The Association between the Concentration of Heavy Metals in the Indoor Atmosphere and Atopic Dermatitis Symptoms in Children Aged between 4 and 13 Years: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Measurement of Air Pollutant Concentration in Indoor Air
2.3. Statistical Analyses
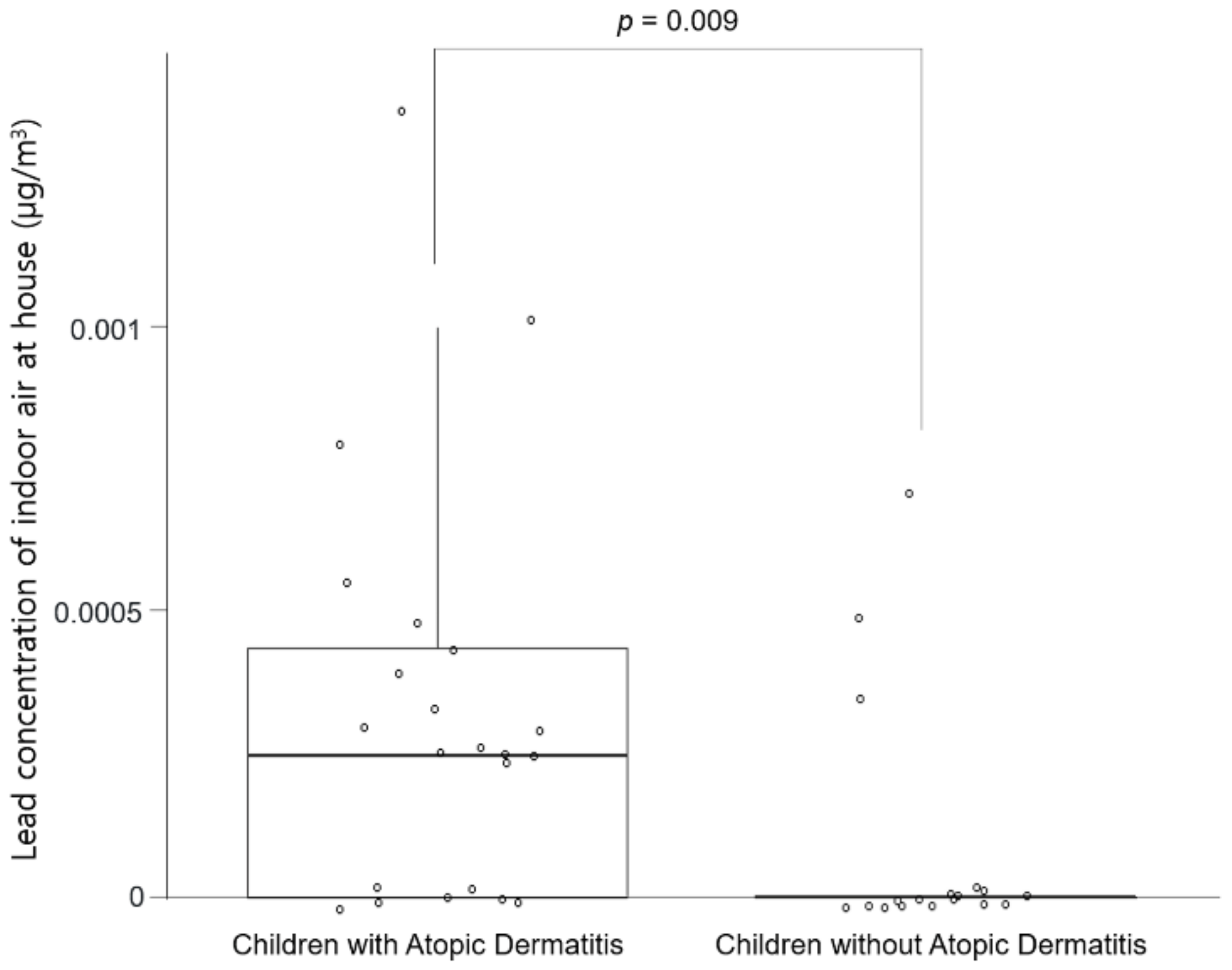
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, H.; Flohr, C. How epidemiology has challenged 3 prevailing concepts about atopic dermatitis. J. Allergy Clin. Immunol. 2006, 118, 209–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, K. The role of air pollutants in atopic dermatitis. J. Allergy Clin. Immunol. 2014, 134, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Gass, K.; Balachandran, S.; Chang, H.H.; Russell, A.G.; Strickland, M.J. Ensemble-Based Source Apportionment of Fine Particulate Matter and Emergency Department Visits for Pediatric Asthma. Am. J. Epidemiol. 2015, 181, 504–512. [Google Scholar] [CrossRef] [Green Version]
- Hasunuma, H.; Ishimaru, Y.; Yoda, Y.; Shima, M. Decline of ambient air pollution levels due to measures to control automobile emissions and effects on the prevalence of respiratory and allergic disorders among children in Japan. Environ. Res. 2014, 131, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Penard-Morand, C.; Raherison, C.; Charpin, D.; Kopferschmitt, C.; Lavaud, F.; Caillaud, D.; Annesi-Maesano, I. Long-term exposure to close-proximity air pollution and asthma and allergies in urban children. Eur. Respir. J. 2010, 36, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Morgenstern, V.; Zutavern, A.; Cyrys, J.; Brockow, I.; Koletzko, S.; Krämer, U.; Behrendt, H.; Herbarth, O.; Von Berg, A.; Bauer, C.P.; et al. Atopic Diseases, Allergic Sensitization, and Exposure to Traffic-related Air Pollution in Children. Am. J. Respir. Crit. Care Med. 2008, 177, 1331–1337. [Google Scholar] [CrossRef]
- Kim, J.; Kim, E.-H.; Oh, I.; Jung, K.; Han, Y.; Cheong, H.-K.; Ahn, K. Symptoms of atopic dermatitis are influenced by outdoor air pollution. J. Allergy Clin. Immunol. 2013, 132, 495–498.e1. [Google Scholar] [CrossRef]
- Kim, J.H.; Jeong, K.S.; Ha, E.-H.; Park, H.; Ha, M.; Hong, Y.-C.; Lee, S.-J.; Lee, K.Y.; Jeong, J.; Kim, Y. Association between Prenatal Exposure to Cadmium and Atopic Dermatitis in Infancy. J. Korean Med. Sci. 2013, 28, 516–521. [Google Scholar] [CrossRef] [Green Version]
- Leung, T.F.; Chan, I.H.; Liu, T.C.; Lam, C.W.; Wong, G.W. Relationship between passive smoking exposure and urinary heavy metals and lung functions in preschool children. Pediatr. Pulmonol. 2013, 48, 1089–1097. [Google Scholar] [CrossRef]
- Hanifin, J.M.; Rajka, G. Diagnostic features of atopic dermatitis. Acta Derm. Venereol. (Stockh) 1980, 92, 44–47. [Google Scholar] [CrossRef]
- Lidsky, T.I.; Schneider, J.S. Lead neurotoxicity in children: Basic mechanisms and clinical correlates. Brain 2003, 126, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Manton, W.; Angle, C.; Stanek, K.; Kuntzelman, D.; Reese, Y.; Kuehnemann, T. Release of lead from bone in pregnancy and lactation. Environ. Res. 2003, 92, 139–151. [Google Scholar] [CrossRef]
- Lee, S.; Park, S.K.; Park, H.; Lee, W.; Kwon, J.H.; Hong, Y.-C.; Ha, M.; Kim, Y.; Lee, B.; Ha, E. Prenatal heavy metal exposures and atopic dermatitis with gender difference in 6-month-old infants using multipollutant analysis. Environ. Res. 2021, 195, 110865. [Google Scholar] [CrossRef] [PubMed]
- Dietert, R.R.; Zelikoff, J.T. Early-life environment, developmental immunotoxicology, and the risk of pediatric allergic disease including asthma. Birth Defects Res. Part B Dev. Reprod. Toxicol. 2008, 83, 547–560. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Perera, F.; Maugeri, U.; Miller, R.L.; Rembiasz, M.; Flak, E.; Mroz, E.; Majewska, R.; Zembala, M. Intrauterine exposure to lead may enhance sensitization to common inhalant allergens in early childhood: A prospective prebirth cohort study. Environ. Res. 2011, 111, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hon, K.-L.E.; Wang, S.S.; Hung, E.C.W.; Lam, H.S.; Lui, H.H.K.; Chow, C.-M.; Ching, G.K.W.; Fok, T.-F.; Ng, P.-C.; Leung, T.-F. Serum levels of heavy metals in childhood eczema and skin diseases: Friends or foes. Pediatr. Allergy Immunol. 2010, 21, 831–836. [Google Scholar] [CrossRef]
- World Health Organization. Air Quality Guidelines for Europe, 2nd ed.; WHO Regional Office for Europe: Geneva, Switzerland, 2000; Volume (91)V-X, pp. 1–273. [Google Scholar]
- Böhme, M.; Kull, I.; Bergström, A.; Wickman, M.; Nordvall, L.; Pershagen, G.; Wahlgren, C.-F. Parental smoking increases the risk for eczema with sensitization in 4-year-old children. J. Allergy Clin. Immunol. 2010, 125, 941–943. [Google Scholar] [CrossRef] [PubMed]
- Yi, O.; Kwon, H.-J.; Kim, H.; Ha, M.; Hong, S.-J.; Hong, Y.-C.; Leem, J.-H.; Sakong, J.; Lee, C.G.; Kim, S.-Y.; et al. Effect of environmental tobacco smoke on atopic dermatitis among children in Korea. Environ. Res. 2012, 113, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Mannino, D.M.; Albalak, R.; Grosse, S.; Repace, J. Second-hand Smoke Exposure and Blood Lead Levels in U.S. Children. Epidemiology 2003, 14, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Ukawa, S.; Araki, A.; Kanazawa, A.; Yuasa, M.; Kishi, R. The relationship between atopic dermatitis and indoor environmental factors: A cross-sectional study among Japanese elementary school children. Int. Arch. Occup. Environ. Health 2012, 86, 777–787. [Google Scholar] [CrossRef]
- Bonino, S. Carbon Dioxide Detection and Indoor Air Quality Control. Occup. Health Saf. 2016, 85, 46–48. [Google Scholar]


{kind=link}
| Variables | Home with AD (n = 22) | Home without AD (n = 18) | p-Value |
|---|---|---|---|
| Sex (boy/girl) $ | 16/6 | 9/9 | 0.194 |
| Age (years) # | 7 (5–11) | 7 (5–11) | 0.946 |
| Temperature (℃) | 25.4 ± 1.0 | 24.9 ± 1.0 | 0.121 |
| Humidity (%) * | 74.8 ± 2.9 | 76.3 ± 2.4 | 0.099 |
| PM10 (µg/m3) # | 25.7 (24.3–32.2) | 25.2 (22.5–27.1) | 0.155 |
| CO2(ppm) # | 534.5 (455.4–637.6) | 447.5 (386.5–563.5) | 0.925 |
| CO (ppm) # | 0.100 (0.100–0.100) | 0.100 (0.100–0.113) | 0.904 |
| NO2 (ppm) # | 0.109 (0.083–0.145) | 0.103 (0.082–0.163) | 0.925 |
| VOCs (µg/m3) * | 227.3 ± 102.6 | 200.3 ± 55.8 | 0.005 |
| Bacterial aerosol * (CFU/m3) | 502.6 ± 240.3 | 437.4 ± 173.6 | 0.341 |
| Mold (CFU/m3) * | 59.4 ± 26.6 | 45.5 ± 20.1 | 0.078 |
| Ozone (ppm) * | 0.17 ± 0.01 | 0.17 ± 0.01 | 0.906 |
| Radon (pCi/L) # | 0.200 (0.175–0.300) | 0.200 (0.138–0.250) | 0.527 |
| Formaldehyde * (µg/m3) * | 31.4 ± 17.2 | 27.9 ± 16.5 | 0.530 |
| p-Value | ||
|---|---|---|
| Variables | Unadjusted | Adjusted # |
| PM10 (µg/m3) | 0.098 * | 0.249 |
| CO2 (ppm) | 0.276 | - |
| CO (ppm) | 0.915 | - |
| NO2 (ppm) | 0.056 * | 0.981 |
| VOCs (µg/m3) | 0.014 ** | 0.038 ** |
| Bacterial aerosol (CFU/m3) | 0.334 | - |
| Mold (CFU/m3) | 0.083 * | 0.566 |
| Ozone (ppm) | 0.653 | - |
| Radon (pCi/L) | 0.274 | - |
| Formaldehyde (µg/m3) | 0.522 | - |
| Lead (µg/m3) | 0.028 ** | 0.035 ** |
| Cadmium (µg/m3) | 0.234 | - |
| Mercury (µg/m3) | 0.278 | - |
| Temperature (℃) | 0.125 | |
| Humidity (%) | 0.103 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.S.; Suh, M.J.; Hong, S.C.; Kang, J.W. The Association between the Concentration of Heavy Metals in the Indoor Atmosphere and Atopic Dermatitis Symptoms in Children Aged between 4 and 13 Years: A Pilot Study. Children 2021, 8, 1004. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111004
Choi HS, Suh MJ, Hong SC, Kang JW. The Association between the Concentration of Heavy Metals in the Indoor Atmosphere and Atopic Dermatitis Symptoms in Children Aged between 4 and 13 Years: A Pilot Study. Children. 2021; 8(11):1004. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111004
Chicago/Turabian StyleChoi, Hyun Seung, Michelle J. Suh, Sung Chul Hong, and Ju Wan Kang. 2021. "The Association between the Concentration of Heavy Metals in the Indoor Atmosphere and Atopic Dermatitis Symptoms in Children Aged between 4 and 13 Years: A Pilot Study" Children 8, no. 11: 1004. https://0-doi-org.brum.beds.ac.uk/10.3390/children8111004