
Comparative Evaluation of New Needleless Local Anesthetic System (INJEX) and Conventional Syringe Needle Technique during Pulpotomy Treatment: A Randomized Clinical Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Ethical Clearance, and Informed Consent
2.2. Sample Size Estimation
2.3. Participant Selection
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
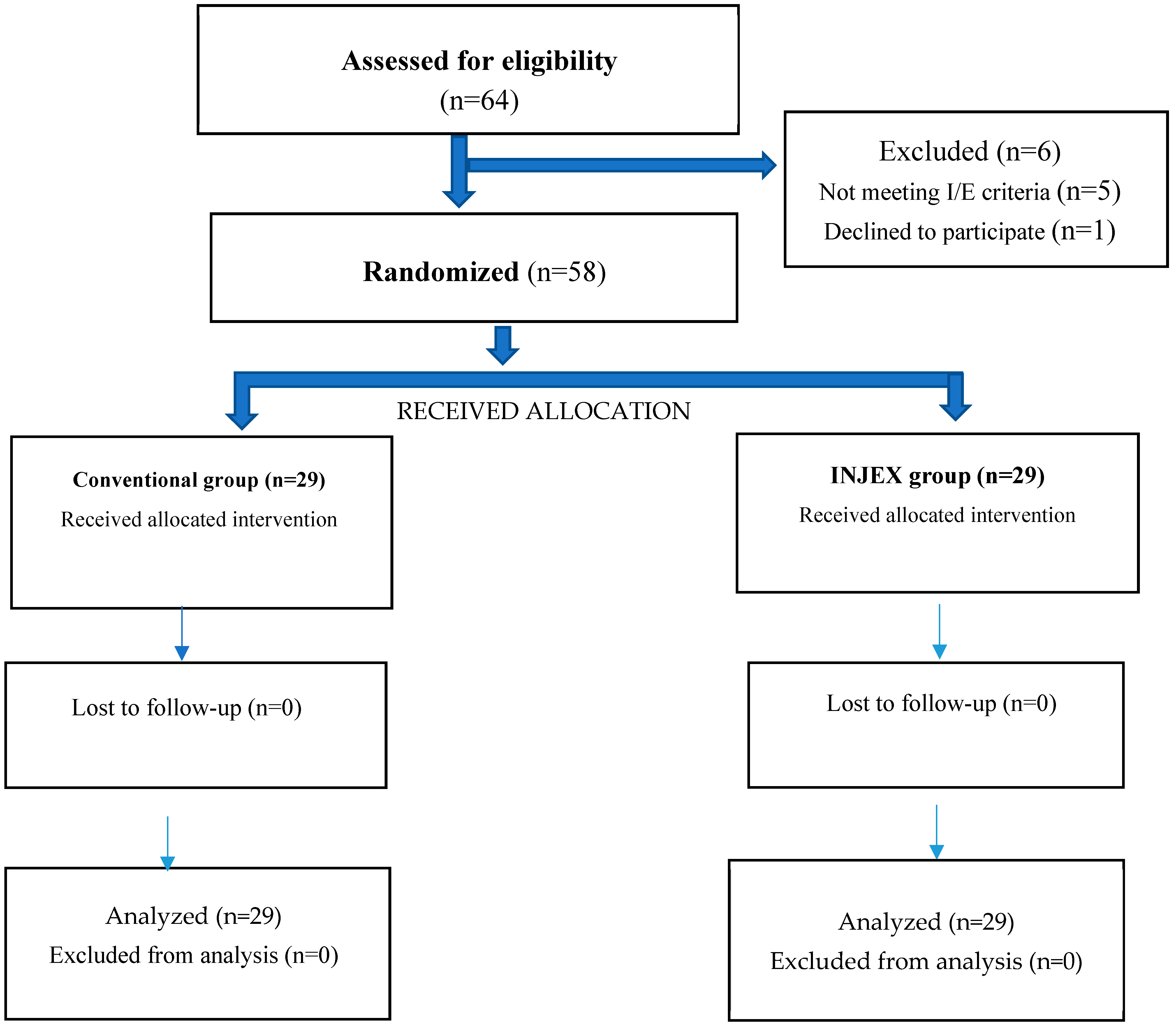
2.3.3. Randomization and Allocation Concealment
2.3.4. Study Groups
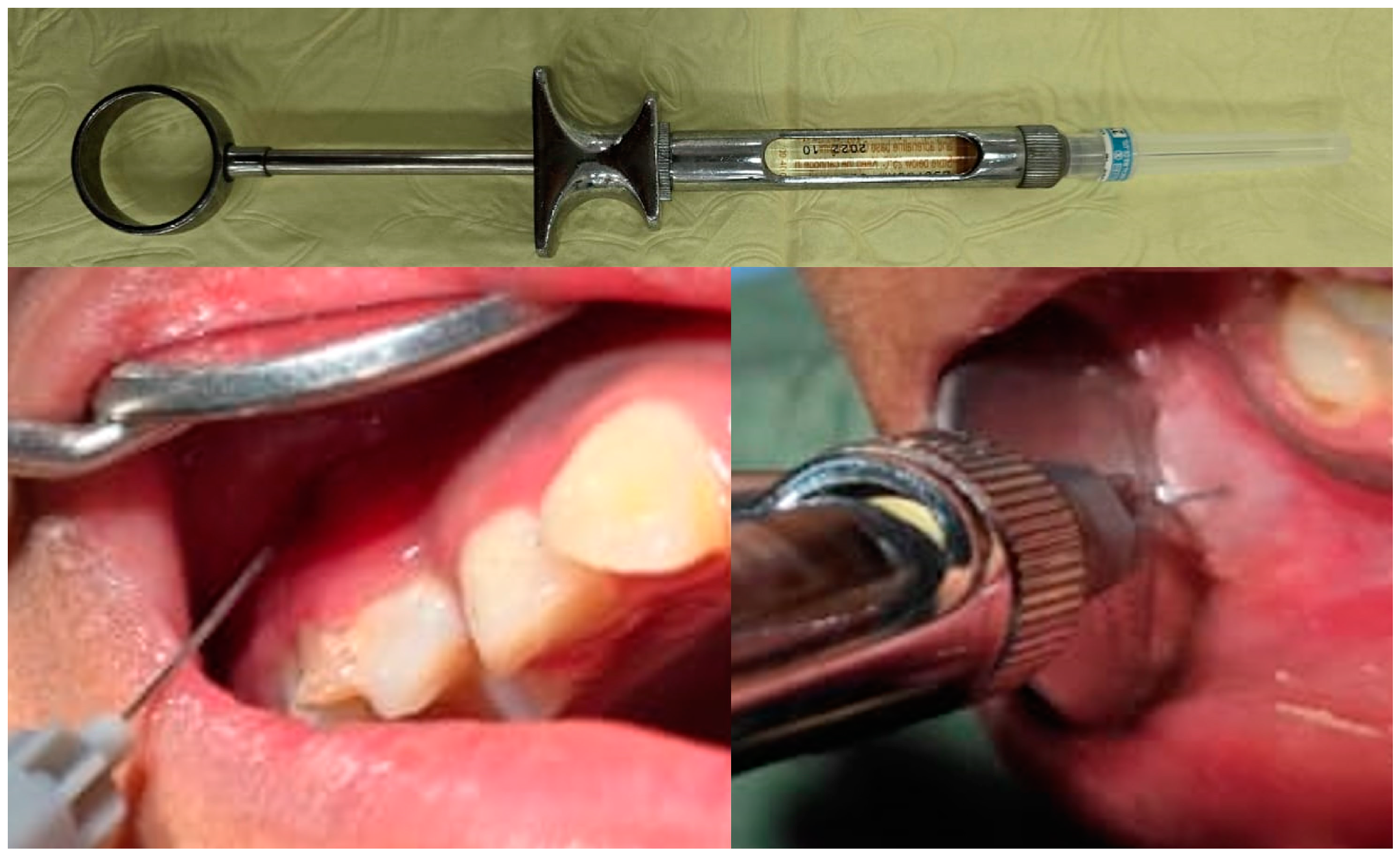
2.4. Intervention Procedure
2.5. Outcomes
2.6. Primary Outcomes
2.6.1. Face, Legs, Activity, Cry, Consolability Scale
2.6.2. Wong–Baker FACES Pain Rating Scale
2.7. Secondary Outcome
2.7.1. Time of Local Anesthesia Administration
2.7.2. Frankl Behavior Rating Scale [25]
2.7.3. Pulse Rate
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alameeri, A.A.; AlShamsi, H.A.; Murad, A.; Alhammadi, M.M.; Alketbi, M.H.; AlHamwi, A.; Rawi, N.H.A.; Kawas, S.A.; Mohammed, M.M.; Shetty, S.R. The feasibility of needleless jet injection versus conventional needle local anesthesia during dental procedures: A systematic review. J. Korean Assoc. Oral Maxillofac. Surg. 2022, 48, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Ogle, O.E.; Mahjoubi, G. Local anesthesia: Agents, techniques, and complications. Dent. Clin. N. Am. 2012, 56, 133–148. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatric Dentistry. Use of local anesthesia for pediatric dental patients. In The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2023; pp. 385–392. [Google Scholar]
- Shankar, P.; Chellathurai, B.N.K.; Kumar, S.A.; Mahendra, J.; Mugri, M.H.; Sayed, M.; Almagbol, M.; Al Wadei, M.H.D.; Vijayalakshmi, R.; Ambalavanan, N.; et al. A comparison in patient comfort using conventional syringe and needleless jet anesthesia technique in periodontal surgery-a split-mouth randomized clinical trial. Medicina 2022, 58, 278. [Google Scholar] [CrossRef] [PubMed]
- Crellin, D.J.; Harrison, D.; Santamaria, N.; Babl, F.E. Systematic review of the Face, Legs, Activity, Cry and Consolability scale for assessing pain in infants and children. Pain 2015, 156, 2132–2151. [Google Scholar] [CrossRef] [PubMed]
- Voepel-Lewis, T.; Merkel, S.; Tait, A.R.; Trzcinka, A.; Malviya, S. The Reliability and Validity of the Face, Legs, Activity, Cry, Consolability Observational Tool as a Measure of Pain in Children with Cognitive Impairment. Anesth. Analg. 2002, 95, 1224–1229. [Google Scholar] [CrossRef] [PubMed]
- Willis, M.H.W.; Merkel, S.; Voepel-Lewis, T.; Malviya, S. FLACC Behavioral Pain Assessment Scale: A comparison with the child’s self-report. Pediatr. Nurs. 2003, 29, 195–198. [Google Scholar] [PubMed]
- Mathur, J.; Diwanji, A.; Sarvaiya, B.; Sharma, D. Identifying Dental Anxiety in Children’s Drawings and correlating It with Frankl’s Behavior Rating Scale. Int. J. Clin. Pediatr. Dent. 2017, 10, 24–28. [Google Scholar] [CrossRef]
- Appukuttan, D.P. Strategies to manage patients with dental anxiety and dental phobia: Literature review. Clin. Cosmet. Investig. Dent. 2016, 8, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, L.; Abd Al Gawad, R.; Aly, M. Pain control of needle-less jet anesthesia versus conventional infiltration anesthesia for pulpotomy of maxillary primary molars in children: A randomized controlled trial. Adv. Dent. J. 2023, 5, 198–209. [Google Scholar] [CrossRef]
- Glaesmer, H.; Geupel, H.; Haak, R. A controlled trial on the effect of hypnosis on dental anxiety in tooth removal patients. Patient Educ. Couns. 2015, 98, 1112–1115. [Google Scholar] [CrossRef]
- Kuzin, A.V. Practical advices in choosing local anesthesia tools in dentistry. Management of carpule’s quality in local anesthesia in dentistry. Stomatologiia 2014, 93, 37–39. [Google Scholar] [PubMed]
- Al-Melh, M.A.; Andersson, L. Comparison of topical anesthetics (EMLA/Oraqix vs. benzocaine) on pain experienced during palatal needle injection. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, e16–e20. [Google Scholar] [CrossRef]
- Friedman, M.J.; Hochman, M.N. The AMSA injection: A new concept for local anesthesia of maxillary teeth using a computer-controlled injection system. Quintessence Int. 1998, 29, 297–303. [Google Scholar] [PubMed]
- Kanaa, M.D.; Meechan, J.G.; Corbett, I.P.; Whitworth, J.M. Speed of injection influences efficacy of inferior alveolar nerve blocks: A double-blind randomized controlled trial in volunteers. J. Endod. 2006, 32, 919–923. [Google Scholar] [CrossRef] [PubMed]
- Gozdemir, M.; Demircioglu, R.I.; Karabayirli, S.; Sert, H.; Muslu, B.; Usta, B.; Yazici, U. A needle-free injection system (INJEX™) with lidocaine for epidural needle insertion: A randomized controlled trial. Pak. J. Med. Sci. 2016, 32, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Schoppink, J.; Fernandez Rivas, D. Jet injectors: Perspectives for small volume delivery with lasers. Adv. Drug Deliv. Rev. 2022, 182, 114109. [Google Scholar] [CrossRef] [PubMed]
- Brunton, P.A.; McLean, M.; Vedagiri, S.; McKeage, J.; Ruddy, B.; Weatherly, K.; White, D.; Taberner, A.; Loch, C. Jet injection needle-free dental anaesthesia: Initial findings. J. Dent. 2022, 122, 104165. [Google Scholar] [CrossRef]
- Munshi, A.K.; Hegde, A.; Bashir, N. Clinical evaluation of the efficacy of anesthesia and patient preference using the needle-less jet syringe in pediatric dental practice. J. Clin. Pediatr. Dent. 2001, 25, 131–136. [Google Scholar] [CrossRef]
- Arapostathis, K.N.; Dabarakis, N.N.; Coolidge, T.; Tsirlis, A.; Kotsanos, N. Comparison of acceptance, preference, and efficacy between jet injection INJEX and local infiltration anesthesia in 6 to 11 year old dental patients. Anesth. Prog. 2010, 57, 3–12. [Google Scholar] [CrossRef]
- Theocharidou, A.; Arhakis, A.; Kotsanos, N.; Arapostathis, K. Jet or conventional local anaesthesia? A randomized controlled split mouth study. Clin. Oral Investig. 2021, 25, 6813–6819. [Google Scholar] [CrossRef]
- Deepak, V.; Challa, R.R.; Kamatham, R.; Nuvvula, S. Comparison of a new auto-controlled injection system with traditional syringe for mandibular infiltrations in children: A randomized clinical trial. Anesth. Essays Res. 2017, 11, 431–438. [Google Scholar]
- Merkel, S.I.; Voepel-Lewis, T.; Shayevitz, J.R.; Malviya, S. The FLACC: A behavioral scale for scoring postoperative pain in young children. Pediatr. Nurs. 1997, 23, 293–297. [Google Scholar] [PubMed]
- Garra, G.; Singer, A.J.; Domingo, A.; Thode, H.C., Jr. The Wong-Baker pain FACES scale measures pain, not fear. Pediatr. Emerg. Care 2013, 29, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Shital, K.; Rohan, B.; Megha, P.; Nilay, S. Pattern and knowledge of Wright’s modification of Frankl’s behavior rating scale followed among postgraduate students of pediatric dentistry in Ahmedabad City—A survey. Adv. Hum. Biol. 2015, 5, 39–42. [Google Scholar]
- Gordon, D.; Heimberg, R.G.; Tellez, M.; Ismail, A.I. A critical review of approaches to the treatment of dental anxiety in adults. J. Anxiety Disord. 2013, 27, 365–378. [Google Scholar] [CrossRef] [PubMed]
- Klingberg, G.; Broberg, A.G. Dental fear/anxiety and dental behaviour management problems in children and adolescents: A review of prevalence and concomitant psychological factors. Int. J. Paediatr. Dent. 2007, 17, 391–406. [Google Scholar] [CrossRef] [PubMed]
- Milgrom, P.; Coldwell, S.E.; Getz, T.; Weinstein, P.; Ramsay, D.S. Four dimensions of fear of dental local anesthesia administration. J. Am. Dent. Assoc. 1997, 128, 756–766. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.C.A.; Amorim, K.S.; Nascimento, E.M.D., Jr.; Duarte, A.C.B.; Groppo, F.C.; Takeshita, W.M.; Souza, L.M.A. Assessment of anesthetic properties and pain during needleless jet injection anesthesia: A randomized clinical trial. J. Appl. Oral Sci. 2019, 27, e20180195. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S. Newer delivery systems for local anesthesia in dentistry. J. Pharm. Sci. Res. 2015, 7, 252–255. [Google Scholar]
- Mohizin, A.; Kim, J.K. Current engineering and clinical aspects of needle-free injectors: A review. J. Mech. Sci. Technol. 2018, 32, 5737–5747. [Google Scholar] [CrossRef]
- Altan, H.; Belevcikli, M.; Coşgun, A.; Demir, O. Comparative evaluation of pain perception with a new needle-free system and dental needle method in children: A randomized clinical trial. BMC Anesthesiol. 2021, 21, 301. [Google Scholar] [CrossRef] [PubMed]
- Ocak, H.; Akkoyun, E.F.; Çolpak, H.A.; Demetoğlu, U.; Yücesoy, T.; Kılıç, E.; Alkan, A. Is the jet injection effective for teeth extraction? J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Lautenbacher, S.; Kunz, M.; Strate, P.; Nielsen, J.; Arendt-Nielsen, L. Age effects on pain thresholds, temporal summation and spatial summation of heat and pressure pain. Pain 2005, 115, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Kaya, E.; Yıldırım, S. Effect of a needle-free system versus traditional anesthesia on pain perception during palatal local anesthesia administration in children. Int. J. Paediatr. Dent. 2023, 33, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Al-kaf, A.G.A.; Othman, A.M. A review on needle free local anesthesia administration. Univ. J. Pharm. Res. 2017, 2, 21–25. [Google Scholar]
- Makade, C.S.; Shenoi, P.R.; Gunwal, M.K. Comparison of acceptance, preference and efficacy between pressure anesthesia and classical needle infiltration anesthesia for dental restorative procedures in adult patients. J. Conserv. Dent. 2014, 17, 169–174. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| SI No. | Parameter | Conventional Syringe Needle n (%) | INJEX n (%) | p-Value |
|---|---|---|---|---|
| 1 | Age | 0.007 ** | ||
| 6–9 years old | 19 (32.75) | 15 (25.8) | ||
| 9–12 years old | 10 (17.24) | 14 (24.13) | ||
| 2 | Gender | 0.189 | ||
| Male | 12 (20.68) | 18 (31.03) | ||
| Female | 17 (29.31) | 11 (18.96) |
| SI No. | Parameter | Conventional Syringe Needle (Mean ± SD) | INJEX (Mean ± SD) | p-Value |
|---|---|---|---|---|
| 1 | Time required for local anesthesia administration in minutes | 1.3 ± 0.39 | 0.34 ± 0.084 | <0.001 *** |
| 2 | Pulse rate | |||
| Before administration of local anesthesia | 92.57 ± 11.3 | 94.14 ± 10.27 | 0.583 | |
| During administration of local anesthesia | 102.93 ± 16.51 | 95.48 ± 13.94 | 0.0687 | |
| 1 min after local anesthesia administration | 95.79 ± 13.23 | 95.03 ± 10.67 | 0.811 |
| SI No. | Parameter | Conventional Syringe Needle [Median (Q1,Q3)] | INJEX [Median (Q1,Q3)] | p-Value |
|---|---|---|---|---|
| 1 | FBRS | |||
| Before anesthesia | 3 (3,4) | 4 (3,4) | 0.177 | |
| During anesthesia | 2 (2,3) | 3 (3,4) | <0.001 *** | |
| After anesthesia | 3 (3,4) | 3 (3,4) | 0.184 | |
| 2 | FLACC scale | 7( 4,10) | 2 (0,4) | 0.005 ** |
| 3 | WBS | |||
| Before procedure | 1 (0,2) | 1 (0,0) | <0.326 | |
| Immediately after local anesthesia administration | 4 (2,6) | 0 (0,2) | <0.001 *** | |
| During treatment | 0 (0,2) | 0 (0,2) | 0.603 | |
| At the end of treatment | 0 (0,0) | 0 (0,0) | 0.542 |
| SI No. | Parameter | Group | Comparison | Mean ± SD/ Median (Q1,Q3) | p-Value |
|---|---|---|---|---|---|
| 1. | Pulse rate | Conventional syringe needle | Before versus during | 92.57 ± 11.3 102.93 ± 16.51 | 0.002 ** |
| Before versus after | 92.57 ± 11.3 95.79 ± 13.23 | 0.289 | |||
| During versus after | 102.93 ± 16.51 95.79 ± 13.23 | <0.001 *** | |||
| INJEX | Before versus during | 94.14 ± 10.27 95.48 ± 13.94 | 0.449 | ||
| Before versus after | 94.14 ± 10.27 95.03 ± 10.67 | 0.362 | |||
| During versus after | 95.48 ± 13.94 95.03 ± 10.67 | 0.727 | |||
| 2. | FBRS | Conventional syringe needle | Before versus during | 3 (3,4) 2 (2,3) | <0.001 *** |
| Before versus after | 3 (3,4) 3 (3,4) | 0.06 | |||
| During versus after | 2 (2,3) 3 (3,4) | <0.001 *** | |||
| INJEX | Before versus during | 4 (3,4) 3 (2,3) | 0.007 *** | ||
| Before versus after | 4 (3,4) 3 (3,4) | 0.145 | |||
| During versus after | 3 (2,3) 3 (3,4) | 0.437 |
| SI No. | Parameters | Group | Comparison | Median (Q1,Q3) | p-Value |
|---|---|---|---|---|---|
| 1. | WBS | Conventional syringe needle | Before versus immediately after local anesthesia administration | 1 (0,2) 4 (2,6) | <0.001 *** |
| Before versus during treatment | 1 (0,2) 0 (0,2) | 0.005 ** | |||
| Before versus at the end of treatment | 1 (0,2) 0 (0,0) | <0.001 *** | |||
| Immediately after injection versus during treatment | 4 (2,6) 0 (0,2) | <0.001 *** | |||
| Immediately after injection versus at the end of treatment | 4 (2,6) 0 (0,0) | <0.001 *** | |||
| During treatment versus at the end of treatment | 0 (0,2) 0 (0,0) | 0.04 * | |||
| 2. | WBS | INJEX | Before versus immediately after injection | 1 (0,0) 0 (0,2) | 0.01 ** |
| Before versus during treatment | 1 (0,0) 0 (0,2) | 0.152 | |||
| Before versus at the end of treatment | 1 (0,0) 0 (0,0) | 0.824 | |||
| Immediately after injection versus during treatment | 0 (0,2) 0 (0,2) | 0.135 | |||
| Immediately after injection versus at the end of treatment | 0 (0,2) 0 (0,0) | 0.03 ** | |||
| During treatment versus at the end of treatment | 0 (0,2) 0 (0,0) | 0.182 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vishwanathaiah, S.; Albar, N.H.; Alraghi, F.T.A.; Jaferi, N.E.M.; Tumayhi, I.A.M.; Panda, S.; Khormi, F.A.H.; Jaafari, A.H.H.; Abiri, Z.A.I.; Maganur, P.C. Comparative Evaluation of New Needleless Local Anesthetic System (INJEX) and Conventional Syringe Needle Technique during Pulpotomy Treatment: A Randomized Clinical Trial. Children 2024, 11, 514. https://0-doi-org.brum.beds.ac.uk/10.3390/children11050514
Vishwanathaiah S, Albar NH, Alraghi FTA, Jaferi NEM, Tumayhi IAM, Panda S, Khormi FAH, Jaafari AHH, Abiri ZAI, Maganur PC. Comparative Evaluation of New Needleless Local Anesthetic System (INJEX) and Conventional Syringe Needle Technique during Pulpotomy Treatment: A Randomized Clinical Trial. Children. 2024; 11(5):514. https://0-doi-org.brum.beds.ac.uk/10.3390/children11050514
Chicago/Turabian StyleVishwanathaiah, Satish, Nassreen H. Albar, Fatemah Tawfeg Abkar Alraghi, Noor Eissa Mousa Jaferi, Ishraq Abdullah Mohammed Tumayhi, Suman Panda, Fatima Ali Hassan Khormi, Atlal Hassan Hussain Jaafari, Zahra Ahmed Ibrahim Abiri, and Prabhadevi C. Maganur. 2024. "Comparative Evaluation of New Needleless Local Anesthetic System (INJEX) and Conventional Syringe Needle Technique during Pulpotomy Treatment: A Randomized Clinical Trial" Children 11, no. 5: 514. https://0-doi-org.brum.beds.ac.uk/10.3390/children11050514