
A Ten-Week Motor Skills Training Program Increases Motor Competence in Children with Developmental Coordination Disorder


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Instrument
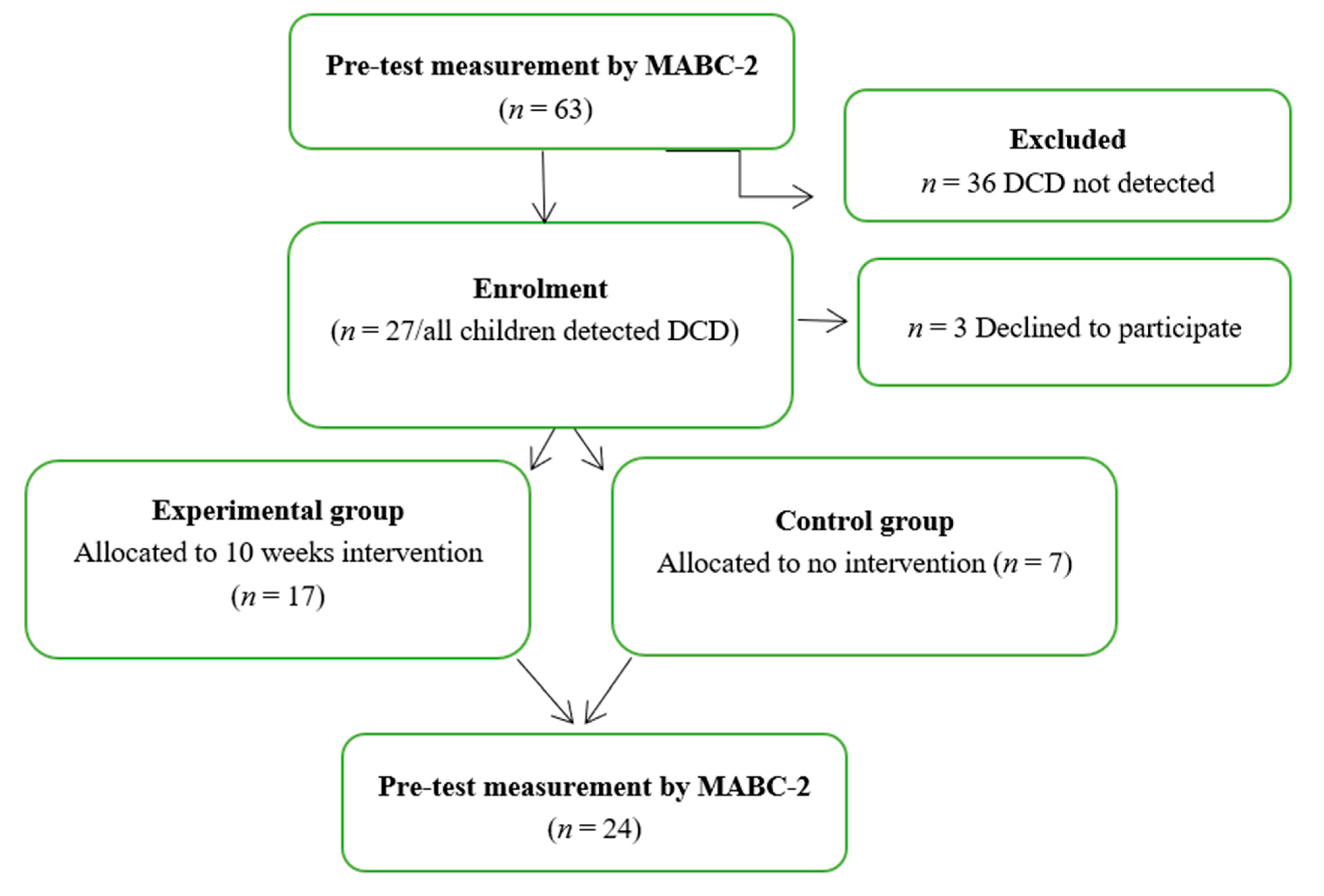
2.3. Procedures
2.4. Data Analysis
3. Results
3.1. Program Effect
3.1.1. Manual Dexterity
3.1.2. Aiming and Catching
3.1.3. Balance
3.1.4. Total Test Score MABC-2
3.2. Gender Effect
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Gaines, R.; Missiuna, C.; Egan, M.; McLean, J. Interprofessional care in the management of a chronic childhood condition: Developmental Coordination Disorder. J. Interprof. Care 2008, 22, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Rivilis, I.; Hay, J.; Cairney, J.; Klentrou, P.; Liu, J.; Faught, B. Physical activity and fitness in children with developmental coordination disorder: A systematic review. Res. Dev. Disabil. 2011, 32, 894–910. [Google Scholar] [CrossRef]
- Haga, M. Physical Fitness in Children With High Motor Competence Is Different From That in Children With Low Motor Competence. Phys. Ther. 2009, 89, 1089–1097. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.; Vinçon, S.; Blank, R.; Quadrado, V.H.; Polatajko, H.; Wilson, P. Evaluating the evidence for motor-based interventions in developmental coordination disorder: A systematic review and meta-analysis. Res. Dev. Disabil. 2018, 74, 72–102. [Google Scholar] [CrossRef]
- Wilson, P.; Larkin, D. New and emerging approaches to understanding developmental coordination disorder. Hum. Mov. Sci. 2008, 27, 171–176. [Google Scholar] [CrossRef]
- Adamchick, J.; Rich, K.M.; Perez, A.M. Self-reporting of risk pathways and parameter values for foot and mouth disease in slaughter cattle from alternative production systems by Kenyan and Ugandan veterinarians. Viruses 2021, 13, 2112. [Google Scholar] [CrossRef]
- Navarro-Patón, R.; Brito-Ballester, J.; Villa, S.; Anaya, V.; Mecías-Calvo, M. Changes in Motor Competence after a Brief Physical Education Intervention Program in 4 and 5-Year-Old Preschool Children. Int. J. Environ. Res. Public Health 2021, 18, 4988. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.J.; Burnett, A.F.; Sit, C.H. Motor Skill Interventions in Children with Developmental Coordination Disorder: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 99, 2076–2099. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.; Blank, R.; Van Der Kaay, A.; Mosterd-Van Der Meijs, R.; Vlugt-Van Den Brand, E.; Polatajko, H.; Wilson, P. Efficacy of interventions to improve motor performance in children with developmental coordination disorder: A combined systematic review and meta-analysis. Dev. Med. Child Neurol. 2013, 55, 229–237. [Google Scholar] [CrossRef]
- Niemeijer, A.S.; Smits-Engelsman, B.C.; Schoemaker, M.M. Neuromotor task training for children with developmental coordination disorder: A controlled trial. Dev. Med. Child Neurol. 2007, 49, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Sugden, D.A.; Chambers, M.E. Intervention in children with Developmental Coordination Disorder: The role of parents and teachers. Br. J. Educ. Psychol. 2003, 73, 545–561. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, M.A.M.; Nevill, A.M.; Buranarugsa, R.; Pereira, S.; Gomes, T.N.Q.F.; Reyes, A.; Barnett, L.M.; Maia, J.A.R. Modeling children’s development in gross motor coordination reveals key modifiable determinants. An allometric approach. Scand. J. Med. Sci. Sports 2018, 28, 1594–1603. [Google Scholar] [CrossRef]
- Reyes, A.C.; Chaves, R.; Baxter-Jones, A.D.G.; Vasconcelos, O.; Barnett, L.M.; Tani, G.; Hedeker, D.; Maia, J. Modelling the dynamics of children’s gross motor coordination. J. Sports Sci. 2019, 37, 2243–2252. [Google Scholar] [CrossRef] [PubMed]
- Hillier, S. Intervention for Children with Developmental Coordination Disorder: A Systematic Review. Internet J. Allied Health Sci. Pract. 2007, 5, 7. [Google Scholar] [CrossRef]
- Nolan, L.; Grigorenko, A.; Thorstensson, A. Balance control: Sex and age differences in 9- to 16-year-olds. Dev. Med. Child Neurol. 2005, 47, 449–454. [Google Scholar] [CrossRef]
- Riach, C.; Starkes, J. Velocity of centre of pressure excursions as an indicator of postural control systems in children. Gait Posture 1994, 2, 167–172. [Google Scholar] [CrossRef]
- Kirshenbaum, N.; Riach, C.; Starkes, J. Non-linear development of postural control and strategy use in young children: A longitudinal study. Exp. Brain Res. 2001, 140, 420–431. [Google Scholar] [CrossRef]
- Kolic, J.; O’Brien, K.; Bowles, K.; Iles, R.; Williams, C.M. Understanding the impact of age, gender, height and body mass index on children’s balance. Acta Paediatr. 2019, 109, 175–182. [Google Scholar] [CrossRef]
- Rodrigues, P.C.; Ribeiro, M.; Sousa, A.; Lopes, S.; Barros, R. Performance on the movement assessment battery for children: A systematic review about gender differences. [Desempeño en la batería de evaluación del movimiento para niños: Una revisión sistemática sobre las diferencias de género]. RICYDE. Rev. Int. Cienc. Deport. 2019, 15, 72–87. [Google Scholar] [CrossRef]
- Henderson, S.E.; Sugden, D.A.; Barnett, A.L. Movement Assessment Battery for Children-2; Harcourt Assessment: London, UK, 2007. [Google Scholar]
- Bardid, F.; Deconinck, F.J.; Descamps, S.; Verhoeven, L.; De Pooter, G.; Lenoir, M.; D’Hondt, E. The effectiveness of a fundamental motor skill intervention in pre-schoolers with motor problems depends on gender but not environmental context. Res. Dev. Disabil. 2013, 34, 4571–4581. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, A.; Toovey, R.; Morgan, P.; Spittle, A.J. Psychometric properties of gross motor assessment tools for children: A systematic review. BMJ Open 2018, 8, e021734. [Google Scholar] [CrossRef]
- Serbetar, I.; Loftesnes, J.M.; Mamen, A. Reliability and Structural Validity of the Movement Assessment Battery for Children-2 in Croatian Preschool Children. Sports 2019, 7, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smits-Engelsman, B.C.M.; Niemeijer, A.S.; Waelvelde, H.V. Is the Movement Assessment Battery for Children-2nd edition a reliable instrument to measure motor performance in 3 year old children? Res. Dev. Disabil. 2011, 32, 1370–1377. [Google Scholar] [CrossRef]
- Ellinoudis, T.; Evaggelinou, C.; Kourtessis, T.; Konstantinidou, Z.; Venetsanou, F.; Kambas, A. Reliability and validi-ty of age band 1 of the Movement Assessment Battery for Children—Second Edition. Res. Dev. Disabil. 2011, 32, 1046–1051. [Google Scholar] [CrossRef] [PubMed]
- Miyahara, M.; Hillier, S.L.; Pridham, L.; Nakagawa, S. Task-oriented interventions for children with developmental co-ordination disorder. Cochrane Database Syst. Rev. 2017, 2017, CD010914. [Google Scholar] [CrossRef]
- Geuze, R.H.; Schoemaker, M.M.; Smits-Engelsman, B.C.M. Clinical and Research Criteria for Developmental Coordination Disorder—Should They Be One and the Same? Curr. Dev. Disord. Rep. 2015, 2, 127–130. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Farhat, F.; Hsairi, I.; Baati, H.; Smits-Engelsman, B.; Masmoudi, K.; Mchirgui, R.; Triki, C.; Moalla, W. The effect of a motor skills training program in the improvement of practiced and non-practiced tasks performance in children with developmental coordination disorder (DCD). Hum. Mov. Sci. 2016, 46, 10–22. [Google Scholar] [CrossRef]
- Caçola, P.; Romero, M.; Ibana, M.; Chuang, J. Effects of two distinct group motor skill interventions in psychological and motor skills of children with Developmental Coordination Disorder: A pilot study. Disabil. Health J. 2015, 9, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Hung, W.; Pang, M. Effects of group-based versus individual-based exercise training on motor performance in children with developmental coordination disorder: A randomized controlled study. J. Rehabil. Med. 2010, 42, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Zanella, L.W.; De Souza, M.S.; Valentini, N. Variáveis que podem explicar mudanças no desempenho motor de crianças com desordem coordenativa desenvolvimental e desenvolvimento típico. J. Phys. Educ. 2018, 29, 2905. [Google Scholar] [CrossRef] [Green Version]
- McGlashan, H.L.; Blanchard, C.C.; Sycamore, N.J.; Lee, R.; French, B.; Holmes, N.P. Improvement in children’s fine motor skills following a computerized typing intervention. Hum. Mov. Sci. 2017, 56, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, G.; Jelsma, D.; Jelsma, J.; Smits-Engelsman, B. The efficacy of two task-orientated interventions for children with Developmental Coordination Disorder: Neuromotor Task Training and Nintendo Wii Fit training. Res. Dev. Disabil. 2013, 34, 2449–2461. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Sit, C.H.P.; Capio, C.M.; Burnett, A.; Ha, A.S.C.; Huang, W.Y.J. Fundamental movement skills proficiency in children with developmental coordination disorder: Does physical self-concept matter? Disabil. Rehabil. 2016, 38, 45–51. [Google Scholar] [CrossRef]
- Wood, G.; Miles, C.A.L.; Coyles, G.; Alizadehkhaiyat, O.; Vine, S.; Vickers, J.N.; Wilson, M.R. A randomized controlled trial of a group-based gaze training intervention for children with Developmental Coordination Disorder. PLoS ONE 2017, 12, e0171782. [Google Scholar] [CrossRef]
- Logan, S.W.; Robinson, L.E.; Wilson, A.E.; Lucas, W.A. Getting the fundamentals of movement: A meta-analysis of the effectiveness of motor skill interventions in children. Child: Care, Health Dev. 2011, 38, 305–315. [Google Scholar] [CrossRef]
- Golding, J.; Emmett, P.; Iles-Caven, Y.; Steer, C.; Lingam, R. A review of environmental contributions to childhood motor skills. J. Child Neurol. 2013, 29, 1531–1547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathisen, G.E. Motor competence and implications in primary school. J. Phys. Educ. Sport 2016, 16, 206–209. [Google Scholar]
- Venter, A.; Pienaar, A.E.; Coetzee, D. Extent and nature of motor difficulties based on age, ethnicity, gender and socio-economic status in a selected group of three-to five-year-old children. S. Afr. J. Res. Sport. Phys. Educ. Recreat. 2015, 37, 169–183. [Google Scholar]
- Valentini, N.C.; Coutinho, M.T.C.; Pansera, S.M.; dos Santos, V.A.P.; Vieira, J.L.L.; Ramalho, M.H.; de Oliveira, M.A. Prevalência de déficits motores e desordem coordenativa desenvolvimental em crianças da região Sul do Brasil. Rev. Paul. Pediatr. 2012, 30, 377–384. [Google Scholar] [CrossRef]
- Kokštejn, J.; Musálek, M.; Tufano, J.J. Are sex differences in fundamental motor skills uniform throughout the entire preschool period? PLoS ONE 2017, 12, e0176556. [Google Scholar] [CrossRef]
- Freitas, C.; Vasconcelos, M.O.; Botelho, M. Handedness and developmental coordination disorder in Portuguese children: Study with the M-ABC test. Laterality 2014, 19, 655–676. [Google Scholar] [CrossRef] [PubMed]
- Psotta, R.; Hendl, J. Movement Assessment Battery for Children—Second edition: Cross-cultural comparison between 11–15 year old children from the Czech Republic and the United Kingdom. Acta Gymnica 2012, 42, 7–16. [Google Scholar] [CrossRef]
- Olesen, L.G.; Kristensen, P.L.; Ried-Larsen, M.; Grøntved, A.; Froberg, K. Physical activity and motor skills in children attending 43 preschools: A cross-sectional study. BMC Pediatr. 2014, 14, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Experimental Group (n = 17) | Control Group (n = 7) | |
|---|---|---|
| Age year, mean (SD) | 5.47 ± 0.514 | 4.71 ± 0.756 |
| Gender (m/f) | 10/7 | 4/3 |
| Manual preference (R/L) | 15/2 | 5/2 |
| MABC-2 Total Score | 5.76 ± 1.39 | 5.29 ± 1.11 |
| Domain | Examples of Activities |
|---|---|
| Manual Dexterity | Placing small beads on the side by plastic clamps Sorting and placing small products of different types with fingers Passing the lacing through the marked holes Hanging nuts on the bolts Hang the plastic clamps in the specified direction To tie clothing buttons Putting the buttons on the marked line Browsing a book and other similar games |
| Aiming and Catching | Catching three different balls (Robo-ball, tennis ball, football ball) Throwing three different balls to designated areas (Robo-ball, tennis ball, football ball) Bowling with twist Ping Pong Ball Catch (Get out those plastic red Solo cups and a few Ping-Pong balls) Bowling (Set up your bowling “lane” with some painter’s tape and use plastic bottles or cups for pins) Different delays and other similar games |
| Balance | Walk on the marked line Picking up items“Night and morning” (when “night” is said, jump into a circle, and when “morning” is said, jump out of the circle) Book balance game (Holding a book on the head without dropping it) Different delays and other similar games |
| Motor Difficulty Category, n | Experimental Group (n = 17) | Control Group (n = 7) | ||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| No motor difficulty (MABC-2 > 16th percentile) | 0 | 17 | 0 | 1 |
| At risk of DCD (from 6th–16th percentile) | 11 | 0 | 3 | 1 |
| Probable DCD (MABC-2 ≤ 5th percentile) | 6 | 0 | 4 | 5 |
| MABC-2 | Group | Mean ± SD | p | η2 |
|---|---|---|---|---|
| Manual Dexterity | Experimental group Control group | 7.76 ± 2.25 4 ± 1.73 | 0.001 | 0.471 |
| Aiming and Catching | Experimental group Control group | 13.9 ± 2.24 9.3 ± 3.35 | 0.003 | 0.317 |
| Balance | Experimental group Control group | 11.1 ± 1.96 6.0 ± 1.63 | 0.920 | 0.626 |
| Total Test Score | Experimental group Control group | 81.6 ± 5.911 51.43 ± 11.85 | 0.524 | 0.759 |
| Experimental Group | Control Group | ||||
|---|---|---|---|---|---|
| MABC-2 | Mean ± SD | p | Mean ± SD | p | |
| Manual Dexterity | Pre-test Post-test | 3.82 ± 1.18 7.76 ± 2.25 | 0.001 | 4.86 ± 1.86 4.00 ± 1.73 | 0.059 |
| Aiming and Catching | Pre-test Post-test | 9.47 ± 2.80 13.18 ± 2.24 | 0.002 | 8.29 ± 2.69 9.29 ± 3.35 | 0.674 |
| Balance | Pre-test Post-test | 8.00 ± 2.34 11.12 ± 1.96 | 0.001 | 7.00 ± 2.30 6.00 ± 1.63 | 0.399 |
| Total Percentile Rank | Pre-test Post-test | 5.76 ± 1.39 10.65 ± 1.53 | 0.001 | 5.29 ± 1.11 4.71 ± 1.89 | 0.459 |
| Experimental Group | Control Group | ||||
|---|---|---|---|---|---|
| MABC-2 | Gender | Mean ± SD | p | Mean ± SD | p |
| Manual Dexterity | Male Female | 3.90 ± 1.28 3.71 ± 1.11 | 0.887 | 5.50 ± 1.73 4.00 ± 2.00 | 0.400 |
| Aiming and Catching | Male Female | 9.80 ± 2.48 9.00 ± 3.36 | 0.536 | 8.50 ± 0.577 8.00 ± 4.58 | 1.000 |
| Balance | Male Female | 8.20 ± 2.39 7.71 ± 2.43 | 0.669 | 6.75 ± 1.89 7.33 ± 3.21 | 1.000 |
| Total Test Score | Male Female | 58.6 ± 9.45 56.2 ± 8.57 | 0.536 | 56.7 ± 4.57 53.6 ± 8.08 | 0.629 |
| Experimental Group | Control Group | ||||
|---|---|---|---|---|---|
| MABC-2 | Gender | Mean ± SD | p | Mean ± SD | p |
| Manual Dexterity | Male Female | 7.80 ± 2.56 7.71 ± 2.56 | 0.813 | 4.00 ± 1.82 4.00 ± 2.00 | 1.000 |
| Aiming and Catching | Male Female | 12.9 ± 2.07 13.5 ± 2.57 | 0.669 | 9.25 ± 3.94 9.33 ± 3.21 | 1.000 |
| Balance | Male Female | 11.1 ± 1.96 11.1 ± 2.11 | 1.000 | 5.50 ± 1.91 6.67 ± 1.15 | 0.400 |
| Total Test Score | Male Female | 81.9 ± 7.18 81.1 ± 3.93 | 0.887 | 49.5 ± 16.0 54.0 ± 4.35 | 0.629 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saidmamatov, O.; Raximov, Q.; Rodrigues, P.; Vasconcelos, O. A Ten-Week Motor Skills Training Program Increases Motor Competence in Children with Developmental Coordination Disorder. Children 2021, 8, 1147. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121147
Saidmamatov O, Raximov Q, Rodrigues P, Vasconcelos O. A Ten-Week Motor Skills Training Program Increases Motor Competence in Children with Developmental Coordination Disorder. Children. 2021; 8(12):1147. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121147
Chicago/Turabian StyleSaidmamatov, Orifjon, Quvondiq Raximov, Paula Rodrigues, and Olga Vasconcelos. 2021. "A Ten-Week Motor Skills Training Program Increases Motor Competence in Children with Developmental Coordination Disorder" Children 8, no. 12: 1147. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121147