The Developmental Pathways of Preschool Children with Acute Lymphoblastic Leukemia: Communicative and Social Sequelae One Year after Treatment

 ,
,
Abstract
:1. Introduction
1.1. Cognitive Sequelae Related to the Illness and Its Treatment
1.2. Motor Performance Delays
1.3. Social Impairments and Academic Difficulties
1.4. Aims
- Are there differences between the clinical and control groups in their developmental task performance?
- Are there differences in developmental tasks throughout the different age groups (between ages three and five years)?
- In which domains do children show more difficulties (communication abilities, daily living skills, socialization competence, motor performance) when compared with Italian norms?
- In which VABS’ cluster domains and items did children show more difficulties?
- Are disease and treatment variables associated with children’s developmental delays?
2. Materials and Methods
2.1. Procedure
2.2. Participants
2.3. Instruments
2.4. Statistical Methods
3. Results
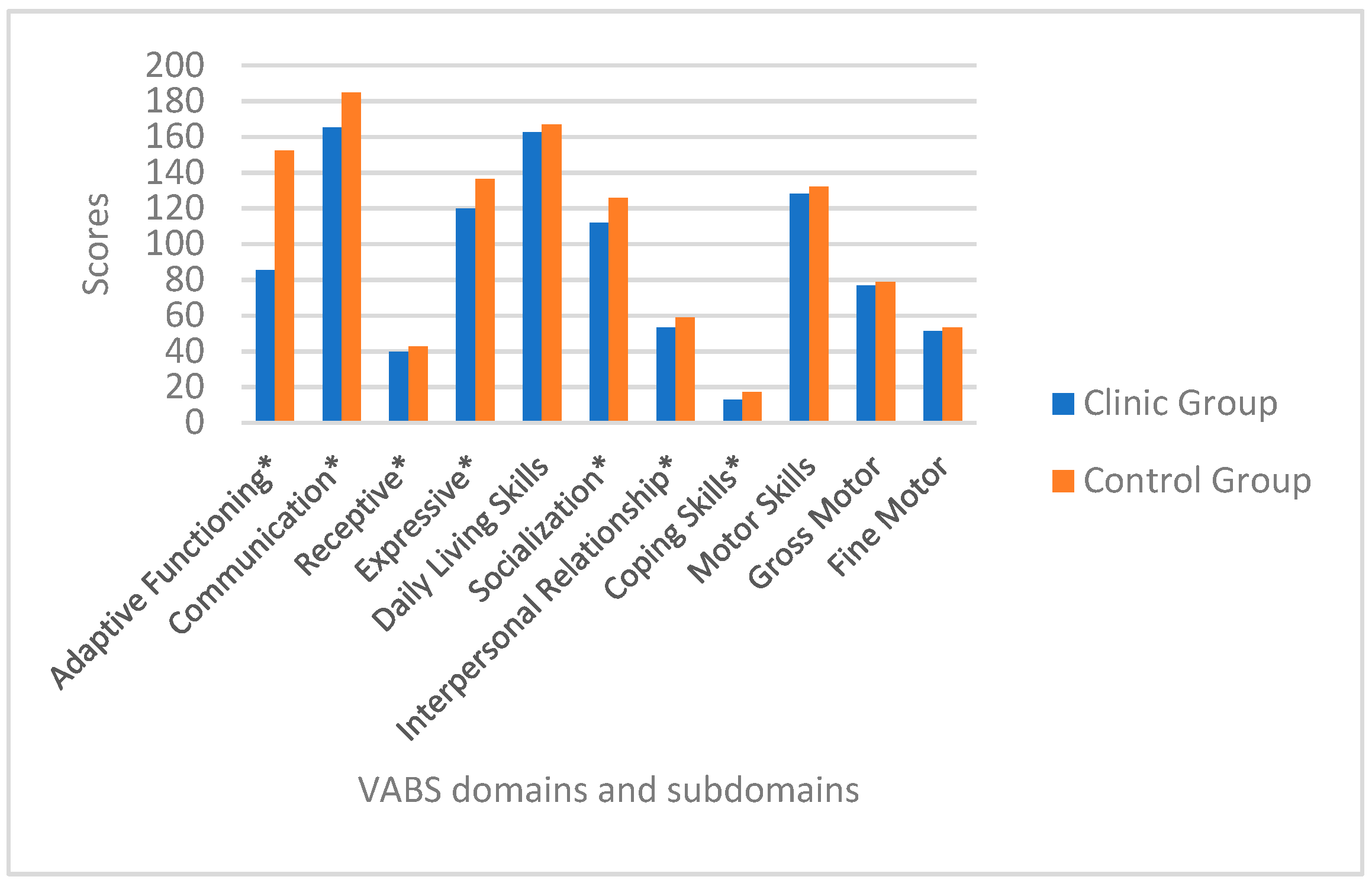
3.1. Developmental Domains in Children with Leukaemia Compared with Healthy Peers
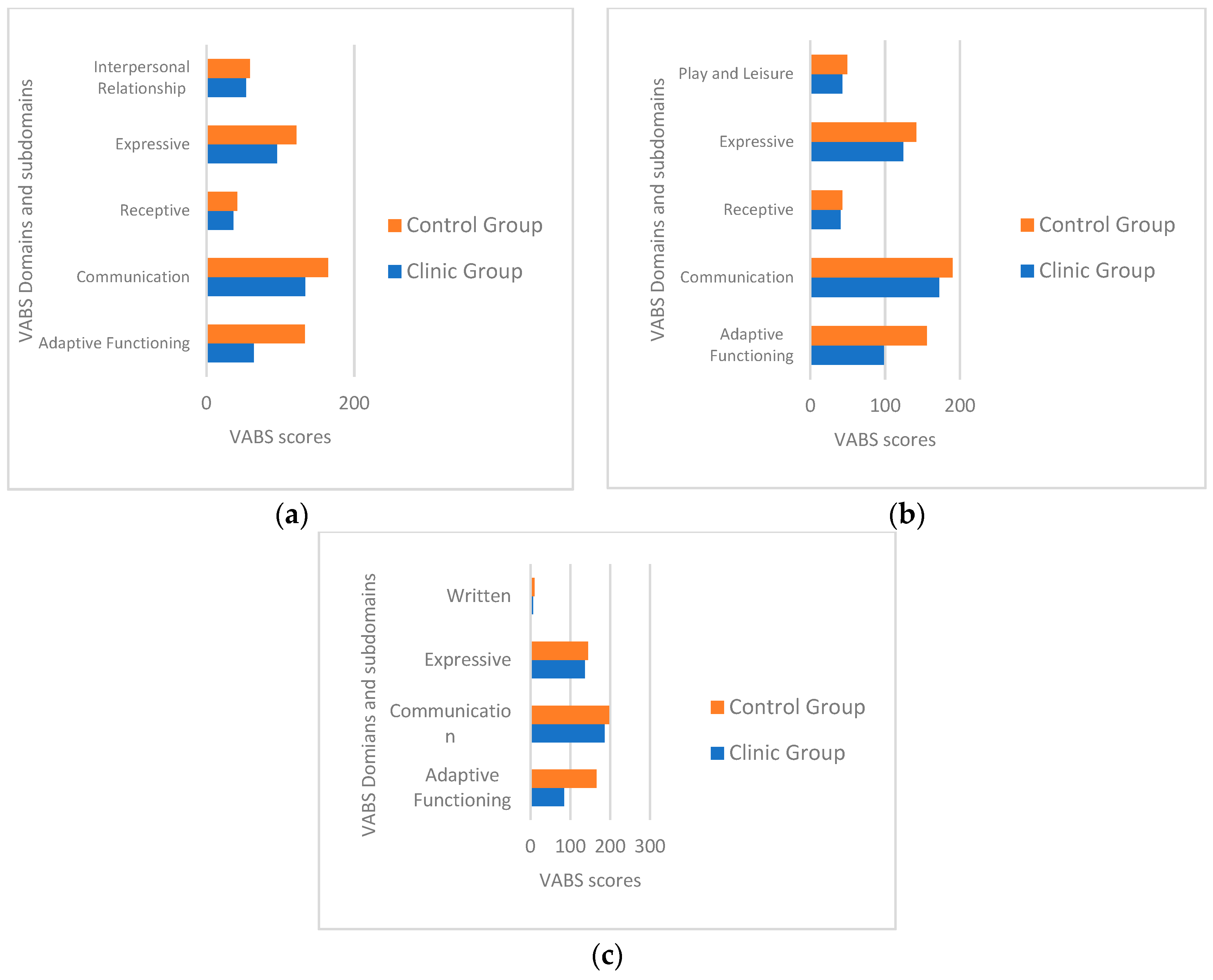
3.2. Differences in Developmental Skill Performance in Age Groups (30–48 Months, 49–60 Months, 61–71 Months)
3.3. In Which Cluster Belonging to Communication and to Socialization Domains Did Children Show More Difficulties?
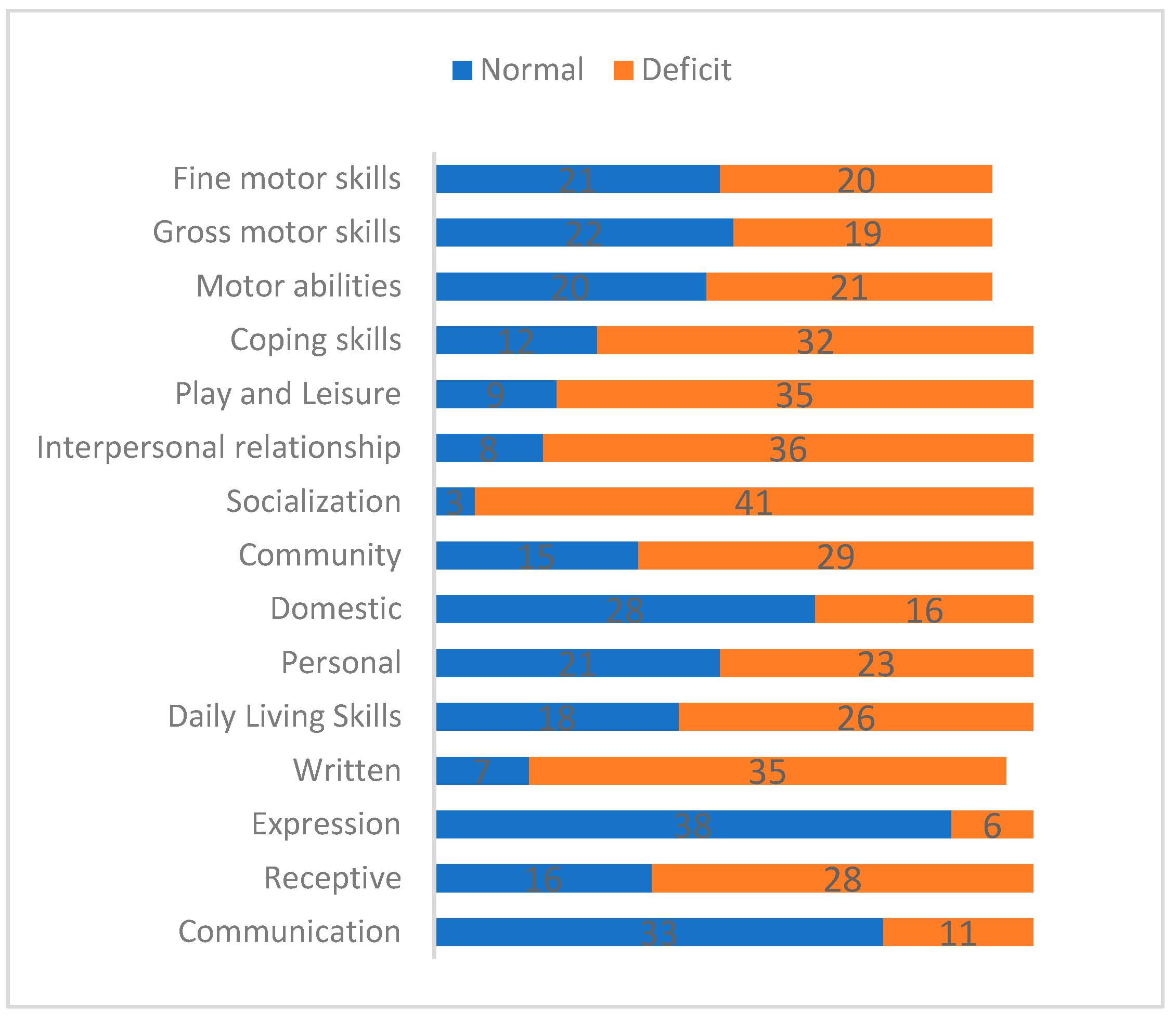
3.4. Pre-School Patients’ Delays Compared with Norms
3.5. Disease and Treatment Variables Associated with Children’s Adaptive Functioning
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shah, A.J.; Epport, K.; Azen, C.; Killen, R.; Wilson, K.; De Clerck, D.; Crooks, G.; Kapoor, N.; Kohn, D.B.; Parkman, R.; et al. Progressive Declines in Neurocognitive Function Among Survivors of Hematopoietic Stem Cell Transplantation for Pediatric Hematologic Malignancies. J. Pediatr. Hematol. 2008, 30, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Lewis, F.M.; Perry, M.L.; Murdoch, B.E. Longitudinal language outcomes following intrathecal chemotherapy for acute lymphoblastic leukaemia. Int. J. Speech Lang Pathol. April. 2013, 152, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Scheede-Bergdahl, C.; Jagoe, R.T. After the chemotherapy: Potential mechanisms for chemotherapy-induced delayed skeletal muscle dysfunction in survivors of acute lymphoblastic leukaemia in childhood. Front. Pharmacol. 2013, 4, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Götte, M.; Kesting, S.V.; Winter, C.C.; Rosenbaum, D.; Boos, J. Motor performance in children and adolescents with cancer at the end of acute treatment phase. Eur. J. Pediatr. 2015, 174, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Tremolada, M.; Taverna, L.; Bonichini, S.; Basso, G.; Pillon, M. Self-Esteem and Academic Difficulties in Preadolescents and Adolescents Healed from Paediatric Leukaemia. Cancers 2017, 9, 55. [Google Scholar] [CrossRef]
- Tremolada, M.; Bonichini, S.; Taverna, L.; Basso, G.; Pillon, M. Health-related quality of life in AYA cancer survivors who underwent HSCT compared with healthy peers. Eur. J. Cancer Care 2018, 27, e12878. [Google Scholar] [CrossRef] [Green Version]
- Moyer, K.H.; Willard, V.W.; Gross, A.M.; Netson, K.L.; Ashford, J.M.; Kahalley, L.S.; Wu, S.; Xiong, X.; Conklin, H.M. The Impact of Attention on Social Functioning in Survivors of Pediatric Acute Lymphoblastic Leukemia and Brain Tumors. Pediatr. Blood Cancer 2012, 59, 1290–1295. [Google Scholar] [CrossRef]
- Armstrong, G.T.; Oeffinger, K.C.; Chen, Y.; Kawashima, T.; Yasui, Y.; Leisenring, W.; Stovall, M.; Chow, E.J.; Sklar, C.A.; Mulrooney, D.A.; et al. Modifiable Risk Factors and Major Cardiac Events Among Adult Survivors of Childhood Cancer. J. Clin. Oncol. 2013, 31, 3673–3680. [Google Scholar] [CrossRef]
- Jansen, N.C. Feasibility of neuropsychological assessment in leukaemia patients shortly after diagnosis: Directions for future prospective research. Arch. Dis. Child. 2005, 90, 301–304. [Google Scholar] [CrossRef]
- Lofstad, G.E.; Reinfjell, T.; Hestad, K.; Diseth, T.H. Cognitive outcome in children and adolescents treated for acute lymphoblastic leukaemia with chemotherapy only. Acta Paediatr. 2009, 98, 180–186. [Google Scholar] [CrossRef]
- van der Plas, E.; Schachar, R.J.; Hitzler, J.; Crosbie, J.; Guger, S.L.; Spiegler, B.J.; Ito, S.; Nieman, B.J. Brain structure, working memory and response inhibition in childhood leukemia survivors. Brain Behav. 2017, 7, e00621. [Google Scholar] [CrossRef] [PubMed]
- Reddick, W.E.; Laningham, F.H.; Glass, J.O.; Pui, C.H. Quantitative morphologic evaluation of magnetic resonance imaging during and after treatment of childhood leukemia. Neuroradiology 2007, 49, 889–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, F.M.; Perry, M.L.; Murdoch, B.E. An investigation of general and high-level language skills in children treated with central nervous system-targeted chemotherapy for acute lymphoblastic leukemia. J. Speech Lang. Pathol. 2011, 19, 27–36. [Google Scholar]
- Bornstein, M.H.; Scrimin, S.; Putnick, D.L.; Capello, F.; Haynes, O.M.; de Falco, S. Neurodevelopmental Functioning in Very Young Children Undergoing Treatment for Non-CNS Cancers. J. Pediatr. Psychol. 2012, 37, 660–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddick, W.E.; Taghipour, D.J.; Glass, J.O.; Ashford, J.; Xiong, X.; Wu, S.; Bonner, M.; Khan, R.B.; Conklin, H.M. Prognostic factors that increase the risk for reduced white matter volumes and deficits in attention and learning for survivors of childhood cancers: Reduced WMV in Childhood Cancer Survivors. Pediatr. Blood Cancer 2014, 61, 1074–1079. [Google Scholar] [CrossRef] [PubMed]
- Carey, M.E.; Hockenberry, M.J.; Moore, I.M.; Hutter, J.J.; Krull, K.R.; Pasvogel, A.; Kaemingk, K.L. Brief Report: Effect of Intravenous Methotrexate Dose and Infusion Rate on Neuropsychological Function One Year after Diagnosis of Acute Lymphoblastic Leukemia. J. Pediatr. Psychol. 2006, 32, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Buizer, A.I.; De Sonneville, L.M.; Veerman, A.J.; Heuvel-Eibrink, M.M.V.D.; Heuvel–Eibrink, M.M.V.D. Chemotherapy and attentional dysfunction in survivors of childhood acute lymphoblastic leukemia: Effect of treatment intensity. Pediatr. Blood Cancer 2005, 45, 281–290. [Google Scholar] [CrossRef]
- Andrews, G.S.; Saunders, F.; Barrera, M.; Atenafu, E. Factors Related to Changes in Cognitive, Educational and Visual Motor Integration in Children who Undergo Hematopoietic Stem Cell Transplant. J. Pediatr. Psychol. 2007, 33, 536–546. [Google Scholar] [Green Version]
- Eime, R.M.; A Young, J.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 98. [Google Scholar] [CrossRef]
- Söntgerath, R.; Eckert, K. Impairments of Lower Extremity Muscle Strength and Balance in Childhood Cancer Patients and Survivors: A Systematic Review. Pediatr. Hematol. Oncol. 2015, 32, 1–28. [Google Scholar] [CrossRef]
- Balsamo, L.M.; Sint, K.J.; Neglia, J.P.; Brouwers, P.; Kadan-Lottick, N.S. The Association Between Motor Skills and Academic Achievement Among Pediatric Survivors of Acute Lymphoblastic Leukemia. J. Pediatr. Psychol. 2016, 41, 319–328. [Google Scholar] [CrossRef]
- Jain, P.; Gulati, S.; Seth, R.; Bakhshi, S.; Toteja, G.S.; Pandey, R.M. Vincristine-induced Neuropathy in Childhood ALL (Acute Lymphoblastic Leukemia) Survivors: Prevalence and Electrophysiological Characteristics. J. Child Neurol. 2014, 29, 932–937. [Google Scholar] [CrossRef]
- Hartman, A.; van den Bos, C.; Stijnen, T.; Pieters, R. Decrease in motor performance in children with cancer is independent of the cumulative dose of vincristine: Motor Performance Independent of VCR. Cancer 2006, 106, 1395–1401. [Google Scholar] [CrossRef]
- Taverna, L.; Tremolada, M.; Bonichini, S.; Tosetto, B.; Basso, G.; Messina, C.; Pillon, M. Motor skill delays in pre-school children with leukemia one year after treatment: Hematopoietic stem cell transplantation therapy as an important risk factor. PLoS ONE 2017, 12, e0186787. [Google Scholar] [CrossRef]
- McLoone, J.K.; Wakefield, C.E.; Cohn, R.J. Childhood cancer survivors’ school (re)entry: Australian parents’ perceptions: School (re)entry after childhood cancer. Eur. J. Cancer Care 2013, 22, 484–492. [Google Scholar] [CrossRef]
- Reiter-Purtill, J.; Waller, J.; Noll, R.B. Empirical and Theoretical Perspectives on the Peer Relationships of Children with Chronic Conditions. In Handbook of Pediatric Psychology; Roberts, M.C., Steele, R., Eds.; Guilford Press: New York, NY, USA, 2009; pp. 672–688. [Google Scholar]
- Tremolada, M.; Bonichini, S.; Basso, G.; Pillon, M. Perceived social support and health-related quality of life in AYA cancer survivors and controls: Perceived social support and HRQoL in AYA cancer survivors. Psychooncology 2016, 25, 1408–1417. [Google Scholar] [CrossRef]
- Katz, L.F.; Leary, A.; Breiger, D.; Friedman, D. Pediatric Cancer and the Quality of Children’s Dyadic Peer Interactions. J. Pediatr. Psychol. 2011, 36, 237–247. [Google Scholar] [CrossRef]
- Balboni, G.; Pedrabissi, L. Adattamento Italiano Delle Vineland Adaptive Behavior Scales; Giunti Organizzazioni Speciali: Firenze, Italy, 2003. [Google Scholar]
- Msall, M.E. Developing preschool surveillance tools for adaptive functioning: Lessons for neuro-oncology. Eur. J. Paediatr. Neurol. 2010, 14, 368–379. [Google Scholar] [CrossRef]
- International Collaborative Treatment Protocol for Children and Adolescents with Acute Lymphoblastic Leukemia-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT01117441 (accessed on 4 May 2019).
- Taverna, L.; Tremolada, M.; Bonichini, S.; Basso, G.; Pillon, M. Adaptive Functioning of Preschooler Children with Leukemia Post 1 Year of Therapies Compared with Sane Peers. Br. J. Educ. Soc. Behav. Sci. 2016, 18, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Tremolada, M.; Bonichini, S.; Taverna, L.; Pillon, M.; Basso, G. I pazienti pediatrici curati per leucemia che ritornano a scuola: Analisi delle narrazioni su vita quotidiana e esperienza di malattia. Psicol. Clin. Dello. Sviluppo. 2018, 1, 69–92. [Google Scholar]
- Tremolada, M.; Bonichini, S.; Taverna, L.; Tumino, M.; Bisogno, G.; Putti, M.C.; Basso, G.; Pillon, M. Post-Traumatic Stress Symptoms in Parents of Children with Leukemias at Day +33: Identifying the Early Predictors. Pediatric Blood Cancer 2018, 65, 594. [Google Scholar] [CrossRef]
- Tremolada, M.; Bonichini, S.; Schiavo, S.; Pillon, M. Post-traumatic stress symptoms in mothers of children with leukaemia undergoing the first 12 months of therapy: Predictive models. Psychol. Health 2012, 27, 1448–1462. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Domain | Subdomain | Cluster | Items content |
|---|---|---|---|
| Communication | Receptive | Attention | How and how long the individual listens to someone, pays attention to activities or stories and understands given information. (E1–E5) |
| Expressive | Articulation | Quality and precision in speech articulation are evaluated. (M1–M4) | |
| Recitation | Ability to recite rhymes, songs, folk tales is assessed. (N1–N4) | ||
| Use of plurals and verbs times | Individual uses verb forms correctly in different tenses. (O1–O6) | ||
| Provide information about yourself | Ability to answer correctly to questions referred to address, telephone number or other personal information is measured. (P1–P7) | ||
| Socialization | Interpersonal Relationships | People identification | Individual knows names of family members and identifies them through features other than their name. (F1–F4) |
| First forms of social communication | Individual is able to participate in conversation. (G1–G3) | ||
| Friendships | Individual has friendships of the same of other sex. (H1–H5) | ||
| Play and Leisure | Games participation | Participation in different types of games (i.e., cards, hazard-based board) is assessed. (G1–G4) | |
| Go out with friends | Individual is able to meet friends outside home in the afternoon or evening. (H1–H4) | ||
| Coping skills | Respect for the rules | Individual respects rules in community and social situations. (A1–A4) | |
| Good education in conversation | Individual is able to have conversations with others showing good education. (C1–C3) | ||
| Responsible time management | Individual shows ability in managing time limits and making projects along time. (D1–D2) |
| Scales | Leukaemic Children | Healthy Peers | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Adaptive functioning composite | 85.53 | 51.53 | 152.34 | 20.16 |
| Communication | 165.34 | 184.77 | 184.77 | 20.58 |
| Receptive | 39.56 | 4.16 | 42.72 | 1.70 |
| Expressive | 119.90 | 26.75 | 136.50 | 16.56 |
| Socialization | 111.93 | 27.68 | 125.72 | 24.79 |
| Interpersonal Relationship | 53.40 | 10.72 | 58.75 | 6.87 |
| Coping Skills | 12.97 | 8.23 | 17.20 | 9.55 |
| Mother’s Schooling Years | |
|---|---|
| VABS composite | r = −0.046 |
| p = 0.77 | |
| VABS Communication | r = −0.030 |
| p = 0.84 | |
| VABS Socialization | r = 0.19 |
| p = 0.31 | |
| VABS Motor abilities | r = 0.027 |
| p = 0.86 |
| Patients | Healthy Peers | Statistical Analyses | |||||
|---|---|---|---|---|---|---|---|
| Sub-domain, Cluster | Item | M | SD | M | SD | Z | p |
| Receptive, Attention | E1 | 1.4 | 0.81 | 1.95 | 0.21 | −4.54 | 0.001 |
| E2 | 1.22 | 0.93 | 1.56 | 0.66 | −2.15 | 0.003 | |
| E3 | 0.9 | 0.91 | 1.68 | 0.51 | −6.20 | 0.0001 | |
| E4 | 0.79 | 0.87 | 1.63 | 0.68 | −5.85 | 0.0001 | |
| E5 | 0.15 | 0.52 | 0.04 | 0.3 | 1.22 | 0.23 ns | |
| Expressive, Articulation | M1 | 1.54 | 0.76 | 1.9 | 0.42 | −2.55 | 0.01 |
| M2 | 1.54 | 0.76 | 1.88 | 0.44 | −2.44 | 0.01 | |
| M3 | 1.38 | 0.86 | 1.9 | 0.42 | −3.1 | 0.002 | |
| M4 | 1.27 | 0.89 | 1.59 | 0.81 | −1.79 | 0.07 ns | |
| Expressive, Recitation | N1 | 1.68 | 0.73 | 1.86 | 0.51 | −1.41 | 0.15 ns |
| N2 | 1.56 | 0.81 | 1.88 | 0.44 | −2.32 | 0.02 | |
| N3 | 0.75 | 0.94 | 1.84 | 0.52 | −4.65 | 0.0001 | |
| N4 | 1.09 | 0.98 | 1.68 | 0.67 | −3.1 | 0.01 | |
| Expressive, Use of plurals and verbs times | O1 | 1.2 | 0.95 | 1.88 | 0.44 | −3.83 | 0.0001 |
| O2 | 1.15 | 0.96 | 1.81 | 0.58 | −3.48 | 0.0001 | |
| O3 | 0.97 | 0.97 | 1.75 | 0.57 | −4.10 | 0.0001 | |
| O4 | 0.86 | 0.97 | 1.72 | 0.69 | −4.30 | 0.0001 | |
| O5 | 0.27 | 0.62 | 1.06 | 0.79 | −4.44 | 0.0001 | |
| O6 | 0.36 | 0.71 | 1.45 | 0.79 | −4.87 | 0.0001 | |
| Expressive, Provide information about yourself | P1 | 1.45 | 0.9 | 1.9 | 0.42 | −3.16 | 0.002 |
| P2 | 1.45 | 0.9 | 1.81 | 0.54 | −2.81 | 0.005 | |
| P3 | 1.31 | 0.95 | 1.88 | 0.44 | −3.50 | 0.0001 | |
| P4 | 0.93 | 0.99 | 1.38 | 0.92 | −2.67 | 0.008 | |
| P5 | 0.43 | 0.81 | 0.7 | 0.87 | −1.34 | 0.18 ns | |
| P6 | 0.13 | 0.5 | 0.18 | 0.58 | −0.45 | 0.65 ns | |
| P7 | 0.36 | 0.78 | 1.22 | 0.86 | −4.08 | 0.0001 | |
| Interpersonal relationships, People identification | F1 | 1.68 | 0.73 | 2 | 0 | −2.64 | 0.008 |
| F2 | 1.63 | 0.78 | 2 | 0 | −2.82 | 0.005 | |
| F3 | 1.43 | 0.87 | 1.86 | 0.44 | −2.73 | 0.006 | |
| F4 | 1.31 | 0.93 | 1.88 | 0.44 | −3.50 | 0.0001 | |
| Interpersonal relationships, First forms of social communication | G1 | 1.22 | 0.93 | 1.65 | 0.71 | −3.04 | 0.002 |
| G2 | 1.27 | 0.97 | 1.61 | 0.78 | −2.10 | 0.035 | |
| G3 | 0.81 | 0.97 | 0.81 | 0.97 | 0.15 | 0.88 ns | |
| Interpersonal relationships, Friendships | H1 | 1.04 | 1.01 | 1.5 | 0.87 | −2.35 | 0.018 |
| H2 | 1 | 1.01 | 1.25 | 0.26 | −1.39 | 0.16 ns | |
| H3 | 0.72 | 0.97 | 1.45 | 0.9 | −3.41 | 0.001 | |
| H4 | 0.06 | 0.33 | 0.22 | 0.64 | −1.53 | 0.12 ns | |
| H5 | 0.59 | 0.92 | 0.86 | 1 | −1.50 | 0.13 ns | |
| Play and Leisure, Following play rules | G1 | 0.18 | 0.58 | 1.52 | 0.82 | −2.28 | 0.022 |
| G2 | 0.9 | 1 | 1.38 | 0.89 | −2.93 | 0.003 | |
| G3 | 0.75 | 0.96 | 1.04 | 0.96 | −2.03 | 0.042 | |
| G4 | 0.7 | 0.95 | 1.13 | 0.92 | −2.32 | 0.021 | |
| Play and Leisure, Games participation | H1 | 0.43 | 0.81 | 0.97 | 0.99 | −3.20 | 0.001 |
| H2 | 0.4 | 0.81 | 0.86 | 1 | −2.89 | 0.004 | |
| H3 | 0.18 | 0.58 | 0.43 | 0.81 | −1.96 | 0.05 | |
| H4 | 0.13 | 0.5 | 0.5 | 0.87 | −2.53 | 0.011 | |
| Play and Leisure, Go out with friends | I1 | 0 | 0 | 0.27 | 0.69 | −2.50 | 0.014 |
| I2 | 0 | 0 | 0.02 | 0.15 | −1 | 0.32 ns | |
| I3 | 0 | 0 | 0.18 | 0.58 | −2 | 0.046 | |
| Coping skills, Respect for the rules | A1 | 1.56 | 0.62 | 1.84 | 0.37 | −2.35 | 0.02 |
| A2 | 1.36 | 0.68 | 1.93 | 0.25 | −4.18 | 0.0001 | |
| A3 | 1.65 | 0.6 | 1.7 | 0.63 | −0.19 | 0.84 ns | |
| A4 | 1.43 | 0.78 | 1.93 | 0.25 | −3.38 | 0.001 | |
| Coping skills, Good education in conversation | C1 | 0.25 | 0.61 | 0.75 | 0.91 | −3.03 | 0.002 |
| C2 | 0.13 | 0.4 | 0.5 | 0.76 | −2.62 | 0.009 | |
| C3 | 0.51 | 0.52 | 0.5 | 0.87 | −2.15 | 0.03 | |
| Coping skills, Responsible time management | D1 | 0 | 0 | 0.41 | 0.81 | −3 | 0.003 |
| D2 | 0 | 0 | 0.25 | 0.65 | −2.33 | 0.02 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tremolada, M.; Taverna, L.; Bonichini, S.; Pillon, M.; Biffi, A. The Developmental Pathways of Preschool Children with Acute Lymphoblastic Leukemia: Communicative and Social Sequelae One Year after Treatment. Children 2019, 6, 92. https://0-doi-org.brum.beds.ac.uk/10.3390/children6080092
Tremolada M, Taverna L, Bonichini S, Pillon M, Biffi A. The Developmental Pathways of Preschool Children with Acute Lymphoblastic Leukemia: Communicative and Social Sequelae One Year after Treatment. Children. 2019; 6(8):92. https://0-doi-org.brum.beds.ac.uk/10.3390/children6080092
Chicago/Turabian StyleTremolada, Marta, Livia Taverna, Sabrina Bonichini, Marta Pillon, and Alessandra Biffi. 2019. "The Developmental Pathways of Preschool Children with Acute Lymphoblastic Leukemia: Communicative and Social Sequelae One Year after Treatment" Children 6, no. 8: 92. https://0-doi-org.brum.beds.ac.uk/10.3390/children6080092