Neuropsychological Development and New Criteria for Extrauterine Growth Restriction in Very Low-Birth-Weight Children

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Description of the Growth of 87 Cases Studied
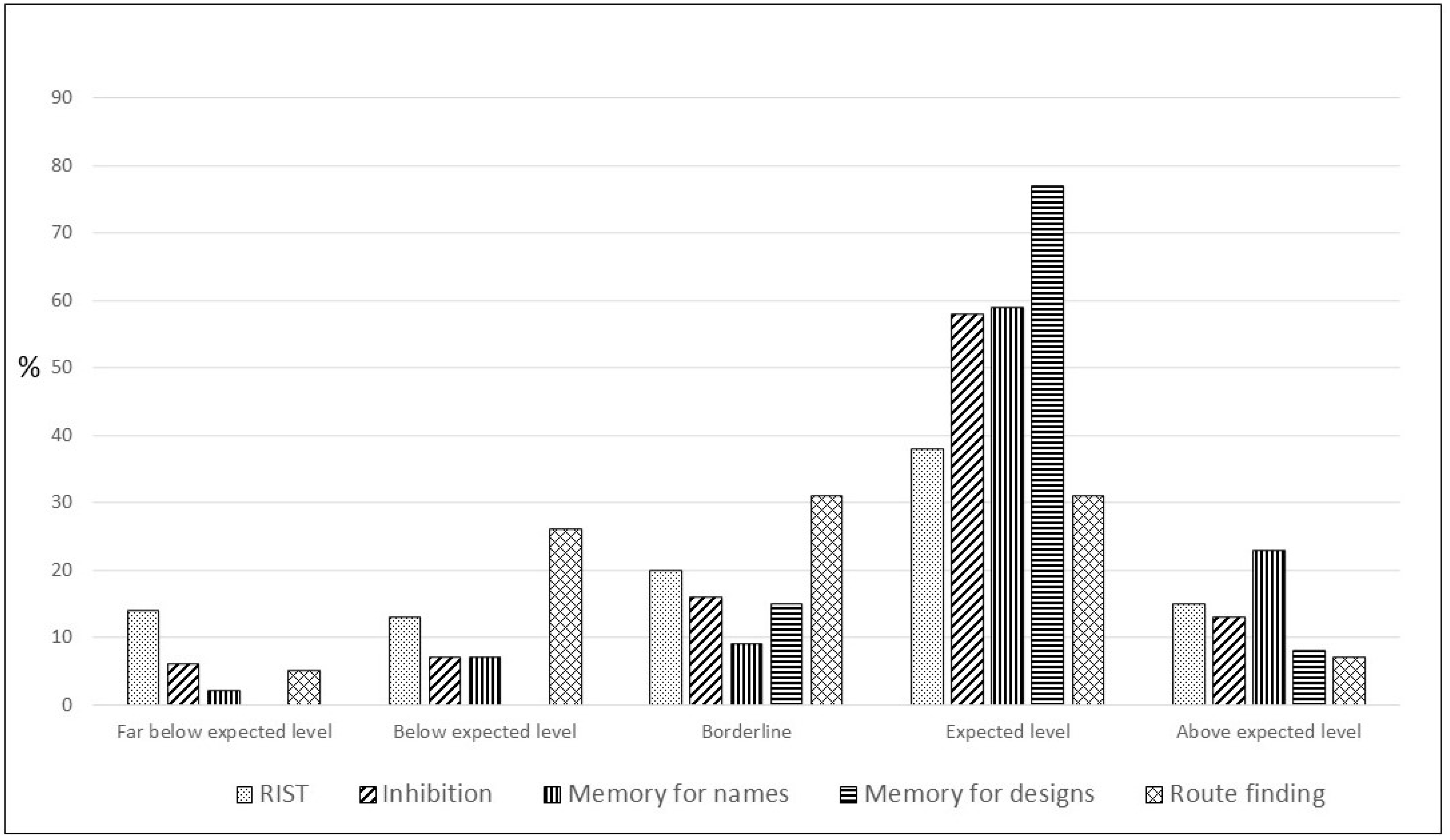
3.2. Description of Results of Neuropsychological Tests
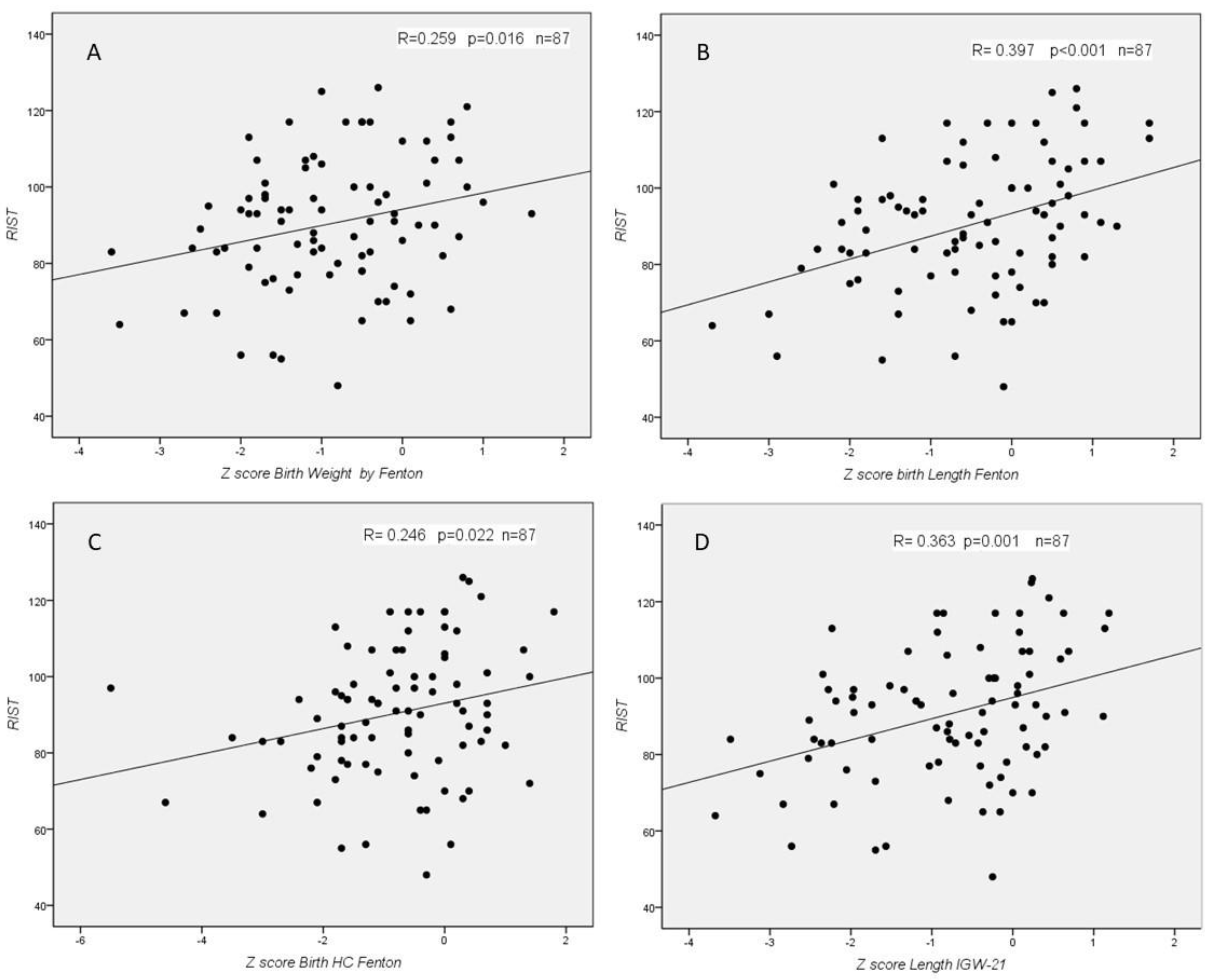
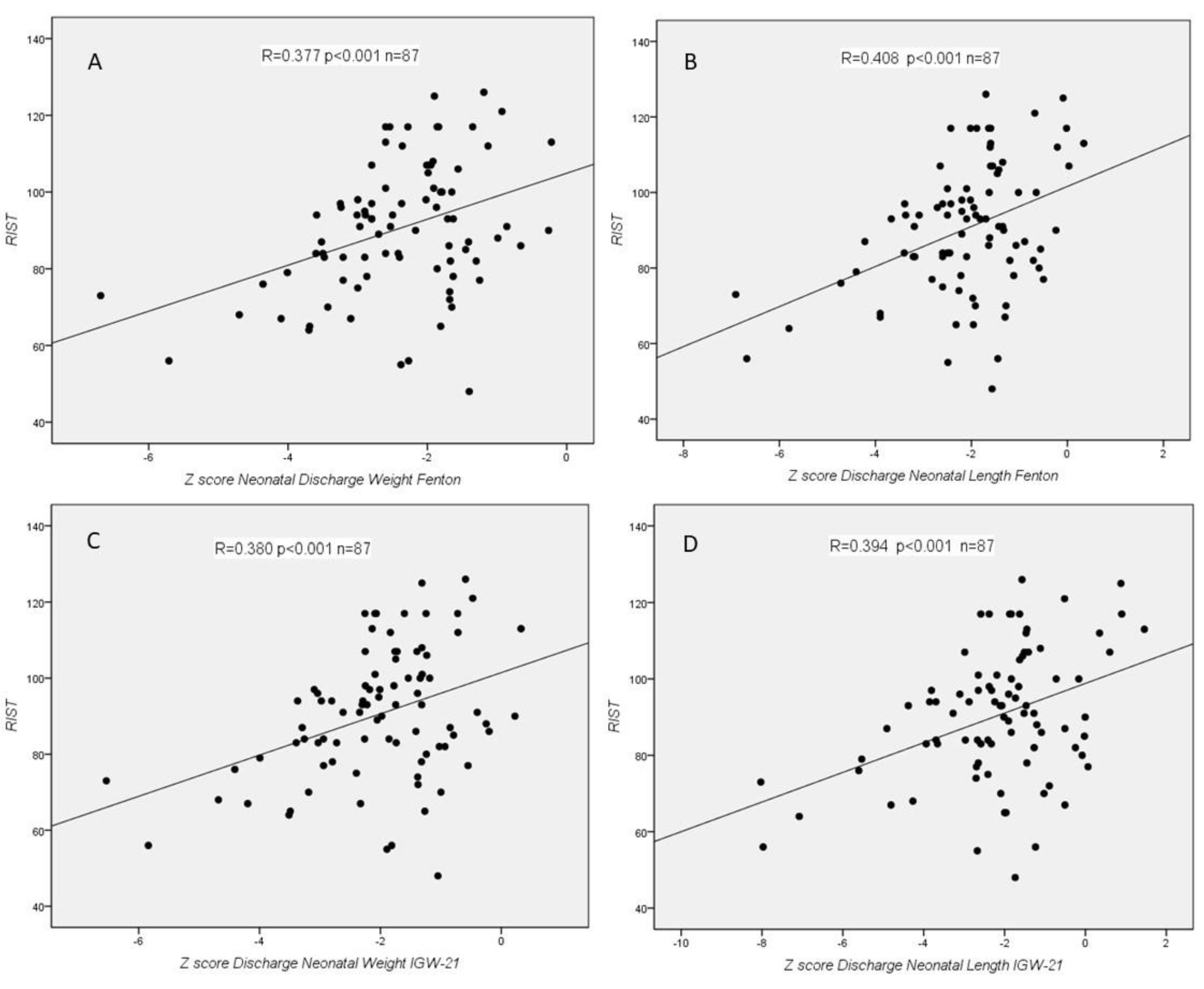
3.3. Relationship between Growth and Neurological Clinical Development and Neuropsychological Tests
4. Discussion
4.1. Growth
4.2. Neuropsychological Test
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Belfort, M.B.; Ehrenkranz, R.A. Neurodevelopmental outcomes and nutritional strategies in very low birth weight infants. Semin. Fetal Neonatal Med. 2017, 22, 42–48. [Google Scholar] [CrossRef]
- Fenton, T.R.; Cormack, B.; Goldberg, D.; Nasser, R.; Alshaikh, B.; Eliasziw, M.; Hay, W.W.; Hoyos, A.; Anderson, D.; Bloomfield, F.; et al. “Extrauterine growth restriction” and “postnatal growth failure” are misnomers for preterm infants. J. Perinatol. 2020, 40, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.S.; Wong, K.Y.; Merko, S.; Bishara, R.; Dunn, M.; Asztalos, E.; Darling, P.B. Postnatal growth failure in preterm infants: Ascertainment and relation to long-term outcome. J. Perinat. Med. 2006, 34, 484–489. [Google Scholar] [CrossRef]
- Zozaya, C.; Díaz, C.; Saenz de Pipaón, M. How should we define postnatal growth restriction in preterm infants? Neonatology 2018, 114, 177–180. [Google Scholar] [CrossRef]
- Franz, A.R.; Pohlandt, F.; Bode, H.; Mihatsch, W.A.; Sander, S.; Kron, M.; Steinmacher, J. Intrauterine, early neonatal, and postdischarge growth and neurodevelopmental outcome at 5.4 years in extremely preterm infants after intensive neonatal nutritional support. Pediatrics 2009, 123, e101–e109. [Google Scholar] [CrossRef] [Green Version]
- Ehrenkranz, R.A.; Dusick, A.M.; Vohr, B.R.; Wright, L.L.; Wrage, L.A.; Poole, W.K. Growth in the neonatal intensive care unit influences neurodevelopmental and growth outcomes of extremely low birth weight infants. Pediatrics 2006, 117, 1253–1261. [Google Scholar] [CrossRef] [Green Version]
- Ong, K.K.; Kennedy, K.; Castañeda-Gutiérrez, E.; Forsyth, S.; Godfrey, K.M.; Koletzko, B.; Latulippe, M.E.; Ozanne, S.E.; Rueda, R.; Schoemaker, M.H.; et al. Postnatal growth in preterm infants and later health outcomes: A systematic review. Acta Paediatr. 2015, 104, 974–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belfort, M.B.; Gillman, M.W.; Buka, S.L.; Casey, P.H.; McCormick, M.C. Preterm infant linear growth and adiposity gain: Trade-offs for later weight status and intelligence quotient. J. Pediatr. 2013, 163, 1549–1564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guellec, I.; Lapillonne, A.; Marret, S.; Picaud, J.C.; Mitanchez, D.; Charkaluk, M.L.; Fresson, J.; Arnaud, C.; Flamand, C.; Cambonie, G.; et al. Effect of intra- and extrautrine growth on long-term neurologic outcomes of very preterm infants. J. Pediatr. 2016, 175, 93–99.e1. [Google Scholar] [CrossRef] [PubMed]
- Lean, R.E.; Paul, R.A.; Smyser, T.A.; Smyser, C.D.; Rogers, C.E. Social Adversity and Cognitive, Language, and Motor Development of Very Preterm Children from 2 to 5 Years of Age. J. Pediatr. 2018, 203, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Baizan, C.; Alcántara-Canabal, L.; Solis, G.; Mendez, M. The association between perinatal and neonatal variables and neuropsychological development in very and extremely low-birth-weight preterm children at the beginning of primary school. Appl. Neuropsychol. Child 2020, 10, 348–358. [Google Scholar] [CrossRef]
- Twilhaar, E.S.; Wade, R.M.; de Kieviet, J.F.; van Goudoever, J.B.; van Elburg, R.M.; Oosterlaan, J. Cognitive Outcomes of Children Born Extremely or Very Preterm Since the 1990s and Associated Risk Factors: A Meta-analysis and Meta-regression. JAMA Pediatr. 2018, 172, 361–367. [Google Scholar] [CrossRef]
- Aanes, S.; Bjuland, K.J.; Skranes, J.; Lohaugen, G.C.C. Memory function and hippocampal volumes in preterm born very-low-birth-weight (VLBW) young adults. Neuroimage 2015, 105, 76–83. [Google Scholar] [CrossRef]
- Omizzolo, C.; Scratch, S.E.; Stargatt, R.; Kidokoro, H.; Thompson, D.K.; Lee, K.J.; Cheong, J.; Neil, J.; Inder, T.E.; Doyle, L.W.; et al. Neonatal Brain Abnormalities and Memory and Learning Outcomes at 7 Years in Children Born Very Preterm. Memory 2014, 22, 605–615. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Baizan, C.; Alcantara-Canabal, L.; Solis, G.; Mendez, M. Development of egocentric and allocentric spatial orientation abilities in children born preterm with very low birth weight. Early Hum. Dev. 2020, 141, 104947. [Google Scholar] [CrossRef] [PubMed]
- van Veen, S.; van Wassenaer-Leemhuis, A.G.; van Kaam, A.H.; Oosterlaan, J.; Aarnoudse-Moens, C.S.H. Visual perceptive skils account for very preterm children’s mathematical difficulties in preschool. Early Hum. Dev. 2019, 129, 11–15. [Google Scholar] [CrossRef]
- Loe, I.M.; Chatav, M.; Alduncin, N. Complementary assessments of executive function in preterm and full-term preeschoolers. Child Neuropsychol. 2015, 21, 331–353. [Google Scholar] [CrossRef] [PubMed]
- Schnider, B.; Disselhoff, V.; Held, U.; Latal, B.; Hagmann, C.F.; Wehrle, F.M. Executive function deficits mediate the association between very preterm birth and behavioral problems at school-age. Early Hum. Dev. 2020, 146, 105076. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, F.; Ismail, L.C.; Bertino, E.; Bhutta, Z.A.; Ohuma, E.O.; Rovelli, I. Monitoring postnatal growth of preterm infants: Present and future. Am. J. Clin. Nutr. 2016, 103, 635S–647S. [Google Scholar] [CrossRef] [Green Version]
- Pearson, F.; Johnson, M.J. How should we chart the growth of very preterm babies? Arch. Dis. Child. Fetal. Neonatal. Ed. 2019, 104, F120–F121. [Google Scholar] [CrossRef]
- Izquierdo Renau, M.; Aldecoa-Bilbao, V.; Balcells Esponera, C.; del Rey Hurtado de Mendoza, B.; Iriondo Sanz, M.; Iglesias-Platas, I. Applying Methods for Postnatal Growth Assessment in the Clinical Setting: Evaluation in a Longitudinal Cohort of Very Preterm Infants. Nutrients 2019, 11, 2772. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatrics, Committee on Nutrition. Nutritional needs of low-birth-weight infants. Pediatrics 1977, 60, 519–530. [Google Scholar]
- Olsen, I.E.; Groveman, S.A.; Lawson, M.L.; Clark, R.H.; Zemel, B.S. New intrauterine growth curves based on United States data. Pediatrics 2010, 125, e214–e224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenton, T.R. A new growth chart for preterm babies: Babson and Benda’s chart updated with recent data and a new format. BMC Pediatr. 2003, 3, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef] [Green Version]
- Ehrenkranz, R.A.; Younes, N.; Lemons, J.A.; Fanaroff, A.A.; Donovan, E.F.; Wright, L.L.; Katsikiotis, V.; Tyson, J.E.; Oh, W.; Shankaran, S.; et al. Longitudinal growth of hospitalized very low birth weight infants. Pediatrics 1999, 104, 280–289. [Google Scholar] [CrossRef]
- Villar, J.; Giuliani, F.; Barros, F.; Roggero, P.; Zarco, I.A.C.; Rego, M.A.S.; Ochieng, R.; Gianni, M.L.; Rao, S.; Lambert, A.; et al. Monitoring the Postnatal Growth of Preterm Infants: A Paradigm Change. Pediatrics 2018, 141, e20172467. [Google Scholar] [CrossRef] [Green Version]
- Villar, J.; Giuliani, F.; Bhutta, Z.A.; Bertino, E.; Ohuma, E.O.; Ismail, L.C.; Barros, F.C.; GAltman, D.; Victora, C.; Noble, J.A.; et al. Postnatal growth standards for preterm infants: The Preterm Postnatal Follow-up Study of the INTERGROWTH-21st Project. Lancet Glob. Health 2015, 3, e681–e691. [Google Scholar] [CrossRef] [Green Version]
- WHO Multicentre Growth Reference Study Group. WHO child growth standards based on length/height, weight and age. Acta Paediatr. 2006, 450, 76–85. [Google Scholar]
- Reddy, K.V.; Sharma, D.; Vardhelli, V.; Bashir, T.; Deshbotla, S.K.; Murki, S. Comparison of Fenton 2013 growth curves and Intergrowth-21 growth standards to assess the incidence of intrauterine growth restriction and extrauterine growth restriction in preterm neonates ≤32 weeks. J. Matern.-Fetal Neonatal Med. 2019, 34, 2634–2641. [Google Scholar] [CrossRef]
- Figueras-Aloy, J.; Palet-Trujols, C.; Matas-Barceló, I.; Botet-Mussons, F.; Carbonell-Estrany, X. Extrauterine growth restriction in very preterm infant: Etiology, diagnosis, and 2-year follow-up. Eur. J. Pediatr. 2020, 179, 1469–1479. [Google Scholar] [CrossRef] [PubMed]
- Reynols, C.R.; Kamphaus, R.W. RIAS (Reynols Intellectual Assessment Scales) and the RIST (Reynols Intellectual Screening Test). In Professional Manual; Psychological Assessement Resources: Lutz, FL, USA, 2003. [Google Scholar]
- Korkman, M.; Kirk, U.; Kemp, S. NEPSY-II: A Developmental Neuropsychological Assessment; The Psychological Corporation: San Antonio, TX, USA, 2007. [Google Scholar]
- Lee, S.M.; Kim, N.; Namgung, R.; Park, M.; Park, K.; Jeon, J. Prediction of Postnatal Growth Failure among Very Low Birth Weight Infants. Sci. Rep. 2018, 8, 3729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peila, C.; Spada, E.; Giuliani, F.; Maiocco, G.; Raia, M.; Cresi, F.; Bertino, E.; Coscia, A. Extrauterine Growth Restriction: Definitions and Predictability of Outcomes in a Cohort of Very Low Birth Weight Infants or Preterm Neonates. Nutrients 2020, 12, 1224. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Shin, S.H.; Cho, H.; Shin, S.H.; Kim, S.H.; Song, I.G.; Kim, E.-K.; Kim, H.S. Extrauterine growth restriction in extremely preterm infants based on the Intergrowth-21st Project Preterm Postnatal Follow-up Study growth charts and the Fenton growth charts. Eur. J. Pediatr. 2021, 180, 817–824. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Studied Cases (n = 87) | Survivors Lost (n = 60) | Statistical Significance | |
|---|---|---|---|
| Weight (g): median (IQR) | 1220 (430) | 1163 (413) | 0.682 # |
| Gestational age (weeks) mean (CI 95%) | 29.6 (29.0–30.2) | 29.8 (29.0–30.6) | 0.774 & |
| Sex: male/female (n) | 51/36 | 31/29 | 0.404 @ |
| Multiple birth (n) | 30 | 15 | 0.220 @ |
| Type of delivery: Vaginal/Caesarean (n) | 27/60 | 23/37 | 0.359 @ |
| Apgar test (n) | |||
| 1 min: 0–3/4–6/>6 | 9/16/62 | 4/10/46 | 0.689 @ |
| 5 min: 0–3/4–6/>6 | 1/5/81 | 2/0/58 | 0.115 @ |
| Neonatal resuscitation (n) | |||
| Oxygen | 74 | 49 | 0.585 @ |
| Ambu with mask | 57 | 32 | 0.137 @ |
| CPAP nasal | 26 | 18 | 0.737 @ |
| Intubation | 35 | 18 | 0.204 @ |
| Heart massage and/or Drugs | 7 | 2 | 0.188 @ |
| Respiratory support: | |||
| Oxygen | 78 | 51 | 0.397 @ |
| Non-invasive ventilation (IMVn) | 46 | 33 | 0.799 @ |
| Conventional ventilation | 47 | 37 | 0.357 @ |
| High frequency ventilation | 2 | 2 | 0.705 @ |
| Diagnoses: | |||
| Hyaline membrane disease | 43 | 31 | 0.789 @ |
| Patent ductus arteriosus | 21 | 16 | 0.728 @ |
| Necrotizing enterocolitis | 4 | 1 | 0.335 @ |
| Early sepsis | 1 | 2 | 0.357 @ |
| Transfusable anaemia | 35 | 23 | 0.678 @ |
| Late sepsis | 23 | 18 | 0.636 @ |
| Intracranial haemorrhage | 21 | ||
| I or II | 2 | 15 | 0.562 @ |
| III or IV | 4 | ||
| Periventricular leukomalacia | 9 | 6 | 0.774 @ |
| Retinopathy of prematurity | |||
| I | 13 | 8 | 0.985 @ |
| II or III | 15 | 9 | |
| Fundus not performed | 4 | 3 | |
| Neurological development: | |||
| - Neurological disorders of any kind | 19 | 14 | 0.831 @ |
| - Major neurological disorders | 7 | 8 | 0.297 @ |
| - Congenital alterations not related | 2 | 2 | 0.704 @ |
| - Cerebral palsy | 5 | 5 | 0.540 @ |
| - Severe developmental disorders | 3 | 2 | 0.969 @ |
| - Language disorders | 12 | 4 | 0.172 @ |
| - Behavioural disorders and/or attention deficit hyperactivity disorder | 3 | 2 | 0.969 @ |
| Weight (g) | Length (cm) | Head Circumference (cm) | |
|---|---|---|---|
| Birth | |||
| Mean (CI 95%) | 1153 (1101–1204) | 37.8 (37.1–38.5) | 26.2 (25.7–26.7) |
| Median (IQR) | 1220 (430) | 38.0 (5) | 27.0 (4) |
| Neonatal discharge | |||
| Mean (CI 95%) | 2325 (2277–2372) | 45.4 (45.0–45.8) | 33.2 (32.9–33.5) |
| Median (IQR) | 2260 (225) | 45.0 (2.5) | 33.0 (1.5) |
| 2 years | |||
| Mean (CI 95%) | 11403 (11030–11775) | 86.0 (84.9–87.1) | 48.4 (48.0–49.8) |
| Median (IQR) | 11425 (2100) | 86.0 (6.5) | 48.5 (2.0) |
| Weight | Length | Head Circumference | ||
|---|---|---|---|---|
| Birth | IUGR | |||
| Fenton less than P10 | 33 (37.9%) | 23 (26.4%) | 29 (33.3%) | |
| IGW-21 less tan P10 | 34 (39.1%) | 28 (32.2%) | 34 (39.1%) | |
| Kappa concordance | 0.879 | 0.807 | 0.826 | |
| Neonatal discharge | Static EUGR (cross-sectional) | |||
| Fenton less than P10 | 78 (89.7%) | 68 (78.2%) | 25 (28.7%) | |
| IGW-21 less than P10 | 66 (75.9%) | 63 (72.4%) | 28 (32.2%) | |
| Kappa concordance | 0.532 | 0.785 | 0.81 | |
| Fenton less than −2 SD | 50 (57.5%) | 41 (47.1%) | 11 (12.6%) | |
| IGW-21 less than −2 SD | 41 (47.1%) | 42 (48.3%) | 15 (17.2%) | |
| Kappa concordance | 0.795 | 0.839 | 0.82 | |
| True EUGR | ||||
| For Fenton | 46 (52.8%) | 45 (51.7%) | 9 (10.3%) | |
| For IGW-21 | 32 (36.8%) | 38 (43.6%) | 10 (11.5%) | |
| Kappa concordance | 0.683 | 0.748 | 0.705 | |
| Dynamic EUGR (logitudinal) | ||||
| More than -1 SD Fenton | 54 (62.1%) | 56 (64.4%) | 17 (19.5%) | |
| More than -1 SD IGW-21 | 41 (47.1%) | 45 (48.3%) | 17 (19.5%) | |
| Kappa concordance | 0.705 | 0.605 | 0.781 | |
| More than −2 SD Fenton | 23 (26.4%) | 26 (29.9%) | 8 (9.2%) | |
| More than −2 SD IGW-21 | 19 (21.8%) | 26 (29.9%) | 8 (9.2%) | |
| Kappa concordance | 0.875 | 0.89 | 0.862 | |
| 2 years | OMS less than −2 SD | 12 (15.2%) | 7 (8.9%) | 4 (5.1%) |
| Diagnosed Clinical Neurological Disorders (n = 19) | Not Diagnosed Clinical Neurological Disorders (N = 68) | Est Sig # (p) | |
|---|---|---|---|
| RIST (median (IQR)) | 89 (42) | 91 (18) | 0.426 |
| Inhibition (median (IQR)) | 7 (5) | 10 (4) | 0.002 |
| Memory for names (median (IQR)) | 9 (7) | 10 (4) | 0.492 |
| Memory for designs (median (IQR)) | 10 (3) | 10 (4) | 0.630 |
| Route finding (median (IQR)) | 1 (1) | 3 (4) | 0.010 |
| Yes | No | Est Sig | |
|---|---|---|---|
| IUGR weight Fenton < P10 | 84 (20) | 95 (25) | 0.037 |
| IUGR length Fenton < P10 | 84 (22) | 93 (25) | 0.027 |
| IUGR length IGW-21 < P10 | 84 (24) | 93 (25) | 0.025 |
| IUGR HC Fenton < P10 | 84 (18) | 93 (25) | 0.006 |
| IUGR HC IGW-21 < P10 | 84 (18) | 93 (25) | 0.047 |
| Static EUGR length Fenton < −2 SD | 84 (20) | 93 (28) | 0.03 |
| Static EUGR length IGW-21 < −2 SD | 84 (19) | 95 (28) | 0.01 |
| Static EUGR HC Fenton < P10 | 83 (25) | 93 (23) | 0.018 |
| Static EUGR HC IGW-21 < P10 | 85 (23) | 92 (23) | 0.001 |
| Two years HC OMS < −2 SD | 70 (28) | 92 (21) | 0.025 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alcántara, L.; Fernández-Baizán, C.; González-García, L.; García-López, E.; González-López, C.; Arias, J.L.; Méndez, M.; Sánchez, G.S. Neuropsychological Development and New Criteria for Extrauterine Growth Restriction in Very Low-Birth-Weight Children. Children 2021, 8, 955. https://0-doi-org.brum.beds.ac.uk/10.3390/children8110955
Alcántara L, Fernández-Baizán C, González-García L, García-López E, González-López C, Arias JL, Méndez M, Sánchez GS. Neuropsychological Development and New Criteria for Extrauterine Growth Restriction in Very Low-Birth-Weight Children. Children. 2021; 8(11):955. https://0-doi-org.brum.beds.ac.uk/10.3390/children8110955
Chicago/Turabian StyleAlcántara, Leticia, Cristina Fernández-Baizán, Lara González-García, Enrique García-López, Clara González-López, Jorge Luis Arias, Marta Méndez, and Gonzalo Solís Sánchez. 2021. "Neuropsychological Development and New Criteria for Extrauterine Growth Restriction in Very Low-Birth-Weight Children" Children 8, no. 11: 955. https://0-doi-org.brum.beds.ac.uk/10.3390/children8110955