The Measurement of Asthma and Allergic Rhinitis Control in Children and Adolescents

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Functional Assessment
2.3. Asthma Control Level
2.4. Asthma Control Test
2.5. Visual Analog Scale (VAS)
2.6. CARAT Questionnaires
2.7. Statistical Analysis
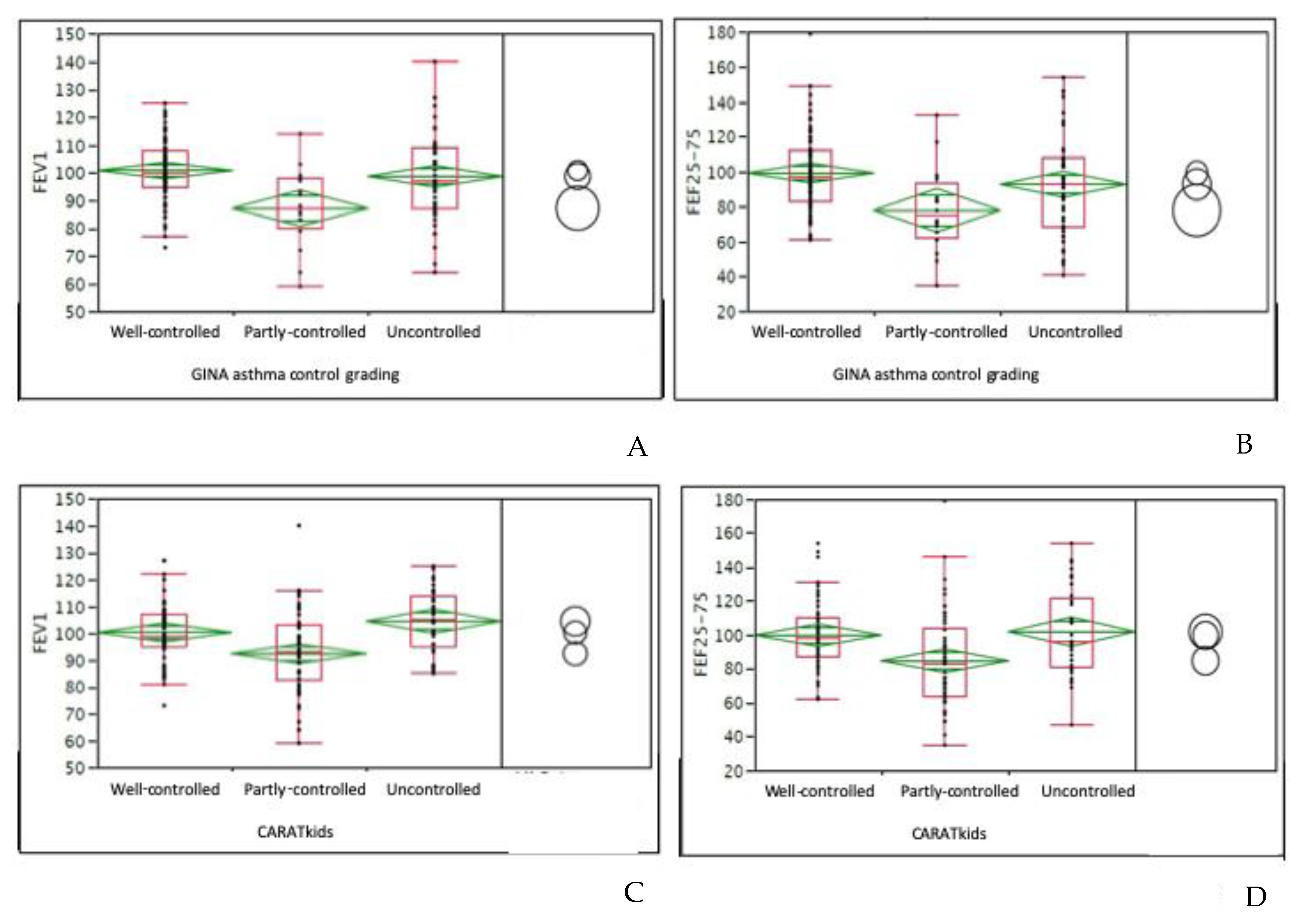
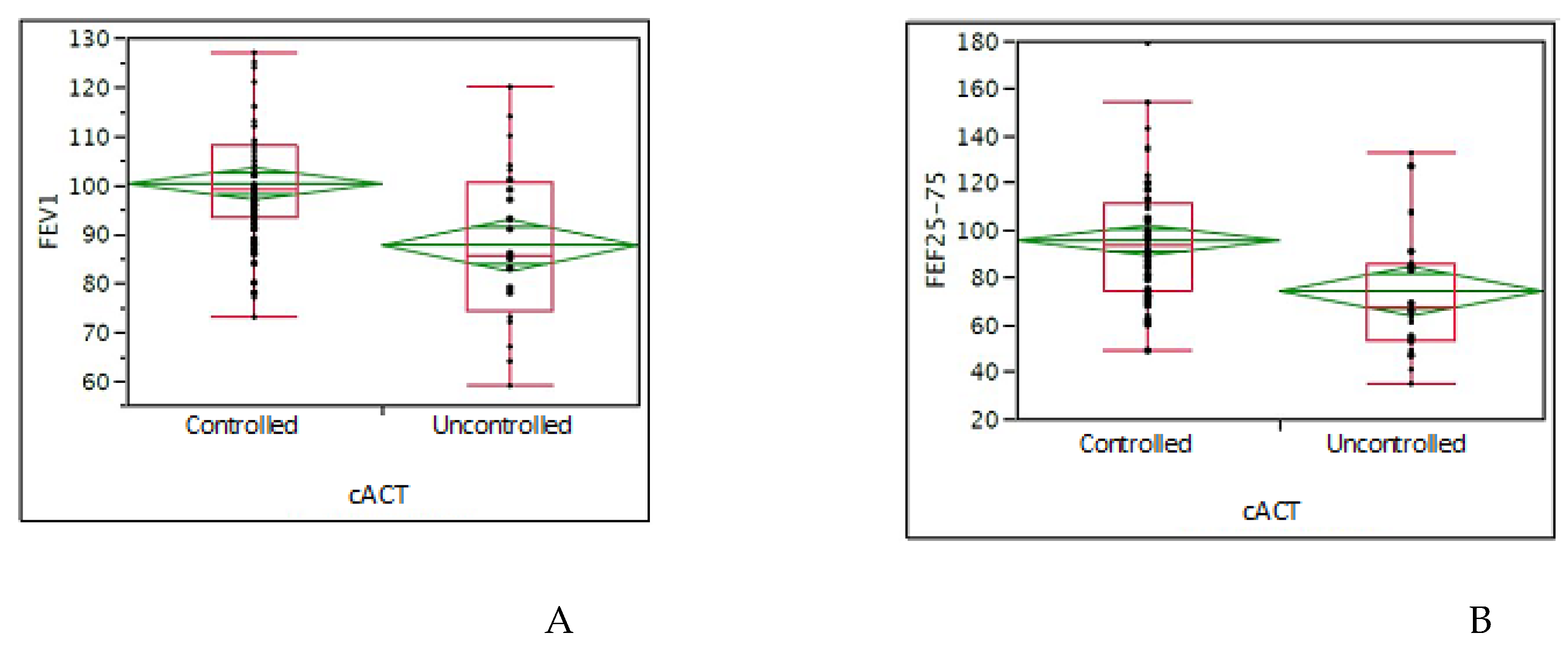
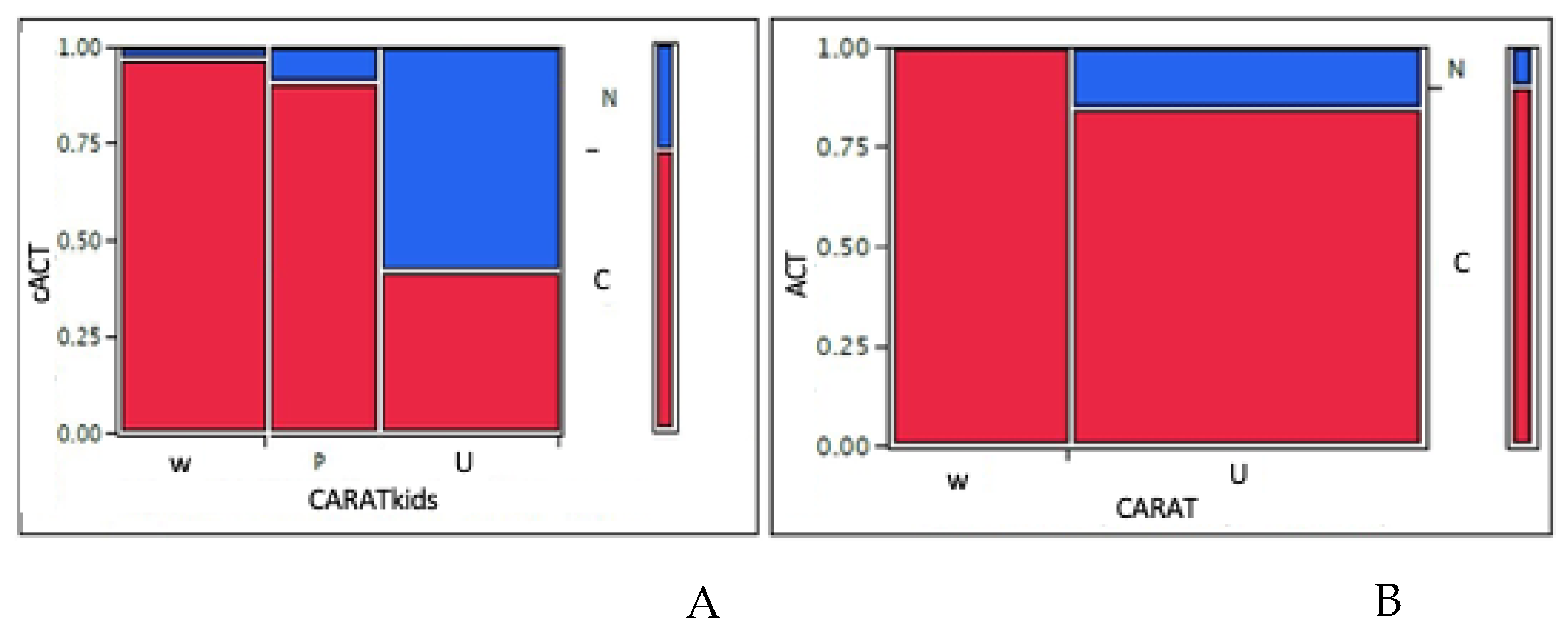
3. Results
CARAT Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bousquet, J.; Schünemann, H.J.; Togias, A.; Bachert, C.; Erhola, M.; Hellings, P.W.; Klimek, L.; Pfaar, O.; Wallace, D.; Ansotegui, I.; et al. Next-generation Allergic Rhinitis and Its Impact on Asthma (ARIA) Guidelines for Allergic Rhinitis Based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and Real-World Evidence. J. Allergy Clin. Immunol. 2020, 145, 70–80.e3. [Google Scholar] [CrossRef] [Green Version]
- Kansen, H.; Le, T.M.; Uiterwaal, C.; Van Ewijk, B.E.; Balemans, W.; Gorissen, D.; De Vries, E.; Van Velzen, M.; Slabbers, G.; Meijer, Y.; et al. Prevalence and Predictors of Uncontrolled Asthma in Children Referred for Asthma and Other Atopic Diseases. J. Asthma Allergy 2020, 13, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Massoth, L.J.; Anderson, C.; McKinney, K.A. Asthma and Chronic Rhinosinusitis: Diagnosis and Medical Management. Med. Sci. 2019, 7, 53. [Google Scholar] [CrossRef] [Green Version]
- Kanda, A.; Kobayashi, Y.; Asako, M.; Tomoda, K.; Kawauchi, H.; Iwai, H. Regulation of Interaction Between the Upper and Lower Airways in United Airway Disease. Med. Sci. 2019, 7, 27. [Google Scholar] [CrossRef] [Green Version]
- Global Initiative for Asthma. GINA Guidelines. Global Strategy for Asthma Management and Prevention. 2019. Available online: https://www.ginasthma.org (accessed on 4 April 2020).
- Meltzer, E.O. Allergic Rhinitis: Burden of Illness, Quality of Life, Comorbidities, and Control. Immunol. Allergy Clin. N. Am. 2016, 36, 235–248. [Google Scholar] [CrossRef]
- Tay, T.R.; Hew, M. Comorbid “treatable traits” in difficult asthma: Current evidence and clinical evaluation. Allergy 2018, 73, 1369–1382. [Google Scholar] [CrossRef]
- Miedinger, D.; Neukomm, E.; Chhajed, P.N.; Schnyder, A.; Naef, M.; Ackermann, M.; Leuppi, J.D. The use of the Asthma Control Test in general practice and its correlation with asthma control according to the GINA guidelines. Curr. Med. Res. Opin. 2011, 27, 2301–2308. [Google Scholar] [CrossRef]
- Ciprandi, G.; Schiavetti, I.; Ricciardolo, F. Symptom perception and asthma control. Postgrad. Med. 2015, 127, 738–743. [Google Scholar] [CrossRef]
- Demoly, P.; Jankowski, R.; Chassany, O.; Bessah, Y.; Allaert, F.A. Validation of a self questionnaire for assessing the control of allergic rhinitis. Clin. Exp. Allergy 2011, 41, 860–868. [Google Scholar] [CrossRef]
- Schatz, M.; Meltzer, E.O.; Nathan, R.; Derebery, M.J.; Mintz, M.L.; Stanford, R.H.; Dalal, A.A.; Silvey, M.J.; Kosinski, M. Psychometric validation of the Rhinitis Control Assessment Test: A brief patient-completed instrument for evaluating rhinitis symptom control. Ann. Allergy Asthma Immunol. 2010, 104, 118–124. [Google Scholar] [CrossRef]
- Nogueira-Silva, L.; Martins, S.; Cruz-Correia, R.; Azevedo, L.F.; Morais-Almeida, M.; Bugalho-Almeida, A.; Vaz, M.; Pereira, A.M.R.D.C.; Fonseca, J.A. Control of allergic rhinitis and asthma test: A formal approach to the development of a measuring tool. Respir. Res. 2009, 10, 5210. [Google Scholar] [CrossRef] [Green Version]
- Fonseca, J.A.; Nogueira-Silva, L.; Morais-Almeida, M.; Azevedo, L.F.; Sa-Sousa, A.; Ferreira, M.B.; Fernandes, L.; Bousquet, J. Validation of a questionnaire (CARAT10) to assess rhinitis and asthma in patients with asthma. Allergy 2010, 65, 1042–1048. [Google Scholar] [CrossRef]
- Fonseca, J.A.; Nogueira-Silva, L.; Morais-Almeida, M.; Sa-Sousa, A.; Azevedo, L.F.; Ferreira, J.A.; Ferreira, M.B.; Alves, R.R.; Bugalho-Almeida, A.; Bousquet, J. Control of Allergic Rhinitis and Asthma Test (CARAT) can be used to assess individual patients over time. Clin. Transl. Allergy 2012, 2, 16. [Google Scholar] [CrossRef] [Green Version]
- Mokkink, L.; Terwee, C.B.; Knol, D.L.; Stratford, P.W.; Alonso, J.; Patrick, D.L.; Bouter, L.M.; De Vet, H.C. The COSMIN checklist for evaluating the methodological quality of studies on measurement properties: A clarification of its content. BMC Med. Res. Methodol. 2010, 10, 22. [Google Scholar] [CrossRef] [Green Version]
- Azevedo, P.; Correia-De-Sousa, J.; Bousquet, J.; Bugalho-Almeida, A.; Del Giacco, S.R.; Demoly, P.; Haahtela, T.; Jacinto, T.; Larsen, V.G.; Van Der Molen, T.; et al. Control of allergic rhinitis and asthma test (CARAT): Dissemination and applications in primary care. Prim. Care Respir. J. 2013, 22, 112–116. [Google Scholar] [CrossRef]
- Domingues, M.; Amaral, R.; Fonseca, J.A.; Azevedo, P.; Correia-de-Sousa, J. Assessment of Asthma Control Using CARAT in Patients with and Without Allergic Rhinitis: A Pilot Study in Primary Care. Rev. Port. Pneumol. 2016, 22, 163–166. [Google Scholar] [CrossRef] [Green Version]
- Emons, J.A.M.; Flokstra, B.M.J.; De Jong, C.; Van Der Molen, T.; Brand, H.K.; Arends, N.J.T.; Amaral, R.; Fonseca, J.A.; Van Wijk, R.G. Use of the Control of Allergic Rhinitis and Asthma Test (CARATkids) in children and adolescents: Validation in Dutch. Pediatric Allergy Immunol. 2017, 28, 185–190. [Google Scholar] [CrossRef]
- Amaral, R.; Carneiro, A.C.; Wandalsen, G.; Fonseca, J.A.; Sole, D. Control of Allergic Rhinitis and Asthma Test for Children (CARATKids) Validation in Brazil and cutoff values. Ann. Allergy Asthma Immunol. 2017, 118, 551–556. [Google Scholar] [CrossRef]
- De Blok, B.M.J.F.; Baretta, H.-J.; Fonseca, J.A.; Van Heijst, E.; Kollen, B.J.; De Kroon, J.; Van Der Molen, T.; Tsiligianni, I.; De Jong, C.; Kocks, J.H. Control of Allergic Rhinitis and Asthma Test with 1-week recall: Validation of paper and electronic version. Allergy 2018, 73, 2381–2385. [Google Scholar] [CrossRef]
- Gani, F.; Lombardi, C.; Bonizzoni, G.; Rolla, G.; Brussino, L.; Landi, M.; Schiappoli, M.; Senna, G.; Savi, E.; Ridolo, E.; et al. The Characteristics of Severe Chronic Upper-Airway Disease (SCUAD) in Patients With Allergic Rhinitis: A Real-Life Multicenter Cross-Sectional Italian Study. Int. Arch. Allergy Immunol. 2019, 178, 333–337. [Google Scholar] [CrossRef]
- Linhares, D.; Fonseca, J.; Borrego, L.; Matos, A.; Pereira, A.; Sousa, A.; Gaspar, Â.; Mendes, C.; Moreira, C.; Gomes, E.; et al. Validation of Control of Allergic Rhinitis and Asthma Test for Children (CARATKids)—A prospective multicenter study. Pediatr. Allergy Immunol. 2014, 25, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Borrego, L.M.; Fonseca, J.A.; Pereire, A.M.; Pinto, V.R.; Linhares, D.; Morais-Almeida, M. Development process and cognitive testing of CARATkids—Control of allergic rhinitis and asthma test for children. BMC Pediatrics 2014, 14, 34. [Google Scholar] [CrossRef] [Green Version]
- Martins, S.P.; Teixeira, P.M.; Yaphe, J.; Fonseca, J.A.; Correia-De-Sousa, J. A Comparison of the CARATKids and CARAT10 Questionnaires for the Evaluation of Control of Asthma and Allergic Rhinitis in Adolescents. J. Investig. Allergol. Clin. Immunol. 2019, 29, 239–250. [Google Scholar] [CrossRef]
- Cilluffo, G.; Fasola, S.; Ferrante, G.; Montalbano, L.; Baiardini, I.; Indinnimeo, L.; Viegi, G.; Fonseca, J.A.; La Grutta, S. Overrating classifier performance in ROC analysis in the absence of a test set: Evidence from simulation and Italian CARATkids validation. Method Inform. Med. 2019, 58, e27–e42. [Google Scholar] [CrossRef]
- Liu, A.H.; Zeiger, R.S.; Sorkness, C.; Mahr, T.; Ostrom, N.; Burgess, S.; Rosenzweig, J.C.; Manjunath, R. Development and cross-sectional validation of the Childhood Asthma Control Test. J. Allergy Clin. Immunol. 2007, 119, 817–825. [Google Scholar] [CrossRef]
- Tosca, M.A.; Silvestri, M.; Olcese, R.; Pistorio, A.; Rossi, G.A.; Ciprandi, G. Breathlessness perception assessed by the visual analog scale and lung function in children with asthma: A real-life study. Pediatric Allergy Immunol. 2012, 23, 537–542. [Google Scholar] [CrossRef]
- Caimmi, D.; Baiz, N.; Tanno, L.K.; Demoly, P.; Arnavielhe, S.; Murray, R.; Bedbrook, A.; Bergmann, K.C.; De Vries, G.; Fokkens, W.J.; et al. Validation of the MASK-rhinitis Visual Analogue Scale on Smartphone Screens to Assess Allergic Rhinitis Control. Clin. Exp. Allergy 2017, 47, 1526–1533. [Google Scholar] [CrossRef]
- Passalacqua, G.; Ciprandi GPasquali, M.; Guerra, L.; Canonica, G.W. An update on the asthma-rhinitis link. Curr. Opin. Allergy Clin. Immunol. 2004, 4, 177–183. [Google Scholar] [CrossRef]
- Ciprandi, G.; Gallo, F.; Ricciardolo, F. A real-life comparison between Asthma Control Test and GINA asthma control grading. Ann. Allergy Asthma Immunol. 2016, 117, 725–727. [Google Scholar] [CrossRef]
- Milger, K.; Korn, S.; Buhl, R.; Hamelmann, E.; Herth, F.J.; Gappa, M.; Drick, N.; Fuge, J.; Suhling, H. Age- and sex-dependent differences in patients with severe asthma included in the German asthma net cohort. Resp. Med. 2020, 162, 105858. [Google Scholar] [CrossRef]
- Sherman, R.E.; Anderson, S.A.; Pan, G.J.D.; Gray, G.W.; Gross, T.; Hunter, N.L.; LaVange, L.; Marinac-Dabic, D.; Marks, P.; Robb, M.A.; et al. Real-world evidence—What is it and what can it tell us? N. Engl. J. Med. 2016, 375, 2293–2297. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| All Patients (N = 138) | Children (N = 88) | Adolescents (N = 50) | |
|---|---|---|---|
| Age (mean, years) | 11.5 | 9.9 | 14.3 |
| Gender (male) | 93/138 (67.4%) | 58/88 (65.9%) | 35/50 (70.0%) |
| GINA-based asthma control | |||
| Well-controlled | 56.5% | 54.6% | 60.0% |
| Partly-controlled | 32.6% | 32.9% | 30.0% |
| Uncontrolled | 10.9% | 12.5% | 10.0% |
| VAS Asthma (mean ± SD) | 7.2 (±2.8) | 7.0 (±2.8) | 7.5 (±2.67) |
| FEV1 (mean ± SD) | 98.0 (±13.7) | 96.8 (±14.13) | 101.5 (±12.75) |
| FEF25-75 (mean ± SD) | 95.0 (±25.9) | 89.8 (±27.2) | 103.8 (±21.1) |
| VAS rhinitis (mean ± SD) | 6.90 (±2.4) | 6.96 (±2.4) | 6.76 (±2.4) |
| cACT (mean ± SD) | N/A | 21.8 (±3.86) | N/A |
| ACT score (mean ± SD) | N/A | N/A | 22.3 (±2.66) |
| CARATKids (mean ± SD) | 4.56 (±2.56) | 4.90 (±2.53) | 3.98 (±2.54) |
| CARAT (mean ± SD) | N/A | N/A | 22.5 (±4.23) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tosca, M.A.; Del Barba, P.; Licari, A.; Ciprandi, G.; Asthma and Rhinitis Control Study Group. The Measurement of Asthma and Allergic Rhinitis Control in Children and Adolescents. Children 2020, 7, 43. https://0-doi-org.brum.beds.ac.uk/10.3390/children7050043
Tosca MA, Del Barba P, Licari A, Ciprandi G, Asthma and Rhinitis Control Study Group. The Measurement of Asthma and Allergic Rhinitis Control in Children and Adolescents. Children. 2020; 7(5):43. https://0-doi-org.brum.beds.ac.uk/10.3390/children7050043
Chicago/Turabian StyleTosca, Maria Angela, Paolo Del Barba, Amelia Licari, Giorgio Ciprandi, and Asthma and Rhinitis Control Study Group. 2020. "The Measurement of Asthma and Allergic Rhinitis Control in Children and Adolescents" Children 7, no. 5: 43. https://0-doi-org.brum.beds.ac.uk/10.3390/children7050043