Antiangiogenic Therapy. Pharmaceuticals 2010, 3, 572–599. [Google Scholar] [CrossRef] [Green Version]
- Murakami, M.; Simons, M. Fibroblast growth factor regulation of neovascularization. Curr. Opin. Hematol. 2008, 15, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Van Cruijsen, H.; Giaccone, G.; Hoekman, K. Epidermal growth factor receptor and angiogenesis: Opportunities for combined anticancer strategies. Int. J. Cancer 2005, 117, 883–888. [Google Scholar] [CrossRef]
- Jacobo, S.M.P.; Kazlauskas, A. Insulin-like Growth Factor 1 (IGF-1) Stabilizes Nascent Blood Vessels. J. Biol. Chem. 2015, 290, 6349–6360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, X.-G.; Li, S.-W.; Zheng, X.-M.; Hu, L.-Q.; Hu, W.-L.; Luo, Y. The effect of platelet-rich plasma on cavernous nerve regeneration in a rat model. Asian J. Androl. 2009, 11, 215–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.; Wu, Y.; Ho, H.; Chen, K.; Sheu, M.; Chiang, H. The Neuroprotective Effect of Platelet-rich Plasma on Erectile Function in Bilateral Cavernous Nerve Injury Rat Model. J. Sex. Med. 2012, 9, 2838–2848. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-N.; Wu, C.-C.; Sheu, M.-T.; Chen, K.-C.; Ho, H.-O.; Chiang, H.-S. Optimization of platelet-rich plasma and its effects on the recovery of erectile function after bilateral cavernous nerve injury in a rat model. J. Tissue Eng. Regen. Med. 2013, 10, E294–E304. [Google Scholar] [CrossRef] [PubMed]
- Epifanova, M.V.; Chalyi, M.E.; Krasnov, A.O. Investigation of mechanisms of action of growth factors of autol-ogous platelet-rich plasma used to treat erectile dysfunction. Urologiia 2017, 4, 46–48. [Google Scholar] [CrossRef]
- Matz, E.L.; Pearlman, A.M.; Terlecki, R.P. Safety and feasibility of platelet rich fibrin matrix injections for treatment of common urologic conditions. Investig. Clin. Urol. 2018, 59, 61–65. [Google Scholar] [CrossRef]
- Reed-Maldonado, A.B.; Lue, T.F. The Current Status of Stem-Cell Therapy in Erectile Dysfunction: A Review. World J. Mens Heal. 2016, 34, 155–164. [Google Scholar] [CrossRef]
- Shan, H.; Chen, F.; Zhang, T.; He, S.; Xu, L.; Wei, A. Stem Cell Therapy for Erectile Dysfunction of Cavernous Nerve Injury Rats: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0121428. [Google Scholar] [CrossRef] [PubMed]
- Soebadi, M.A.; Moris, L.; Castiglione, F.; Weyne, E.; Albersen, M. Advances in stem cell research for the treatment of male sexual dysfunctions. Curr. Opin. Urol. 2016, 26, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Bahk, J.Y.; Jung, J.H.; Han, H.; Min, S.K.; Lee, Y.S. Treatment of diabetic impotence with umbilical cord blood stem cell intracavernosal transplant: Preliminary report of 7 cases. Exp. Clin. Transplant. 2010, 8, 150–160. [Google Scholar] [PubMed]
- Yiou, R.; Hamidou, L.; Birebent, B.; Bitari, D.; Lecorvoisier, P.; Contremoulins, I.; Khodari, M.; Rodriguez, A.-M.; Augustin, D.; Roudot-Thoraval, F.; et al. Safety of Intracavernous Bone Marrow-Mononuclear Cells for Postradical Prostatectomy Erectile Dysfunction: An Open Dose-Escalation Pilot Study. Eur. Urol. 2016, 69, 988–991. [Google Scholar] [CrossRef] [PubMed]
- Haahr, M.K.; Jensen, C.H.; Toyserkani, N.M.; Andersen, D.C.; Damkier, P.; Sørensen, J.A.; Sheikh, S.P.; Lund, L. A 12-Month Follow-up After a Single Intracavernous Injection of Autologous Adipose-Derived Regenerative Cells in Patients with Erectile Dysfunction Following Radical Prostatectomy: An Open-Label Phase I Clinical Trial. Urology 2018, 121, 203.e6–203.e13. [Google Scholar] [CrossRef] [Green Version]
- Levy, J.A.; Marchand, M.; Iorio, L.; Cassini, W.; Zahalsky, M.P. Determining the Feasibility of Managing Erectile Dysfunction in Humans With Placental-Derived Stem Cells. J. Am. Osteopat. Assoc. 2016, 116, e1–e5. [Google Scholar] [CrossRef] [Green Version]
- Casiraghi, F.; Remuzzi, G.; Abbate, M.; Perico, N. Multipotent Mesenchymal Stromal Cell Therapy and Risk of Malignancies. Stem Cell Rev. Rep. 2013, 9, 65–79. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Neurogenic
|
Endocrinologic
|
Vasculogenic
|
Drug-induced depression
|
Systemic diseases and general ill health
|
Local penile (cavernous) factors
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sangiorgi, G.; Cereda, A.; Benedetto, D.; Bonanni, M.; Chiricolo, G.; Cota, L.; Martuscelli, E.; Greco, F. Anatomy, Pathophysiology, Molecular Mechanisms, and Clinical Management of Erectile Dysfunction in Patients Affected by Coronary Artery Disease: A Review. Biomedicines 2021, 9, 432. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9040432
Sangiorgi G, Cereda A, Benedetto D, Bonanni M, Chiricolo G, Cota L, Martuscelli E, Greco F. Anatomy, Pathophysiology, Molecular Mechanisms, and Clinical Management of Erectile Dysfunction in Patients Affected by Coronary Artery Disease: A Review. Biomedicines. 2021; 9(4):432. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9040432
Chicago/Turabian StyleSangiorgi, Giuseppe, Alberto Cereda, Daniela Benedetto, Michela Bonanni, Gaetano Chiricolo, Linda Cota, Eugenio Martuscelli, and Francesco Greco. 2021. "Anatomy, Pathophysiology, Molecular Mechanisms, and Clinical Management of Erectile Dysfunction in Patients Affected by Coronary Artery Disease: A Review" Biomedicines 9, no. 4: 432. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9040432