
Innovative Techniques Associated with Traditional Abdominal Surgery in Complex Pediatric Cases: A Tertiary Center Experience

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Endoscopy and Robotic-Assisted Abdominal Surgery
3. Endoscopy and Abdominal Surgery
4. Endoscopic Retrograde Cholangiopancreatography (ERCP) and Laparoscopic Abdominal Surgery
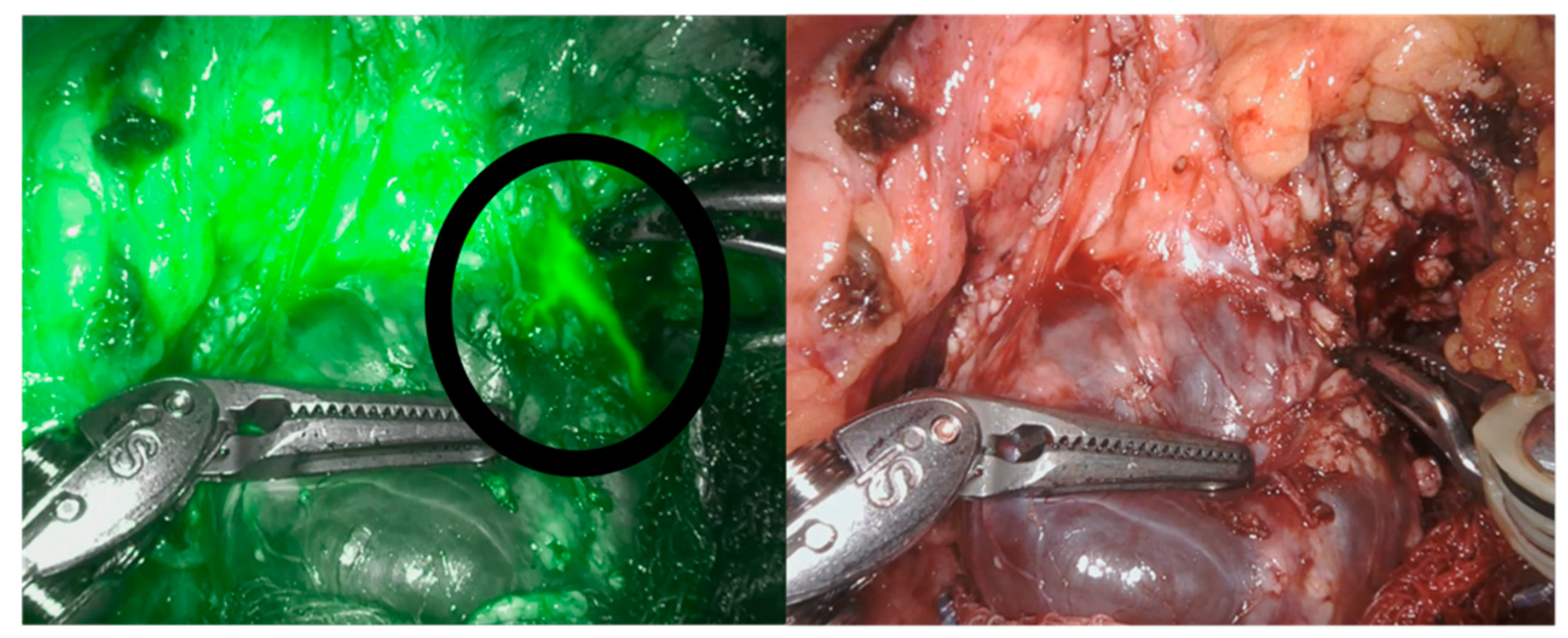
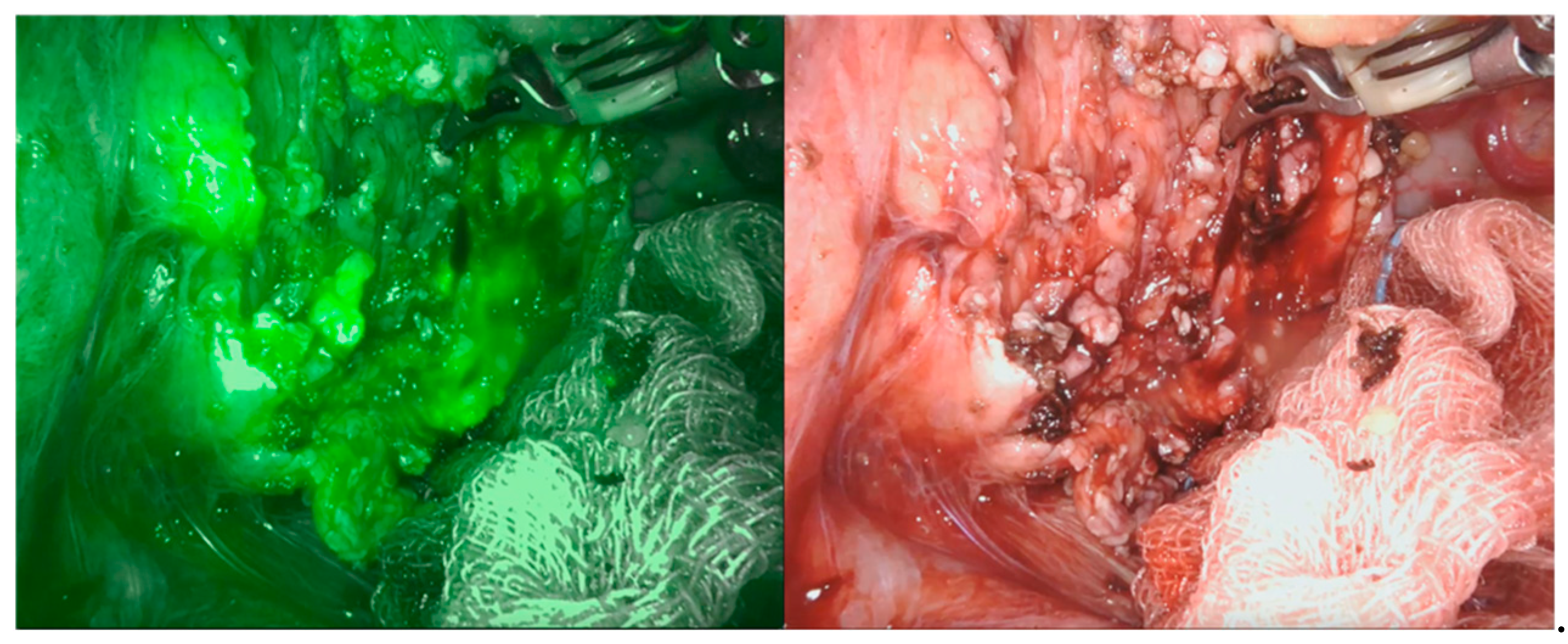
5. Near-Infrared Fluorescence and Robotic-Assisted Abdominal Surgery
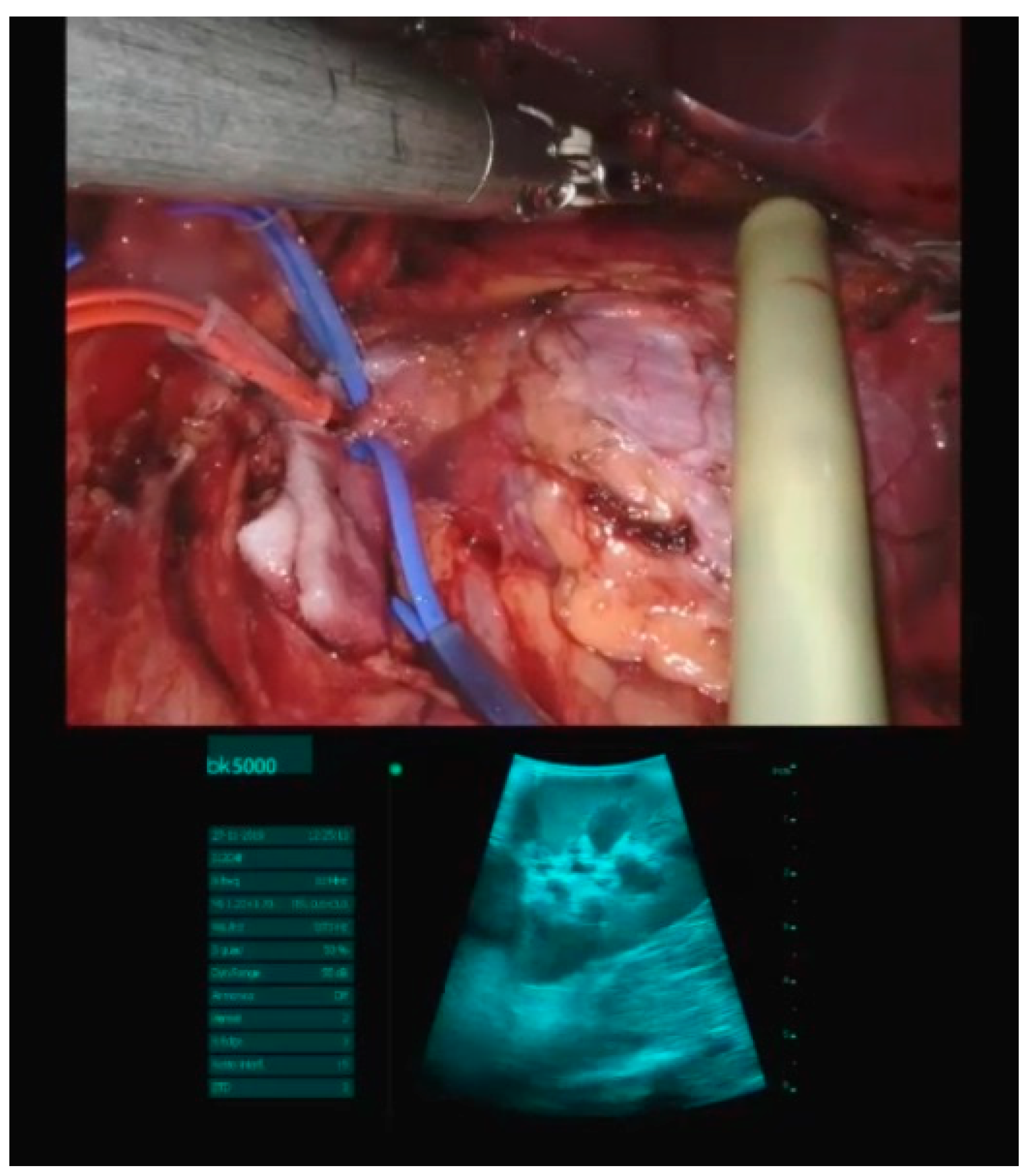
6. Intraoperative Ultrasonography and Robotic-Assisted Surgery
7. Brachytherapy and Abdominal Surgery
8. Microwave Ablation and Abdominal Surgery
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Klein, M.D.; Langenburg, S.E.; Kabeer, M.; Lorincz, A.; Knight, C.G. Pediatric robotic surgery: Lessons from a clinical experience. J. Laparoendosc. Adv. Surg. Tech. A 2007, 17, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Varda, B.K.; Johnson, E.K.; Clark, C.; Chung, B.I.; Nelson, C.P.; Chang, S.L. National trends of perioperative outcomes and costs for open, laparoscopic and robotic pediatric pyeloplasty. J. Urol. 2014, 191, 1090–1095. [Google Scholar] [CrossRef] [PubMed]
- Esposito, C.; Settimi, A.; Del Conte, F.; Cerulo, M.; Coppola, V.; Farina, A.; Crocetto, F.; Ricciardi, E.; Esposito, G.; Escolino, M. Image-Guided Pediatric Surgery Using Indocyanine Green (ICG) Fluorescence in Laparoscopic and Robotic Surgery. Front. Pediatr. 2020, 8, 314. [Google Scholar] [CrossRef] [PubMed]
- Tringali, A.; Thomson, M.; Dumonceau, J.-M.; Tavares, M.; Tabbers, M.M.; Furlano, R.; Spaander, M.; Hassan, C.; Tzvinikos, C.; Ijsselstijn, H.; et al. Pediatric gastrointestinal endoscopy: European Society of Gastrointestinal Endoscopy (ESGE) and European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) Guideline Executive summary. Endoscopy 2017, 49, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Demirel, B.D.; Yagiz, B.; Hancioglu, S.; Caltepe, G. Comparing Different Techniques in Children With or Without a Simultaneous Fundoplication: Does the Gastrostomy Technique Matter? J. Laparoendosc. Adv. Surg. Tech. A 2021, 31, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Zambaiti, E.; Virgone, C.; Bisoffi, S.; Stefanizzi, R.; Fascetti Leon, F.; Gamba, P. Long-Term Analysis of Respiratory-Related Complications Following Gastrostomy Placement with or without Fundoplication in Neurologically Impaired Children: A Retrospective Cohort Study. Children 2021, 8, 22. [Google Scholar] [CrossRef]
- Frazzoni, M.; Piccoli, M.; Conigliaro, R.; Frazzoni, L.; Melotti, G. Laparoscopic fundoplication for gastroesophageal reflux disease. World J. Gastroenterol. 2014, 20, 14272–14279. [Google Scholar] [CrossRef]
- Seeras, K.; Bittar, K.; Siccardi, M.A. Nissen Fundoplication; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Perger, L.; Watch, L.; Weinsheimer, R.; Fahl, J.; Azzie, G. Laparoscopically supervised PEG at time of Nissen fundoplication: A safe option. J. Laparoendosc. Adv. Surg. Tech. A 2008, 18, 136–139. [Google Scholar] [CrossRef]
- Jesch, N.K.; Schmidt, A.I.; Strassburg, A.; Glüer, S.; Ure, B.M. Laparoscopic fundoplication in neurologically impaired children with percutaneous endoscopic gastrostomy. Eur. J. Pediatr. Surg. 2004, 14, 89–92. [Google Scholar] [CrossRef]
- Gauderer, M.W.; Ponsky, J.L.; Izant, R.J.J. Gastrostomy without laparotomy: A percutaneous endoscopic technique. J. Pediatr. Surg. 1980, 15, 872–875. [Google Scholar] [CrossRef]
- Markar, S.R.; Karthikesalingam, A.P.; Hagen, M.E.; Talamini, M.; Horgan, S.; Wagner, O.J. Robotic vs. laparoscopic Nissen fundoplication for gastro-oesophageal reflux disease: Systematic review and meta-analysis. Int. J. Med. Robot. 2010, 6, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Cundy, T.P.; Harling, L.; Marcus, H.J.; Athanasiou, T.; Darzi, A.W. Meta analysis of robot-assisted versus conventional laparoscopic fundoplication in children. J. Pediatr. Surg. 2014, 49, 646–652. [Google Scholar] [CrossRef]
- Pio, L.; Musleh, L.; Paraboschi, I.; Pistorio, A.; Mantica, G.; Clermidi, P.; Leonelli, L.; Mattioli, G.; Sarnacki, S.; Blanc, T. Learning curve for robotic surgery in children: A systematic review of outcomes and fellowship programs. J. Robot. Surg. 2020, 14, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Jiwane, A.; Varjavandi, A.; Kennedy, A.; Henry, G.; Dilley, A.; Currie, B.; Adams, S.; Krishnan, U. Comparison of percutaneous endoscopic, laparoscopic and open gastrostomy insertion in children. Pediatr. Surg. Int. 2013, 29, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Mpody, C.; Hayes, S.; Rusin, N.; Tobias, J.D.; Nafiu, O.O. Risk Assessment for Postoperative Pneumonia in Children Living With Neurologic Impairments. Pediatrics 2021, 148, e2021050130. [Google Scholar] [CrossRef]
- Harte, C.; Ren, M.; Querciagrossa, S.; Druot, E.; Vatta, F.; Sarnacki, S.; Dahmani, S.; Orliaguet, G.; Blanc, T. Anaesthesia management during paediatric robotic surgery: Preliminary results from a single centre multidisciplinary experience. Anaesth. Crit. Care Pain Med. 2021, 40, 100837. [Google Scholar] [CrossRef]
- Muñoz, C.J.; Nguyen, H.T.; Houck, C.S. Robotic surgery and anesthesia for pediatric urologic procedures. Curr. Opin. Anaesthesiol. 2016, 29, 337–344. [Google Scholar] [CrossRef]
- Siau, K.; Levi, R.; Howarth, L.; Broughton, R.; Feeney, M.; Beales, I.L.P.; Tzivinikos, C.; Narula, P. Validity Evidence for Direct Observation of Procedural Skills in Paediatric Gastroscopy. J. Pediatr. Gastroenterol. Nutr. 2018, 67, e111–e116. [Google Scholar] [CrossRef]
- Siau, K.; Levi, R.; Iacucci, M.; Howarth, L.; Feeney, M.; Anderson, J.T.; Tzivinikos, C.; Thomson, M.; Narula, P. Paediatric Colonoscopy Direct Observation of Procedural Skills: Evidence of Validity and Competency Development. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 18–23. [Google Scholar] [CrossRef]
- Fusaro, F.; Tambucci, R.; Romeo, E.; Bagolan, P.; Dall’Oglio, L.; Ceccarelli, S.; Francalanci, P.; Hermans, D.; Pietrobattista, A.; Diamanti, A.; et al. Anastomotic ulcers in short bowel syndrome: New suggestions from a multidisciplinary approach. J. Pediatr. Surg. 2018, 53, 483–488. [Google Scholar] [CrossRef]
- Lee, H.-J.; Kim, H.-S.; Jeon, J.; Park, S.-H.; Lim, S.-U.; Jun, C.-H.; Park, S.-Y.; Park, C.-H.; Choi, S.-K.; Rew, J.-S. Endoscopic foreign body removal in the upper gastrointestinal tract: Risk factors predicting conversion to surgery. Surg. Endosc. 2016, 30, 106–113. [Google Scholar] [CrossRef]
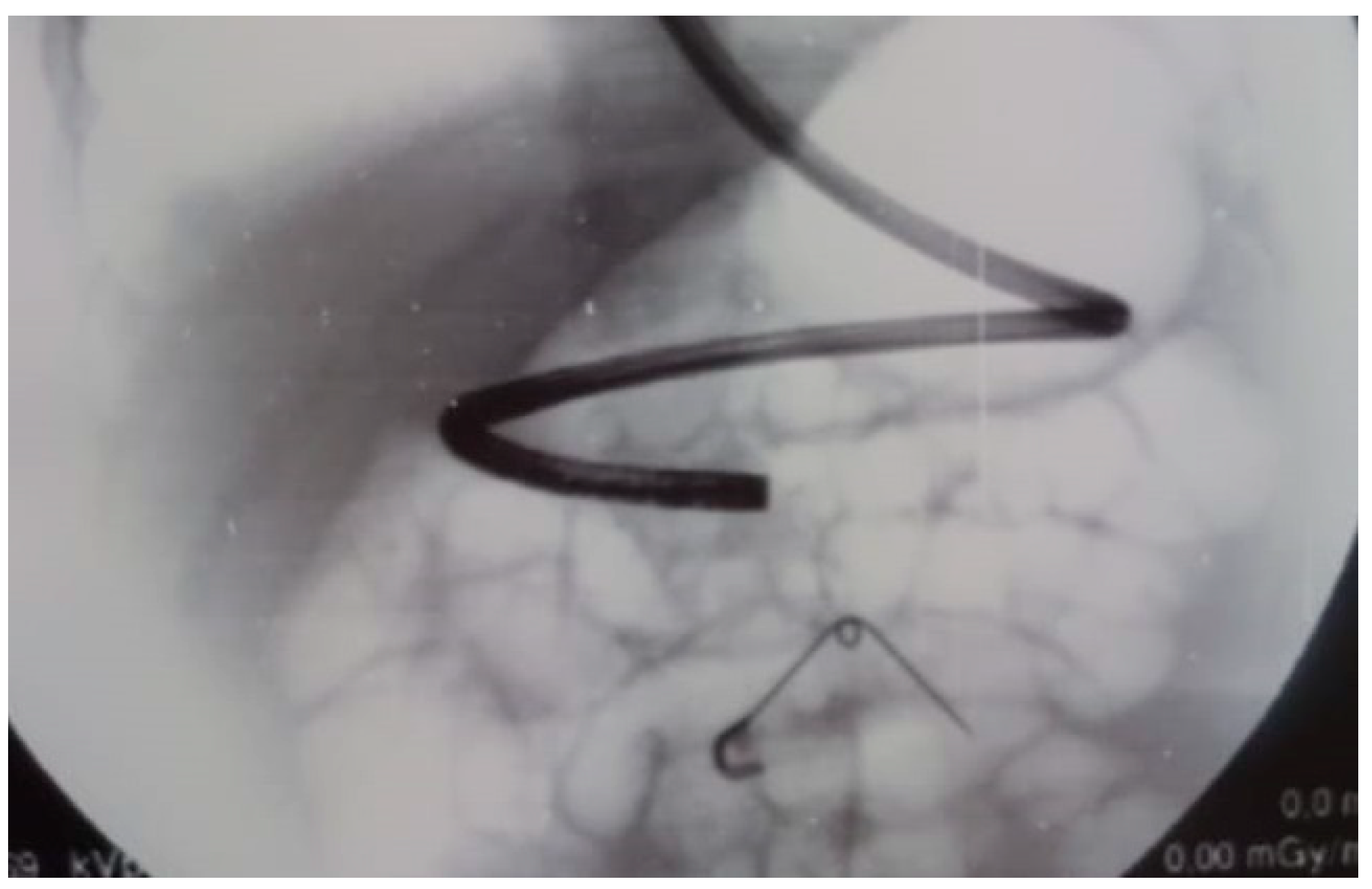
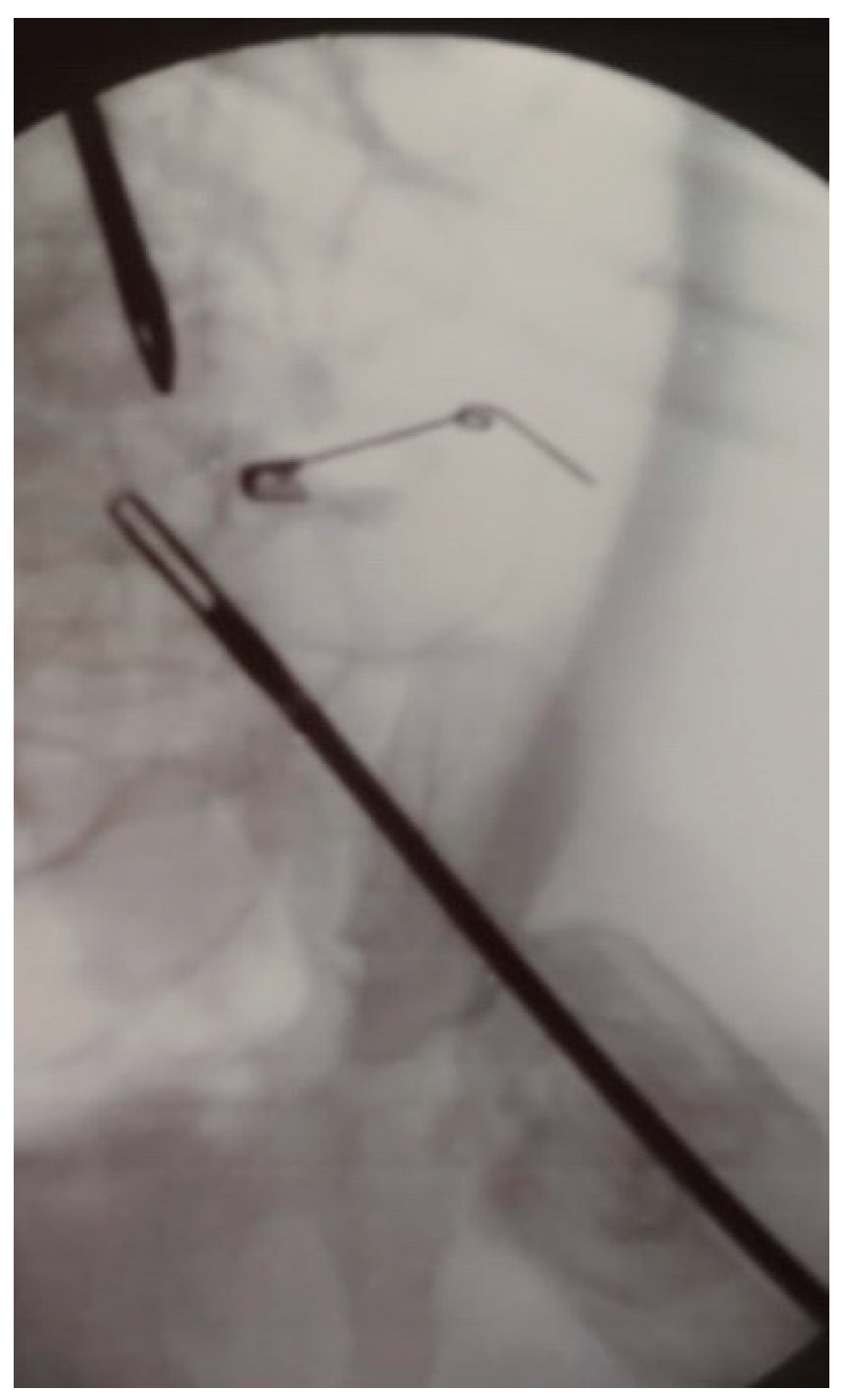
- Bisoffi, S.; Leon, F.F.; Zambaiti, E.; Sgrò, A.; Antoniello, L.M.; Gamba, P. Laparo-endoscopic combination for the safe extraction of an open safety pin in a 9-month-old child. Case report. Ann. Med. Surg. 2021, 69, 102716. [Google Scholar] [CrossRef]
- Turcu, F. The laparoscopic approach to cholecysto-choledocholithiasis.The “rendez-vous” technique. Chirurgia 2000, 95, 463–467. [Google Scholar]
- Rancan, A.; Andreetta, M.; Gaio, P.; Cananzi, M.; Rossoni, R.; La Pergola, E.; Fascetti Leon, F.; Gamba, P. “Rendezvous” Procedure in Children with Cholecysto-Choledocholithiasis. J. Laparoendosc. Adv. Surg. Tech. A 2019, 29, 1081–1084. [Google Scholar] [CrossRef]
- Cianci, P.; Restini, E. Management of cholelithiasis with choledocholithiasis: Endoscopic and surgical approaches. World J. Gastroenterol. 2021, 27, 4536–4554. [Google Scholar] [CrossRef] [PubMed]
- Pezzilli, R.; Romboli, E.; Campana, D.; Corinaldesi, R. Mechanisms involved in the onset of post-ERCP pancreatitis. JOP 2002, 3, 162–168. [Google Scholar]
- Masci, E.; Mariani, A.; Curioni, S.; Testoni, P.A. Risk factors for pancreatitis following endoscopic retrograde cholangiopancreatography: A meta-analysis. Endoscopy 2003, 35, 830–834. [Google Scholar] [CrossRef] [PubMed]
- La Greca, G.; Barbagallo, F.; Di Blasi, M.; Di Stefano, M.; Castello, G.; Gagliardo, S.; Latteri, S.; Russello, D. Rendezvous technique versus endoscopic retrograde cholangiopancreatography to treat bile duct stones reduces endoscopic time and pancreatic damage. J. Laparoendosc. Adv. Surg. Tech. A 2007, 17, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Arezzo, A.; Vettoretto, N.; Famiglietti, F.; Moja, L.; Morino, M. Laparoendoscopic rendezvous reduces perioperative morbidity and risk of pancreatitis. Surg. Endosc. 2013, 27, 1055–1060. [Google Scholar] [CrossRef]
- Iodice, G.; Giardiello, C.; Francica, G.; Sarrantonio, G.; Angelone, G.; Cristiano, S.; Finelli, R.; Tramontano, G. Single-step treatment of gallbladder and bile duct stones: A combined endoscopic-laparoscopic technique. Gastrointest. Endosc. 2001, 53, 336–338. [Google Scholar] [CrossRef]
- La Barba, G.; Gardini, A.; Cavargini, E.; Casadei, A.; Morgagni, P.; Bazzocchi, F.; D’Acapito, F.; Cavaliere, D.; Curti, R.; Tringali, D.; et al. Laparoendoscopic rendezvous in the treatment of cholecysto-choledocholitiasis: A single series of 200 patients. Surg. Endosc. 2018, 32, 3868–3873. [Google Scholar] [CrossRef] [PubMed]
- Denning, N.-L.; Kallis, M.P.; Prince, J.M. Pediatric Robotic Surgery. Surg. Clin. North Am. 2020, 100, 431–443. [Google Scholar] [CrossRef]
- Spinoglio, G.; Bertani, E.; Borin, S.; Piccioli, A.; Petz, W. Green indocyanine fluorescence in robotic abdominal surgery. Updates Surg. 2018, 70, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Boni, L.; David, G.; Mangano, A.; Dionigi, G.; Rausei, S.; Spampatti, S.; Cassinotti, E.; Fingerhut, A. Clinical applications of indocyanine green (ICG) enhanced fluorescence in laparoscopic surgery. Surg. Endosc. 2015, 29, 2046–2055. [Google Scholar] [CrossRef] [Green Version]
- Zhu, P.; Liao, W.; Ding, Z.-Y.; Luo, H.-C.; Zhang, B.-H.; Zhang, W.-G.; Zhang, W.; Zhang, Z.-G.; Zhang, B.-X.; Chen, X.-P. Intraoperative ultrasonography of robot-assisted laparoscopic hepatectomy: Initial experiences from 110 consecutive cases. Surg. Endosc. 2018, 32, 4071–4077. [Google Scholar] [CrossRef]
- Li, Q.; Li, N.; Luo, Y.; Yu, H.; Ma, X.; Zhang, X.; Tang, J. Role of intraoperative ultrasound in robotic-assisted radical nephrectomy with inferior vena cava thrombectomy in renal cell carcinoma. World J. Urol. 2020, 38, 3191–3198. [Google Scholar] [CrossRef]
- Komasara, L.; Gołębiewski, A.; Anzelewicz, S.; Czauderna, P. A review on surgical techniques and organ sparing procedures in bladder/prostate rhabdomyosarcoma. Eur. J. Pediatr. Surg. 2014, 24, 467–473. [Google Scholar] [CrossRef]
- Heinzelmann, F.; Thorwarth, D.; Lamprecht, U.; Kaulich, T.W.; Fuchs, J.; Seitz, G.; Ebinger, M.; Handgretinger, R.; Bamberg, M.; Weinmann, M. Comparison of different adjuvant radiotherapy approaches in childhood bladder/prostate rhabdomyosarcoma treated with conservative surgery. Strahlenther. Onkol. 2011, 187, 715–721. [Google Scholar] [CrossRef]
- Castagnetti, M.; Herbst, K.W.; Esposito, C. Current treatment of pediatric bladder and prostate rhabdomyosarcoma (bladder preserving vs. radical cystectomy). Curr. Opin. Urol. 2019, 29, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, J.; Paulsen, F.; Bleif, M.; Lamprecht, U.; Weidner, N.; Zips, D.; Neunhoeffer, F.; Seitz, G. Conservative surgery with combined high dose rate brachytherapy for patients suffering from genitourinary and perianal rhabdomyosarcoma. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2016, 121, 262–267. [Google Scholar] [CrossRef]
- Michel, J.; Sauter, L.; Neunhoeffer, F.; Hofbeck, M.; Kumpf, M.; Paulsen, F.; Schmidt, A.; Fuchs, J. Sedation practices during high dose rate brachytherapy for children with urogenital and perianal Rhabdomyosarcoma. J. Pediatr. Surg. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Chargari, C.; Haie-Meder, C.; Guérin, F.; Minard-Colin, V.; de Lambert, G.; Mazeron, R.; Escande, A.; Marsolat, F.; Dumas, I.; Deutsch, E.; et al. Brachytherapy Combined With Surgery for Conservative Treatment of Children With Bladder Neck and/or Prostate Rhabdomyosarcoma. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 352–359. [Google Scholar] [CrossRef]
- Martelli, H.; Borrego, P.; Guérin, F.; Boubnova, J.; Minard-Colin, V.; Dumas, I.; Chargari, C.; Haie-Meder, C. Quality of life and functional outcome of male patients with bladder-prostate rhabdomyosarcoma treated with conservative surgery and brachytherapy during childhood. Brachytherapy 2016, 15, 306–311. [Google Scholar] [CrossRef]
- Knavel, E.M.; Brace, C.L. Tumor ablation: Common modalities and general practices. Tech. Vasc. Interv. Radiol. 2013, 16, 192–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinzler, E.S.; Shivaram, G.M.; Shaw, D.W.; Monroe, E.J.; Koo, K.S.H. Microwave ablation of osteoid osteoma: Initial experience and efficacy. Pediatr. Radiol. 2019, 49, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Della Corte, A.; Ratti, F.; Monfardini, L.; Marra, P.; Gusmini, S.; Salvioni, M.; Venturini, M.; Cipriani, F.; Aldrighetti, L.; De Cobelli, F. Comparison between percutaneous and laparoscopic microwave ablation of hepatocellular carcinoma. Int. J. Hyperth. Off. J. Eur. Soc. Hyperthermic Oncol. N. Am. Hyperth. Gr. 2020, 37, 542–548. [Google Scholar] [CrossRef]
- Cui, R.; Yu, J.; Gu, Y.; Cao, F.; Liu, F.-Y.; Dong, L.-N.; Liang, P. Microwave ablation assisted by three-dimensional visualization system as local therapy for relapsed hepatoblastoma: A small pilot study. Abdom. Radiol. 2019, 44, 2909–2915. [Google Scholar] [CrossRef]
- Borghi, E.; Tognon, C.; Marchini, A.; Virgone, C.; Cillo, U.; Gamba, P. Videolaparoscopic MicroWave Ablation: An innovative technique to treat pancreatoblastoma liver metastases in children. J. Pediatr. Surg. Case Rep. 2021, 69, 101876. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pulvirenti, R.; Tognon, C.; Bisoffi, S.; Ghidini, F.; De Corti, F.; Fascetti Leon, F.; Antoniello, L.M.; Gamba, P. Innovative Techniques Associated with Traditional Abdominal Surgery in Complex Pediatric Cases: A Tertiary Center Experience. Children 2021, 8, 898. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100898
Pulvirenti R, Tognon C, Bisoffi S, Ghidini F, De Corti F, Fascetti Leon F, Antoniello LM, Gamba P. Innovative Techniques Associated with Traditional Abdominal Surgery in Complex Pediatric Cases: A Tertiary Center Experience. Children. 2021; 8(10):898. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100898
Chicago/Turabian StylePulvirenti, Rebecca, Costanza Tognon, Silvia Bisoffi, Filippo Ghidini, Federica De Corti, Francesco Fascetti Leon, Luca Maria Antoniello, and Piergiorgio Gamba. 2021. "Innovative Techniques Associated with Traditional Abdominal Surgery in Complex Pediatric Cases: A Tertiary Center Experience" Children 8, no. 10: 898. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100898