
Radiological Outcomes of Femoral Head Resection in Patients with Cerebral Palsy: A Retrospective Comparative Study of Two Surgical Procedures


Abstract
:1. Introduction
2. Materials and Methods
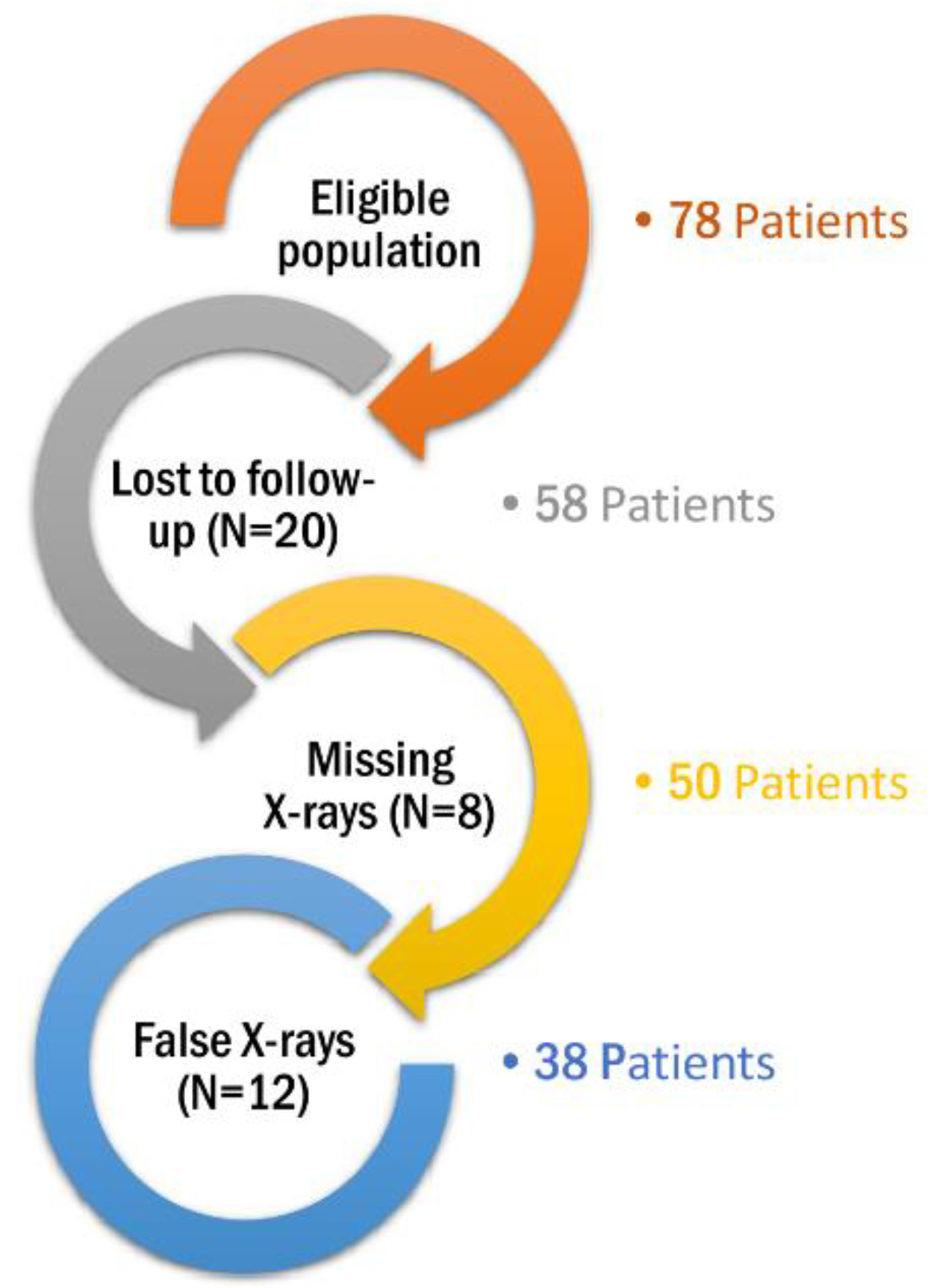
2.1. Study Design and Eligibility Criteria
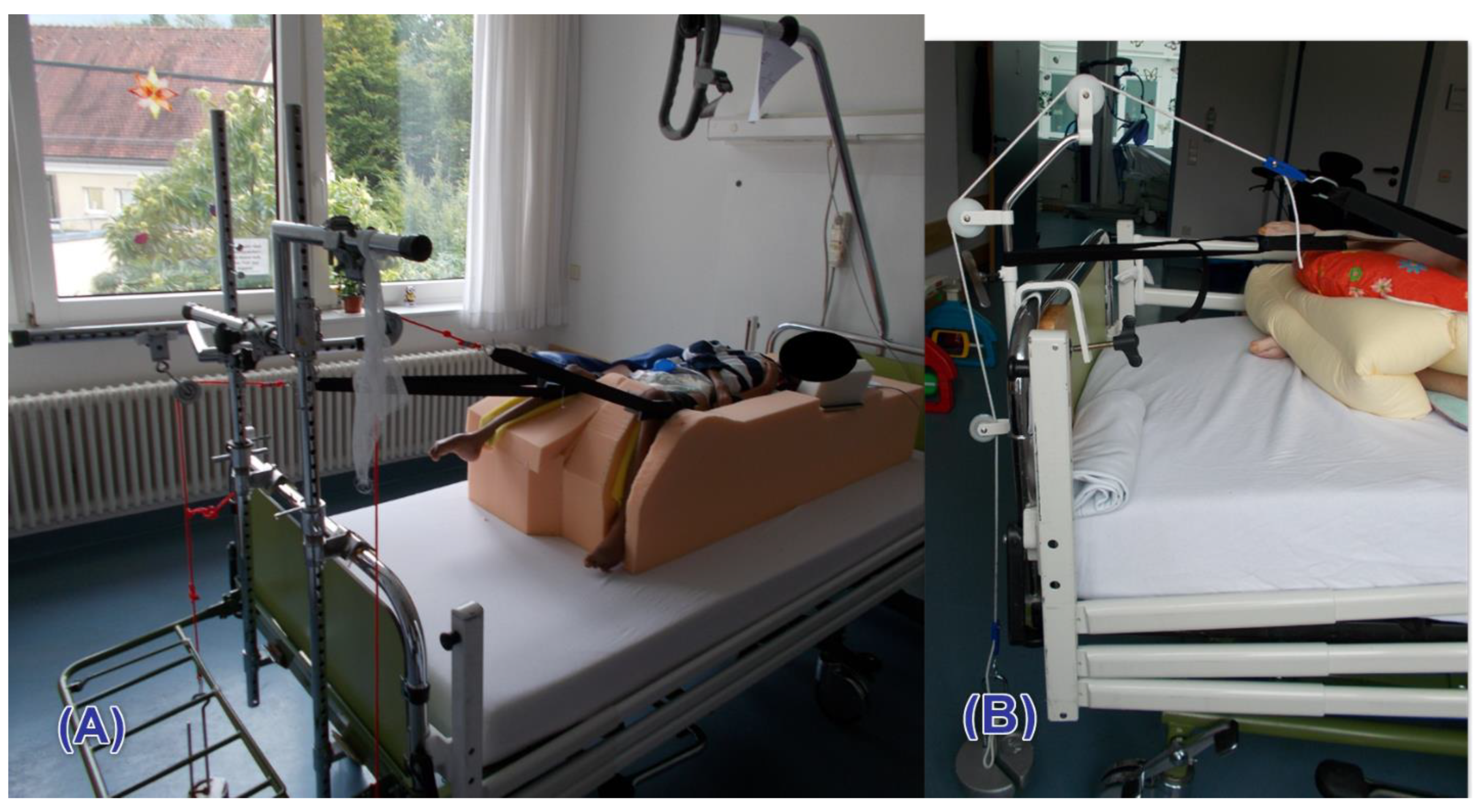
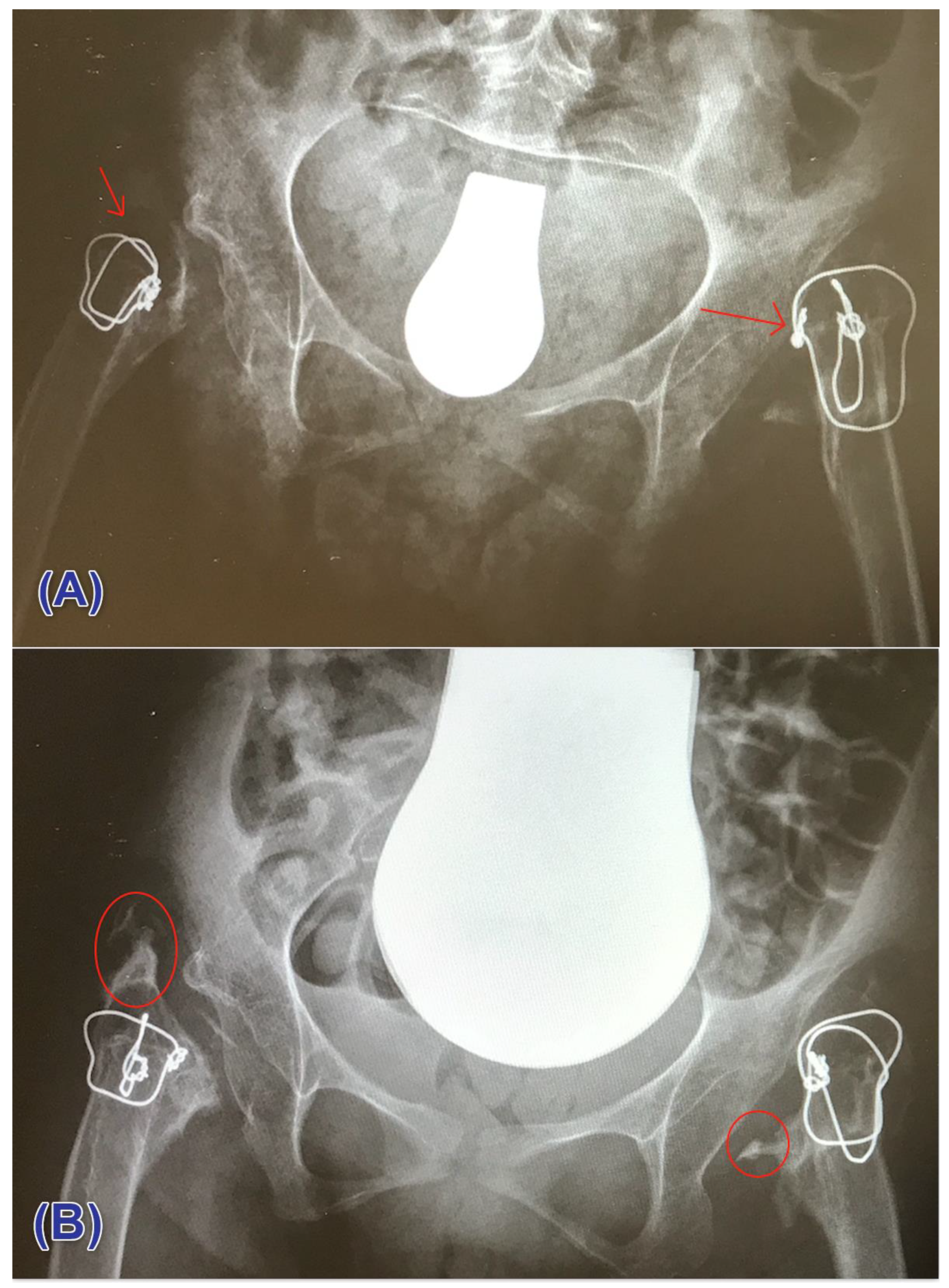
2.2. Study Procedures and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Procedural Outcomes
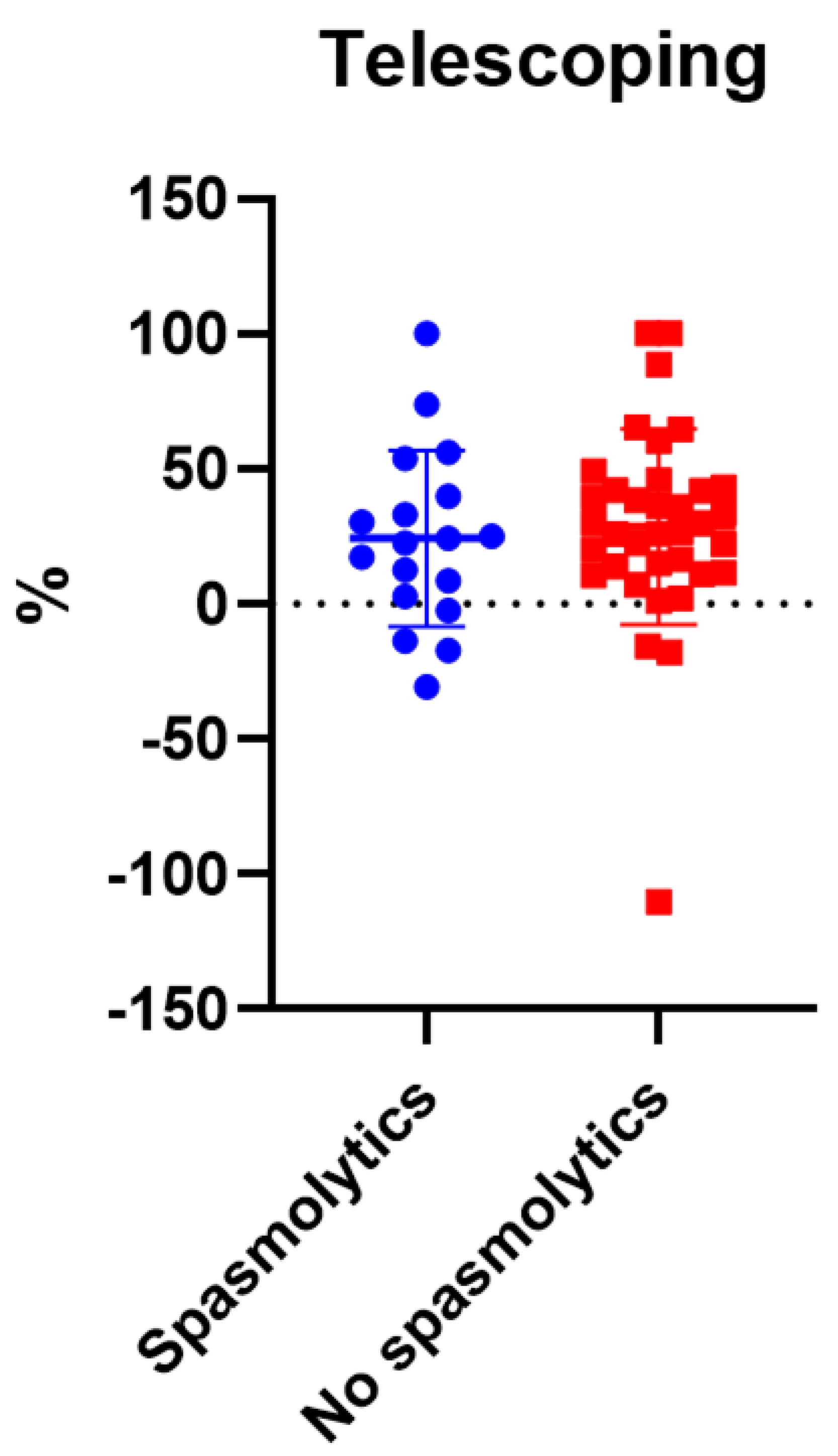
3.2.1. Telescoping
3.2.2. Spasmolytic Use and Telescoping
3.2.3. Traction Weight and Telescoping
3.2.4. Traction Duration and Telescoping
3.3. Heterotopic Ossification
3.4. Postoperative Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Odding, E.; Roebroeck, M.E.; Stam, H.J. The epidemiology of cerebral palsy: Incidence, impairments and risk factors. Disabil. Rehabil. 2006, 28, 183–191. [Google Scholar] [CrossRef]
- Terjesen, T. The natural history of hip development in cerebral palsy. Dev. Med. Child Neurol. 2012, 54, 951–957. [Google Scholar] [CrossRef]
- Robin, J.; Graham, H.K.; Selber, P.; Dobson, F.; Smith, K.; Baker, R. Proximal femoral geometry in cerebral palsy: A population-based cross-sectional study. J. Bone Jt. Surg. Br. Vol. 2008, 90, 1372–1379. [Google Scholar] [CrossRef] [Green Version]
- Shore, B.J.; Yu, X.; Desai, S.; Selber, P.; Wolfe, R.; Graham, H.K. Adductor surgery to prevent hip displacement in children with cerebral palsy: The predictive role of the Gross Motor Function Classification System. J. Bone Jt. Surg. Am. 2012, 94, 326–334. [Google Scholar] [CrossRef] [Green Version]
- Penner, M.; Xie, W.Y.; Binepal, N.; Switzer, L.; Fehlings, D. Characteristics of pain in children and youth with cerebral palsy. Pediatrics 2013, 132, e407–e413. [Google Scholar] [CrossRef] [Green Version]
- Cooperman, D.R.; Bartucci, E.; Dietrick, E.; Millar, E.A. Hip dislocation in spastic cerebral palsy: Long-term consequences. J. Pediatr. Orthop. 1987, 7, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Noonan, K.J.; Jones, J.; Pierson, J.; Honkamp, N.J.; Leverson, G. Hip function in adults with severe cerebral palsy. J. Bone Jt. Surg. Am. 2004, 86, 2607–2613. [Google Scholar] [CrossRef]
- Flynn, J.M.; Miller, F. Management of hip disorders in patients with cerebral palsy. J. Am. Acad. Orthop. Surg. 2002, 10, 198–209. [Google Scholar] [CrossRef]
- Shaw, K.A.; Hire, J.M.; Cearley, D.M. Salvage Treatment Options for Painful Hip Dislocations in Nonambulatory Cerebral Palsy Patients. J. Am. Acad. Orthop. Surg. 2020, 28, 363–375. [Google Scholar] [CrossRef]
- Dartnell, J.; Gough, M.; Paterson, J.M.H.; Norman-Taylor, F. Proximal femoral resection without post-operative traction for the painful dislocated hip in young patients with cerebral palsy: A review of 79 cases. Bone Joint J. 2014, 96-b, 701–706. [Google Scholar] [CrossRef]
- Heinen, F.; Michaelis, U.; Berweck, S. Gross Motor Function Classification System GMFCS. Klassif. Ther. Kinder Cereb. 2010, 19. Available online: https://cerebralpalsy.org.au/our-research/about-cerebral-palsy/what-is-cerebral-palsy/severity-of-cerebral-palsy/gross-motor-function-classification-system/ (accessed on 10 September 2021).
- Brooker, A.F.; Bowerman, J.W.; Robinson, R.A.; Riley, L.H., Jr. Ectopic ossification following total hip replacement. Incidence and a method of classification. J. Bone Jt. Surg. Am. 1973, 55, 1629–1632. [Google Scholar] [CrossRef]
- Della Valle, A.G.; Ruzo, P.S.; Pavone, V.; Tolo, E.; Mintz, D.N.; Salvati, E.A. Heterotopic ossification after total hip arthroplasty: A critical analysis of the Brooker classification and proposal of a simplified rating system. J. Arthroplast. 2002, 17, 870–875. [Google Scholar] [CrossRef]
- Dodwell, E.R.; Pathy, R.; Widmann, R.F.; Green, D.W.; Scher, D.M.; Blanco, J.S.; Doyle, S.M.; Daluiski, A.; Sink, E.L. Reliability of the Modified Clavien-Dindo-Sink Complication Classification System in Pediatric Orthopaedic Surgery. JB JS Open Access 2018, 3, e0020. [Google Scholar] [CrossRef]
- Castle, M.E.; Schneider, C. Proximal femoral resection-interposition arthroplasty. J. Bone Jt. Surg. Am. 1978, 60, 1051–1054. [Google Scholar] [CrossRef]
- Abu-Rajab, R.B.; Bennet, G.C. Proximal femoral resection-interposition arthroplasty in cerebral palsy. J. Pediatr. Orthop. B 2007, 16, 181–184. [Google Scholar] [CrossRef]
- Ackerly, S.; Vitztum, C.; Rockley, B.; Olney, B. Proximal femoral resection for subluxation or dislocation of the hip in spastic quadriplegia. Dev. Med. Child Neurol. 2003, 45, 436–440. [Google Scholar] [CrossRef] [Green Version]
- Baxter, M.P.; D’Astous, J.L. Proximal femoral resection-interposition arthroplasty: Salvage hip surgery for the severely disabled child with cerebral palsy. J. Pediatr. Orthop. 1986, 6, 681–685. [Google Scholar] [CrossRef]
- Dartnell, J.; Paterson, J.M.H.; Magill, N.; Norman-Taylor, F. Proximal femoral resection for the painful dislocated hip in cerebral palsy: Does indomethacin prevent heterotopic ossification? J. Pediatr. Orthop. 2014, 34, 295–299. [Google Scholar] [CrossRef]
- Egermann, M.; Döderlein, L.; Schläger, E.; Müller, S.; Braatz, F. Autologous capping during resection arthroplasty of the hip in patients with cerebral palsy. J. Bone Jt. Surg. Br. 2009, 91, 1007–1012. [Google Scholar] [CrossRef] [Green Version]
- Knaus, A.; Terjesen, T. Proximal femoral resection arthroplasty for patients with cerebral palsy and dislocated hips: 20 patients followed for 1–6 years. Acta Orthop. 2009, 80, 32–36. [Google Scholar] [CrossRef]
- Lampropulos, M.; Puigdevall, M.H.; Zapozko, D.; Malvárez, H.R. Proximal femoral resection and articulated hip distraction with an external fixator for the treatment of painful spastic hip dislocations in pediatric patients with spastic quadriplegia. J. Pediatr. Orthop. B 2008, 17, 27–31. [Google Scholar] [CrossRef]
- McCarthy, R.E.; Simon, S.; Douglas, B.; Zawacki, R.; Reese, N. Proximal femoral resection to allow adults who have severe cerebral palsy to sit. J. Bone Joint Surg. Am. 1988, 70, 1011–1016. [Google Scholar] [CrossRef]
- Muthusamy, K.; Simon, S.; Douglas, B.; Zawacki, R.; Reese, N. Femoral head resection as a salvage procedure for the severely dysplastic hip in nonambulatory children with cerebral palsy. J. Pediatr. Orthop. 2008, 28, 884–889. [Google Scholar] [CrossRef]
- Widmann, R.F.; Do, T.T.; Doyle, S.M.; Burke, S.W.; Root, L. Resection arthroplasty of the hip for patients with cerebral palsy: An outcome study. J. Pediatr. Orthop. 1999, 19, 805–810. [Google Scholar] [CrossRef]
- Patel, N.K.; Sabharwal, S.; Gooding, C.R.; Hashemi-Nejad, A.; Eastwood, D.M. Proximal femoral excision with interposition myoplasty for cerebral palsy patients with painful chronic hip dislocation. J. Child. Orthop. 2015, 9, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Alriksson-Schmidt, A.; Hägglund, G. Pain in children and adolescents with cerebral palsy: A population-based registry study. Acta Paediatr. 2016, 105, 665–670. [Google Scholar] [CrossRef] [Green Version]
- Ramstad, K.; Terjesen, T. Hip pain is more frequent in severe hip displacement: A population-based study of 77 children with cerebral palsy. J. Pediatr. Orthop. B 2016, 25, 217–221. [Google Scholar] [CrossRef]
- Dobson, F.; Boyd, R.N.; Parrott, J.; Nattrass, G.R.; Graham, H.K. Hip surveillance in children with cerebral palsy. Impact on the surgical management of spastic hip disease. The Journal of bone and joint surgery. Br. Vol. 2002, 84, 720–726. [Google Scholar] [CrossRef]
- Reidy, K.; Heidt, C.; Dierauer, S.; Huber, H. A balanced approach for stable hips in children with cerebral palsy: A combination of moderate VDRO and pelvic osteotomy. J. Child. Orthop. 2016, 10, 281–288. [Google Scholar] [CrossRef] [Green Version]
- Davis, E.; Williams, K.; Matheney, T.H.; Snyder, B.; Marcus, K.J.; Shore, B.J. Radiation Prophylaxis for Hip Salvage Surgery in Cerebral Palsy: Can We Reduce the Incidence of Heterotopic Ossification? J. Pediatr. Orthop. 2019, 39, e386–e391. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Sub-Category | FHR (N = 15) | FCP (N = 23) |
|---|---|---|---|
| Age (years); mean (SD) | |||
| 25.93 | 26.74 | ||
| Gender; N (%) | |||
| Male | 9 (60%) | 14 (60.9%) | |
| Female | 6 (40%) | 9 (39.1%) | |
| Operated side; N (%) | |||
| Unilateral | 7 (46.7%) | 15 (65.2%) | |
| Bilateral | 8 (53.3%) | 8 (34.8%) | |
| GMFCS; N (%) | |||
| Grade IV | 2 (13.3%) | 5 (21.7%) | |
| Grade V | 13 (86.7%) | 18 (78.3%) | |
| Follow-up (months); mean (SD) | |||
| 32.25 | 24.6 | ||
| Grade | FHR (N = 25) | FCP (N = 30) | ||
|---|---|---|---|---|
| N | % | N | % | |
| 0 | 5 | 20.00% | 5 | 16.70% |
| I | 9 | 36% | 6 | 20% |
| II | 9 | 36% | 16 | 53.30% |
| III | 2 | 8.00% | 3 | 10% |
| IV | 0 | 0% | 0 | 0% |
| Grade | FHR (N = 25) | FCP (N = 30) | ||
|---|---|---|---|---|
| N | % | N | % | |
| Grade I | 7 | 28% | 4 | 13.30% |
| Grade II | 7 | 28% | 10 | 33.30% |
| Grade III | 1 | 4% | 3 | 10% |
| Grade IV | 5 | 20% | 5 | 16.70% |
| Grade V | 0 | 0% | 1 | 3.30% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horsch, A.; Hahne, F.; Ghandour, M.; Platzer, H.; Alimusaj, M.; Putz, C. Radiological Outcomes of Femoral Head Resection in Patients with Cerebral Palsy: A Retrospective Comparative Study of Two Surgical Procedures. Children 2021, 8, 1105. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121105
Horsch A, Hahne F, Ghandour M, Platzer H, Alimusaj M, Putz C. Radiological Outcomes of Femoral Head Resection in Patients with Cerebral Palsy: A Retrospective Comparative Study of Two Surgical Procedures. Children. 2021; 8(12):1105. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121105
Chicago/Turabian StyleHorsch, Axel, Finja Hahne, Maher Ghandour, Hadrian Platzer, Merkur Alimusaj, and Cornelia Putz. 2021. "Radiological Outcomes of Femoral Head Resection in Patients with Cerebral Palsy: A Retrospective Comparative Study of Two Surgical Procedures" Children 8, no. 12: 1105. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121105