Idiopathic Hypertrophic Pachymeningitis: Does Earlier Treatment Improve Outcome?
by
Emilia Rizzo
1,2, 
Ailsa Elizabeth Ritchie
3,
Vinay Shivamurthy
4,
Ata Siddiqui
5 and
Ming Lim
6,7,* 1
Faculty of Medicine and Surgery, University of Catania, Piazza dell’Università 2, 95124 Catania, Italy
2
Great Ormond Street Hospital for Children NHS Foundation Trust, London WC1N 3JH, UK
3
Paediatric Ophthalmology, Evelina London Children’s Hospital at Guy’s and St Thomas’ NHS Foundation Trust, London SE1 7EH, UK
4
Paediatric Rheumatology, Evelina London Children’s Hospital at Guy’s and St Thomas’ NHS Foundation Trust, London SE1 7EH, UK
5
Department of Neuroradiology, King’s College Hospital NHS Foundation Trust, London SE5 9RS, UK
6
Children’s Neurosciences, Evelina London Children’s Hospital at Guy’s and St Thomas’ NHS Foundation Trust, King’s Health Partners Academic Health Science Centre, London SE1 7RS, UK
7
Faculty of Life Sciences and Medicine, Kings College London, London SE1 7RS, UK
*
Author to whom correspondence should be addressed.
Children 2021, 8(1), 11; https://0-doi-org.brum.beds.ac.uk/10.3390/children8010011
Submission received: 23 November 2020
/
Revised: 23 December 2020
/
Accepted: 25 December 2020
/
Published: 28 December 2020
(This article belongs to the Section Child Neurology)
Abstract
:Background/goal: Hypertrophic pachymeningitis is a rare chronic inflammatory disorder characterized by marked fibrous thickening of the cerebral and/or spinal dura mater. This condition has largely been reported in adults, but there are very few reports in children. Methods: We describe a 14-year-old boy with idiopathic hypertrophic pachymeningitis, who presented with deteriorating vision on a background of severe headache. We evaluated pediatric cases of hypertrophic pachymeningitis and compared treatments and their relation to outcomes. Results: There are only eleven pediatric cases of hypertrophic pachymeningitis reported in the literature. In the patients treated with steroids either at presentation or subsequent relapses, a good response was reported. In the cases with delayed initiation of steroid treatment, this was often related to an incomplete recovery. In our patient, this delay may have contributed to his poor visual outcome. Conclusions: Early initiation of steroid treatment in children with idiopathic hypertrophic pachymeningitis may improve outcomes.
1. Introduction
Hypertrophic pachymeningitis is a rare inflammatory disorder characterized by localized or diffuse thickening of the cranial or spinal dura mater, resulting in progressive neurological deficits. The etiology of the pachymeningitis is thought to be immune in nature or secondary to other possible causes of dural reaction, such as infectious conditions (neurosyphilis, tuberculosis, fungal infections, syphilis, Lyme’s disease); collagen vascular disorders (granulomatosis with polyangiitis, rheumatoid arthritis, systemic lupus erythematosus, mixed connective tissue disease); neoplasia (dural carcinomatosis, meningioma en plaque, lymphoma) and miscellaneous disorders such as sarcoidosis, mucopolysaccharidosis, intracranial hypotension syndrome and intrathecal drug administration [1,2]. IgG4-related hypertrophic pachymeningitis (IgG4-RHP), a recently described entity, is an increasingly recognized manifestation of IgG4-related disease, a fibroinflammatory condition that can affect virtually any organ [3]. The present report describes a 14-year-old boy with idiopatic hypertrophic pachymeningitis, the course of his illness, his response to treatment and a comparison to the other cases reported in literature.
2. Case Study
A previously healthy 14-year-old boy presented with a several-week history of deteriorating vision on a background of experiencing headaches 9 months prior, which worsened over recent months. He reported double vision and progressive loss of vision in the right eye over the few weeks prior to presentation. There were no other constitutional symptoms like fever, night sweats or weight loss. The patient reported a non-specific insect bite 3 months prior, and there was no history of recent foreign travel.
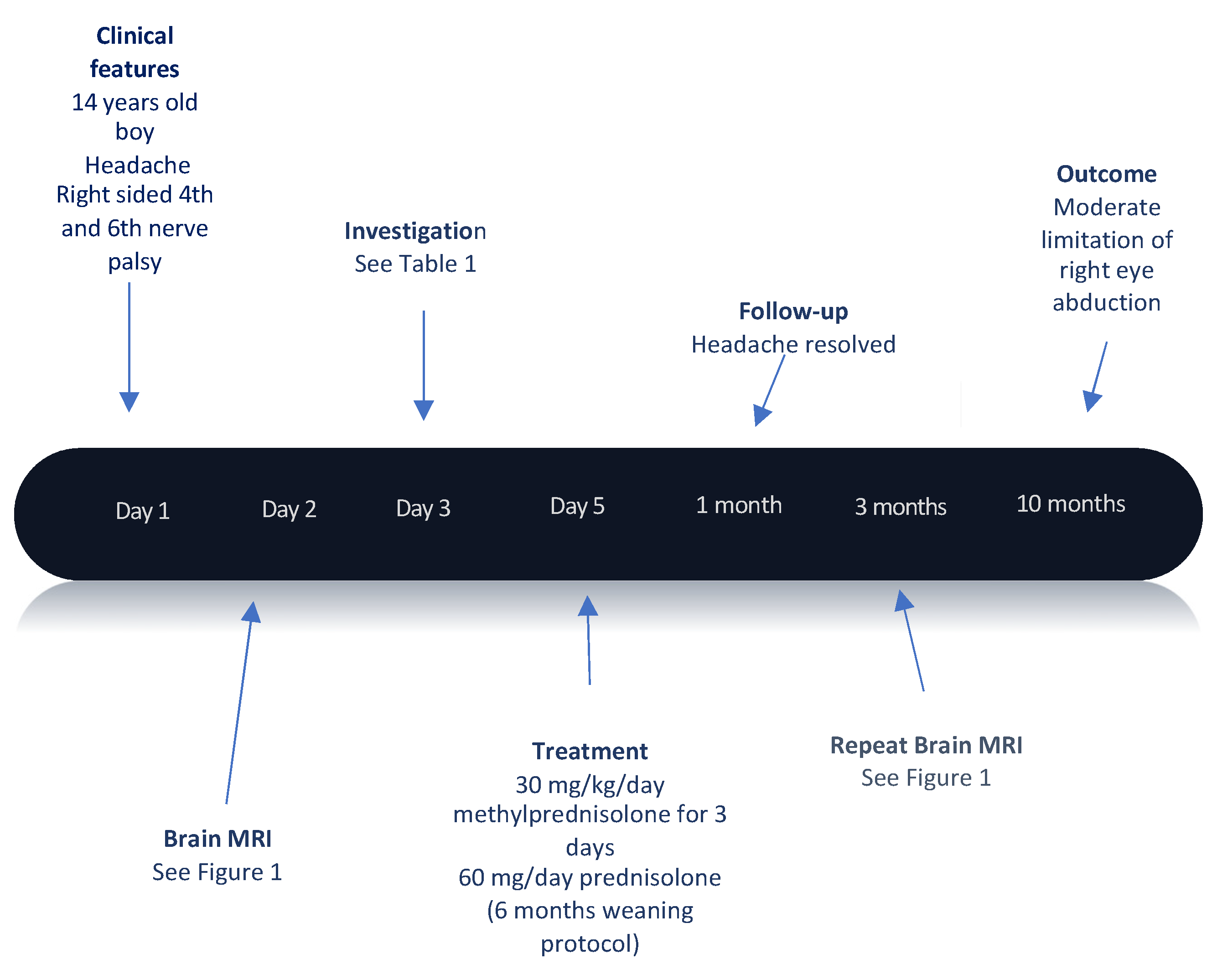
The key finding on clinical examination was a fulminant right optic neuritis, where he could only perceive light, alongside right sided 4th and 6th cranial nerve palsy. There was no evidence of uveal disease. He had a full neurological examination, which did not reveal any abnormality. His systemic examination was normal and in particular there was no evidence of lymphadenopathy, organomegaly or cutaneous features of connective tissue disease.
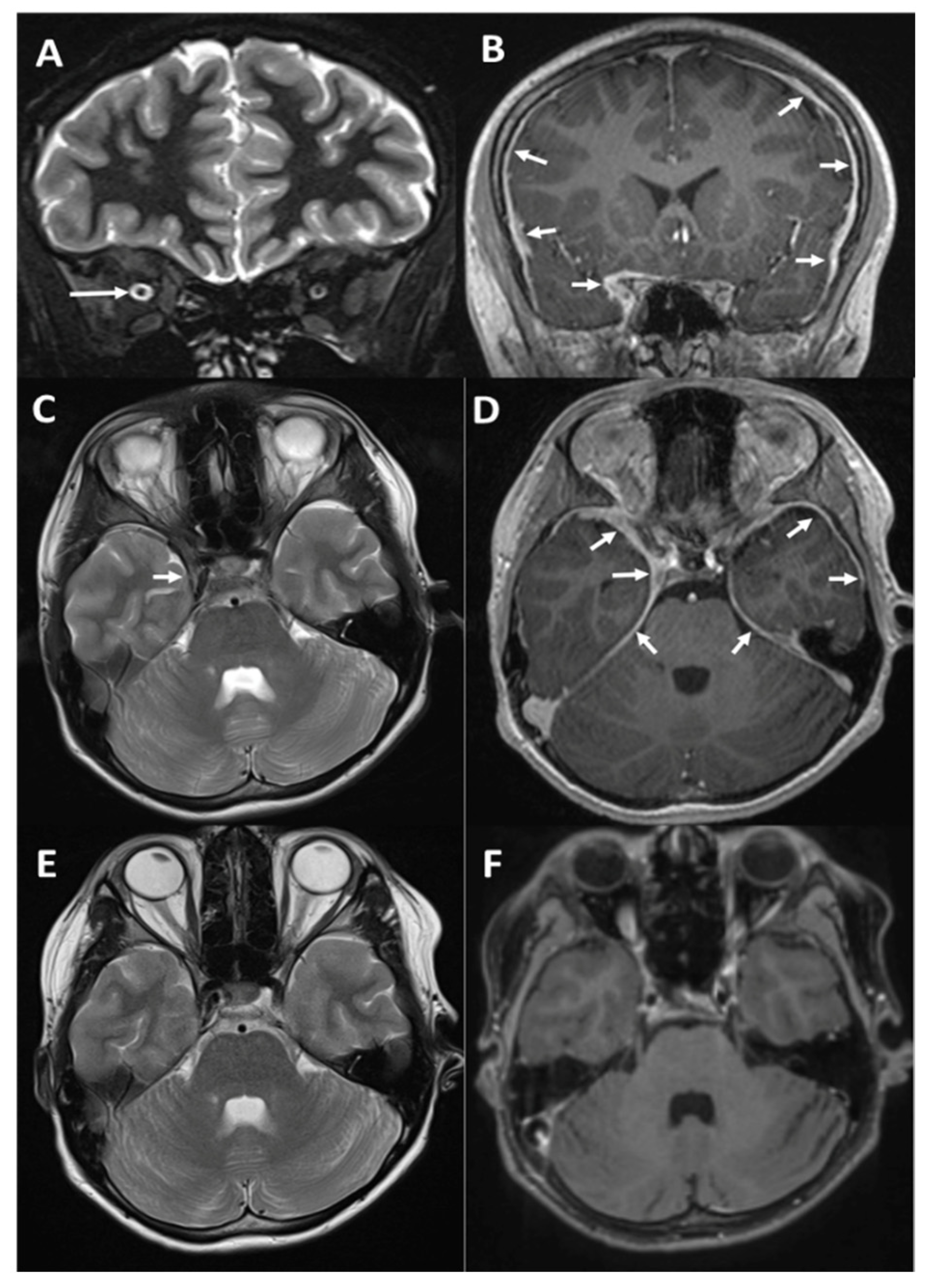
Magnetic resonance imaging (MRI) identified widespread dural (pachymeningeal) thickening with contiguous involvement of the cavernous sinus on the right side (Figure 1) with no evidence of brain parenchymal or white matter involvement.
Following consultation with the infectious diseases and rheumatology team, investigations were initiated which did not reveal an infective or immune etiology for the presumed pachymeningitis (Table 1).
High-dose pulsed intravenous methylprednisolone 30 mg/kg/day was administered for 3 consecutive days and his vision began to improve (counting fingers), along with a vast improvement in his headaches. He was converted to 60 mg prednisolone orally daily. Although dural biopsy was considered, a marked improvement in his imaging (Figure 1) to a near resolution of the lesion did not present us with a biopsy target. Similarly, systemic imaging with a whole-body MRI also failed to identify a potential lesion to biopsy or any underlying systemic process.
He was reviewed in the outpatient clinic a month after discharge and was doing well. His headaches had resolved completely (timeline detailed in Figure 2). Ophthalmology assessment revealed an ongoing reduction of vision in the right eye with a central visual acuity of LogMAR 1.52 (2/60) and remaining limitation of abduction in the right eye to the mid-line. His optical coherence tomography showed retinal nerve fiber layer thinning in the right eye and a stable, normal retinal nerve fiber layer in the left eye.
At 3 months from symptom presentation, while on a slow steroid taper (10 mg daily, 6 months weaning protocol), repeat imaging continues to demonstrate no active dural disease. At latest follow-up (10 months), he remains well clinically and his visual acuity has improved to LogMAR 0.50 (6/19) in the right eye. His eye movements also continue to improve, with only 25% limitation of right abduction and he has no esotropia or double vision when looking straight ahead. He continues to have a mild right relative afferent pupillary defect and a pale right optic disc.
3. Discussion
Hypertrophic pachymeningitis was first described by Charcot and Joffroy in 1869 [4]. It is a rare chronic inflammatory disorder characterized by marked thickening of the cerebral and/or spinal dura matter. It has been described in association with infection, trauma, tumors and immune-mediated disease such as granulomatosis with polyangiitis, neurosarcoidosis or IgG4 related disease [1,2,3,5]. In cases when no causative factors can be identified, the condition is referred to as ‘idiopathic” [6].
The thickened dura causes progressive neurological impairment. Chronic headache and multiple cranial neuropathies are the most common clinical manifestations [5,6]. These may include ataxia, facial pain, cranial nerve involvement and neuro-ophthalmic complications such as papilledema and various neurological deficits [1,2].
The diagnostic workup should include serology tests for VZV, Mycoplasma pneumoniae, Haemophilus influenzae type B, HTLV1(Human T-cell lymphotropic virus type 1), HHV6(Human Herpes Virus 6), Enterovirus, Borrelia burgdorferi, CMV(cytomegalovirus), HIV(Human Immunodeficiency Virus), syphilis, EBV(Epstein-Barr Virus) and, in endemic areas, tuberculosis tests (Quantiferon tests and/or Mantoux skin testing). Moreover, an autoimmune screening is recommended, including neuronal surface antibody research and a complete CSF (Cerebral Spinal Fluid) exam.
The definitive diagnosis is based on MRI or brain biopsy of the thickened dura mater, which reveals interstitial fibrosis and inflammatory cell infiltration.
This condition has largely been reported in adults, but there are very few reports in children. We performed a review of the literature (Medline 1990–present) using the search terms (hypertrophic pachymeningitis) AND (paediatric OR pediatric OR children OR childhood). Twelve cases referring to children (<18 years old) were identified and the full manuscripts were available for review [7,8,9,10,11,12,13,14,15,16,17,18].
Among the twelve pediatric cases of hypertrophic pachymeningitis reported in the literature, three cases developed in association with tuberculosis [10,11,17], one was PR3-ANCA-associated [13], two developed in association with IgG4-RD [16,18] and six were regarded as idiopathic [7,8,9,12,14,15]. The clinical features, MRI findings, biopsy results, treatment and outcomes are summarized in Table 2.
In the patients treated with steroids either at presentation or subsequent relapses, a good response to steroids was reported (6 events; Case 2 relapse (R) 1; Case 3 presentation (P) and R1; Case 5 P; Case 7 R1; Case 9 P; Case 12 P and R1).
However, the course of the disease was chronic and relapsing in six of the 13 cases, necessitating more aggressive immune therapy such as methotrexate, cyclophosphamide, intraventricular cytarabine, azathriopine or rituximab (Cases 2, 3, 6, 7, 9 and 12).
Of the two patients (Cases 1 and 2) treated conservatively, one patient relapsed, who then responded to steroids (Case 2). Overall, all but one case (Case 6), had a satisfactory outcome (mRS 0–2). Residual visual deficits occurred in two cases and hypoglossal palsy in one case (Cases 3, 5 and 9); one chronically deteriorated neurologically into a chronic vegetative state (Case 6).
Although immunotherapy-responsive, the delay in initiating steroid treatment in our patient may have contributed to his poor visual outcome. In the reported cases with a lag in initiating steroid treatment, this was often related to an incomplete recovery (Case 2 initiating 21 months later at relapse; Case 3 6 months from prior episode managed as viral meningitis; Case 6 10 weeks).
In conclusion, idiopathic hypertrophic pachymeningitis can present in children and should be considered in cases of pachymeningitis and negative findings from diagnostic evaluation.
Early initiation of steroid treatment may improve the outcome.
Author Contributions
E.R. and M.L. performed the literature review, derived the key messages of the manuscript, wrote and revised all versions of manuscripts. A.E.R., V.S. and A.S. reviewed the relevant specialty-specific data and revised all versions of the manuscripts. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Patent and family have consented to clinical history and investigations being presented in this publication.
Data Availability Statement
Authors will be happy to share anonymized clinical data additional to those provided in manuscript uopn request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dash, G.K.; Thomas, B. Clinico-radiological spectrum and outcome in idiopathic hypertrophic pachymeningitis. J. Neurol. Sci. 2015, 350, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Kupersmith, M.J.; Martin, V. Idiopathic hypertrophic pachymeningitis. Neurology 2004, 62, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Melenotte, C.; Seguier, J. Clinical presentation, treatment and outcome of IgG4-related pachymeningitis: From a national case registry and literature review. Semin. Arthritis Rheum. 2019, 49, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Charcot, J.M.; Joffroy, A. Deux cas d’atrphie musculaire progressive avec lesions de la substance grise et des faisceaux anterolateraux de la moelle epiniere (in French). Arch. Physiol. Norm. Pathol. 1869, 2, 354–367, 629–649, 744–746. [Google Scholar]
- Hahn, L.D.; Fulbright, R. Hypertrohic pachymeningitis. J. Neurolog. Sci. 2016, 367, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Riku, S.; Kato, S. Idiopathic hypertrophic pachymeningitis. Neuropathology 2003, 23, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Asano, T.; Hayashida, M. Hypertrophic cranial pachymeningitis in a patient with aplastic anemia. Ann. Hematol. 1998, 77, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Van Toorn, R.; Esser, M. Idiopathic hypertrophic cranial pachymeningitis causing progressive polyneuropathies in a child. Eur. J. Paediatr. Neurol. 2008, 12, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Aburahma, S.K.; Anabtawi, A.G. Idiopathic hypertrophic pachymeningitis in a child with hydrocephalus. Pediatr. Neurol. 2009, 40, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Karimi, A.; Tabatabaei, S.R. Tuberculous pachymeningitis in a young child with spinal involvement: A case report. Arch. Pediatr. Infect. Dis. 2013, 1, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.K.; Saikia, B. Pachymeningitis in a young child responded to antitubercular therapy: A case report. J. Child Neurol. 2014, 29, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, K.; Fukumura, S. Rapidly progressive fatal idiopathic hypertrophic pachymeningitis with brainstem involvement in a child. Childs Nerv. Syst. 2018, 34, 1795–1798. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Akiyama, M. Adolescent PR3-ANCA-positive hypertrophic pachymeningitis. A case report and review of the literature. Medicine 2018, 97, 17. [Google Scholar] [CrossRef] [PubMed]
- Brand, B.; Somers, D. Diplopia with dural fibrotic thickening. Semin. Pediatr. Neurol. 2018, 26, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, D.T.; Faux, B.M. Headache and hypoglossal nerve palsy in a child with idiopathic hypertrophic pachymeningitis. Headache 2019, 59, 1390–1391. [Google Scholar] [CrossRef] [PubMed]
- Nambirajan, A.; Sharma, M. Large dural-based mass with bony hyperostosis in a 16-year-old male: IgG4-related disease mimicking lymphoplasmacyte-rich meningioma. Childs Nerv. Syst. 2019, 35, 1423–1427. [Google Scholar] [CrossRef] [PubMed]
- Sharawat, I.K.; Saini, A.G. “Encased brain” in hypertrophic pachymeningitis. Childs Nerv. Syst. 2019, 35, 585–587. [Google Scholar] [CrossRef] [PubMed]
- Vakrakou, G.; Evangelopoulos, M. Recurrent myelitis and asymptomatic hypophysitis in IgG4-related disease: Case-based review. Rheumatol. Int. 2020, 40, 337–343. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
MRI findings in our patient. Top row (A,B): Coronal STIR image at presentation showing mild congestion of the right orbit with a dilated optic nerve sheath but normal signal of the optic nerve ((A), long arrow); coronal post-contrast T1w (T1 weighted) image showing diffuse dural thickening extending to the right cavernous sinus and optic canal, where it surrounds the optic nerve ((B), small arrows). Middle row (C,D): Axial T2w (C) and post-contrast T1w (D) images showing normal brain appearances but diffuse bilateral dural thickening with subtle corresponding low signal on T2. Bottom row ((E,F)): Follow-up imaging after a month showing resolution of the dural enhancement, though there is still some evidence of right 6th cranial nerve palsy (note the adducted right globe).
Figure 1.
MRI findings in our patient. Top row (A,B): Coronal STIR image at presentation showing mild congestion of the right orbit with a dilated optic nerve sheath but normal signal of the optic nerve ((A), long arrow); coronal post-contrast T1w (T1 weighted) image showing diffuse dural thickening extending to the right cavernous sinus and optic canal, where it surrounds the optic nerve ((B), small arrows). Middle row (C,D): Axial T2w (C) and post-contrast T1w (D) images showing normal brain appearances but diffuse bilateral dural thickening with subtle corresponding low signal on T2. Bottom row ((E,F)): Follow-up imaging after a month showing resolution of the dural enhancement, though there is still some evidence of right 6th cranial nerve palsy (note the adducted right globe).

Figure 2.
Timeline of our patient’s history.


{kind=link}
{kind=link}
Table 1.
Investigations excluding infectious and immune etiology of pachymeningitis in our case.
| Infective Etiology | Serology/PCR * | |
| VZV, Mycoplasma pneumoniae, Haemophilus influenzae type B, HTLV1 *, HHV6 *, Enterovirus *, Borrelia burgdorferi, CMV *, HIV, Syphilis, EBV | Negative | |
| Immune-Mediated Disease | Autoimmune screening | |
| ANA, Anti-dsDNA, Anti-SSA, Anti-SSB, Anti-phospholipid, Anti-cardiolipin, ANCA | Negative | |
| Neuronal surface and glial antibodies | ||
| MOG, Aquaporin 4, Glycine receptor | Negative | |
| CSF | ||
| WBC/mm3 | <1 | |
| Protein (mg/dL) and Glucose (mg/dL) | Normal | |
| Serum ACE level | 44 (normal) | |
| Other Investigations | Chest XR | Normal |
| Abdomen US | Normal |
HTLV1: Human T-cell lymphotropic virus type 1; HHV6: Human Herpes Virus 6; CMV: cytomegalovirus; HIV: Human Immunodeficiency Virus; EBV: Epstein-Barr Virus; MOG: Myelin-oligodentrocyte glycoprotein; CSF: Cerebral Spinal Fluid; asterisk by PCR would indicate that those with asterisk indicate PCR tersting.
Table 2.
Clinical data of 13 patients with hypertrophic pachymeningitis.
| Case Report | Clinical Features and Course | MRI | Investigation and Aetiology | Treatment | Outcome (mRS Score) |
|---|---|---|---|---|---|
| Case 1 Asano et al. (1998) 13 years F [7] | P: Headache, vomiting and aplastic anemia | P: Enhancement T1: Thickening of dura mater in tentorial region | Brain biopsy ND Idiopathic | P: Conservative | Full recovery, 6 months (mRS 0) |
| Case 2 Van Toorn et al. (2008) 10 years M [8] | P: Right 6th nerve palsy R1 21 months: Progressive cranial polyneuropathies | P: Normal R1: Enhancement T1: Widespread dural thickening | Brain biopsy ND Idiopathic | P: Conservative R1: IVMP; prednisone; MTX | Residual small angle esotropia, 1 year (mRS 1) |
| Case 3 Aburahma et al. (2009) 3 years 6 months M [9] | P: Headache, vomiting and irritability. R1 1 month: Progression of pachymeningitis R2 3 months: Headache, vomiting and irritability. Decline visual activity R3 6 months: Headache, ataxia, poor vision and focal seizures. | P: Enhancement T1 in tentorium cerebelli and spinal meninges; non-communicating hydrocephalus R1–R3: increasing meningeal enhancement | Brain biopsy: thickened and fibrotic dura mater Idiopathic | P: IVMP, prednisone R1: Steroids R2: CP R3: Intratecal cytarabine, hydrocortisone | Disinhibition, hyperactivity, poor vision and mildly ataxic gait, 3 years (mRS 2) |
| Case 4 Karimi et al. (2013) 4 years M [10] | P: Fever, meningism and left hemiparesis | P: Meningeal enhancement in frontal lobe; T10–T11 mass | Brain biopsy ND Spinal biopsy: tuberculous | P: TB therapy | Full recovery, 4 weeks (mRS 0) |
| Case 5 Sharma et al. (2014) 2 years 11 months F [11] | P: Fever, bilateral visual loss, left 3rd and 7th palsy | P: Enhancement T1 dura mater; cavernous sinus thrombosis; multifocal acute infarcts | Brain biopsy ND QuantiFERON-TB +ve | P: TB therapy; steroids | Residual mild left ptosis, 6 months (mRS 1) |
| Case 6 Tsuchida et al. (2018) 3 years F [12] | P: Headache, vomiting and weakness Weight loss; R1 10w: Seizure and encephalopathy R2 4 months: Lost of light reflex and spontaneous respiration | P: Gadolinium enhancement T1: widespread thickening of dura; communicating hydrocephalus R1–R2: Progressive dural thickening and brainstem lesions | Brain biopsy: thickened and fibrotic dura mater Idiopathic | P: Conservative R1–R2: IVMP, CP intrathecal cytarabine | Chronic vegetative state prior to death, 4 months (mRS 6) |
| Case 7 Matsumoto et al. (2018) [13] 14 years F | P: fullness and pain in her right ear R1: headache and dysarthria | P: mastoiditis involving the right temporal bone R1: extensive hypertrophy of the right hemispheric dura mater | Brain Biopsy: prominent inflammation and severe fibrosis. PR3-ANCA positive | P: Mastoidectomy + steroids + MTXR1: Steroids + CP | Full recovery, 1 month (mRS 0) |
| Case 8 Brand et al. (2018) 13 years M [14] | P: Headache, left 6th palsy R1 3w: Right eye diplopia | P: nodular dural enhancement and thickening in the right cerebrum, right cavernous sinus, and basilar cistern. | Brain biopsy: atypical lymphocytic infiltrate Idiopathic | P: IV cancomycin, ceftriaxone, and azithromycin R1: Conservative | Full recovery, 1 month (mRS 0) |
| Case 9 Hsieh et al. (2019) 16 years F [15] | P: Headache, right 12th nerve palsy R1 2w: Headache, right 12th nerve palsy | P: Gadolinium enhancement T1: Posterior fossa pachymeningeal thickening R1: No improvement of dural thickening | Brain biopsy: dural mixed inflammation Idiopathic | P: Steroids R1: Rituximab | Residual hypoglossal palsy, 2 years (mRS 1) |
| Case 10 Nambirajan et al. (2019) 16 years M [16] | P: right-sided focal seizures | P: large extra-axial contrast-enhancing lesion in the left frontoparietal region | Brain biopsy: inflammatory infiltrate along the dura–brain interface and predominated in histiocytes; IgG4-positive plasma cells IgG4-RD | P: Mass excision | Full recovery, 4 months (mRS 0) |
| Case 11 Sharawat et al.(2019) [17] 4 years F | P: left hemiparesis, communicating hydrocephalous R1: Left-sided ptosis, incomplete ophtalmoparesis, left-sided facial paresis, left hemiparesis | R1: mid-brain lesions, left-sided subdural collection, diffuse hypertrophic pachymeningitis, encephalomalacic changes in the right basal ganglia | Brain biopsy ND Tuberculous | P: TB therapy R1: TB therapy, steroids | Data not available |
| Case 12 Vakrakou et al. (2020) 17 years F [18] | P: mild upper limb weakness and a loss of dexterity with left hand R1 2 years: numbness of lower limb | P: Spine-longitudinal intramedullary damage, extending to the body of the C5 vertebra; Brain high-intensity lesions in the deep white matter, enlargement of hypophysis with homogeneous gadolinium enhancement R1: decline in lesion size and pituitary gland signal intensity | Brain biopsy ND IgG4-RD | P: Steroids + azathioprine R1: Steroids | Full recovery, 5 years (mRS 0) |
| Case 13 Our case 14 years M | P: Headache, double vision and visual loss; right 2nd, 4th and 6th nerve palsy | P Gadolinium enhancement T1: Thickening of dura mater and cavernous sinus on the right | Brain biopsy ND | P: IVMP, prednisolone | Moderate visual loss right eye, no esotropia, 10 months (mRS 1) |
M is Male and F female; CP: cyclophosphamide; IVMP: intravenous methylprednisolone; MTX: methotrexate; ND: not done; P: presentation; R: relapse; TB: tuberculous; IgG4-RD: IgG4-related cisease.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Rizzo, E.; Ritchie, A.E.; Shivamurthy, V.; Siddiqui, A.; Lim, M. Idiopathic Hypertrophic Pachymeningitis: Does Earlier Treatment Improve Outcome? Children 2021, 8, 11. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010011
AMA Style
Rizzo E, Ritchie AE, Shivamurthy V, Siddiqui A, Lim M. Idiopathic Hypertrophic Pachymeningitis: Does Earlier Treatment Improve Outcome? Children. 2021; 8(1):11. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010011
Chicago/Turabian StyleRizzo, Emilia, Ailsa Elizabeth Ritchie, Vinay Shivamurthy, Ata Siddiqui, and Ming Lim. 2021. "Idiopathic Hypertrophic Pachymeningitis: Does Earlier Treatment Improve Outcome?" Children 8, no. 1: 11. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010011
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.