
The Current Status of Neuroprotection in Congenital Heart Disease
by
 ,
,
Kei Kobayashi
1,2,† ,
,
Christopher Liu
1,3,†,
Richard A. Jonas
1,2,4,‡ and
Nobuyuki Ishibashi
1,2,4,*,‡ 1
Center for Neuroscience Research, Sheikh Zayed Institute for Pediatric Surgical Innovation, Children’s National Hospital, Washington, DC 20010, USA
2
Children’s National Heart Institute, Children’s National Hospital, Washington, DC 20010, USA
3
School of Medicine, Virginia Commonwealth University, Richmond, VA 23298, USA
4
School of Medicine and Health Science, George Washington University, Washington, DC 20052, USA
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
‡
These authors also contributed equally to this work.
Children 2021, 8(12), 1116; https://0-doi-org.brum.beds.ac.uk/10.3390/children8121116
Submission received: 3 November 2021
/
Revised: 26 November 2021
/
Accepted: 29 November 2021
/
Published: 2 December 2021
(This article belongs to the Special Issue Advances in the Treatment of Congenital Cardiovascular Malformations in Children)
Abstract
:Neurological deficits are a serious and common sequelae of congenital heart disease (CHD). While their underlying mechanisms have not been fully characterized, their manifestations are well-known and understood to persist through adulthood. Development of therapies to address or prevent these deficits are critical to attenuate future morbidity and improve quality of life. In this review, we aim to summarize the current status of neuroprotective therapy in CHD. Through an exploration of present research in the pre-operative, intra-operative, and post-operative phases of patient management, we will describe existing clinical and bench efforts as well as current endeavors underway within this research area.
1. Introduction
Congenital Heart Disease (CHD) is the leading cause of death in infancy out of all known birth defects, occurring in 8 out of 1000 live births [1,2].However, the mortality of CHD has trended downwards as a result of improved diagnostic modalities, better surgical techniques, and advances in intensive care [3,4]. Now, most children affected by CHD will reach adulthood evident by the over 50% increase in adult prevalence rates from the years 2000 to 2010 [3]. This increase in survival rates has led to a corresponding shift in research focus from short-term survival to long-term morbidity and quality of life outcomes [5,6].
Neurodevelopmental deficits are a common and crucial sequela in patients with critical CHD, contributing to long-term morbidity that starts in infancy and persists into adulthood [3,6,7,8,9,10]. The prevalence and severity of such deficits are correlated with greater complexity of CHD and are estimated to reach an incidence of approximately 50% in infants [6,11]. Specifically, manifestations of neurodevelopmental deficits include impaired cognition, gross and fine motor skills, social interaction, communication, executive function as well as impulsive behavior and inattention [6,12,13,14] as presented from following clinical studies.
1.1. Boston Circulatory Arrest Trial
Longitudinal studies following patients with CHD throughout childhood have delivered valuable information about neurodevelopment. The Boston Circulatory Arrest Trial was a single-center longitudinal study that has followed a cohort of patients with dextrotransposition of the great arteries (d-TGA) who underwent the arterial switch operation (NCT03073122) [10,15,16]. In their patients’ infancy, Bellinger et al. reported numerous neurodevelopmental challenges including lower than normal scores on the Bayley Scales of Infant Development and substandard expressive language capabilities [17]. Childhood years continued this pattern of abnormal neurodevelopment evident in observations of lower intelligence quotient (IQ), worse mathematics and reading scores, poorer memory scores, attenuated visual-spatial skills, increased prevalence of behavioral problems, and immature motor function. Importantly noted was the finding that over a third of the cohort had received remedial services in school [13,14]. Age 16 follow-up demonstrated similar findings with persistent neuro-deficits and impaired psychosocial, physical, and emotional health [10,18]. Another study conducted at Boston Children’s Hospital observed similar neurodevelopmental outcomes in a cohort of 156 patients who had undergone Fontan procedures for single ventricle pathophysiology. Lower IQ scores, individual achievement, memory, executive function as well as an increased incidence of attention deficit hyperactivity disorder (ADHD), anxiety disorders, and MRI abnormalities paralleled the d-TGA cohort’s findings [19,20].
1.2. Single Ventricle Reconstruction Trial
Results consistent with these were also observed in the Single Ventricle Reconstruction (SVR) trial (NCT02692443). Recently published 6-year outcome data from the SVR trial revealed impairments in adaptive behavior, quality of life, functional status, and adaptive skills within a cohort of newborns with single right ventricular anomalies [21,22]. The incidence of these deficits surpasses that of the normal population with mild and severe motor disabilities occurring at 6 and 11 times the normal incidence rate respectively while the odds ratio for parent-reported executive function impairment has been reported to be 4.37 when compared to normative controls [23,24]. These reports are supported by several other studies describing similar results for cognitive, motor, and behavioral aspects of neurodevelopment [25,26,27,28,29,30]. Indeed, these deficits are common and are not specific to a single CHD subtype.
1.3. Risk Factors Associated with Neurological Deficits in Children with CHD
The causes of neurodevelopmental deficits associated with CHD are cumulative, multifactorial, and synergistic (Figure 1) [5]. Genetic components are unquestionably a broad underlying factor in the development of CHD and also a key contributor to a patient’s vulnerability to neurologic injury [5,31,32]. Additionally in the in utero phase, chronic fetal hypoxia resulting from abnormal physiology and altered regulatory pathways is largely responsible for immature brain development [33,34]. Establishment of a link between cerebral hypoxia and reduced brain volumes as well as poorer neurodevelopmental outcomes in CHD patients has been a crucial element in the push to develop pre-operative neuroprotective treatment aimed at addressing insufficient oxygen delivery to the fetus (Figure 2) [34,35].
Approximately 25% of neonates with CHD will require corrective cardiac surgery within their first year of life and will be at risk for neurological injury associated with cardiac surgery particularly when cardiopulmonary bypass (CPB) is required [36,37,38]. CPB causes systemic inflammatory response syndrome, ischemia-reperfusion, and reoxygenation injury as well as subsequent microglia mediated inflammation and enhanced oxidative stress, all of which contribute to the high incidence of white matter injury (WMI) observed in neonates and infants with CHD after surgery [39,40]. Although yet to be clearly defined, the mechanisms behind WMI are potential targets for neuroprotective therapy.
Post-operatively, factors contributing to neurodevelopmental delay are more broad in nature. Environment, socioeconomic status, and incidence of infections are factors that influence the maturation and growth for all infants, not only those with CHD [5,41,42,43,44]. Nonetheless, their significance in a patient population already at risk of neurodevelopmental deficits is elevated and must be explored to determine optimal methods of promoting healthy growth.
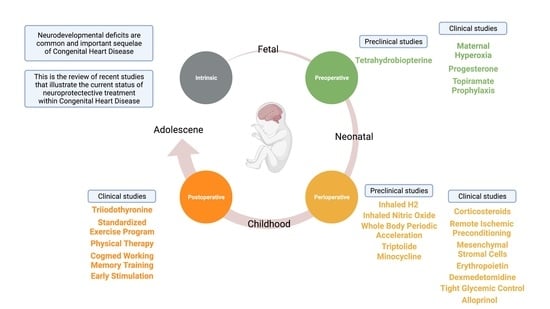
The gravity and prevalence of neurodevelopmental deficits within the CHD population necessitate therapies at each phase of patient management to prevent neurological injury and to promote neurodevelopment. Here, we review recent studies that illustrate the current status of neuroprotective treatment within CHD through analysis of existing strategies within the maternal, peri-operative, and post-operative stages of patient care (Table 1, Figure 3).
2. Maternal Neuroprotection—Clinical Studies
2.1. Maternal Hyperoxia
Chronic hypoxia is a key disruptor of fetal neurodevelopment in CHD. Recently, Lawrence et al. elucidated the role of chronic hypoxia in neurological injury by employing a fetal sheep model. They showed that chronic hypoxia in their artificial womb model reduced neuronal density and impaired myelination in the fetus resembling similar findings observed in neonates with CHD [45]. These neurological insults may be attenuated by supplementing oxygen supply. Previous studies have investigated the possibility of increasing oxygen levels in the fetus through maternal hyperoxygenation and have confirmed its feasibility through observed resultant increases in fetal oxygenation [46,47]. One clinical study in Canada has recently been initiated to investigate the effects of supplemental maternal oxygen during the 3rd trimester in mothers whose fetuses have been identified as having some form of CHD (https://clinicaltrials.gov/ ct2/show/NCT03944837, accessed on 3 November 2021). 10 to 15 L/min of oxygen by mask is given which briefly increases fetal oxygen levels to those reached in the newborn with spontaneous breathing. Although neurodevelopment is not directly defined as an endpoint, outcome measures of cerebral oxygen delivery, cerebral oxygen consumption, oximetry of major vessels, fetal brain volumetry, and brain size will provide valuable information about the physiological effects of maternal hyperoxygenation.
2.2. Progesterone
Although its exact cellular mechanism is still unknown, several animal studies have suggested that progesterone and its metabolites have a neuroprotective role in the developing brain [48]. In an acute hypoxia sheep model, allopregnanolone, a metabolite of progesterone through the enzymatic action of 5α-reductase, was found to be upregulated and correlated with an observed neuroprotective response after introduction of acute brain hypoxia [49]. A separate experiment confirmed this observation by observing a subsequent increase in neurological injury after inhibition of 5α-reductase via finasteride [50]. In addition, the same group also showed no increase in the fetal sheep brain allopregnanolone concentration after 20 days of chronic hypoxia created with a model of placental insufficiency in pregnant sheep, indicating a possible beneficial effect of allopregnanolone usage even in a chronic hypoxic state [51]. Investigation of WMI and brain immaturity in a neonatal rat model of chronic hypoxia, applied to mimic infants with cyanotic CHD, yielded similarly positive results. Notably, an increase in brain weights and greater motor and coordination abilities were observed in the progesterone treated group compared to controls [48]. Furthermore, progesterone has been implicated in oligodendrocyte maturation, oligodendrocyte progenitor cell proliferation, and myelination promotion through direct interaction with progesterone receptors [52]. As these effects of progesterone address cellular mechanisms of neurological injury observed in CHD, clinical translation of these studies has been pursued. Currently, a randomized phase 2 trial is underway in the USA to evaluate 3rd trimester Progesterone administration to a mother carrying a fetus with CHD (https://clinicaltrials.gov/ct2/show/NCT02133573, accessed on 3 November 2021). With endpoints specifically studying neurodevelopmental scores and brain maturation via MRI, a more thorough understanding of progesterone’s effects on neuroprotection will be achieved at its conclusion.
2.3. Topiramate Prophylaxis
Topiramate is an α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptor antagonist approved for the treatment of partial and generalized epileptic seizures. Recently it has been shown that Topiramate offers a potential therapy for hypoxic-ischemic encephalopathy by reducing underlying over-excitatory mechanisms of neural injury through increased gamma butyric acid activity (GABA) and decreased glutamate activity to address excessive glutamate production in the brain [53]. Combining study results that have demonstrated its neuroprotective capacity and ability to preserve oligodendrocytes in traumatic brain injury (TBI), stroke, epilepsy, and periventricular leukomalacia models with reports of improved long term cognition, memory, and attenuated WMI when used in tandem with therapeutic hypothermia has propelled Topiramate to the clinical trial phase [54,55,56,57]. Filippi et al. recently reported the results of a phase 2 multi-centre randomized control trial evaluating topiramate in neonates with hypoxic ischemic encephalopathy (HIE) [58]. In their study, they observed a non-significant downward trend in rates of epilepsy development in the topiramate treated group compared to controls but no significant difference in mortality and severe neurodevelopmental disability. However, this study was limited by its small number in the original cohort and the one-third reduction in sample size due to incorrect randomization. A separate study completed in 2017 studying the effects of topiramate prophylaxis in infants with CHD undergoing cardiac surgery will provide more information about the applicability of topiramate specifically in CHD as well as the future direction of this intervention (https://clinicaltrials.gov/ct2/show/NCT01426542, accessed on 3 November 2021).
3. Maternal Neuroprotection—Preclinical Studies for Future Translation
Tetrahydrobiopterin
Tetrahydrobiopterin (BH4) is key component of neuronal NO synthase function. During cerebral hypoxia, BH4 levels are depleted, leading to neuronal NO synthase uncoupling and a subsequent shift in production from NO to peryoxynitrite [59,60]. The ensuing damage generated by peryoxynitrite’s interaction with DNA and the increased production of reactive oxygen species escalates apoptotic and necrotic cell death, ultimately culminating in neurological injury [61]. As such, addressing the exhaustion of BH4 could be advantageous in protecting against WMI injury in the context of hypoxia. A recent study from Romanowicz et al. tested this hypothesis in a hypoxic rat model mimicking 3rd trimester human development [62]. In their experiment, they revealed that BH4 treatment prevented chronic hypoxia-associated delayed myelination and diminished mature oligodendrocyte populations while broadly decreasing apoptosis, although not specifically in oligodendrocytes. Crucially, BH4 treated mice showed protected motor-sensory coordination compared to control mice. These data are promising, suggesting possible auxiliary use of an FDA-approved agent for prenatal neuroprotective therapy.
4. Peri-Operative Neuroprotection—Clinical Studies
4.1. Corticosteroids
Corticosteroids have been used in cardiac surgery for more than 60 years. Mechanisms of action include modulation of CPB associated systemic inflammatory response [63] and possible counteraction of surgery-related relative adrenal insufficiency [64]. Several randomized controlled studies have shown that perioperative steroids reduce post-CPB inflammatory markers [65,66,67] However, the intraoperative use of corticosteroids in corrective congenital cardiac surgery is a highly debated topic [68]. Notwithstanding the numerous trials conducted, the long-term neurological effects of corticosteroids have yet to be studied [69,70]. Recently, a secondary analysis of a two-center, double-blind, randomized, placebo-controlled trial by Zyblewski et al. finally offered a glimpse into the neuroprotective effects of methylprednisolone [71]. They found that no significant difference was present in 12-month Bayley-III Developmental scores and post-operative brain injury biomarker levels between patients who received intra-operative methylprednisolone or placebo. Currently a phase 3 trial investigating the safety and efficacy of methylprednisolone in infants undergoing heart surgery with CPB is ongoing. The trial, when completed, will be one of the largest trials ever and will hopefully provide some clear answers regarding the use of corticosteroids for congenital heart surgery. (https://clinicaltrials.gov/ct2/show/NCT03229538, accessed on 3 November 2021).
4.2. Remote Ischemic Preconditioning
Ischemic preconditioning is a protective strategy against ischemia-reperfusion brain injury and is defined as the introduction of transient periods of ischemia prior to a prolonged period of ischemia such as hypothermic circulatory arrest [72]. The concept of remote ischemic preconditioning (RIPC) is similar but is distinguished by its ability to protect organs separate from the organ being exposed to transient ischemia [72]. Several animal studies have demonstrated the effects of RIPC in the protection of cerebral injury from stroke and hypothermic circulatory arrest [72,73,74]. As a result numerous clinical trials have been launched to translate these results to the clinical setting. Gaynor et al. recently published a randomized control trial evaluating RIPC and sham interventions in neonates before CPB commencement [75]. They identified no significant difference in WMI incidence or change in WMI volume change between groups. Another trial reported a similar lack of difference in neurodevelopmental outcomes when measuring post-operative neuron-specific enolase (NSE) and S100B levels [76]. However, they did observe cardioprotective effects with a decrease in post-operative Troponin1 and Creatine Kinase-MB levels in patients who received RIPC. Although these studies provide a greater understanding of the immediate post-operative effects of RIPC, a clinical trial underway in the United States will elaborate on RIPC in a longer term setting by being the first trial to report 12-month Bayley Developmental Scores in patients with CHD (https://clinicaltrials.gov/ct2/show/NCT01835392, accessed on 3 November 2021).
4.3. Mesenchymal Stromal Cells
Mesenchymal stromal cells (MSC) are a potential therapeutic agent for hypoxic brain injury due to their immunomodulatory and regenerative properties [77]. Various studies have shown that MSCs accelerate white matter remyelination through the activation of endogenous oligodendrocyte progenitors, promote neurogenesis from subventricular zone neural progenitors, and regulate microglia activation after hypoxic ischemic brain insults [78,79]. A recent laboratory study showed that MSC delivery through CPB has the potential to mitigate effects of CPB on neural stem/progenitor cells and to promote migration of neuroblasts in the subventricular zone [79]. In that study MSCs were delivered intraoperatively rather than preoperatively because cardiac surgery’s use of CPB provides arterial access which prevents loss of MSCs in the lungs observed during venous injection. The practicality of this method of delivery was recently assessed in an ex vivo CPB model. The study found that MSC delivery does not interfere with oxygenator function and does not elicit an immunogenic response in the host [80]. Together these findings have culminated in the initiation of a phase 1 prospective, open-label, single-center study which will determine the safety and feasibility of delivering MSCs in patients with CHD as well as any neurodevelopmental, neuroimaging, and postoperative inflammatory differences (https://clinicaltrials.gov/ct2/show/NCT04236479, accessed on 3 November 2021).
4.4. Erythropoietin
Erythropoietin (EPO) has been investigated as a potential neuroprotective pharmacologic intervention in neonates [81]. Although a previous meta-analysis of four randomized trials by Hendrik et al. demonstrated EPO reduced the risk of neurodevelopmental impairment as measured by the Mental Developmental Index score at an age of 18 to 24 months [82], a recent randomized trial by Juul et al. showed high-dose EPO administration to extremely preterm infants did not result in a lower risk of severe neurodevelopmental impairment or death at 2 years of age [83]. In addition a clinical trial specifically focusing on intraoperative and peri-operative effects of EPO administration failed to show significant neurodevelopment outcome improvement at 1 year of life in neonates who underwent surgery for D-transposition of the great vessels, hypoplastic left heart syndrome, or aortic arch reconstruction, albeit with a small sample size [84]. Nevertheless, this study showed that the studied doses of EPO were safe in the neonate and will require future appropriately powered studies to elucidate the true effects of EPO on neurodevelopment in CHD patients following neonatal corrective surgery.
4.5. Dexmedetomidine
Prolonged and repeated use of anesthetics results in an important risk of developmental neurotoxicity in patients with CHD [85,86]. Dexmedetomidine, an α2 adrenergic receptor agonist, has been explored in several studies to test its neuroprotective properties in a CHD population [87,88,89]. Results have demonstrated an association between Dexmedetomidine administration and reduced levels of biomarkers of neurological injury, NES and S-100B, and have led to the initiation of ongoing clinical trial in CHD patient populations (https://clinicaltrials.gov/ct2/show/NCT02492269, accessed on 3 November 2021). Additionally other investigations into the utilization of Sevoflurane and specific anesthetic strategies have joined Dexmedetomidine in the clinical trial phase and may produce valuable insights as to how to better promote preservation of neurologic function in CHD patients undergoing cardiac surgery (https://clinicaltrials.gov/ct2/show/NCT03882788, accessed on 3 November 2021, https://clinicaltrials.gov/ct2/show/NCT02492269, accessed on 3 November 2021, https://clinicaltrials.gov/ct2/show/NCT03366597, accessed on 3 November 2021, https://clinicaltrials.gov /ct2/show/NCT04484922, accessed on 3 November 2021). Despite the safety and effectiveness of dexmedetomidine, it is known to have cardiac toxicities including bradycardia and hypotension. Dose adjustments should be considered especially with neonates who have reduced clearance [90]
4.6. Tight Glycemic Control
Neurodevelopment has been assessed within the context of perioperative glycemic control.
Studies linking neonatal hypoglycemia with adverse neurodevelopmental outcomes and hyperglycemia with microglial activation and neuronal damage to the hippocampal and frontal cortex have established the importance of maintaining a euglycemic state in neonates [91,92]. This has led to the idea that there may be a role for tight glycemic control in the care of neonates with CHD. In 2016, Sadhwani et al. reported the results of a two-center, prospective, randomized trial assessing infant neurodevelopment in CHD patients randomized to tight glycemic control or standard care post-operatively, ultimately finding no differences in neurodevelopmental scores at 1 year of age between groups [93]. Furthermore a study and its post hoc analysis by Agus et al. revealed that while infections were reduced in infants greater than 60 days old within the tight glycemic control group, tight glycemic control did not lead to a difference in mortality, length of stay, or overall infection rates [94]
4.7. Allopurinol
Xanthine oxidase is a potent source of free oxygen radicals, especially superoxide. Allopurinol is a xanthine oxidase inhibitor, which reduces the production of oxygen radicals [95]. In a rodent model of acute hypoxia-ischemic brain injury, allopurinol was shown to decrease brain injury through its antioxidant properties grounded in its ability to chelate unbound iron and scavenge free hydroxyl radicals [96]. Several clinical studies demonstrated a possible neuroprotective effect in neonates with HIE. Gunes et al. later found in a small randomized clinical trial of neonates with HIE that allopurinol treatment was associated with better developmental outcomes compared with placebo at one year of age [97]. Four to five-year follow ups of a separate trial of asphyxiated patients broadly showed no difference in mortality or adverse developmental outcomes [98]. However, sub-group analysis revealed a decrease in severe adverse outcomes defined as mortality or severe disability in neonates with moderate HIE who received allopurinol. While the effects of allopurinol in the context of CHD are unknown, these studies have demonstrated potential benefits in animal models and neonates with encephalopathy. A prospective randomized phase 3 trial currently taking place in the Netherlands is studying the perioperative and postnatal administration of allopurinol in CHD patients (https://clinicaltrials.gov/ct2/show/NCT04217421, accessed on 3 November 2021).
5. Peri-Operative Neuroprotection—Preclinical Studies for Future Translation
5.1. Inhaled H2
H2 gas is a potential agent capable of addressing CPB-associated neurological injury. It is known that the generation of superoxide anions and subsequent production of toxic hydroxyl radicals occurs in neurodegenerative and neuroinflammatory disorders [99]. Without an endogenous detoxification mechanism to neutralize these hydroxyl radicals, humans are susceptible to the cellular injury and increased apoptosis that take place when reactive oxygen species (ROS) interact with cellular components [100]. H2 gas may be able to fill this deficit through its role as a reducing agent [101]. Indeed, improved neurological scores, myocardial function, and survival have been associated with H2 gas treatment in a study comparing H2 treated rodents to rodents treated with only therapeutic hypothermia after 5 min of asphyxia induced cardiac arrest [102]. These results paired with CPB’s association with cerebral hypoxia have led to further study in CPB models. Recently Cole et al. studied continuous pre- and post-operative administration of 2.4% H2 gas in a neonatal swine model of CPB-induced cerebral hypoxic-ischemic injury [103]. They found that H2 gas administration led to greater rates of neurologically intact survival, improved neurologic deficit scores, and lower volumes of WMI both by MRI and histological analysis. The positive results of this study have led the authors to suggest possible applications of H2 in CHD heart surgery as well as in the settings of extracorporeal membrane oxygenation, myocardial infarction, and stroke.
5.2. Inhaled Nitric Oxide
In addition to CPB, deep hypothermic circulatory arrest (DHCA) potentiates development of neurological injury in CHD patients. One of the causes is disruption of nitric oxide (NO) regulated processes including ischemia/reperfusion, cerebral blood flow autoregulation, and microglial activation [104]. Inhaled NO (iNO) use during pediatric CPB has become popular and several trials have been reported [105,106]. These studies demonstrate improvement of post-operative outcomes determined by the anti-inflammatory effects of NO but are not specific to neuronal protection. The use of iNO requires further studies.
iNO exerts its neuroprotective effects by preserving cerebral autoregulation, an important factor in preserving oxygen delivery to the brain. This mechanism was better defined in a porcine model of TBI which showed that protection of cerebral autoregulation and subsequent decrease in hippocampal injury can be attributed to inhibition of Endothelin 1 (ET-1) and Extracellular Signal-Regulated Kinase (ERK)/Mitogen Activated Protein Kinase (MAPK) and simultaneous IL-6 upregulation [107]. The translation of these findings to models of cardiac surgery is reasonable as TBI and cardiac surgery share sequelae of impaired cerebral autoregulation and neuronal damage. Kajimoto et al. recently investigated the anti-inflammatory effects of inhaled Nitric Oxide in porcine models specifically in the setting of heart surgery with DHCA [104]. The study showed that iNO treated pigs had less neuronal degeneration, smaller microglial cell body volume, longer dendrite process length, and a larger quantity of branch segments and terminal branch points. Altogether these findings are suggestive of decreased microglial activation and maintain consistency with previous studies of iNO’s neuroprotective mechanisms. These results from basic research will likely lead to future clinical studies to determine the effectiveness of iNO in mitigating the deleterious effects of CPB and cardiac surgery on neuronal development.
5.3. Whole Body Periodic Acceleration
The suggested neuroprotective effects of whole-body periodic acceleration (pGz) are also based on its potential to modulate NO regulated pathways. Defined as a rhythmic pattern of acceleration and deceleration along the head to foot axis akin to the motion generated when pushing a stroller back and forth, pGz has been hypothesized to activate endothelial Nitric Oxide Synthase (eNOS) pathways via pulsatile shear stress generation [108]. Upregulation of these pathways, in turn, promotes cardiac and neuroprotective effects through their anti-inflammatory and anti-apoptotic properties [109]. A porcine model was used to investigate pGz preconditioning as a strategy for neuroprotection in cardiac surgery and found expected activation of eNOS and increased activation of anti-apoptotic p-Akt/Akt and Bcl/Bax signaling [110].
5.4. Triptolide
Triptolide is an extract of Tripterygium wilfordii, a plant commonly used in traditional Chinese medicine [111]. Known for its anti-inflammatory and immunosuppressive activity, Triptolide is a prospective therapeutic for addressing upregulated inflammatory pathways associated with CPB. Previous in vitro studies modeling traumatic brain injury, cerebral ischemia/reperfusion injury, and stroke have confirmed the presence of anti-inflammatory effects driven by suppressed activation of the NF-kB and p38MAPK pathways [112,113,114]. Importantly, these studies showed attenuated neurological deficits to be associated with Triptolide treatment [113]. A more recent experimental study applied these results to a 12–14 week rat model of CPB with DHCA and concluded that Triptolide treatment led to decreased levels of TNF a, IL1b, IL6, malondialdehyde, and ROS while increasing glutathione and superoxide dismutase levels [115]. Moreover mitigated microglia activation, NF-kB activity inhibition, and upregulation of the NRF2 pathway were observed, further emphasizing Triptolide’s anti-inflammatory and neuroprotective qualities. Neurodevelopmental endpoints in the same study were found to be positively impacted by Triptolide administration evident in improved spatial learning, memory, and anxiety-like behaviors. Given that the model used in this study was an adult rat, the results should be interpreted carefully for neonates. Further study in a neonate model is needed.
5.5. Minocycline
Minocycline is a tetracycline antibiotic commonly used for chronic recurrent bacterial infections [116]. Lately, it’s anti-inflammatory and neuroprotective properties have been highlighted in several animal models. Drabek et al. showed in their rat model that minocycline significantly attenuated brain tumor necrosis factor alpha, a principal mediator of neuroinflammation, after CPB followed by DHCA [117]. Aida et al. demonstrated significant attenuation of markers for hypoxia and apoptosis in cells from the hippocampus of 4-week-old piglets with 90 min of CPB followed by minocycline administration [118]. Results from these animal studies may provide sufficient rationale to perform clinical studies in the near future. Although developments in the understanding of minocycline’s neuroprotective capacity suggest potential applications for attenuation of neurologic injury, it should be remembered that in neonates, tetracycline can cause stunting of bone growth and bilirubin-induced brain damage [119].
6. Post-Operative Neuroprotection—Clinical Studies
6.1. Triiodothyronine
Thyroid hormones are a critical component of neurodevelopment in the post-natal period. In particular, the processes of cerebellar neurogenesis, gliogenesis, and myelogenesis rely on adequate Triiodothyronine levels while hypothyroxinemia has been observed to be associated with developmental delay [120]. Even transient congenital hypothyroidism in neonates has been reported to be associated with lower IQ at 7–8 years of age [121].
Reductions in thyroid hormone levels have been reported postoperatively after pediatric and adult cardiac surgery [122,123]. Bettendorf et al. attempted to raise thyroid levels in a cohort of 40 children undergoing cardiac surgery with triiodothyronine treatment and was able to verify that triiodothyronine is efficacious in elevating triiodothyronine plasma levels while improving myocardial function and reducing postoperative intensive care [124]. The long-term neuroprotective effects of triiodothyronine supplementation were assessed for the first time in the same cohort 10 years later. In the follow-up study, no significant differences were observed in IQ, gross and fine motor skills, and executive function between the triiodothyronine treated and control groups [125].
6.2. Standardized Exercise Program
The numerous benefits of physical activity are well established [126]. Importantly the impact of physical activity has also been shown to extend to aspects of cognition and neurodevelopment. Several studies in adults have demonstrated evidence suggestive of relationships between physical activity and hippocampal volume preservation as well as increased brain volume [127,128,129,130]. One randomized control trial even demonstrated a 2% increase in hippocampal volume corresponding to better spatial memory in response to a physical activity regimen [131]. In preadolescent children, improved executive function, attention, and academic performance have also been found to be associated with physical activity [132].
Similar results have been reported in CHD. Dulfer et al. randomized patients 10 to 25 years old with Tetralogy of Fallot or single ventricle anomalies into a 3-month standardized exercise program [133]. Aside from demonstrating better quality of life measures in the exercise group, the authors also observed positive effects in self-reported cognitive functioning and parent-reported social functioning. In addition, an ongoing clinical trial at Columbia University will attempt to show similar findings in a younger patient group through IQ, cognitive function, and adaptive behavior evaluations at 24 months (https://clinicaltrials.gov/ct2/show/NCT02542683, accessed on 3 November 2021).
6.3. Physical Therapy
The effects of physical therapy in the context of CHD have been rarely described. However, an observational cohort study in 2021 looking at gross motor development in children with CHD found increased Bayley-III scores during 12–24 month up assessments in patients who received regular physical therapy compared to those who received either no physical therapy or occasional physical therapy [134]. A recent study reported that the majority of a CHD cohort did not meet guidelines for physical fitness and had not received physical therapy 2 years post-operatively. Further investigation should be conducted to determine if participation in physical therapy by patients with CHD will promote motor skill development [135].
6.4. Cogmed Working Memory Training
The Cogmed Working Memory Training is a 5 week computerized program designed to enhance executive function, organization, and attention [136]. While its use has been shown to impart these benefits in children and adolescents with ADHD, learning disabilities as well as those who were born pre-term, its effects have yet to be demonstrated in patients with CHD [137,138,139]. Recently a clinical trial studied the efficacy of Cogmed Working Memory Training in a group of 13–16 year old adolescents. This trial specifically found that the training improved inhibitory control, attention, planning, and organizational skills immediately after training and at 3-month follow-up [136]. Furthermore the group assigned to the training demonstrated higher social responsiveness and communication scores. Although components of working memory and processing speed did not improve as previously reported in other patient populations, the Cogmed Working Memory Training had an overall positive impact on the neurological function of adolescents with CHD. A trial recently completed in 2020 is anticipated to show similar improvements specifically in patients with CHD in the age range of 7–12 years https://clinicaltrials.gov/ct2/show/NCT03023644, accessed on 3 November 2021).
6.5. Early Stimulation
The environment of the patient with CHD is crucial for their neurodevelopment. Among known non-biological factors such as maternal education and deprivation, a cognitively stimulating environment is known to be a modifiable factor with the capability to overcome other factors contributing to deficits in neurodevelopment [140,141,142,143]. Bonthrone et al. retrospectively assessed the level of cognitive stimulation of children with CHD by their parents and found that higher parent cognitive stimulation scores were associated with higher 22 month language and cognitive abilities [144]. A research group at the Instituto de Cardiologia de Rio Grande do Sul is investigating the effects of parent-administered early stimulation programs for children with CHD in a randomized prospective clinical trial by using 3 and 6 month neurodevelopmental scores as their primary endpoints (https://clinicaltrials.gov/ct2/show/NCT04152330, accessed on 3 November 2021).
7. Socioeconomic Status
We can’t disregard and close this review without talking about socioeconomic status (SES). SES is a measure of one’s overall status and position in society, which is well-recognized predictor of neurodevelopmental outcome in preterm children and may attenuate the effect of brain injury particularly on cognitive development [44]. Indeed, in many studies reporting shorter and longer-term neurodevelopmental outcomes, lower SES has been identified as an independent risk factor for worse outcomes in the CHD population [10,145,146,147]. Less maternal education has been associated with lower mental development index in infants with CHD [148]. Thus, particular attention must be given to neurodevelopmental care during the hospitalization and after discharge in children from disadvantaged families. Recent study reporting the relationship between a stimulating home environment and cognitive abilities in toddlers with CHD showed no relationship between outcome scores and SES, clinical factors, or brain injury severity at 22 months [144] However, the sample size is relatively small and future studies assessing the impact of home environment stimulation with larger samples are required.
8. Concluding Remarks and Future Perspectives
Neurodevelopmental deficits are common and important sequelae of CHD that are highly complex with cumulative, multifactorial, and synergistic etiologies. An important current limitation is that many clinical trials undertaken in the CHD population are based on clinical trials in other populations or on preclinical studies that target different mechanisms of injury. Therefore, the signaling pathways of the possible mechanisms and physiological events in children with CHD are not fully understood. While current therapies are being developed, continued collaboration and effort are needed to elucidate and dictate future areas of potential neuroprotective therapy in all stages of patient care. In addition, genetic contributions are now becoming a very important topic [31,32]. Although there is a need for better understanding of the impact of CHD-linked genes on brain development, the studies presented in this paper shed light on potential future therapeutic options.
Author Contributions
Conceptualization, K.K., R.A.J. and N.I.; writing-original draft preparation, K.K. and C.L.; writing-review and editing, R.A.J. and N.I.; supervision, R.A.J. and N.I. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by National Institutes of Health (NIH) grant R33 HL146394 (N.I., R.A.J.), R01HL139712 (N.I.) and R01HL146670 (N.I.) and by the Office of the Assistant Secretary of Defense for Health Affairs through the Peer Reviewed Medical Research Program under Award No. W81XWH2010199 (N.I.). We are thankful for the vision and generosity of the Foglia and Hill families who supported our studies.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Images on Figure 3 were retrieved from BioRender templates.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gilboa, S.M.; Salemi, J.; Nembhard, W.N.; Fixler, D.E.; Correa, A. Mortality Resulting from Congenital Heart Disease among Children and Adults in the United States, 1999 to 2006. Circulation 2010, 122, 2254–2263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernier, P.-L.; Stefanescu, A.; Samoukovic, G.; Tchervenkov, C.I. The Challenge of Congenital Heart Disease Worldwide: Epidemiologic and Demographic Facts. Semin. Thorac. Cardiovasc. Surgery Pediatr. Card. Surg. Annu. 2010, 13, 26–34. [Google Scholar] [CrossRef]
- Marelli, A.J.; Ionescu-Ittu, R.; Mackie, A.; Guo, L.; Dendukuri, N.; Kaouache, M. Lifetime Prevalence of Congenital Heart Disease in the General Population from 2000 to 2010. Circulation 2014, 130, 749–756. [Google Scholar] [CrossRef] [Green Version]
- Boneva, R.S.; Botto, L.D.; Moore, C.A.; Yang, Q.; Correa, A.; Erickson, J.D. Mortality Associated with Congenital Heart Defects in the United States. Circulation 2001, 103, 2376–2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morton, P.D.; Ishibashi, N.; Jonas, R.A. Neurodevelopmental Abnormalities and Congenital Heart Disease. Circ. Res. 2017, 120, 960–977. [Google Scholar] [CrossRef] [Green Version]
- Marino, B.S.; Lipkin, P.; Newburger, J.W.; Peacock, G.; Gerdes, M.; Gaynor, J.W.; Mussatto, K.A.; Uzark, K.; Goldberg, C.S.; Johnsonjr, W.H.; et al. Neurodevelopmental Outcomes in Children with Congenital Heart Disease: Evaluation and Management. Circulation 2012, 126, 1143–1172. [Google Scholar] [CrossRef] [Green Version]
- Moons, P.; Bovijn, L.; Budts, W.; Belmans, A.; Gewillig, M. Temporal Trends in Survival to Adulthood among Patients Born with Congenital Heart Disease from 1970 to 1992 in Belgium. Circulation 2010, 122, 2264–2272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newburger, J.W.; Sleeper, L.A.; Bellinger, D.C.; Goldberg, C.S.; Tabbutt, S.; Lu, M.; Mussatto, K.A.; Williams, I.A.; Gustafson, K.E.; Mital, S.; et al. Early Developmental Outcome in Children with Hypoplastic Left Heart Syndrome and Related Anomalies. Circulation 2012, 125, 2081–2091. [Google Scholar] [CrossRef] [Green Version]
- Calderon, J.; Bonnet, D.; Courtin, C.; Concordet, S.; Plumet, M.-H.; Angeard, N. Executive function and theory of mind in school-aged children after neonatal corrective cardiac surgery for transposition of the great arteries. Dev. Med. Child Neurol. 2010, 52, 1139–1144. [Google Scholar] [CrossRef]
- Bellinger, D.C.; Wypij, D.; Rivkin, M.J.; DeMaso, D.R.; Robertson, R.; Dunbar-Masterson, C.; Rappaport, L.A.; Wernovsky, G.; Jonas, R.A.; Newburger, J.W. Adolescents with d-Transposition of the Great Arteries Corrected with the Arterial Switch Procedure. Circulation 2011, 124, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Mahle, W.T.; Wernovsky, G. Long-Term Developmental Outcome Of Children with Complex Congenital Heart Disease. Clin. Perinatol. 2001, 28, 235–247. [Google Scholar] [CrossRef]
- Gaynor, J.W.; Nord, A.S.; Wernovsky, G.; Bernbaum, J.; Solot, C.B.; Burnham, N.; Zackai, E.; Heagerty, P.J.; Clancy, R.R.; Nicolson, S.C.; et al. Apolipoprotein E Genotype Modifies the Risk of Behavior Problems after Infant Cardiac Surgery. Pediatrics 2009, 124, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Bellinger, D.C.; Newburger, J.W.; Wypij, D.; Kuban, K.C.K.; Duplesssis, A.J.; Rappaport, L.A. Behaviour at eight years in children with surgically corrected transposition: The Boston Circulatory Arrest Trial. Cardiol. Young 2009, 19, 86–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellinger, D.C.; Wypij, D.; Duplessis, A.J.; Rappaport, L.A.; Jonas, R.A.; Wernovsky, G.; Newburger, J.W. Neurodevelopmental status at eight years in children with dextro-transposition of the great arteries: The Boston Circulatory Arrest Trial. J. Thorac. Cardiovasc. Surg. 2003, 126, 1385–1396. [Google Scholar] [CrossRef] [Green Version]
- Bellinger, D.C.; Wypij, D.; Kuban, K.; Rappaport, L.A.; Hickey, P.R.; Wernovsky, G.; Jonas, R.A.; Newburger, J.W. Developmental and Neurological Status of Children at 4 Years of Age after Heart Surgery with Hypothermic Circulatory Arrest or Low-Flow Cardiopulmonary Bypass. Circulation 1999, 100, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Newburger, J.W.; Jonas, R.A.; Wernovsky, G.; Wypij, D.; Hickey, P.R.; Kuban, K.; Farrell, D.M.; Holmes, G.L.; Helmers, S.L.; Constantinou, J.; et al. A Comparison of the Perioperative Neurologic Effects of Hypothermic Circulatory Arrest versus Low-Flow Cardiopulmonary Bypass in Infant Heart Surgery. N. Engl. J. Med. 1993, 329, 1057–1064. [Google Scholar] [CrossRef]
- Bellinger, D.C.; Rappaport, L.A.; Wypij, D.; Wernovsky, G.; Newburger, J.W. Patterns of Developmental Dysfunction after Surgery during Infancy to Correct Transposition of the Great Arteries. J. Dev. Behav. Pediatr. 1997, 18, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Robson, V.K.; Stopp, C.; Wypij, D.; Dunbar-Masterson, C.; Bellinger, D.C.; DeMaso, D.R.; Rappaport, L.A.; Newburger, J.W. Longitudinal Associations between Neurodevelopment and Psychosocial Health Status in Patients with Repaired D-Transposition of the Great Arteries. J. Pediatr. 2019, 204, 38–45.e1. [Google Scholar] [CrossRef] [PubMed]
- DeMaso, D.R.; Calderon, J.; Taylor, G.A.; Holland, J.E.; Stopp, C.; White, M.T.; Bellinger, D.C.; Rivkin, M.J.; Wypij, D.; Newburger, J.W. Psychiatric Disorders in Adolescents with Single Ventricle Congenital Heart Disease. Pediatrics 2017, 139, e20162241. [Google Scholar] [CrossRef] [Green Version]
- Bellinger, D.C.; Watson, C.G.; Rivkin, M.J.; Robertson, R.L.; Roberts, A.E.; Stopp, C.; Dunbar-Masterson, C.; Bernson, D.; DeMaso, D.R.; Wypij, D.; et al. Neuropsychological Status and Structural Brain Imaging in Adolescents with Single Ventricle Who Underwent the Fontan Procedure. J. Am. Heart Assoc. 2015, 4, e002302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sananes, R.; Goldberg, C.S.; Newburger, J.W.; Hu, C.; Trachtenberg, F.; Gaynor, J.W.; Mahle, W.T.; Miller, T.; Uzark, K.; Mussatto, K.A.; et al. Six-Year Neurodevelopmental Outcomes for Children with Single-Ventricle Physiology. Pediatrics 2021, 147, e2020014589. [Google Scholar] [CrossRef]
- Goldberg, C.S.; Hu, C.; Brosig, C.; Gaynor, J.W.; Mahle, W.T.; Miller, T.; Mussatto, K.A.; Sananes, R.; Uzark, K.; Trachtenberg, F.; et al. Behavior and Quality of Life at 6 Years for Children with Hypoplastic Left Heart Syndrome. Pediatrics 2019, 144, e20191010. [Google Scholar] [CrossRef]
- Sanz, J.H.; Berl, M.; Ma, A.C.A.; Wang, J.; Cheng, Y.I.; Donofrio, M.T. Prevalence and pattern of executive dysfunction in school age children with congenital heart disease. Congenit. Heart Dis. 2017, 12, 202–209. [Google Scholar] [CrossRef] [Green Version]
- Holm, I.; Fredriksen, P.M.; Fosdahl, M.A.; Olstad, M.; Vøllestad, N. Impaired Motor Competence in School-aged Children with Complex Congenital Heart Disease. Arch. Pediatr. Adolesc. Med. 2007, 161, 945–950. [Google Scholar] [CrossRef] [Green Version]
- Limperopoulos, C.; Majnemer, A.; Shevell, M.I.; Rosenblatt, B.; Rohlicek, C.; Tchervenkov, C.; Darwish, H. Functional limitations in young children with congenital heart defects after cardiac surgery. Pediatrics 2001, 108, 1325–1331. [Google Scholar] [CrossRef] [PubMed]
- Cheatham, S.L.; Carey, H.; Chisolm, J.L.; Heathcock, J.C.; Steward, D. Early Results of Neurodevelopment Following Hybrid Stage I for Hypoplastic Left Heart Syndrome. Pediatr. Cardiol. 2014, 36, 685–691. [Google Scholar] [CrossRef]
- Cassidy, A.R.; White, M.T.; DeMaso, D.R.; Newburger, J.W.; Bellinger, D.C. Executive Function in Children and Adolescents with Critical Cyanotic Congenital Heart Disease. J. Int. Neuropsychol. Soc. 2015, 21, 34–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunbar-Masterson, C.; Wypij, D.; Bellinger, D.C.; Rappaport, L.A.; Baker, A.L.; Jonas, R.A.; Newburger, J.W. General Health Status of Children with d-Transposition of the Great Arteries after the Arterial Switch Operation. Circulation 2001, 104, I-138. [Google Scholar] [CrossRef]
- Hövels-Gürich, H.H.; Konrad, K.; Skorzenski, D.; Herpertz-Dahlmann, B.; Messmer, B.J.; Seghaye, M.-C. Attentional Dysfunction in Children after Corrective Cardiac Surgery in Infancy. Ann. Thorac. Surg. 2007, 83, 1425–1430. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Harrison, T.; Heathcock, J. Infants with complex congenital heart diseases show poor short-term memory in the mobile paradigm at 3 months of age. Infant Behav. Dev. 2015, 40, 12–19. [Google Scholar] [CrossRef]
- Homsy, J.; Zaidi, S.; Shen, Y.; Ware, J.S.; Samocha, K.E.; Karczewski, K.J.; DePalma, S.R.; McKean, D.; Wakimoto, H.; Gorham, J.; et al. De novo mutations in congenital heart disease with neurodevelopmental and other congenital anomalies. Science 2015, 350, 1262–1266. [Google Scholar] [CrossRef] [Green Version]
- Jin, S.C.; Homsy, J.; Zaidi, S.; Lu, Q.; Morton, S.; DePalma, S.R.; Zeng, X.; Qi, H.; Chang, W.; Sierant, M.C.; et al. Contribution of rare inherited and de novo variants in 2871 congenital heart disease probands. Nat. Genet. 2017, 49, 1593–1601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Licht, D.J.; Wang, D.; Silvestre, D.W.; Nicolson, S.C.; Montenegro, L.M.; Wernovsky, G.; Tabbutt, S.; Durning, S.M.; Shera, D.M.; Gaynor, J.W.; et al. Preoperative cerebral blood flow is diminished in neonates with severe congenital heart defects. J. Thorac. Cardiovasc. Surg. 2004, 128, 841–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, G.M.; Brosig, C.L.; Mussatto, K.A.; Tweddell, J.S.; Ghanayem, N.S. Perioperative cerebral oxygen saturation in neonates with hypoplastic left heart syndrome and childhood neurodevelopmental outcome. J. Thorac. Cardiovasc. Surg. 2013, 146, 1153–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, L.; Macgowan, C.; Sled, J.G.; Yoo, S.-J.; Manlhiot, C.; Porayette, P.; Grosse-Wortmann, L.; Jaeggi, E.; McCrindle, B.W.; Kingdom, J.; et al. Reduced Fetal Cerebral Oxygen Consumption Is Associated with Smaller Brain Size in Fetuses with Congenital Heart Disease. Circulation 2015, 131, 1313–1323. [Google Scholar] [CrossRef] [Green Version]
- Moller, J.H.; Taubert, K.A.; Allen, H.D.; Clark, E.B.; Lauer, R.M. Cardiovascular health and disease in children: Current status. A Special Writing Group from the Task Force on Children and Youth, American Heart Association. Circulation 1994, 89, 923–930. [Google Scholar] [CrossRef] [Green Version]
- Andropoulos, D.B.; Hunter, J.V.; Nelson, D.P.; Stayer, S.A.; Stark, A.R.; McKenzie, E.D.; Heinle, J.S.; Graves, D.; Fraser, C.D. Brain immaturity is associated with brain injury before and after neonatal cardiac surgery with high-flow bypass and cerebral oxygenation monitoring. J. Thorac. Cardiovasc. Surg. 2010, 139, 543–556. [Google Scholar] [CrossRef] [Green Version]
- Beca, J.; Gunn, J.K.; Coleman, L.; Hope, A.; Reed, P.W.; Hunt, R.W.; Finucane, K.; Brizard, C.; Dance, B.; Shekerdemian, L.S. New White Matter Brain Injury after Infant Heart Surgery Is Associated with Diagnostic Group and the Use of Circulatory Arrest. Circulation 2013, 127, 971–979. [Google Scholar] [CrossRef] [Green Version]
- Fudulu, D.; Angelini, G. Oxidative Stress after Surgery on the Immature Heart. Oxidative Med. Cell. Longev. 2016, 2016, 1971452. [Google Scholar] [CrossRef] [Green Version]
- Korotcova, L.; Kumar, S.; Agematsu, K.; Morton, P.D.; Jonas, R.A.; Ishibashi, N. Prolonged White Matter Inflammation after Cardiopulmonary Bypass and Circulatory Arrest in a Juvenile Porcine Model. Ann. Thorac. Surg. 2015, 100, 1030–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, E.Z.; Pertsovskaya, V.; Forbes, T.A.; Dupree, J.L.; Gallo, V. Prolonged Environmental Enrichment Promotes Developmental Myelination. Front. Cell Dev. Biol. 2021, 9, 1066. [Google Scholar] [CrossRef] [PubMed]
- Adams-Chapman, I.; Stoll, B.J. Neonatal infection and long-term neurodevelopmental outcome in the preterm infant. Curr. Opin. Infect. Dis. 2006, 19, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Hackman, D.; Farah, M.J.; Meaney, M.J. Socioeconomic status and the brain: Mechanistic insights from human and animal research. Nat. Rev. Neurosci. 2010, 11, 651–659. [Google Scholar] [CrossRef]
- Benavente-Fernandez, I.; Siddiqi, A.; Miller, S.P. Socioeconomic status and brain injury in children born preterm: Modifying neurodevelopmental outcome. Pediatr. Res. 2019, 87, 391–398. [Google Scholar] [CrossRef]
- Lawrence, K.M.; McGovern, P.E.; Mejaddam, A.; Rossidis, A.C.; Baumgarten, H.; Kim, A.; Grinspan, J.B.; Licht, D.; Didier, R.A.; Vossough, A.; et al. Chronic intrauterine hypoxia alters neurodevelopment in fetal sheep. J. Thorac. Cardiovasc. Surg. 2019, 157, 1982–1991. [Google Scholar] [CrossRef] [PubMed]
- You, W.; Andescavage, N.N.; Kapse, K.; Donofrio, M.T.; Jacobs, M.; Limperopoulos, C. Hemodynamic Responses of the Placenta and Brain to Maternal Hyperoxia in Fetuses with Congenital Heart Disease by Using Blood Oxygen–Level Dependent MRI. Radiology 2020, 294, 141–148. [Google Scholar] [CrossRef]
- Nicolaides, K.; Bradley, R.; Soothill, P.; Campbell, S.; Bilardo, C.; Gibb, D. Maternal Oxygen Therapy for Intrauterine Growth Retardation. Lancet 1987, 329, 942–945. [Google Scholar] [CrossRef]
- Liu, G.; Yan, Y.; Shi, B.; Huang, J.; Mu, H.; Li, C.; Chen, H.; Zhu, Z. Benefits of progesterone on brain immaturity and white matter injury induced by chronic hypoxia in neonatal rats. J. Thorac. Cardiovasc. Surg. 2020, 160, e55–e66. [Google Scholar] [CrossRef]
- Hirst, J.J.; Yawno, T.; Nguyen, P.; Walker, D.W. Stress in Pregnancy Activates Neurosteroid Production in the Fetal Brain. Neuroendocrinology 2006, 84, 264–274. [Google Scholar] [CrossRef]
- Yawno, T.; Yan, E.; Walker, D.; Hirst, J. Inhibition of neurosteroid synthesis increases asphyxia-induced brain injury in the late gestation fetal sheep. Neuroscience 2007, 146, 1726–1733. [Google Scholar] [CrossRef]
- Nguyen, P.N.; Billiards, S.S.; Walker, D.W.; Hirst, J.J. Changes in 5α-Pregnane Steroids and Neurosteroidogenic Enzyme Expression in Fetal Sheep with Umbilicoplacental Embolization. Pediatr. Res. 2003, 54, 840–847. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, M.; Liere, P.; Ghoumari, A. Progesterone and fetal-neonatal neuroprotection. Best Pr. Res. Clin. Obstet. Gynaecol. 2020, 69, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Landucci, E.; Filippi, L.; Gerace, E.; Catarzi, S.; Guerrini, R.; Pellegrini-Giampietro, D.E. Neuroprotective effects of topiramate and memantine in combination with hypothermia in hypoxic-ischemic brain injury in vitro and in vivo. Neurosci. Lett. 2018, 668, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Shuaib, A.; Li, Q.; Siddiqui, M.M. Neuroprotection by delayed administration of topiramate in a rat model of middle cerebral artery embolization. Brain Res. 1998, 804, 169–176. [Google Scholar] [CrossRef]
- Follett, P.L.; Deng, W.; Dai, W.; Talos, D.M.; Massillon, L.J.; Rosenberg, P.A.; Volpe, J.J.; Jensen, F.E. Glutamate Receptor-Mediated Oligodendrocyte Toxicity in Periventricular Leukomalacia: A Protective Role for Topiramate. J. Neurosci. 2004, 24, 4412–4420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoover, R.C.; Motta, M.; Davis, J.; Saatman, K.E.; Fujimoto, S.T.; Thompson, H.J.; Stover, J.F.; Dichter, M.A.; Twyman, R.; White, H.S.; et al. Differential Effects of the Anticonvulsant Topiramate on Neurobehavioral and Histological Outcomes following Traumatic Brain Injury in Rats. J. Neurotrauma 2004, 21, 501–512. [Google Scholar] [CrossRef]
- Liu, Y.; Barks, J.D.; Xu, G.; Silverstein, F.S. Topiramate Extends the Therapeutic Window for Hypothermia-Mediated Neuroprotection after Stroke in Neonatal Rats. Stroke 2004, 35, 1460–1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippi, L.; Fiorini, P.; Catarzi, S.; Berti, E.; Padrini, L.; Landucci, E.; Donzelli, G.; Bartalena, L.; Fiorentini, E.; Boldrini, A.; et al. Safety and efficacy of topiramate in neonates with hypoxic ischemic encephalopathy treated with hypothermia (NeoNATI): A feasibility study. J. Matern. Neonatal Med. 2018, 31, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Alkaitis, M.S.; Crabtree, M.J. Recoupling the Cardiac Nitric Oxide Synthases: Tetrahydrobiopterin Synthesis and Recycling. Curr. Heart Fail. Rep. 2012, 9, 200–210. [Google Scholar] [CrossRef] [Green Version]
- Robertson, C.L.; Scafidi, S.; McKenna, M.C.; Fiskum, G. Mitochondrial mechanisms of cell death and neuroprotection in pediatric ischemic and traumatic brain injury. Exp. Neurol. 2009, 218, 371–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blomgren, K.; Hagberg, H. Free radicals, mitochondria, and hypoxia–ischemia in the developing brain. Free Radic. Biol. Med. 2006, 40, 388–397. [Google Scholar] [CrossRef]
- Romanowicz, J.; Leonetti, C.; Dhari, Z.; Korotcova, L.; Ramachandra, S.D.; Saric, N.; Morton, P.D.; Bansal, S.; Cheema, A.; Gallo, V.; et al. Treatment with Tetrahydrobiopterin Improves White Matter Maturation in a Mouse Model for Prenatal Hypoxia in Congenital Heart Disease. J. Am. Heart Assoc. 2019, 8, e012711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, J.H.; Tanaka, K.A. Inflammatory response to cardiopulmonary bypass. Ann. Thorac. Surg. 2003, 75, S715–S720. [Google Scholar] [CrossRef]
- Ando, M.; Park, I.-S.; Wada, N.; Takahashi, Y. Steroid Supplementation: A Legitimate Pharmacotherapy after Neonatal Open Heart Surgery. Ann. Thorac. Surg. 2005, 80, 1672–1678. [Google Scholar] [CrossRef]
- Bronicki, R.A.; Backer, C.L.; Baden, H.P.; Mavroudis, C.; Crawford, S.E.; Green, T.P. Dexamethasone reduces the inflammatory response to cardiopulmonary bypass in children. Ann. Thorac. Surg. 2000, 69, 1490–1495. [Google Scholar] [CrossRef]
- Checchia, P.A.; Backer, C.L.; Bronicki, R.A.; Baden, H.P.; Crawford, S.E.; Green, T.P.; Mavroudis, C. Dexamethasone reduces postoperative troponin levels in children undergoing cardiopulmonary bypass*. Crit. Care Med. 2003, 31, 1742–1745. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, V.A.; Pearl, J.M.; Schwartz, S.; Shanley, T.; Manning, P.B.; Nelson, D.P. Combined Steroid Treatment for Congenital Heart Surgery Improves Oxygen Delivery and Reduces Postbypass Inflammatory Mediator Expression. Circulation 2003, 107, 2823–2828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fudulu, D.P.; Gibbison, B.; Upton, T.; Stoica, S.C.; Caputo, M.; Lightman, S.; Angelini, G.D. Corticosteroids in Pediatric Heart Surgery: Myth or Reality. Front. Pediatr. 2018, 6, 112. [Google Scholar] [CrossRef] [Green Version]
- Graham, E.M.; Martin, R.H.; Buckley, J.R.; Zyblewski, S.C.; Kavarana, M.N.; Bradley, S.M.; Alsoufi, B.; Mahle, W.T.; Hassid, M.; Atz, A.M. Corticosteroid Therapy in Neonates Undergoing Cardiopulmonary Bypass. J. Am. Coll. Cardiol. 2019, 74, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Graham, E.M.; Atz, A.M.; Butts, R.J.; Baker, N.L.; Zyblewski, S.C.; Deardorff, R.L.; DeSantis, S.M.; Reeves, S.T.; Bradley, S.M.; Spinale, F.G. Standardized preoperative corticosteroid treatment in neonates undergoing cardiac surgery: Results from a randomized trial. J. Thorac. Cardiovasc. Surg. 2011, 142, 1523–1529. [Google Scholar] [CrossRef] [Green Version]
- Zyblewski, S.C.; Martin, R.H.; Shipes, V.B.; Hamlin-Smith, K.; Atz, A.M.; Bradley, S.M.; Kavarana, M.N.; Mahle, W.T.; Everett, A.D.; Graham, E.M. Intraoperative Methylprednisolone and Neurodevelopmental Outcomes in Infants after Cardiac Surgery. Ann. Thorac. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Jensen, H.A.; Loukogeorgakis, S.; Yannopoulos, F.; Rimpiläinen, E.; Petzold, A.; Tuominen, H.; Lepola, P.; MacAllister, R.J.; Deanfield, J.; Mäkelä, T.; et al. Remote Ischemic Preconditioning Protects the Brain Against Injury after Hypothermic Circulatory Arrest. Circulation 2011, 123, 714–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, C.; Gao, M.; Dornbos, D.; Ding, Y.; Zeng, X.; Luo, Y.; Ji, X. Remote ischemic post-conditioning reduced brain damage in experimental ischemia/reperfusion injury. Neurol. Res. 2011, 33, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Ren, C.; Gao, X.; Steinberg, G.; Zhao, H. Limb remote-preconditioning protects against focal ischemia in rats and contradicts the dogma of therapeutic time windows for preconditioning. Neuroscience 2008, 151, 1099–1103. [Google Scholar] [CrossRef] [Green Version]
- Gaynor, J.W.; Nicolson, S.C.; Spray, D.M.; Burnham, N.B.; Chittams, J.L.; Sammarco, T.; Walsh, K.W.; Spray, T.L.; Licht, D. Remote Ischemic Preconditioning Does Not Prevent White Matter Injury in Neonates. Ann. Thorac. Surg. 2018, 106, 151–155. [Google Scholar] [CrossRef] [Green Version]
- Zhong, H.; Gao, Z.; Chen, M.; Zhao, J.; Wang, F.; Li, L.; Dong, H.; Liu, L.; Wang, Q.; Xiong, L. Cardioprotective effect of remote ischemic postconditioning on children undergoing cardiac surgery: A randomized controlled trial. Pediatr. Anesth. 2013, 23, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Bernardo, M.E.; Fibbe, W.E. Mesenchymal Stromal Cells: Sensors and Switchers of Inflammation. Cell Stem Cell 2013, 13, 392–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Velthoven, C.T.; Kavelaars, A.; Heijnen, C.J. Mesenchymal stem cells as a treatment for neonatal ischemic brain damage. Pediatr. Res. 2012, 71, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Maeda, T.; Sarkislali, K.; Leonetti, C.; Kapani, N.; Dhari, Z.; Al Haj, I.; Ulrey, R.; Hanley, P.J.; Jonas, R.A.; Ishibashi, N. Impact of Mesenchymal Stromal Cell Delivery Through Cardiopulmonary Bypass on Postnatal Neurogenesis. Ann. Thorac. Surg. 2019, 109, 1274–1281. [Google Scholar] [CrossRef] [PubMed]
- Maeda, T.; Briggs, C.M.; Datar, A.; Brantner, C.A.; Hanley, P.J.; Jonas, R.A.; Ishibashi, N. Influence of administration of mesenchymal stromal cell on pediatric oxygenator performance and inflammatory response. JTCVS Open 2021, 5, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Rangarajan, V.; Juul, S.E. Erythropoietin: Emerging Role of Erythropoietin in Neonatal Neuroprotection. Pediatr. Neurol. 2014, 51, 481–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, H.; Reibel, N.J.; Bührer, C.; Dame, C. Prophylactic Early Erythropoietin for Neuroprotection in Preterm Infants: A Meta-analysis. Pediatrics 2017, 139, e20164317. [Google Scholar] [CrossRef] [Green Version]
- Juul, S.E.; Comstock, B.A.; Wadhawan, R.; Mayock, D.E.; Courtney, S.E.; Robinson, T.; Ahmad, K.; Bendel-Stenzel, E.; Baserga, M.; LaGamma, E.F.; et al. A Randomized Trial of Erythropoietin for Neuroprotection in Preterm Infants. N. Engl. J. Med. 2020, 382, 233–243. [Google Scholar] [CrossRef]
- Andropoulos, D.B.; Brady, K.; Easley, R.B.; Dickerson, H.A.; Voigt, R.G.; Shekerdemian, L.S.; Meador, M.R.; Eisenman, C.A.; Hunter, J.V.; Turcich, M.; et al. Erythropoietin neuroprotection in neonatal cardiac surgery: A phase I/II safety and efficacy trial. J. Thorac. Cardiovasc. Surg. 2013, 146, 124–131. [Google Scholar] [CrossRef] [Green Version]
- Diaz, L.K.; Gaynor, J.W.; Koh, S.J.; Ittenbach, R.F.; Gerdes, M.; Bernbaum, J.C.; Zackai, E.H.; Clancy, R.R.; Rehman, M.A.; Pennington, J.W.; et al. Increasing cumulative exposure to volatile anesthetic agents is associated with poorer neurodevelopmental outcomes in children with hypoplastic left heart syndrome. J. Thorac. Cardiovasc. Surg. 2016, 152, 482–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, G.G.; Robertson, C.M.T.; Alton, G.Y.; Joffe, A.R.; Cave, D.A.; Dinu, I.A.; Creighton, D.E.; Ross, D.B.; Rebeyka, I.M.; The Western Canadian Complex Pediatric Therapies Follow-Up Group. Neurodevelopmental outcome following exposure to sedative and analgesic drugs for complex cardiac surgery in infancy*. Pediatr. Anesth. 2011, 21, 932–941. [Google Scholar] [CrossRef] [PubMed]
- Zuppa, A.F.; Nicolson, S.C.; Wilder, N.S.; Ibla, J.C.; Gottlieb, E.A.; Burns, K.M.; Stylianou, M.; Trachtenberg, F.; Ni, H.; Skeen, T.H.; et al. Results of a phase 1 multicentre investigation of dexmedetomidine bolus and infusion in corrective infant cardiac surgery. Br. J. Anaesth. 2019, 123, 839–852. [Google Scholar] [CrossRef] [PubMed]
- Ming, S.; Xie, Y.; Du, X.; Huang, H.; Fan, Y.; Liang, Q.; Xie, Y. Effect of dexmedetomidine on perioperative hemodynamics and organ protection in children with congenital heart disease. Medicine 2021, 100, e23998. [Google Scholar] [CrossRef]
- Gong, J.; Zhang, R.; Shen, L.; Xie, Y.; Li, X. The brain protective effect of dexmedetomidine during surgery for paediatric patients with congenital heart disease. J. Int. Med. Res. 2019, 47, 1677–1684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, F.; Gastonguay, M.R.; Nicolson, S.C.; DiLiberto, M.; Ocampo-Pelland, A.; Zuppa, A.F. Dexmedetomidine Pharmacology in Neonates and Infants after Open Heart Surgery. Anesth. Analg. 2016, 122, 1556–1566. [Google Scholar] [CrossRef]
- Sonneville, R.; Hertog, H.M.D.; Güiza, F.; Gunst, J.; Derese, I.; Wouters, P.J.; Brouland, J.-P.; Polito, A.; Gray, F.; Chrétien, F.; et al. Impact of Hyperglycemia on Neuropathological Alterations during Critical Illness. J. Clin. Endocrinol. Metab. 2012, 97, 2113–2123. [Google Scholar] [CrossRef] [Green Version]
- Lucas, A.; Morley, R.; Cole, T.J. Adverse neurodevelopmental outcome of moderate neonatal hypoglycaemia. BMJ 1988, 297, 1304–1308. [Google Scholar] [CrossRef] [Green Version]
- Sadhwani, A.; Asaro, L.; Goldberg, C.; Ware, J.; Butcher, J.; Gaies, M.; Smith, C.; Alexander, J.L.; Wypij, D.; Agus, M.S. Impact of Tight Glycemic Control on Neurodevelopmental Outcomes at 1 Year of Age for Children with Congenital Heart Disease: A Randomized Controlled Trial. J. Pediatr. 2016, 174, 193–198.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agus, M.S.; Asaro, L.; Steil, G.M.; Alexander, J.L.; Silverman, M.; Wypij, D.; Gaies, M.G. Tight Glycemic Control after Pediatric Cardiac Surgery in High-Risk Patient Populations. Circulation 2014, 129, 2297–2304. [Google Scholar] [CrossRef] [PubMed]
- Epstein, F.H.; Mccord, J.M. Oxygen-Derived Free Radicals in Postischemic Tissue Injury. N. Engl. J. Med. 1985, 312, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.; Towfighi, J.; Roberts, R.L.; Heitjan, D.F. Allopurinol Administered after Inducing Hypoxia-Ischemia Reduces Brain Injury in 7-Day-Old Rats. Pediatr. Res. 1993, 33, 405–411. [Google Scholar] [CrossRef] [Green Version]
- Gunes, T.; Ozturk, M.A.; Koklu, E.; Kose, K.; Gunes, I. Effect of Allopurinol Supplementation on Nitric Oxide Levels in Asphyxiated Newborns. Pediatr. Neurol. 2007, 36, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Kaandorp, J.J.; Van Bel, F.; Veen, S.; Derks, J.B.; Groenendaal, F.; Rijken, M.; Roze, E.; Venema, M.M.A.U.; Rademaker, C.M.A.; Bos, A.F.; et al. Long-term neuroprotective effects of allopurinol after moderate perinatal asphyxia: Follow-up of two randomised controlled trials. Arch. Dis. Child. Fetal Neonatal. Ed. 2012, 97, F162–F166. [Google Scholar] [CrossRef]
- Sayre, L.M.; Perry, G.; Smith, M.A. Oxidative Stress and Neurotoxicity. Chem. Res. Toxicol. 2008, 21, 172–188. [Google Scholar] [CrossRef] [Green Version]
- Sheu, S.-S.; Nauduri, D.; Anders, M. Targeting antioxidants to mitochondria: A new therapeutic direction. Biochim. Biophys. Acta Mol. Basis Dis. 2006, 1762, 256–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.H.; Matei, N.; Camara, R. Emerging mechanisms and novel applications of hydrogen gas therapy. Med. Gas Res. 2018, 8, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Jia, L.; Chen, B.; Zhang, L.; Liu, J.; Long, J.; Li, Y. Hydrogen Inhalation is Superior to Mild Hypothermia in Improving Cardiac Function and Neurological Outcome in an Asphyxial Cardiac Arrest Model of Rats. Shock 2016, 46, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Cole, A.R.; Perry, D.A.; Raza, A.; Nedder, A.P.; Pollack, E.; Regan, W.L.; Bosch, S.J.V.D.; Polizzotti, B.D.; Yang, E.; Davila, D.; et al. Perioperatively Inhaled Hydrogen Gas Diminishes Neurologic Injury Following Experimental Circulatory Arrest in Swine. JACC Basic Transl. Sci. 2019, 4, 176–187. [Google Scholar] [CrossRef]
- Kajimoto, M.; Nuri, M.; Sleasman, J.R.; Charette, K.A.; Nelson, B.R.; Portman, M.A. Inhaled nitric oxide reduces injury and microglia activation in porcine hippocampus after deep hypothermic circulatory arrest. J. Thorac. Cardiovasc. Surg. 2021, 161, e485–e498. [Google Scholar] [CrossRef]
- Checchia, P.A.; Bronicki, R.A.; Muenzer, J.T.; Dixon, D.; Raithel, S.; Gandhi, S.; Huddleston, C.B. Nitric oxide delivery during cardiopulmonary bypass reduces postoperative morbidity in children—A randomized trial. J. Thorac. Cardiovasc. Surg. 2013, 146, 530–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, C.; Millar, J.; Horton, S.; Brizard, C.; Molesworth, C.; Butt, W. Nitric oxide administration during paediatric cardiopulmonary bypass: A randomised controlled trial. Intensiv. Care Med. 2016, 42, 1744–1752. [Google Scholar] [CrossRef]
- Curvello, V.; Pastor, P.; Hekierski, H.; Armstead, W.M. Inhaled Nitric Oxide Protects Cerebral Autoregulation and Reduces Hippocampal Necrosis after Traumatic Brain Injury Through Inhibition of ET-1, ERK MAPK and IL-6 Upregulation in Pigs. Neurocrit Care 2018, 30, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Uryash, A.; Bassuk, J.; Kurlansky, P.; Giridharan, G.A.; Shakeri, M.; Estrada, R.; Sethu, P.; Adams, J.A. Mechanisms of Periodic Acceleration Induced Endothelial Nitric Oxide Synthase (eNOS) Expression and Upregulation Using an In Vitro Human Aortic Endothelial Cell Model. Cardiovasc. Eng. Technol. 2012, 3, 292–301. [Google Scholar] [CrossRef]
- Endres, M.; Laufs, U.; Liao, J.K.; Moskowitz, M.A. Targeting eNOS for stroke protection. Trends Neurosci. 2004, 27, 283–289. [Google Scholar] [CrossRef]
- Adams, J.A.; Pastuszko, P.; Uryash, A.; Wilson, D.; Padrino, J.R.L.; Nadkarni, V.; Pastuszko, A. Whole Body Periodic Acceleration (pGz) as a non-invasive preconditioning strategy for pediatric cardiac surgery. Med. Hypotheses 2018, 110, 144–149. [Google Scholar] [CrossRef]
- Yu, H.; Shi, L.; Zhao, S.; Sun, Y.; Gao, Y.; Sun, Y.; Qi, G. Triptolide Attenuates Myocardial Ischemia/Reperfusion Injuries in Rats by Inducing the Activation of Nrf2/HO-1 Defense Pathway. Cardiovasc. Toxicol. 2015, 16, 325–335. [Google Scholar] [CrossRef]
- Hao, M.; Li, X.; Feng, J.; Pan, N. Triptolide Protects Against Ischemic Stroke in Rats. Inflammation 2015, 38, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.-L.; Jin, X.-Q.; Ye, F.; Zhao, Y.; Zhang, J.-J. Triptolide attenuates cerebral ischemia and reperfusion injury in rats through the inhibition the nuclear factor kappa B signaling pathway. Neuropsychiatr. Dis. Treat. 2015, 11, 1395–1403. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-F.; Lee, T.-S.; Kou, Y.R. Anti-inflammatory and neuroprotective effects of triptolide on traumatic brain injury in rats. Respir. Physiol. Neurobiol. 2012, 182, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Lei, Y.-Q.; Liu, J.-F.; Wang, Z.-C.; Cao, H. Triptolide improves neurobehavioral functions, inflammation, and oxidative stress in rats under deep hypothermic circulatory arrest. Aging 2021, 13, 3031–3044. [Google Scholar] [CrossRef]
- Romero-Miguel, D.; Lamanna-Rama, N.; Casquero-Veiga, M.; Gómez-Rangel, V.; Desco, M.; Soto-Montenegro, M.L. Minocycline in neurodegenerative and psychiatric diseases: An update. Eur. J. Neurol. 2021, 28, 1056–1081. [Google Scholar] [CrossRef]
- Drabek, T.; Janata, A.; Wilson, C.D.; Stezoski, J.; Janesko-Feldman, K.; Tisherman, S.A.; Foley, L.M.; Verrier, J.D.; Kochanek, P.M. Minocycline attenuates brain tissue levels of TNF-α produced by neurons after prolonged hypothermic cardiac arrest in rats. Resuscitation 2014, 85, 284–291. [Google Scholar] [CrossRef] [Green Version]
- Salameh, A.; Einenkel, A.; Kühne, L.; Grassl, M.; Von Salisch, S.; Kiefer, P.; Vollroth, M.; Dähnert, I.; Dhein, S. Hippocampal Neuroprotection by Minocycline and Epigallo-Catechin-3-Gallate against Cardiopulmonary Bypass-Associated Injury. Brain Pathol. 2015, 25, 733–742. [Google Scholar] [CrossRef]
- Buller, K.M.; Carty, M.L.; Reinebrant, H.; Wixey, J. Minocycline: A neuroprotective agent for hypoxic-ischemic brain injury in the neonate? J. Neurosci. Res. 2009, 87, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Ares, S.; Saenz-Rico, B.; Quero, J.; De Escobar, G.M. Iodine and the Effects on Growth in Premature Newborns: A Focus on the Role of Thyroid Hormones in Neurodevelopment and Growth. In Handbook of Growth and Growth Monitoring in Health and Disease; Springer: New York, NY, USA, 2012. [Google Scholar]
- Calaciura, F.; Mendorla, G.; Distefano, M.; Castorina, S.; Fario, T.; Motta, R.M.; Sava, L.; Delange, F.; Vigneri, R. Childhood IQ measurements in infants with transient congenital hypothyroidism. Clin. Endocrinol. 1995, 43, 473–477. [Google Scholar] [CrossRef]
- Plumpton, K.; Haas, N.A. Identifying infants at risk of marked thyroid suppression post-cardiopulmonary bypass. Intensiv. Care Med. 2005, 31, 581–587. [Google Scholar] [CrossRef]
- Dimmick, S.J.; Badawi, N.; Randell, T. Thyroid hormone supplementation for the prevention of morbidity and mortality in infants undergoing cardiac surgery. Cochrane Database Syst. Rev. 2004, CD004220. [Google Scholar] [CrossRef] [PubMed]
- Bettendorf, M.; Schmidt, K.G.; Grulich-Henn, J.; Ulmer, H.E.; Heinrich, U.E. Tri-iodothyronine treatment in children after cardiac surgery: A double-blind, randomised, placebo-controlled study. Lancet 2000, 356, 529–534. [Google Scholar] [CrossRef]
- Mittnacht, J.; Choukair, D.; Kneppo, C.; Brunner, R.; Parzer, P.; Gorenflo, M.; Bettendorf, M. Long-Term Neurodevelopmental Outcome of Children Treated with Tri-Iodothyronine after Cardiac Surgery: Follow-Up of a Double-Blind, Randomized, Placebo-Controlled Study. Horm. Res. Paediatr. 2015, 84, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soshi, T.; Andersson, M.; Kawagoe, T.; Nishiguchi, S.; Yamada, M.; Otsuka, Y.; Nakai, R.; Abe, N.; Aslah, A.; Igasaki, T.; et al. Prefrontal Plasticity after a 3-Month Exercise Intervention in Older Adults Relates to Enhanced Cognitive Performance. Cereb. Cortex 2021, 31, 4501–4517. [Google Scholar] [CrossRef] [PubMed]
- Wilckens, K.A.; Stillman, C.M.; Waiwood, A.M.; Kang, C.; Leckie, R.L.; Peven, J.C.; Foust, J.E.; Fraundorf, S.H.; Erickson, K.I. Exercise interventions preserve hippocampal volume: A meta-analysis. Hippocampus 2021, 31, 335–347. [Google Scholar] [CrossRef]
- Rovio, S.; Spulber, G.; Nieminen, L.J.; Niskanen, E.; Winblad, B.; Tuomilehto, J.; Nissinen, A.; Soininen, H.; Kivipelto, M. The effect of midlife physical activity on structural brain changes in the elderly. Neurobiol. Aging 2010, 31, 1927–1936. [Google Scholar] [CrossRef]
- Pereira, A.C.; Huddleston, D.E.; Brickman, A.M.; Sosunov, A.A.; Hen, R.; McKhann, G.M.; Sloan, R.; Gage, F.H.; Brown, T.R.; Small, S.A. An in vivo correlate of exercise-induced neurogenesis in the adult dentate gyrus. Proc. Natl. Acad. Sci. USA 2007, 104, 5638–5643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [Green Version]
- de Greeff, J.W.; Bosker, R.J.; Oosterlaan, J.; Visscher, C.; Hartman, E. Effects of physical activity on executive functions, attention and academic performance in preadolescent children: A meta-analysis. J. Sci. Med. Sport 2018, 21, 501–507. [Google Scholar] [CrossRef]
- Dulfer, K.; Duppen, N.; Kuipers, I.M.; Schokking, M.; van Domburg, R.T.; Verhulst, F.C.; Helbing, W.A.; Utens, E.M. Aerobic Exercise Influences Quality of Life of Children and Youngsters with Congenital Heart Disease: A Randomized Controlled Trial. J. Adolesc. Health 2014, 55, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Fourdain, S.; Simard, M.-N.; Dagenais, L.; Materassi, M.; Doussau, A.; Goulet, J.; Gagnon, K.; Prud’Homme, J.; Vinay, M.-C.; Dehaes, M.; et al. Gross Motor Development of Children with Congenital Heart Disease Receiving Early Systematic Surveillance and Individualized Intervention: Brief Report. Dev. Neurorehabilit. 2021, 24, 56–62. [Google Scholar] [CrossRef]
- Dam, J.C.; van, E.-V.; Vlieland, T.P.M.V.; Kuipers, I.M.; Blom, N.A.; Harkel, A.D.J.T. Improvement of physical activity levels in children and adolescents after surgery for congenital heart disease: Preferences and use of physical therapy. Disabil. Rehabil. 2021, 1–8. [Google Scholar] [CrossRef]
- Calderon, J.; Wypij, D.; Rofeberg, V.; Stopp, C.; Roseman, A.; Albers, D.; Newburger, J.W.; Bellinger, D.C. Randomized Controlled Trial of Working Memory Intervention in Congenital Heart Disease. J. Pediatr. 2020, 227, 191–198.e3. [Google Scholar] [CrossRef] [PubMed]
- Klingberg, T.; Fernell, E.; Olesen, J.; Johnson, M.; Gustafsson, P.; Dahlström, K.; Gillberg, C.G.; Forssberg, H.; Westerberg, H. Computerized Training of Working Memory in Children with ADHD-A Randomized, Controlled Trial. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 177–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grunewaldt, K.H.; Løhaugen, G.C.C.; Austeng, D.; Brubakk, A.-M.; Skranes, J. Working Memory Training Improves Cognitive Function in VLBW Preschoolers. Pediatrics 2013, 131, e747–e754. [Google Scholar] [CrossRef] [Green Version]
- Løhaugen, G.C.; Antonsen, I.; Håberg, A.; Gramstad, A.; Vik, T.; Brubakk, A.-M.; Skranes, J. Computerized Working Memory Training Improves Function in Adolescents Born at Extremely Low Birth Weight. J. Pediatr. 2011, 158, 555–561.e4. [Google Scholar] [CrossRef]
- Nampijja, M.; Kizindo, R.; Apule, B.; Lule, S.; Muhangi, L.; Titman, A.; Elliott, A.; Alcock, K.; Lewis, C. The role of the home environment in neurocognitive development of children living in extreme poverty and with frequent illnesses: A cross-sectional study. Wellcome Open Res. 2018, 3, 152. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.; Orton, J.; Anderson, P.; Boyd, R.; Doyle, L. Early developmental intervention programmes provided post hospital discharge to prevent motor and cognitive impairment in preterm infants. Cochrane Database Syst. Rev. 2015, 11, CD005495. [Google Scholar] [CrossRef] [PubMed]
- Greene, M.M.; Patel, A.L.; Meier, P.; Patra, K. Maternal Education Level Predicts Cognitive, Language, and Motor Outcome in Preterm Infants in the Second Year of Life. Am. J. Perinatol. 2016, 33, 738–744. [Google Scholar] [CrossRef] [Green Version]
- Mackes, N.K.; Golm, D.; Sarkar, S.; Kumsta, R.; Rutter, M.; Fairchild, G.; Mehta, M.A.; Sonuga-Barke, E.J.S.; Era Young Adult Follow-Up on behalf of the ERA Young Adult Follow-up team. Early childhood deprivation is associated with alterations in adult brain structure despite subsequent environmental enrichment. Proc. Natl. Acad. Sci. USA 2020, 117, 641–649. [Google Scholar] [CrossRef] [Green Version]
- Bonthrone, A.F.; Chew, A.; Kelly, C.J.; Almedom, L.; Simpson, J.; Victor, S.; Edwards, A.D.; Rutherford, M.A.; Nosarti, C.; Counsell, S.J. Cognitive function in toddlers with congenital heart disease: The impact of a stimulating home environment. Infancy 2021, 26, 184–199. [Google Scholar] [CrossRef] [PubMed]
- Limperopoulos, C.; Majnemer, A.; Shevell, M.I.; Rohlicek, C.; Rosenblatt, B.; Tchervenkov, C.; Darwish, H. Predictors of developmental disabilities after open heart surgery in young children with congenital heart defects. J. Pediatr. 2002, 141, 51–58. [Google Scholar] [CrossRef]
- Forbess, J.M.; Visconti, K.J.; Hancock-Friesen, C.; Howe, R.C.; Bellinger, D.C.; Jonas, R.A. Neurodevelopmental Outcome after Congenital Heart Surgery: Results from an Institutional Registry. Circulation 2002, 106, I-95. [Google Scholar] [CrossRef]
- Atallah, J.; Dinu, I.A.; Joffe, A.R.; Robertson, C.M.T.; Sauve, R.S.; Dyck, J.D.; Ross, D.B.; Rebeyka, I.M.; Western the Western Canadian Complex Pediatric Therapies Follow-Up Group. Two-Year Survival and Mental and Psychomotor Outcomes after the Norwood Procedure. Circulation 2008, 118, 1410–1418. [Google Scholar] [CrossRef]
- Gaynor, J.W.; Stopp, C.; Wypij, D.; Andropoulos, D.B.; Atallah, J.; Atz, A.M.; Beca, J.; Donofrio, M.T.; Duncan, K.; Ghanayem, N.S.; et al. Neurodevelopmental Outcomes after Cardiac Surgery in Infancy. Pediatrics 2015, 135, 816–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Risk factors associated with neurodevelopmental outcomes in congenital heart disease during progressive epochs of brain development. Adapted from Morton et al. Circ Res. 2017.
Figure 1.
Risk factors associated with neurodevelopmental outcomes in congenital heart disease during progressive epochs of brain development. Adapted from Morton et al. Circ Res. 2017.

Figure 2.
In utero cerebral hypoxemia in complex congenital heart defects. Figure shows fetal hemodynamics in representative examples of (A) Normal Fetal Circulation, (B) d-Transposition of the Great Arteries, and (C) Hypoplastic Left Heart Syndrome (Leonetti et al. Trends Neurosci 2019).
Figure 2.
In utero cerebral hypoxemia in complex congenital heart defects. Figure shows fetal hemodynamics in representative examples of (A) Normal Fetal Circulation, (B) d-Transposition of the Great Arteries, and (C) Hypoplastic Left Heart Syndrome (Leonetti et al. Trends Neurosci 2019).

Figure 3.
The current status of neuroprotective treatment for congenital heart disease.


{kind=link}
{kind=link}
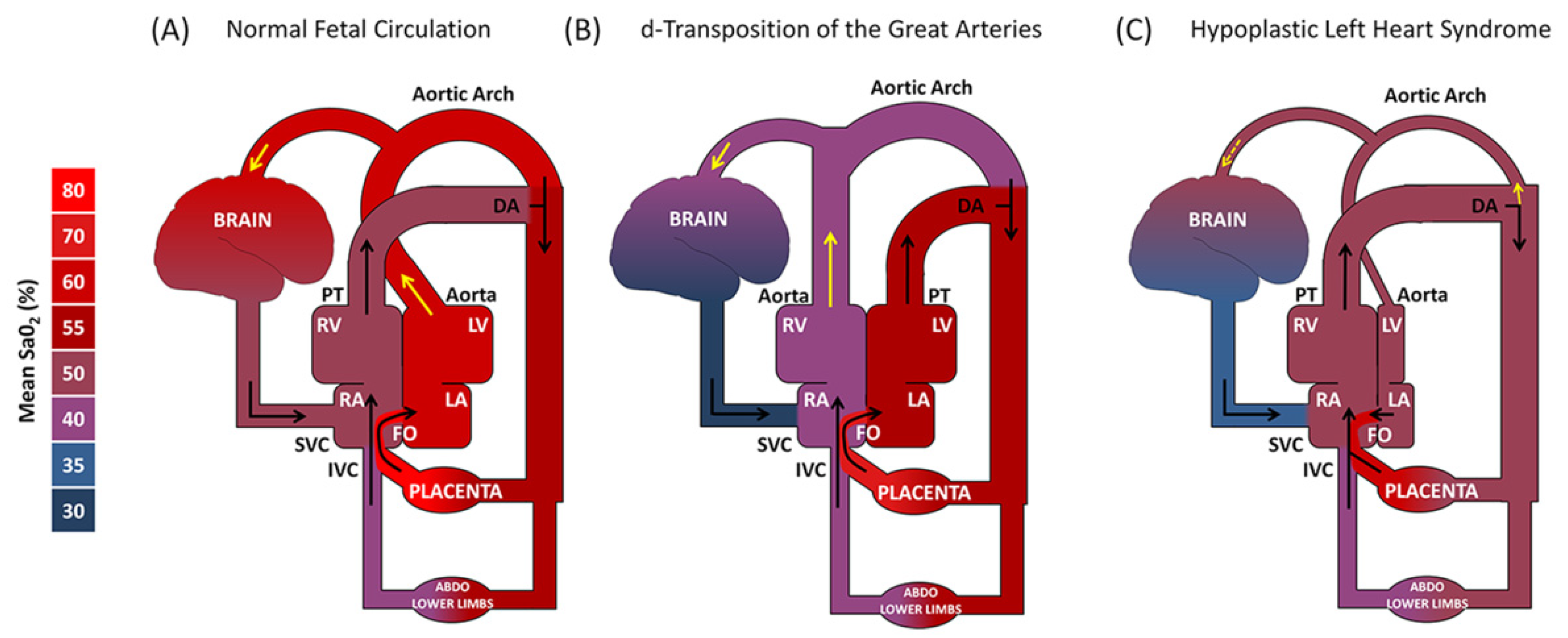{kind=link}
{kind=link}
Table 1.
The current status of neuroprotective treatment for congenital heart disease. n/a, not applicable.
Table 1.
The current status of neuroprotective treatment for congenital heart disease. n/a, not applicable.
| Stage of Patient Care | Type of Study | Treatment | References | Clinical Trial |
|---|---|---|---|---|
| Maternal | Clinical | Maternal Hyperoxia | [45,46,47] | https://clinicaltrials.gov/ct2/show/NCT03944837, accessed on 3 November 2021 |
| Progesterone | [48,49,50,51,52] | https://clinicaltrials.gov/ct2/show/NCT02133573, accessed on 3 November 2021 | ||
| Topiramate Prophylaxis | [53,54,55,56,57,58] | https://clinicaltrials.gov/ct2/show/NCT01426542, accessed on 3 November 2021 | ||
| Pre-clinical | Tetrahydrobiopterine | [59,60,61,62] | n/a | |
| Perioperative | Clinical | Corticosteroids | [63,64,65,66,67,68,69,70,71] | https://clinicaltrials.gov/ct2/show/NCT03229538, accessed on 3 November 2021 |
| Remote Ischemic Preconditioning | [72,73,74,75,76] | https://clinicaltrials.gov/ct2/show/NCT01835392, accessed on 3 November 2021 | ||
| Mesenchymal Stromal Cells | [77,78,79,80] | https://clinicaltrials.gov/ct2/show/NCT04236479, accessed on 3 November 2021 | ||
| Erythropoietin | [81,82,83,84] | n/a | ||
| Dexmedetomidine | [85,86,87,88,89,90] | https://clinicaltrials.gov/ct2/show/NCT02492269, accessed on 3 November 2021 | ||
| https://clinicaltrials.gov/ct2/show/NCT03882788, accessed on 3 November 2021 | ||||
| https://clinicaltrials.gov/ct2/show/NCT02492269, accessed on 3 November 2021 | ||||
| https://clinicaltrials.gov/ct2/show/NCT03366597, accessed on 3 November 2021 | ||||
| https://clinicaltrials.gov/ct2/show/NCT04484922, accessed on 3 November 2021 | ||||
| Tight Glycemic Control | [91,92,93,94] | n/a | ||
| Alloprinol | [95,96,97,98] | https://clinicaltrials.gov/ct2/show/NCT04217421, accessed on 3 November 2021 | ||
| Pre-clinical | Inhaled H2 | [99,100,101,102,103] | n/a | |
| Inhaled Nitric Oxide | [104,105,106,107] | n/a | ||
| Whole Body Periodic Acceleration | [108,109,110] | n/a | ||
| Triptoide | [111,112,113,114,115] | n/a | ||
| Minocycline | [116,117,118,119] | n/a | ||
| Postoperative | Clinical | Triiodothyronine | [120,121,122,123,124,125] | n/a |
| Standardized Exercise Program | [126,127,128,129,130,131,132,133] | https://clinicaltrials.gov/ct2/show/NCT02542683, accessed on 3 November 2021 | ||
| Physical Therapy | [134,135] | n/a | ||
| Cogmed Working Memory Training | [136,137,138,139] | https://clinicaltrials.gov/ct2/show/NCT03023644, accessed on 3 November 2021 | ||
| Early Stimulation | [140,141,142,143] | https://clinicaltrials.gov/ct2/show/NCT04152330, accessed on 3 November 2021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kobayashi, K.; Liu, C.; Jonas, R.A.; Ishibashi, N. The Current Status of Neuroprotection in Congenital Heart Disease. Children 2021, 8, 1116. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121116
AMA Style
Kobayashi K, Liu C, Jonas RA, Ishibashi N. The Current Status of Neuroprotection in Congenital Heart Disease. Children. 2021; 8(12):1116. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121116
Chicago/Turabian StyleKobayashi, Kei, Christopher Liu, Richard A. Jonas, and Nobuyuki Ishibashi. 2021. "The Current Status of Neuroprotection in Congenital Heart Disease" Children 8, no. 12: 1116. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121116
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.