


Body Image and Other Mood Vulnerabilities in Adolescents with Polycystic Ovary Syndrome and Metabolic Alterations
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Cohort
2.2. Psychometric Questionnaires
2.2.1. Body Image
2.2.2. Eating Disorders
2.2.3. Mood
2.2.4. Perceived Stress
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Teede, H.J.; Tay, C.T.; Laven, J.J.E.; Dokras, A.; Moran, L.J.; Piltonen, T.T.; Costello, M.F.; Boivin, J.; Redman, L.M.; Boyle, J.A.; et al. International PCOS Network. Recommendations from the 2023 international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Eur. J. Endocrinol. 2023, 189, G43–G64. [Google Scholar] [CrossRef]
- Peña, A.S.; Witchel, S.F.; Hoeger, K.M.; Oberfield, S.E.; Vogiatzi, M.G.; Misso, M.; Garad, R.; Dabadghao, P.; Teede, H. Adolescent polycystic ovary syndrome according to the international evidence-based guideline. BMC Med. 2020, 18, 72. [Google Scholar] [CrossRef]
- WHO. Adolescent Friendly Health Services: An Agenda for Change; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Teede, H.; Deeks, A.; Moran, L. Polycystic ovary syndrome: A complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010, 8, 41. [Google Scholar] [CrossRef]
- Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef]
- Lim, S.S.; Davies, M.J.; Norman, R.J.; Moran, L.J. Overweight, obesity and central obesity in women with polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. Update 2012, 18, 618–637. [Google Scholar] [CrossRef]
- Amisi, C.A. Markers of insulin resistance in Polycystic ovary syndrome women: An update. World J. Diabetes 2022, 13, 129–149. [Google Scholar] [CrossRef]
- Barberis, N.; Calaresi, D.; Cannavò, M.; Verrastro, V. Body mass index and quality of life in individuals with polycystic ovary syndrome: Dysmorphic concerns and eating disorders as mediators. Front. Public Health 2022, 10, 962083. [Google Scholar] [CrossRef]
- Quick, V.; Eisenberg, M.E.; Bucchianeri, M.M.; Neumark-Sztainer, D. Prospective Predictors of Body Dissatisfaction in Young Adults: 10-year Longitudinal Findings. Emerg. Adulthood 2013, 1, 271–282. [Google Scholar] [CrossRef] [PubMed]
- Thannickal, A.; Brutocao, C.; Alsawas, M.; Morrow, A.; Zaiem, F.; Murad, M.H.; Javed Chattha, A. Eating, sleeping and sexual function disorders in women with polycystic ovary syndrome (PCOS): A systematic review and meta-analysis. Clin. Endocrinol. 2020, 92, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Nasiri-Amiri, F.; Faramarzi, M.; Omidvar, S.; Alizadeh-Navaei, R. Depression and anxiety in adolescents and young women with polycystic ovary syndrome: A systematic review and meta-analysis. Int. J. Adolesc. Med. Health 2023, 35, 233–242. [Google Scholar] [CrossRef]
- Amato, M.C.; Giordano, C.; Galia, M.; Criscimanna, A.; Vitabile, S.; Midiri, M.; Galluzzo, A.; AlkaMeSy Study Group. Visceral Adiposity Index: A reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care 2010, 33, 920–922. [Google Scholar] [CrossRef]
- Probst, M.; Vandereycken, W.; Van Coppenolle, H.; Vanderlinden, J. The Body Attitude Test for patients with an eating disorder: Psycometric characteristics of a new questionnaire. Eat. Disord. 1995, 3, 133–144. [Google Scholar] [CrossRef]
- Henderson, M.; Freeman, C.P. A self-rating scale for bulimia. The ‘BITE’. Br. J. Psychiatry 1987, 150, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The eating attitudes test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Richter, P.; Werner, J.; Heerlein, A.; Kraus, A.; Sauer, H. On the validity of the Beck Depression Inventory. A review. Psychopathology 1998, 31, 160–168. [Google Scholar] [CrossRef]
- Cohen, S.; Karmarck, T.; Mermerlstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Preacher, K.J.; Kelley, K. Effect size measures for mediation models: Quantitative strategies for communicating indirect effects. Psychol. Methods 2011, 16, 93–115. [Google Scholar] [CrossRef] [PubMed]
- Salvia, M.G.; Ritholz, M.D.; Craigen, K.L.E.; Quatromoni, P.A. Managing type 2 diabetes or prediabetes and binge eating disorder: A qualitative study of patients’ perceptions and lived experiences. J. Eat. Disord. 2022, 10, 148. [Google Scholar] [CrossRef] [PubMed]
- Cooney, L.G.; Milman, L.W.; Hantsoo, L.; Kornfield, S.; Sammel, M.D.; Allison, K.C.; Epperson, C.N.; Dokras, A. Cognitive-behavioral therapy improves weight loss and quality of life in women with polycystic ovary syndrome: A pilot randomized clinical trial. Fertil. Steril. 2018, 110, 161–171.e1. [Google Scholar] [CrossRef]
- Çoban, Ö.G.; Tulacı, Ö.D.; Adanır, A.S.; Önder, A. Psychiatric Disorders, Self-Esteem, and Quality of Life in Adolescents with Polycystic Ovary Syndrome. J. Pediatr. Adolesc. Gynecol. 2019, 32, 600–604. [Google Scholar] [CrossRef]
- Ibáñez, L.; de Zegher, F. Adolescent PCOS: A postpubertal central obesity syndrome. Trends Mol. Med. 2023, 29, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Barry, J.A.; Kuczmierczyk, A.R.; Hardiman, P.J. Anxiety and depression in polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. 2011, 26, 2442–2451. [Google Scholar] [CrossRef] [PubMed]
- Farrell, K.; Antoni, M.H. Insulin resistance, obesity, inflammation, and depression in polycystic ovary syndrome: Biobehavioral mechanisms and interventions. Fertil. Steril. 2010, 94, 1565–1574. [Google Scholar] [CrossRef]
- Pariante, C.M.; Miller, A.H. Glucocorticoid receptors in major depression: Relevance to pathophysiology and treatment. Biol. Psychiatry 2001, 49, 391–404. [Google Scholar] [CrossRef] [PubMed]
- Dunn, A.J.; Swiergiel, A.H.; de Beaurepaire, R. Cytokines as mediators of depression: What can we learn from animal studies? Neurosci. Biobehav. Rev. 2005, 29, 891–909. [Google Scholar] [CrossRef] [PubMed]
- Alur-Gupta, S.; Chemerinski, A.; Liu, C.; Lipson, J.; Allison, K.; Sammel, M.D.; Dokras, A. Body-image distress is increased in women with polycystic ovary syndrome and mediates depression and anxiety. Fertil. Steril. 2019, 112, 930–938. [Google Scholar] [CrossRef] [PubMed]
- Cronin, L.; Guyatt, G.; Griffith, L.; Wong, E.; Azziz, R.; Futterweit, W.; Cook, D.; Dunaif, A. Development of a health-related quality-of-life questionnaire (PCOSQ) for women with polycystic ovary syndrome (PCOS). J. Clin. Endocrinol. Metab. 1998, 83, 1976–1987. [Google Scholar] [CrossRef] [PubMed]
- Jarrar, Y.; Awobamise, A.O.; Nweke, G.E. The Mediating Effect of Social Anxiety on the Relationship Between Social Media Use and Body Dissatisfaction Among University Students. Front. Commun. 2022, 7, 900257. [Google Scholar] [CrossRef]
- Izydorczyk, B.; Sitnik-Warchulska, K. Sociocultural Appearance Standards and Risk Factors for Eating Disorders in Adolescents and Women of Various Ages. Front. Psychol. 2018, 9, 429. [Google Scholar] [CrossRef]
- Verri, A.; Nappi, R.E.; Cecchini, A.P.; Vallero, E.; Luzi, S.; Zara, C. Eating disorders and Axis I psychiatric comorbidity in amenorrheic women. Int. J. Eat. Disord. 1998, 24, 137–146. [Google Scholar] [CrossRef]
- Krug, I.; Giles, S.; Paganini, C. Binge eating in patients with polycystic ovary syndrome: Prevalence, causes, and management strategies. Neuropsychiatr. Dis. Treat. 2019, 15, 1273–1285. [Google Scholar] [CrossRef] [PubMed]
- Naessén, S.; Carlström, K.; Garoff, L.; Glant, R.; Hirschberg, A.L. Polycystic ovary syndrome in bulimic women--an evaluation based on the new diagnostic criteria. Gynecol. Endocrinol. 2006, 22, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Douglas, K.M.; Fenton, A.J.; Eggleston, K.; Porter, R.J. Rate of polycystic ovary syndrome in mental health disorders: A systematic review. Arch. Women’s Ment. Health 2022, 25, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Sundblad, C.; Landén, M.; Eriksson, T.; Bergman, L.; Eriksson, E. Effects of the androgen antagonist flutamide and the serotonin reuptake inhibitor citalopram in bulimia nervosa: A placebo-controlled pilot study. J. Clin. Psychopharmacol. 2005, 25, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Genazzani, A.R.; Gastaldi, M.; Bidzinska, B.; Mercuri, N.; Genazzani, A.D.; Nappi, R.E.; Segre, A.; Petraglia, F. The brain as a target organ of gonadal steroids. Psychoneuroendocrinology 1992, 17, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Unluhizarci, K.; Karaca, Z.; Kelestimur, F. Role of insulin and insulin resistance in androgen excess disorders. World J. Diabetes 2021, 12, 616–629. [Google Scholar] [CrossRef] [PubMed]
- Ozgen Saydam, B.; Yildiz, B.O. Polycystic Ovary Syndrome and Brain: An Update on Structural and Functional Studies. J. Clin. Endocrinol. Metab. 2021, 106, e430–e441. [Google Scholar] [CrossRef] [PubMed]
- De Giuseppe, R.; Braschi, V.; Bosoni, D.; Biino, G.; Stanford, F.C.; Nappi, R.E.; Cena, H. Dietary underreporting in women affected by polycystic ovary syndrome: A pilot study. Nutr. Diet. 2019, 76, 560–566. [Google Scholar] [CrossRef]
- Bartholome, L.T.; Peterson, R.E.; Raatz, S.K.; Raymond, N.C. A comparison of the accuracy of self-reported intake with measured intake of a laboratory overeating episode in overweight and obese women with and without binge eating disorder. Eur. J. Nutr. 2013, 52, 193–202. [Google Scholar] [CrossRef]
- Jones, L.; Ness, A.; Emmett, P. Misreporting of Energy Intake from Food Records Completed by Adolescents: Associations with Sex, Body Image, Nutrient, and Food Group Intake. Front. Nutr. 2021, 8, 749007. [Google Scholar] [CrossRef]
- Cowan, S.; Lim, S.; Alycia, C.; Pirotta, S.; Thomson, R.; Gibson-Helm, M.; Blackmore, R.; Naderpoor, N.; Bennett, C.; Ee, C.; et al. Lifestyle management in polycystic ovary syndrome–beyond diet and physical activity. BMC Endocr. Disord. 2023, 23, 14. [Google Scholar] [CrossRef]
- Lee, I.; Cooney, L.G.; Saini, S.; Sammel, M.D.; Allison, K.C.; Dokras, A. Increased odds of disordered eating in polycystic ovary syndrome: A systematic review and meta-analysis. Eat. Weight Disord. 2019, 24, 787–797. [Google Scholar] [CrossRef]
- Steegers-Theunissen, R.P.M.; Wiegel, R.E.; Jansen, P.W.; Laven, J.S.E.; Sinclair, K.D. Polycystic Ovary Syndrome: A Brain Disorder Characterized by Eating Problems Originating during Puberty and Adolescence. Int. J. Mol. Sci. 2020, 21, 8211. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PCOS Adolescents (n = 128) | ||
|---|---|---|
| Mean ± SD | Median (IQR) | |
| Demographic characterstics | ||
| Age (years) | 17.2 ± 1.6 | 17 (16–19) |
| Age at menarche (years) | 11.9 ± 1.3 | 12 (11–13) |
| Gynecological age (years) | 5.2 ± 1.8 | 5 (4–7) |
| Education (years) | 11.2 ± 1.6 | 11 (10–13) |
| Clinical characteristics | ||
| Birth weight (g) | 3112.7 ± 589.9 | 3120 (2790–3465) |
| Weight (kg) | 66.4 ± 16.9 | 62 (55.1–70.4) |
| Body mass index (kg/m2) | 24.8 ± 6.2 | 23.1 (20.4–27.6) |
| Waist circumference (cm) | 79.7 ± 14.1 | 77 (70–85) |
| Waist/hip ratio | 0.8 ± 0.07 | 0.8 (0.75–0.84) |
| Systolic blood pressure (mmHg) | 111.7 ± 14.6 | 110 (105–120) |
| Diastolic blood pressure (mmHg) | 70.7 ± 8.3 | 70 (65–75) |
| Metabolic profile | ||
| Fasting glycemia (mg/dL) | 81.2 ± 8.1 | 70 (65–70) |
| Fasting insulin (mIU/mL) | 11.5 ± 9.3 | 9.2 (6.2–14.8) |
| HOMA index | 2.4 ± 2.06 | 1.8 (1.3–3.01) |
| Visceral adiposity index | 2.6 ± 1.7 | 2.2 (1.4–3.2) |
| Total cholesterol (mg/dL) | 152.4 ± 30.9 | 149 (133–174) |
| High-density lipoprotein cholesterol (mg/dL) | 52 ± 12.7 | 51 (43–58) |
| Low-density lipoprotein cholesterol (mg/dL) | 77.8 ± 35.2 | 80.4 (62.3–101.2) |
| Triglycerides (mg/dL) | 69.7 ± 36.9 | 58 (44–89) |
| Aspartate transaminase (mU/mL) | 19.7 ± 9.9 | 18 (15–20) |
| Alanine transaminase (mU/mL) | 20.5 ± 19.7 | 15 (13–19.8) |
| Hormonal profile | ||
| Luteinizing hormone (LH) (IU/L) | 8.9 ± 5.6 | 7.3 (5.2–11.2) |
| Follicle-stimulating hormone (FSH) (IU/L) | 5.3 ± 1.8 | 5.2 (4.1–6.1) |
| LH/FSH ratio | 1.7 ± 0.9 | 1.5 (1–2.2) |
| 17β-estradiol (pg/mL) | 61.1 ± 51.2 | 46.5 (33.9–63.5) |
| Androstenedione (ng/mL) | 4.1 ± 2 | 3.7 (2.7–4.8) |
| Total Testosterone (ng/mL) | 0.7 ± 0.4 | 0.7 (0.4–1) |
| DHEAS (ng/mL) | 3.3 ± 2.8 | 2.7 (2–3.6) |
| PCOS Adolescents (n = 128) | ||
|---|---|---|
| Median of Total Score (IQR) | Percentage of Patients with a Pathological Score (%) | |
| Body attitude (BAT) | 35 (26–48) | 49.2% (n = 63/128) |
| State anxiety (STAI-I) | 43 (36–51.8) | 57% (n = 73/128) |
| Trait anxiety (STAI-2) | 44.5 (36.2–53) | 63.1% (n = 81/128) |
| Depression (BDI) | 8 (3.2–12) | 39.1% (n = 50/128) |
| Bulimia (BITE) | 9 (6–14) | 41.4% (n = 53/128) |
| Eating disorder (EAT) | 7 (3–13) | 11.7% (n = 15/128) |
| Perceived stress (PSS) | 21 (18–25) | 68.2% (n = 60/88) |
| Body Mass Index (BMI) | p-Value | Insulin Resistance (IR) | p-Value | BMI & IR | p-Value | |
|---|---|---|---|---|---|---|
| Median of Total Score (IQR) | Median of Total Score (IQR) | Median of Total Score(IQR) | ||||
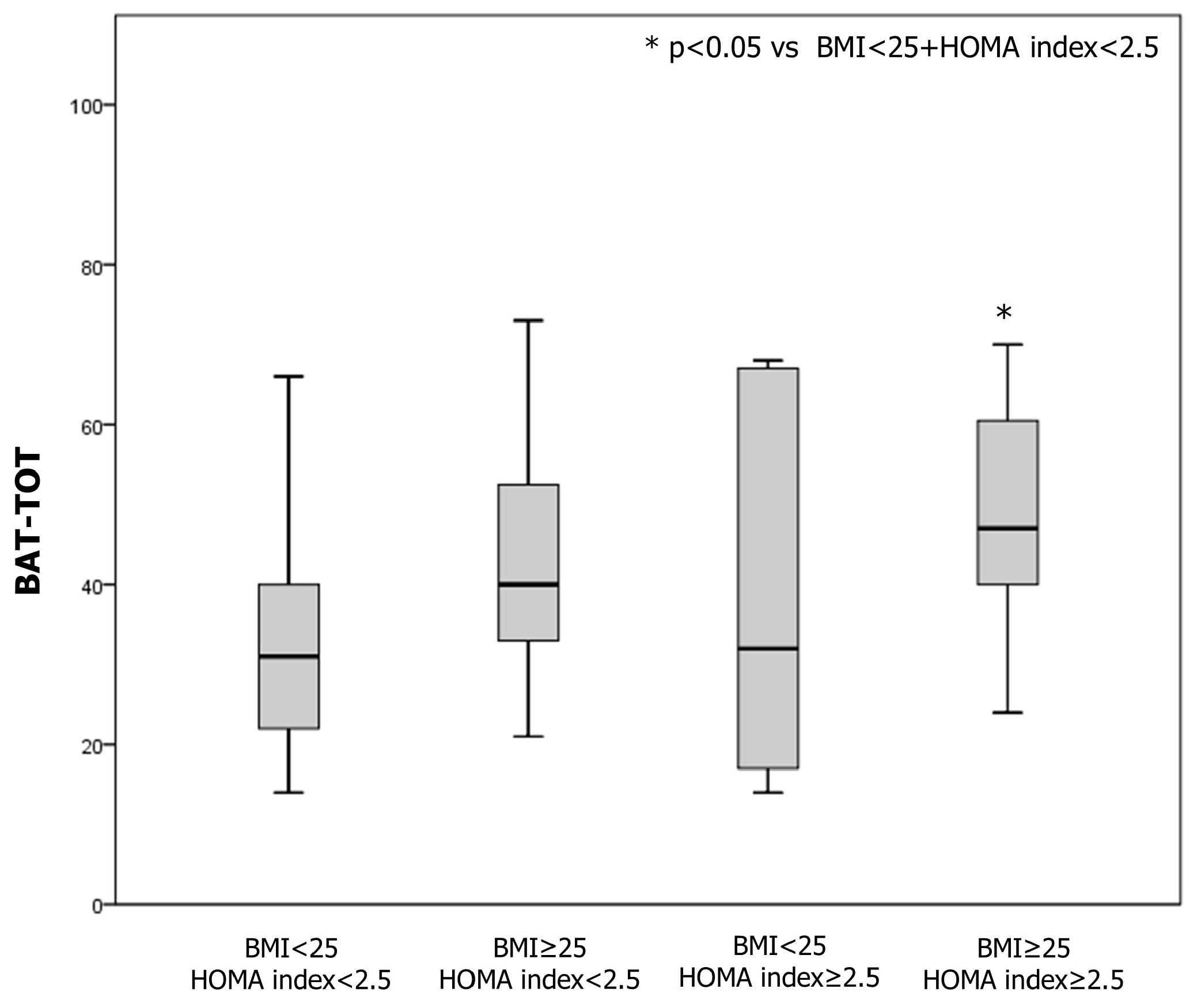
| Body attitude (BAT) | <18.5 (n = 9) 20 (17.5–29) 18.5–24.9 (n = 76) 32 (23.25–46.2) 25–29.9 (n = 19) 38 (32–44) >30 (n = 24) 52.5 (40.2–64.7) | <0.001 | IR (n = 30) 47 (32.5–58) NO IR (n = 98) 32 (24–40) | 0.003 | BMI < 25 + HOMA < 2.5 (n = 73) 20 (17.5–29) BMI ≥ 25 + HOMA < 2.5 (n = 27) 32 (23.25–46.25) BMI < 25 + HOMA ≥ 2.5 (n = 5) 38 (32–44) BMI ≥ 25 + HOMA ≥ 2.5 (n = 23) 52.50 (40.25–64.75) | p < 0.001 |
| State anxiety (STAI-I) | <18.5 (n = 9) 42 (30.5–52) 18.5–24.9 (n = 76) 42.5 (36.25–50) 25–29.9 (n = 19) 38 (35–50) >30 (n = 24) 47.5 (36.5–57) | 0.61 | IR (n = 30) 44 (36–55.5) NO IR (n = 98) 42 (36–50) | 0.032 | BMI < 25 + HOMA < 2.5 (n = 73) 42 (30.5–52) BMI ≥ 25 + HOMA < 2.5 (n = 27) 42.5 (36.25–50) BMI < 25 + HOMA ≥ 2.5 (n = 5) 38 (35–50) BMI ≥ 25 + HOMA ≥ 2.5 (n = 23) 47.5 0 (36.50–57.50) | 0.085 |
| Trait anxiety (STAI-2) | <18.5 (n = 9) 45 (37–52) 18.5–24.9 (n = 76) 44.5 (37–51.75) 25–29.9 (n = 19) 41 (34–50) >30 (n = 24) 49.5 (36–55.7) | 0.65 | IR (n = 30) 45 (36–53) NO IR (n = 98) 44 (37–53) | 0.10 | BMI < 25 + HOMA < 2.5 (n = 73) 45 (37–52) BMI ≥ 25 + HOMA < 2.5 (n = 27) 44.50 (37–51.75) BMI < 25 + HOMA ≥ 2.5 (n = 5) 41 (34–50) BMI ≥ 25 + HOMA ≥ 2.5 (n = 23) 49.5 (36–55.75) | 0.458 |
| Depression (BDI) | <18.5 (n = 9) 9 (5–18) 18.5–24.9 (n = 76) 7.5 (4–11.75) 25–29.9 (n = 19) 8 (4–12) >30 (n = 24) 8 (2–14.75) | 0.80 | IR (n = 30) 8 (4–12.5) NO IR (n = 98) 7 (3–12) | 0.21 | BMI < 25 + HOMA < 2.5 (n = 73) 9 (5–18) BMI ≥ 25+HOMA < 2.5 (n = 27) 7.5 (4–11.75) BMI < 25 + HOMA ≥ 2.5 (n = 5) 8 (4–12) BMI ≥ 25 + HOMA≥2.5 (n = 23) 8 (2–14.75) | 0.544 |
| Bulimia (BITE) | <18.5 (n = 9) 7 (6–12.5) 18.5–24.9 (n = 76) 8 (5–14) 25–29.9 (n = 19) 9 (6–12) >30 (n = 24) 11 (6–14.75) | 0.74 | IR (n = 30) 9 (6–14) NO IR (n = 98) 8.5 (5.7–13.25) | 0.83 | BMI < 25 + HOMA < 2.5 (n = 73) 7 (6–12-5) BMI ≥ 25 + HOMA < 2.5 (n = 27) 8 (5–14) BMI < 25 + HOMA ≥ 2.5 (n = 5) 9 (6–12) BMI ≥ 25 + HOMA ≥ 2.5 (n = 23) 11 (6–14.75) | 0.815 |
| Eating disorder (EAT) | <18.5 (n = 9) 4 (3–9.5) 18.5–24.9 (n = 76) 6.5 (3–13.5) 25–29.9 (n = 19) 6.5 (3.7–12) >30 (n = 24) 10 (5.7–16.5) | 0.20 | IR (n = 30) 7 (4–13.5) NO IR (n = 98) 7 (3–13) | 0.70 | BMI < 25 + HOMA < 2.5 (n = 73) 4 (3–9.5) BMI ≥ 25 + HOMA < 2.5 (n = 27) 6.5 (3–13.5) BMI < 25 + HOMA ≥ 2.5 (n = 5) 6.5 (3.75–12) BMI ≥ 25 + HOMA ≥ 2.5 (n = 23) 10 (5.75–16.5) | 0.841 |
| Perceived stress (PSS) | <18.5 (n = 9) 20 (18–23) 18.5–24.9 (n = 76) 22 (16–25.25) 25–29.9 (n = 19) 21 (14.2–27) >30 (n = 24) 21 (19–25) | 0.72 | IR (n = 30) 21 (18–25) NO IR (n = 98) 21 (17–25) | 0.035 | BMI < 25 + HOMA < 2.5 (n = 73) 20 (18–23) BMI ≥ 25 + HOMA < 2.5 (n = 27) 22 (16–25.25) BMI < 25 + HOMA ≥ 2.5 (n = 5) 21 (14.25–27) BMI ≥ 25 + HOMA ≥ 2.5 (n = 23) 21 (19–25) | 0.329 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbagallo, F.; Tiranini, L.; Placentino, C.; Mariacci, G.; Piccinino, M.; Cucinella, L.; Calogero, A.E.; Nappi, R.E. Body Image and Other Mood Vulnerabilities in Adolescents with Polycystic Ovary Syndrome and Metabolic Alterations. Children 2024, 11, 521. https://0-doi-org.brum.beds.ac.uk/10.3390/children11050521
Barbagallo F, Tiranini L, Placentino C, Mariacci G, Piccinino M, Cucinella L, Calogero AE, Nappi RE. Body Image and Other Mood Vulnerabilities in Adolescents with Polycystic Ovary Syndrome and Metabolic Alterations. Children. 2024; 11(5):521. https://0-doi-org.brum.beds.ac.uk/10.3390/children11050521
Chicago/Turabian StyleBarbagallo, Federica, Lara Tiranini, Chiara Placentino, Giacomo Mariacci, Manuela Piccinino, Laura Cucinella, Aldo E. Calogero, and Rossella E. Nappi. 2024. "Body Image and Other Mood Vulnerabilities in Adolescents with Polycystic Ovary Syndrome and Metabolic Alterations" Children 11, no. 5: 521. https://0-doi-org.brum.beds.ac.uk/10.3390/children11050521