
Effects of Ankle Foot Orthoses on the Gait Patterns in Children with Spastic Bilateral Cerebral Palsy: A Scoping Review

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.2.1. Eligibility Criteria
2.2.2. Study Selection
2.3. Methodological Quality (Risk of Bias)
2.4. Data Extraction
3. Results
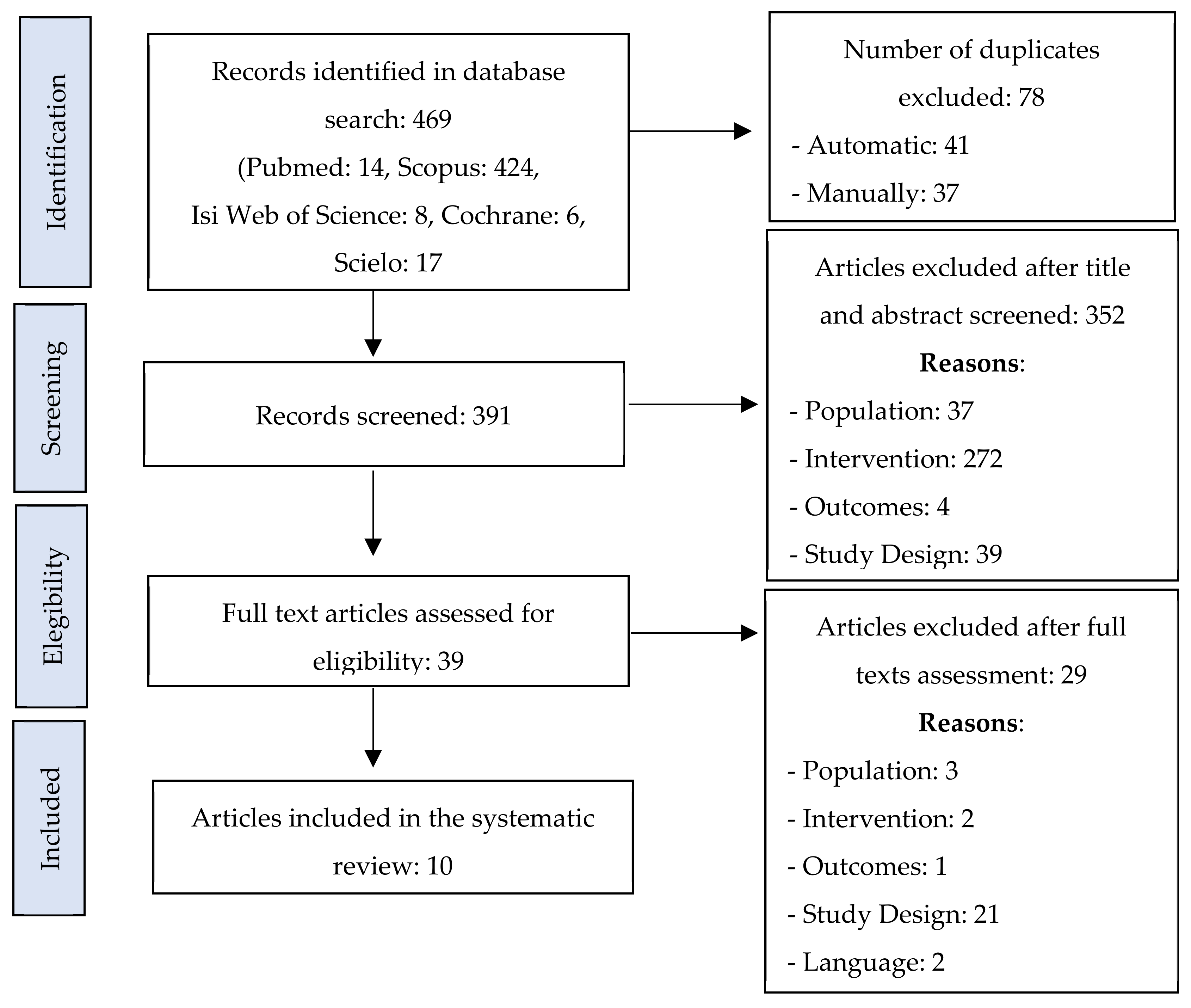
3.1. Article Selection
3.2. Article Characteristics
3.2.1. Characteristics of the Participants (Sagittal Gait Patterns)
3.2.2. Types of AFO
3.2.3. Type of Outcomes
Spatial-Temporal Parameters
Kinematic Outcomes
Kinetic Outcomes
Functional Outcomes
4. Discussion
Methodological Considerations of This Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
PICO Question Key Words
- “cerebral palsy” [mh]
- child *[mh]
- adolescent
- #1–#3
- “sagittal gait patterns”
- “spastic diplegia”
- “true equinus”
- “jump gait”
- “apparent equinus”
- “crouch gait”
- “asymmetric gait”
- #5–#11
- “ankle foot orthoses”
- AFO
- “orthotic devices” [mh]
- “foot orthoses” [mh]
- splints [mh]
- #12–#17
- gait [mh]
- walking [mh]
- kinematics [mh]
- kinetics [mh]
- “spatiotemporal analysis”
- functionality
- “functional activities”
- ICF
- “gross motor function measure”
- #19–#27
- “randomised controlled trial” [pt]
- “controlled clinical trial” [pt]
- “clinical trial” [pt]
- “comparative study” [pt]
- #29–#32
- #1–#3 AND #5–#11 AND #12–#17 AND #19–#27 AND #29–#32

{kind=link}
| Date | Source | Search Question | Nº of Results | Notes |
|---|---|---|---|---|
| 13 January 2020 | Pubmed | #1 | 14 | |
| 27 January 2020 | Scopus | #2 | 363 | |
| 27 January 2020 | Isi Web of Science | #1 | 8 | No filter |
| 27 January 2020 | Scielo | #3 | 17 | No filter |
| 27 January 2020 | Cochrane | #1 | 6 |
References
- Rosenbaum, P. Definition and Clinical Classification. In Cerebral Palsy: Science and Clinical Practice, 1st ed.; Dan, B., Mayston, M., Paneth, N., Rosenbloom, L., Eds.; Mac Keith Press: London, UK, 2014; pp. 17–26. [Google Scholar]
- Graham, H.; Rosenbaum, P.; Paneth, N.; Dan, B.; Lin, J.-P.; Damiano, D.; Becher, J.; Gaebler-Spira, D.; Colver, A.; Reddihough, D.; et al. Cerebral palsy. Nat. Rev. Dis. Prim. 2016, 2, 15082. [Google Scholar] [CrossRef]
- Eunson, P. Aetiology and epidemiology of cerebral palsy. Paediatr. Child Health 2016, 26, 367–372. [Google Scholar] [CrossRef]
- Blair, E.; Cans, C.; Sellier, E. Epidemiology of the Cerebral Palsies. In Cerebral Palsy: A Multidisciplinary Approach, 3rd ed.; Panteliadis, C., Ed.; Springer International Publishing AG: Cham, Switzerland, 2018; pp. 19–28. [Google Scholar] [CrossRef]
- Colver, A.; Fairhurst, C.; Pharoah, P. Cerebral palsy. Lancet 2014, 383, 1240–1249. [Google Scholar] [CrossRef]
- Maenner, M.; Blumberg, S.; Kogan, M.; Christensen, D.; Yeargin-Allsopp, M.; Schieve, L. Prevalence of cerebral palsy and intellectual disability among children identified in two U.S. National Surveys, 2011–2013. Ann. Epidemiol. 2016, 26, 222–226. [Google Scholar] [CrossRef] [Green Version]
- Hoffer, M.; Perry, J. Pathodynamics of Gait Alterations in Cerebral Palsy and the Significance of Kinetic Electromyography in Evaluating Foot and Ankle Problems. Foot Ankle Int. 1983, 4, 128–134. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M. The Definition and Classification of Cerebral Palsy. Dev. Med. Child Neurol. 2007, 49, 3–7. [Google Scholar]
- Dobson, F.; Morris, M.; Baker, R.; Graham, H. Gait classification in children with cerebral palsy: A systematic review. Gait Posture 2007, 25, 140–152. [Google Scholar] [CrossRef]
- Papageorgiou, E.; Nieuwenhuys, A.; Vandekerckhove, I.; van Campenhout, A. Gait & Posture Systematic review on gait classifications in children with cerebral palsy: An update. Gait Posture 2019, 69, 209–223. [Google Scholar] [CrossRef]
- Rodda, J.; Graham, H.; Carson, L.; Galea, M.; Wolfe, R. Sagittal gait patterns in spastic diplegia. J. Bone Jt. Surg.—Ser. B 2004, 86, 251–258. [Google Scholar] [CrossRef]
- Danino, B.; Erel, S.; Kfir, M.; Khamis, S.; Batt, R.; Hemo, Y.; Wientroub, S.; Hayek, S. Are Gait Indices Sensitive Enough to Reflect the Effect of Ankle Foot Orthosis on Gait Impairment in Cerebral Palsy. J. Pediatr. Orthop. 2016, 36, 294–298. [Google Scholar] [CrossRef]
- Davids, J.; Rowan, F.; Davis, R. Indications for orthoses to improve gait in children with cerebral palsy. J. Am. Acad. Orthop. Surg. 2007, 15, 178–188. [Google Scholar] [CrossRef]
- Eddison, N.; Chockalingam, N. The effect of tuning ankle foot orthoses-footwear combination on the gait parameters of children with cerebral palsy. Prosthet. Orthot. Int. 2012, 37, 95–107. [Google Scholar] [CrossRef]
- El-Kafy, E. The clinical impact of orthotic correction of lower limb rotational deformities in children with cerebral palsy: A randomized controlled trial. Clin. Rehabil. 2014, 28, 1004–1014. [Google Scholar] [CrossRef]
- Ries, A.; Schwartz, M. Ground reaction and solid ankle-foot orthoses are equivalent for the correction of crouch gait in children with cerebral palsy. Dev. Med. Child Neurol. 2018, 61, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Chui, K.; Jorge, M.; Yen, S.; Lusardi, M. Orthotics and Prosthetics in Rehabilitation, 4th ed.; Saunders Elsevier: St. Louis, MO, USA, 2020. [Google Scholar]
- Winters, T.; Gage, J.; Hicks, R. Gait patterns in spastic hemiplegia in children and young adults. J. Bone Jt. Surg. 1987, 69, 437–441. [Google Scholar]
- Vasiliauskaite, E.; Ielapi, A.; Beule, M.; Paepegem, W.; Deckers, J.; Vermandel, M.; Forward, M.; Vasiliauskaite, E.; Ielapi, A.; Beule, M.; et al. Disability and Rehabilitation: Assistive Technology A study on the efficacy of AFO stiffness prescriptions. Disabil. Rehabil. Assist. Technol. 2019, 16, 27–39. [Google Scholar] [CrossRef]
- Butler, P.; Thompson, N.; Major, R. Improvement in walking performance of chindren with cerebral palsy: Preliminary results. Dev. Med. Child Neurol. 1992, 34, 567–576. [Google Scholar] [CrossRef]
- Aboutorabi, A.; Arazpour, M.; Bani, M.A.; Saeedi, H.; Head, J. Efficacy of ankle foot orthoses types on walking in children with cerebral palsy: A systematic review. Ann. Phys. Rehabil. Med. 2017, 60, 393–402. [Google Scholar] [CrossRef]
- Betancourt, J.; Eleeh, P.; Stark, S.; Jain, N. Impact of Ankle-Foot Orthosis on Gait Efficiency in Ambulatory Children with Cerebral Palsy: A Systematic Review and Meta-analysis. Am. J. Phys. Med. Rehabil. 2019, 98, 759–770. [Google Scholar] [CrossRef]
- Lintanf, M.; Bourseul, J.; Houx, L.; Lempereur, M.; Brochard, S.; Pons, C. Effect of ankle-foot orthoses on gait, balance and gross motor function in children with cerebral palsy: A systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 1175–1188. [Google Scholar] [CrossRef]
- Firouzeh, P.; Sonnenberg, L.; Morris, C.; Pritchard-Wiart, L. Ankle foot orthoses for young children with cerebral palsy: A scoping review. Disabil. Rehabil. 2021, 43, 726–738. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.; Owens, T.; Keitz, S.; Fontelo, P. BMC Medical Informatics and Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Henderson, L.; Craig, J.; Willis, N.; Tovey, D.; Webster, A. How to write a Cochrane systematic review. Clin. Res. Nephrol. 2010, 15, 617–624. [Google Scholar] [CrossRef]
- Ayyangar, R. Health maintenance and management in childhood disability. Phys. Med. Rehabil. Clin. N. Am. 2002, 13, 793–821. [Google Scholar] [CrossRef]
- Verhagen, A.; Vet, H.; Bie, R.; Alphons, G. The Delphi List: A Criteria List for Quality Assessment of Randomized Clinical Trials for Conducting Systematic Reviews Developed by Delphi Consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef] [Green Version]
- Armijo-olivo, S.; Costa, B.; Cummings, G.; Ha, C.; Fuentes, J.; Saltaji, H.; Egger, M. PEDro or Cochrane to Assess the Quality of Clinical Trials? A Meta-Epidemiological Study. PLoS ONE 2015, 10, e0132634. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Xiao, N.; Li, H.; Du, S. Day vs. day-night use of ankle-foot orthoses in young children with spastic diplegia: A randomized controlled study. Am. J. Phys. Med. Rehabil. 2013, 92, 905–911. [Google Scholar] [CrossRef]
- Bjornson, K.; Schmale, G.A.; Adamczyk-Foster, A.; McLaughlin, J. The effect of ankle foot orthoses on mechanical energy in children with cerebral palsy. J. Pediatr. Orthop. 2006, 26, 773–776. [Google Scholar] [CrossRef]
- Bjornson, K.; Zhou, C.; Fatone, S.; Orendurff, M.; Stevenson, R.; Rashid, S. The effect of ankle-foot orthoses on community-based walking in cerebral palsy: A clinical pilot study. Pediatr. Phys. Ther. 2016, 28, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Buckon, C.; Thomas, S.; Jakobson-huston, S.; Moor, M.; Sussman, M.; Aiona, M. Comparison of three ankle—Foot orthosis configurations for children with spastic diplegia. Dev. Med. Child Neurol. 2004, 46, 590–598. [Google Scholar] [CrossRef]
- Degelean, M.; de Borre, L.; Salvia, P.; Pelc, K.; Kerckhofs, E.; de Meirleir, L.; Cheron, G.; Dan, B. Effect of ankle-foot orthoses on trunk sway and lower limb intersegmental coordination in children with bilateral cerebral palsy. J. Pediatr. Rehabil. Med. 2012, 5, 171–179. [Google Scholar] [CrossRef]
- Lam, W.; Leong, J.; Li, Y.; Hu, Y.; Lu, W. Biomechanical and electromyographic evaluation of ankle foot orthosis and dynamic ankle foot orthosis in spastic cerebral palsy. Gait Posture 2005, 22, 189–197. [Google Scholar] [CrossRef]
- Radtka, S.; Skinner, S.; Johanson, M. A comparison of gait with solid and hinged ankle-foot orthoses in children with spastic diplegic cerebral palsy. Gait Posture 2005, 21, 303–310. [Google Scholar] [CrossRef]
- Radtka, S.; Skinner, S.; Dixon, D.; Johanson, M. A comparison of gait with solid, dynamic, and no ankle-foot orthoses in children with spastic cerebral palsy. Phys. Ther. 1997, 77, 395–409. [Google Scholar] [CrossRef] [Green Version]
- Smith, P.; Hassani, S.; Graf, A.; Flanagan, A.; Reiners, K.; Kuo, K.N.; Roh, J.-Y.; Harris, G.F. Brace evaluation in children with diplegic cerebral palsy with a jump gait pattern. J. Bone Jt. Surg. Am. 2009, 91, 356–365. [Google Scholar] [CrossRef]
- Han, T.; Gray, N.; Vasquez, M.; Zou, L.; Shen, K.; Duncan, B. Comparison of the GMFM-66 and the PEDI Functional Skills Mobility domain in a group of Chinese children with cerebral palsy. Child Care. Health Dev. 2011, 37, 398–403. [Google Scholar] [CrossRef]
- Wright, E.; Dibello, S. Principles of Ankle-Foot Orthosis Prescription in Ambulatory Bilateral Cerebral Palsy. Phys. Med. Rehabil. Clin. N. Am. 2020, 31, 69–89. [Google Scholar] [CrossRef]
- Ries, A.; Novacheck, T.; Schwartz, M. The Efficacy of Ankle-Foot Orthoses on Improving the Gait of Children With Diplegic Cerebral Palsy: A Multiple Outcome Analysis. PM&R 2015, 7, 922–929. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley-Black Well: Hoboken, NJ, USA, 2019. [Google Scholar]
- Russell, D.; Rosenbaum, P.; Cadman, D.; Gowland, C.; Hardy, S.; Jarvis, S. The gross motor function measure: A means to evaluate the effects of physical therapy. Dev. Med. Child Neurol. 1989, 31, 341–352. [Google Scholar] [CrossRef]
- Guyatt, G.; Rennie, D.; Meade, M.; Cook, D. Users’ Guides to the Medical Literature, 3rd ed.; McGraw Hill Education: New York, NY, USA, 2015. [Google Scholar] [CrossRef]
- Rasmussen, H.; Pedersen, N.; Overgaard, S.; Hansen, L. Gait analysis for individually tailored interdisciplinary interventions in children with cerebral palsy: A randomized controlled trial. Dev. Med. Child Neurol. 2019, 61, 1189–1195. [Google Scholar] [CrossRef]
- Rasmussen, H.; Pedersen, N.; Overgaard, S.; Hansen, L.; Dunkhase-heinl, U.; Petkov, Y.; Engell, V.; Baker, R.; Holsgaard-larsen, A. The use of instrumented gait analysis for individually tailored interdisciplinary interventions in children with cerebral palsy: A randomised controlled trial protocol. BMC Pediatr. 2015, 15, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerkum, Y.; Houdijk, H.; Brehm, M.; Buizer, A.; Kessels, M.; Sterk, A.; van den Noort, J.; Harlaar, J. The Shank-to-Vertical-Angle as a parameter to evaluate tuning of Ankle-Foot Orthoses. Gait Posture 2015, 42, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Evans, S. Clinical trial structures. J. Exp. Stroke Transl. Med. 2010, 3, 8–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerkum, Y.; Buizer, A.; van den Noort, J.; Becher, J.; Harlaar, J.; Brehm, M. The effects of varying ankle foot orthosis stiffness on gait in children with spastic cerebral palsy who walk with excessive knee flexion. PLoS ONE 2015, 10, e0142878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eddison, N.; Mulholland, M.; Chockalingam, N. Do research papers provide enough information on design and material used in ankle foot orthoses for children with cerebral palsy? A systematic review. J. Child Orthop. 2017, 11, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Kerkum, Y.; Harlaar, J.; Buizer, A.; van den Noort, J.; Becher, J.; Brehm, M. An individual approach for optimizing ankle-foot orthoses to improve mobility in children with spastic cerebral palsy walking with excessive knee flexion. Gait Posture 2016, 46, 104–111. [Google Scholar] [CrossRef]
- Eddison, N.; Healy, A.; Needham, R.; Chockalingam, N. The effect of tuning ankle foot orthoses-footwear combinations on gait kinematics of children with cerebral palsy: A case series. Foot 2020, 43, 101660. [Google Scholar] [CrossRef]
- Almoajil, H.; Wilson, N.; Theologis, T.; Hopewell, S.; Toye, F.; Dawes, H. Outcome domains and measures after lower limb orthopaedic surgery for ambulant children with cerebral palsy: An updated scoping review. Dev. Med. Child Neurol. 2020, 62, 1138–1146. [Google Scholar] [CrossRef]
- Daryabor, A.; Arazpour, M.; Aminian, G. Effect of different designs of ankle-foot orthoses on gait in patients with stroke: A systematic review. Gait Posture 2018, 62, 268–279. [Google Scholar] [CrossRef]
- McGinley, J.; Baker, R.; Wolfe, R.; Morris, M. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef]
- Monaghan, K.; Delahunt, E.; Caulfield, B. Increasing the number of gait trial recordings maximises intra-rater reliability of the CODA motion analysis system. Gait Posture 2007, 25, 303–315. [Google Scholar] [CrossRef] [PubMed]
- Stief, F. Variations of Marker Sets and Models for Standard Gait Analysis. In Handbook of Human Motion, 1st ed.; Müller, B., Wolf, S., Eds.; Springer International Publishing AG: Cham, Switzerland, 2018; pp. 509–523. [Google Scholar]
- Steinwender, G.; Saraph, V.; Scheiber, S.; Zwick, E.; Uitz, C.; Hackl, K. Intrasubject repeatability of gait analysis data in normal and spastic children. Clin. Biomech. 2000, 15, 134–139. [Google Scholar] [CrossRef]
- Ricardo, D.; Teles, J.; Raposo, M.R.; Veloso, A.P.; João, F. Test-Retest Reliability of a 6DoF Marker Set for Gait Analysis in Cerebral Palsy Children. Appl. Sci. 2021, 11, 6515. [Google Scholar] [CrossRef]
- Danino, B.; Erel, S.; Kfir, M.; Khamis, S.; Batt, R.; Hemo, Y.; Wientroub, S.; Hayek, S. Influence of orthosis on the foot progression angle in children with spastic cerebral palsy. Gait Posture 2015, 42, 518–522. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF. 2001. Available online: https://apps.who.int/iris/handle/10665/42407 (accessed on 5 March 2020).
- Limsakul, C.; Noten, S.; Selb, M.; Stam, H.; van der Slot, W.; Roebroeck, M. Developing an ICF Core Set for adults with cerebral palsy: A Global expert survey of relevant functions and contextual factors. J. Rehabil. Med. 2020, 52, 1–9. [Google Scholar] [CrossRef] [Green Version]

| Authors | Year | Study Design | Population Characteristics | Eligibility Criteria | N | Duration | Intervention/Procedure | Variables | Measurement Instruments | Main Results and Author’s Conclusions |
|---|---|---|---|---|---|---|---|---|---|---|
| Bjornson, 2006 [31] | 2006 | Randomized crossover controlled trial | 23 children with spastic CP (age: 4.3 ± 1.5 years) | Children with spastic diplegia CP, 12 to 96 months, GMFCS I to III, bilateral use of AFO with free plantarflexion. | 23 | 1 day | DAFO and shoes. GMFM used once with/without the orthoses during a same day evaluation. | Functional skills (GMFM scores). | GMFM. | The GMFM percentage scores for all dimensions were significantly higher with the patients wearing the DAFO (p ˂ 0.001). There seems to be a non-significant negative correlation of age to standing skills change, suggesting that DAFO effect may decrease with age, up to the age of approximately 7 years (p ˂ 0.001). |
| Bjornson, 2016 [32] | 2016 | Randomized crossover controlled trial | 11 children with spastic CP (age: 4.3 ± 1.04 years) | Children with spastic diplegia CP; GMFCS I to III; bilateral use of AFO > 8 h/day, >1 month. | 11 | 4 weeks (2 weeks without AFO and 2 weeks with AFO) | SAFO and shoes. Community based walking with/without AFO with a multiaxis accelerometer. | Functional skills (average total strides per day; % daytime hours walking; average number strides >30 strides/min; peak activity index). | StepWatch (Ankle accelerometer). | No significant difference was found in the primary outcome of average daily total step count between AFO-ON and AFO-OFF (p = 0.48). AFO did not improve walking activity levels. |
| Buckon, 2004 [33] | 2004 | Randomized crossover controlled trial | 16 children with spastic CP (age: 8.3 ± 2.3 years) | Children with spastic diplegia CP; GMFCS I to II; bilateral use of AFO, 6 to 12 h daily >3 month. | 16 | 1 year (a baseline assessment after three months of no AFO wear, and an assessment at the end of each AFO three-month wearing period | Barefoot or HAFO or PLS or SAFO. | Functional skills (GMFM scores); gait analysis data (kinematic variables at the pelvis, hip, knee, and ankle; Kinetic variables at the hip, knee, and ankle; Velocity, stride length, step length, and cadence). | Optoelectronic system; force plates; GMFM. | AFO use, regardless of configuration, did not significantly alter pelvic and hip kinematics and/or kinetics from the barefoot condition. At the knee there was no significant kinematic change. All AFO configurations significantly altered ankle kinematics during the stance and swing phases of gait: dorsiflexion at initial contact (p = 0.0001), peak dorsiflexion in stance (p < 0.009), timing of peak dorsiflexion in stance (p < 0.003), peak dorsiflexion in swing (p < 0.0002), and dynamic ankle range (p < 0.0001) compared with barefoot. Between the configurations, peak dorsiflexion in stance was significantly greater in the HAFO than the SAFO (p = 0.01), and the timing of peak dorsiflexion in stance was significantly later in the stance phase in the HAFO compared with the SAFO (p = 0.005). In conjunction with the changes in ankle kinematics, ankle kinetics (peak dorsiflexion moment in early stance [p = 0.0001], peak plantarflexion moment in early stance [p = 0.0001], peak power generation in stance [p < 0.008], and the timing of peak power generation [p < 0.005]) changed significantly in all the AFO configurations compared with barefoot. All of the AFO configurations significantly increased step (p < 0.005) and stride length (p < 0.006) compared with barefoot, while significantly decreasing cadence (p < 0.0005). Therefore, velocity did not increase significantly with AFO use compared with barefoot. Velocity was significantly slower in the HAFO compared with the PLS (p = 0.009), owing to a 17% decrease in cadence in the HAFO, an 11% decrease in the PLS, and a 13% decrease in the SAFO, compared with barefoot. AFO use did not significantly improve skills within the standing dimension of the GMFM. However, all AFO configurations significantly improved skills within the W/R/J dimension compared with the barefoot condition (p < 0.002). |
| Degelean, 2012 [34] | 2012 | Non-randomized controlled clinical trial plus healthy controls (repeated measures design) | 20 children with spastic diplegic CP (mean age: 7.6 ± 1.7 years) + 20 typically developing children (mean age: 7.8; ± 1.4 years) | Children with CP of the spastic diplegia type within the age of 4 and 12 years; no history of orthopedic surgery; no botulinum toxin injections within the last year; GMFCS level I or II; use of posterior leaf spring-type or solid AFO either in habitual walking or during physical therapy sessions. | 20 + 20 | 1 day | Spring AFO or SAFO vs. barefoot. Participants walked at a comfortable speed on an 8 m walkway with AFO and barefoot. The task was recorded using an optoelectronic system detecting passive retro-reflective markers. | Gait analysis data (trunk movements; angular velocities; peak-to-peak excursions in trunk angular displacements; elevation angles of the thigh, shank, and foot). | Optoeletronic system. | Children with CP showed greater trunk sway excursion and angular velocity in both the sagittal and frontal directions compared to the control group (p ˂ 0.05). Children with CP have greater sagittal and frontal trunk movements compared to typically developing children, but the difference in frontal motion was higher than in sagittal motion (p ˂ 0.05). The use of any of AFO improved lower limb intersegmental coordination during gait in children with spastic diplegia by making it closer to a typical, mature gait pattern (p ˂ 0.05). This was indicated by a significant greater ROM of the shank and a decreased ROM foot. However, wearing AFO results in increased trunk motion, which may be problematic in the context of difficult postural control. |
| El-Kafy, 2014 [15] | 2014 | Randomized parallel group controlled trial | 57 children with spastic diplegic (mean age: 7.3 ± 1.3 years) | Children with CP of the spastic diplegia type within the age of 6–8 years old; under 40 kg; cognitively able to understand simple instructions; no recurrent medical issues; no allergic reactions to the adhesive tape or any other materials; no visual, auditory, or perceptual deficits or seizures; no previously use of TheraTogs orthotic undergarment, or strapping system and ground reaction ankle foot orthosis; no botulinum toxin in the lower extremity musculature during the past 6 months or other spasticity medication within 3 months of pre-treatment testing. | 19 + 19 + 19 | 2 h/day, 5 days/week for a total of 12 weeks | Control group (A)—traditional neuro- developmental physical therapy. Study group (B)—A + TheraTogsTM orthotic undergarment and strapping system for both lower extremities. Study group (C)—B + received GRAFO in both lower limbs. Participants walked at a comfortable speed on an 8 m walkway with AFO and barefoot. The task was recorded using an optoelectronic system detecting passive retro-reflective markers. | Gait analysis data (gait speed; cadence; stride length; hip and knee flexion angles). | Optoeletronic system. | There were significant differences among the 3 groups pre-treatment in all measured variables (gait speed, cadence, stride length, and bilateral hip and knee flexion angles), and that they were present post-treatment (p ˂ 0.05). This is due to the improvement of the plantar flexion, knee extension coupling, and knee and hip extension angle in mid stance provided by the GRAFO. The statistically significant differences post-treatment, in all parameters, were greater in group C than that in both groups A and B (p ˂ 0.05). The results concerning the mean values of bilateral hip and knee rotational angles between both groups B and C revealed that there were no statistically significant differences in either pre- or post-treatment evaluation times (p ˂ 0.05). |
| Lam, 2005 [35] | 2005 | Non-randomized controlled clinical trial plus healthy controls (repeated measures design) | 7 boys and 6 girls with spastic diplegic CP (mean age: 5.9 ± 1.81 years) + 18 typically developing children (age matched) | Spastic diplegia CP with mainly moderate dynamic equinus (modified Ashworth scale 1–3); no significant coronal or rotational deformities; no botulinum toxin injections within the preceding 5 months; good vision; the ability to comprehend instructions; be able to walk independently. | 13 + 18 | 1 day | AFO and DAFO. Barefoot (healthy subjects control group). | Gait analysis data (stride length; stride time; speed; stance time; swing time; stance/swing ratio; cadence; range of motion parameters; moment parameters; power parameters). | Optoeletronic system; force platform. | CP patients had significantly shorter stride length than normal. Both AFO and DAFO conditions significantly increased stride length (p ˂ 0.05). The mean stride length in CP patients walking barefoot (0.69 ± 0.14) was 65% of the healthy age matched children. The stride length was significantly increased when the subjects were wearing AFO (0.74 ± 0.15) or DAFO (0.81 ± 0.15). Concerning the total ROM, there was a reduction in range of motion at the ankle joint between the barefoot (22.39 ± 6.78), AFO (12.44 ± 5.55), and DAFO (19.72 ± 4.46). At initial contact children with DAFO presented a significantly increased knee and hip flexion by 4.8° (p < 0.016) and 5.3° (p = 0.012), respectably, when compared to barefoot walking. No significant difference was found at the ROM in the knee and hip between the AFO and DAFO. There was a significantly higher ground reaction force at the second peak wearing an AFO (0.97 ± 0.06) than when walking barefoot (0.89 ± 0.11). Both the AFO (0.96 ± 0.27) and the DAFO (1.11 ± 0.43) showed a significant improvement in the maximum plantar flexion moment compared to barefoot (0.69 ± 0.25). It was 0.28 Nm/kg higher in the AFO and 0.42 Nm/kg higher in the DAFO. There was no significant difference determined among barefoot, SAFO, and DAFO in all knee and hip power parameters. |
| Radtka, 1997 [37] | 1997 | Non-randomized controlled clinical trial (repeated measures design) | 10 children with spastic CP (6 diplegic; 4 hemiplegic) (mean age: 6.5 ± 1.86 years) | Spastic diplegia and unilateral CP; community ambulatory with plantigrade foot in standing, excessive plantar flexion during the stance, passive dorsiflexion of 5 degrees or more with knee extended, passive hip extension of 10 degrees or more, passive hamstring muscle length of 60 degrees or more in straight leg raise, mild to moderate spasticity in lower limb; no use of assistive device in ambulation; no orthopedic surgery in the previous year. | 10 | 3 months (2 weeks barefoot + 1 month with AFO + 2 weeks barefoot + 1 month with DAFO) | AFO and DAFO. | Gait analysis data (walking speed; stride length; cadence; range of motion of the trunk, pelvis, hip, knee, and ankle at initial contact and mid-stance). | Contact closing foot switches; optoelectronic system. | There was an increased stride length wearing the AFO (0.97 ± 0.16) and DAFO (0.93 ± 0.13) compared with the barefoot condition (0.82 ± 0.13). The cadence was higher barefoot (148.33 ± 15.73) than with the AFO (140.10 ± 8.79) and DAFO (136.55 ± 10.96). The excessive ankle plantar flexion with no orthoses (8.54 ± 5.61) was over reduced with AFO (−2.62 ± 3.93) and DAFO (−1.66 ± 6.23). There were no differences (p < 0.002) at the level in joint motions of the knee, hip, and pelvis at initial contact and mid-stance with AFO or DAFO. The amount of ankle plantar flexion that occurred at initial contact and mid-stance in the interventions with no orthoses was reduced with both AFO and DAFO. No differences were found for the gait variables when comparing the two orthoses (p ˂ 0.02). |
| Radtka, 2005 [36] | 2005 | Non-randomized controlled clinical trial (repeated measures design) | 12 children with spastic diplegic CP (mean age: 7.5 ± 3.83 years) | Spastic diplegia CP; community ambulatory with ankle dorsiflexion to 0 degrees during static standing, excessive ankle plantar flexion of 5 degrees or more during stance in gait, passive ankle dorsiflexion to 5 degrees with knee extended passive hip extension to −10 degrees or less in the Thomas test, passive hamstring length of 50 degrees or more as measured by a straight leg raise; mild spasticity of the triceps surae, hamstrings and quadriceps; no surgical procedures in the past or any other orthopedic surgery during the year prior to the study. | 12 | 3 months (2 weeks barefoot + 1 month with AFO + 2 weeks barefoot + 1 month with HAFO) | SAFO and HAFO. | Gait analysis data (range of motion of the knee and ankle during the stance phase; walking velocity; stride length; cadence; knee and ankle sagittal joint moments and powers during the stance phase). | Optoelectronic system; force plates. | The mean stride length was increased with both SAFO (0.87 ± 0.19) and HAFO (0.90 ± 0.19) when compared to no AFO (0.79 ± 0.19). No significant differences in walking velocity, cadence, and stride length when comparing no AFO, SAFO, and HAFO (p ˂ 0.05). At the knee joint there were no findings of significant differences between barefoot, SAFO, or HAFO. When compared to the barefoot condition, at the ankle joint there were significant differences with the AFO and HAFO. The HAFO produced more normal dorsiflexion at the terminal stance phase than the SAFO, and more excessive dorsiflexion during loading phase than barefoot. There were significant differences when comparing no AFO (0.69 ± 0.14), SAFO (0.96 ± 0.22), and HAFO (0.94 ± 0.25) in the peak ankle moments. There was a significant difference in peak ankle moments during the terminal stance phase between barefoot (−1.30 ± 6.59) and SAFO (11.50 ± 4.28) and barefoot and HAFO (16.13 ± 6.17). The mean values were similar between both AFO. |
| Smith, 2009 [38] | 2009 | Non-randomized controlled clinical trial plus healthy controls (repeated measures design) | 15 children with spastic diplegic CP (mean age: 7.5 ± 2.9 years) + 20 typically developing children (mean age: 10.6 ± 2.8 years) | Spastic diplegia CP; able to walk independently without an assistive device; jump gait pattern; GMFCS level I; no orthopedic surgery in the past 12 months; no botulinum toxin injections in the past 6 months; range of ankle dorsiflexion to at least neutral on static physical examination with the knee extended. | 15 + 20 | 2.5 months (barefoot baseline + 4 weeks with DAFO or HAFO + 2 weeks barefoot + 4 weeks with DAFO or HAFO) | DAFO and HAFO. Barefoot (healthy subjects control group). | Gait analysis data (walking speed; cadence; stride length; range of motion; joint moments; joints powers); functional skills (GMFM scores). | Optoelectronic system; force plates; GMFM. | Significant improvements in gait metrics were seen during brace wear (p ≤ 0.05). When compared with barefoot condition, CP children wearing HAFO and DAFO showed a significant increase in stride length (0.98 ± 0.05) and (1.01 ± 0.05) and walking speed (1.09 ± 0.6) and (1.11 ± 0.6). When using HAFO or DAFO there was a significant decrease in normal cadence (p ≤ 0.006) compared with the children with CP in barefoot condition. When comparing gait cycles of children with CP and healthy children there was no significant difference in terms of stride length, walking speed, or cadence. At the ankle significant differences between the HAFO or DAFO and the barefoot condition were found during the stance and swing phase (p ≤ 0.05). The knee peak flexion during swing was significantly different between the DAFO and barefoot condition (p ≤ 0.05). Children with CP using HAFO or DAFO had no significant effect on hip ROM. No significant differences were seen between the two different braces used (p ≤ 0.05). The barefoot and braced conditions differed most significantly in terms of ankle kinematics and kinetics (p ≤ 0.05). During the terminal stance of pre-swing, the ankle moment was significantly increased for both DAFO (0.98 ± 0.1) and HAFO (1.05 ± 0.1) when compared to the barefoot condition (0.80 ± 0.1). When compared to healthy children, in the barefoot and AFO condition, CP children presented a significant increase in plantar flexor moment during the initial contact (p ≤ 0.05). No significant differences in ankle powers were found between DAFO and HAFO. |
| Zhao, 2013 [30] | 2013 | Randomized parallel group controlled trial | 70 boys and 42 girls with spastic diplegic CP (mean age: 2.69 ± 0.81 years) | Spastic diplegic CP; between 1 and 4 years of age; ability to walk independently, with or without an assistive device; GMFCS levels I-II; able to accept and follow AFO treatment strategy; no unstable seizures; no orthopedic surgery for spasticity within the preceding 6 months; no botulinum toxin injections within the preceding 3 months; without any other diseases that interfered with physical activity, and existence of serious cognitive disabilities. | 56 + 56 | 5 to 8 weeks | Day AFO. Night and day AFO. | Gait analysis data (passive ankle dorsiflexion angle). | Sections D and E of the 66-item GMFM. | No evidence was found that the prolonged wearing time with AFOs leads to increased benefits (p ˂ 0.05). The GMFM-66 improvement in the day-night AFO-wearing group was lower than in the day AFO-wearing group rather than higher. AFO day-night use was not more effective than daytime use alone in children with spastic diplegia at GMFCS levels I to II. |
| Article ID | PEDro Score | Total Score | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Eligibility Criteria * | Random Allocation | Blind Distribution | Similar Prognosis | Blind Subject | Blind Therapist | Blind Assessors | 85% Follow-Up | Intention to Treat | Statistical Comparisons | Point of Measure/Measures of Variability | ||
| Bjornson, 2006 [31] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | 8/10 |
| Bjornson, 2016 [32] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | No | 5/10 |
| Buckon, 2004 [33] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6/10 |
| Degelean, 2012 [34] | Yes | No | No | No | No | No | No | Yes | Yes | Yes | Yes | 4/10 |
| El-Kafy, 2014 [15] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8/10 |
| Lam, 2005 [35] | Yes | No | No | No | No | No | No | Yes | Yes | Yes | Yes | 4/10 |
| Radtka, 1997 [37] | Yes | No | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 5/10 |
| Radtka, 2005 [36] | Yes | No | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 5/10 |
| Smith, 2009 [38] | Yes | No | No | No | No | No | No | Yes | Yes | Yes | Yes | 4/10 |
| Zhao, 2013 [30] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricardo, D.; Raposo, M.R.; Cruz, E.B.; Oliveira, R.; Carnide, F.; Veloso, A.P.; João, F. Effects of Ankle Foot Orthoses on the Gait Patterns in Children with Spastic Bilateral Cerebral Palsy: A Scoping Review. Children 2021, 8, 903. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100903
Ricardo D, Raposo MR, Cruz EB, Oliveira R, Carnide F, Veloso AP, João F. Effects of Ankle Foot Orthoses on the Gait Patterns in Children with Spastic Bilateral Cerebral Palsy: A Scoping Review. Children. 2021; 8(10):903. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100903
Chicago/Turabian StyleRicardo, Diogo, Maria Raquel Raposo, Eduardo Brazete Cruz, Raul Oliveira, Filomena Carnide, António Prieto Veloso, and Filipa João. 2021. "Effects of Ankle Foot Orthoses on the Gait Patterns in Children with Spastic Bilateral Cerebral Palsy: A Scoping Review" Children 8, no. 10: 903. https://0-doi-org.brum.beds.ac.uk/10.3390/children8100903