1. Introduction
The transition from enteral to autonomous oral feeding is a fundamental concern for both parents and caregivers, since it is a determinant for the length of a preterm neonate’s hospital stay. Premature infants (<37 weeks GA) are at risk of feeding difficulties and have a delay in achieving oral food intake autonomy, especially in the context of prolonged artificial nutrition [
1]. Oral feeding requires a coordination of sucking, swallowing, and breathing. This coordination is not mature until 32 weeks GA [
2]. In a hospital setting, it is the coordination of sucking in conjunction with swallowing and respiratory control that will ultimately lead to the learning of oral feeding in a safe and effective manner [
3].
A distinction is made between nutritive sucking (NS) when ingesting milk, and non-nutritive sucking (NNS) without the ingestion of liquid (nipple or dummy). NNS provides certain benefits that are not directly related to the acquisition of oral feeding [
4,
5]. These include promoting weight gain, producing an analgesic effect, reducing stress, stabilizing the child’s behavior and accelerating the progression of oral nutrition. Additionally, it is a good marker of the level of maturation of sucking itself. Factors that to help promote the maturation of NNS include oral stimulation through NNS or sensorimotor stimulation of the oral structures, performed during enteral feeding of clinically stable premature infants over 30 weeks GA [
6].
Early interventions in NICU are essentially based on two main axes: traditional educational intervention strategies and neuroprotective strategies of various kinds. The NIDCAP program grew out of Brazelton’s work on newborn competence, which was continued by Ashbaugh [
7]. It is an early developmental care program integrated into daily medical care and individualized through behavioral observations focused on the child and family. It aims to promote the harmonious development of the child in its various components: physiological, neurological, behavioral and relational and to improve the future quality of life. The QUALIN questionnaire was used in our study as a hetero-assessment of quality of life [
8]. Research shows that prematurely born children’s development takes place more in a multi-sensory dynamic rather than single-sensory stimulation. Weekly parent-administered massage therapy, when combined with visual interactions between the parents and children, result in a more rapid acquisition of food autonomy. There is often a two-fold increase in breastfeeding rates at discharge, including reduced maternal stress, and a likely increase in breastfeeding efficiency [
9,
10,
11], suggest that vagal stimulation resulting from combined tactile and kinesthetic stimulation allows an increase in gastric motility, which leads to an increase in weight gain. In addition, multisensory intervention (auditory, visual, tactile, and vestibular) stimulates brain development by modifying the cerebral structure of the child. This allows the maturation of food capacities by increasing the number of sucks and the average number of sucks per burst, after performing this intervention after 32 weeks of GA corrected age, in newborns between 29 and 34 weeks of age [
12,
13].
Finally, three studies compared multimodal and unimodal stimulation and suggested: (1) that a combined oral and tactile stimulation program would be more effective than a tactile stimulation program alone, for the duration of acquisition of food autonomy, weight gain, and length of hospital stay for premature infants [
14]; (2) multimodal oral, tactile and kinesthetic stimulation would improve food efficiency compared to unimodal stimulation: oral or tactile/kinesthetic [
15]; and (3) multimodal stimulation by NNS and auditory stimulation would shorten the transition period between autonomous enteral and oral feeding as compared to NNS alone [
16]. This phenomenon could be explained by the synergistic effect of multimodal stimulation on food parameters.
In 2002, Fucile et al. reported that there was a more rapid acquisition of food autonomy after 10 days of unimodal oral stimulation, with no differences found on the duration of hospitalization [
17]. Recently, a review of the Cochrane library [
18] suggested a decrease in the transition time to autonomous oral feeding and a shorter hospital stay with NNS.
However, to our knowledge, there are no studies that have found any effect on the presence of cardio-respiratory events while improving food autonomy or weight gain. However, studies are methodologically heterogeneous, thus making it difficult to interpret the results. This calls into question the usefulness of these interventions in current practice.
Our study’s objectives were to evaluate if early NNS unimodal orofacial stimulation (OFS) reduces apnea–bradycardia and/or desaturations, and improves food autonomy in very premature infants.
2. Methods
2.1. Design
This study was monocentric, controlled, open, and randomized into two groups. Recruitment was prospective. The experimental group was represented by newborns receiving OFS associated with enteral nutrition, based on a program inspired by Fucile [
6,
16]. The control group corresponded to newborns having enteral feeding without receiving any OFS. Both groups received NNS from a pacifier.
2.2. Ethics Approval and Consent to Participate
The protocol was approved by the institutional ethics committee and by the French Protection Committee (N° IDRCB 2009-A01191-56, 1 January 2010), by the French National Institution of Pharmacovigilance (ANSM, Agence Nationale de Sécurité du Médicament et des produits de santé) (27 November 2009). Informed consent was obtained once the information leaflet was reviewed by the parents or legal representatives of the children. Participants were advised they could withdraw their consent at any time, and that the data would be kept confidential.
The ClinicalTrials.gov identifier is NCT01116765.
2.3. Sample
This centrally administered trial was conducted in a level 3 maternity unit in Marseille, France, and included neonates born between January 2013 and December 2014. In the study hospital, there are 2700 live births per year, 8% of which are preterm births (1.9% very preterm birth).
The inclusion criteria were:
- (1)
Neonate born between 26 and 29 completed week GA;
- (2)
Less or equal 33 week GA corrected age (CA);
- (3)
Hospitalized in our neonatal unit;
- (4)
Without neurological pathologies; confirmed by a normal transfontanellar ultrasound or grade 1 or 2 intraventricular hemorrhage [
19], as well as a normal cerebral MRI (performed at corrected-term age) or type 1 to 6 brain abnormalities according to the modified Paneth classification [
20] (in Paneth’s modified classification, six types of MRI are outlined: (1) normal MRI; (2) localized abnormality of white matter; (3) non-parenchymal hemorrhage: subependymal and intraventricular; (4) delay in myelination; (5) diffuse abnormality of white matter; and (6) other lesions: basal ganglia, cerebellum. MRI results were divided into two stages of severity: Group I with normal MRI or moderate abnormalities (Types 1, 2, 3, and 4) and Group II with severe abnormalities (Types 5 and 6));
- (5)
Well-tolerated enteral feeding (without clinical symptoms suggestive of necrotizing enterocolitis defined by abdominal distension and/or increased gastric residuals (>20% of enteral feeding volume) and/or blood in stools (macro- or microscopic), greater than 100 mL/kg/day;
- (6)
Without infectious pathologies making them clinically unstable (reactive C protein less than 7 mg/L);
- (7)
Any CPAP (control positive airway pressure) for at least 48 h;
- (8)
Had no congenital anomalies;
- (9)
Both parents and their legal representatives agreed to participate in the study and signed an informed consent.
The exclusion criteria were: (1) children for whom one of the parents/legal guardians had withdrawn consent before the end of the study; (2) children with co-morbidity during the stimulation period requiring the sessions to be stopped (nosocomial infection and/or ulcerative-necrotizing enteritis and/or respiratory worsening requiring cessation of feeding and/or resumption of CPAP and/or an intensive care admission; (3) children transferred to another establishment before the end of the program; (4) children whose program sequence was not fully completed; and (5) deceased children.
The total duration of inclusion was set at 18 months.
In our NICU, the standard of care protocol is:
- -
Initiation of enteral feeding: from the first few days of life, for all newborns;
- -
Rate of increase in feeding;
- -
Birth weight < 10th percentile, Weight < 1000 g, Preterm < 28 GA: start with digestive stimulation (same 20 mL/kg/d for 3–5 days); after digestive stimulation if well tolerated, increase enteral feeding by 20–25 mL/kg/d daily;
- -
For eutrophic newborn and weight >1000 g: start at 20 mL/kg/d: if well tolerated, increase enteral feeding by 30–35 mL/kg/D daily.
The start of active feeding, for newborns born <33 weeks GA, is 33 weeks CA.
2.4. Intervention
The program included 10 consecutive days of OFS for the very preterm newborns, before 33 weeks GA corrected age. Twice a day, for 10 consecutive days, a 15 to 20 min sensorimotor tactile stimulation was performed 15 to 30 min before feeding by gastric tube. The caretaker performed careful handwashing and gloving prior to each session. The first 12 min of stimulation involved the cheeks, lips, gums and tongue, and the last 3 min consisted of suction stimulation (NNS).
The children were calm and awake in either their crib or incubator and placed in a semi-seated position. The pediatric nurse or parent supported the child’s head and assumed an enveloping and secure position. No stimulation was performed if the child was in deep sleep, or if they showed signs of discomfort or fatigue. This was evaluated by nurses who had been trained in NIDCAP development care and used the Newborn Individualized Developmental Care and Assessment Program (NIDCAP) grid [
21,
22].
2.5. Measurements
The primary endpoint was the assessment of apnea–bradycardia (with or without associated desaturations). Apnea–bradycardia with or without desaturation corresponded to a respiratory pause >10 s associated with bradycardia <80 beats per minute, associated, or not, with desaturation <80–85% in pulse oximetry. An isolated desaturation corresponded to an oxygen saturation <90%. The monitoring of the cardio-respiratory manifestations of the children of the two groups was carried out from their inclusion in the study to discharge from the neonatology department. The vital constants were assessed in real time or by retrospectively analyzing traces recorded by the scope. Cardio-respiratory events were recorded 30 min before, during, and three hours after each feeding.
The secondary objectives included outcomes variables (impact of early NNS unimodal OFS) were:
- -
Evaluation of isolated desaturations during the learning period towards food autonomy with an analysis at four different times: (1) at the first autonomous feeding; (2) up to four independent feedings; (3) up to eight independent feedings on 2 consecutive days; and (4) and then all these autonomous feedings combined.
- -
A validation of our OFS protocol by evaluating its tolerance and listing the cardio-respiratory manifestations (apneas, bradycardias, and desaturations at all feeds from day 1 to day 10 of the stimulation program, always 30 min before, during and in the hour after feeding).
- -
The acquisition of food autonomy, which was defined when the newborn achieved eight independent feedings for two consecutive days.
- -
The date of the first autonomous feeding.
- -
The amount of milk ingested (mL/d).
- -
Weight increase (g/kg/d).
- -
The length of hospital stay.
- -
Dietary monitoring at six months corrected age.
- -
The quality of life of the child, assessed by the parents, using the QUALIN questionnaire [
8], at 6 and 12 months of corrected age.
3. Statistical Analyses
Randomization was established using the OLAN procedure (SAS software), in order to divide the participants into two parallel and comparable groups. Data analyses were performed using SPSS version 20.0 software. The qualitative variables were presented in the form of percentages and the quantitative variables were in the form of mean ± standard deviation. The normality of the distributions of the quantitative data was systematically sought using the Shapiro–Wilks test. If several variables were not normally distributed, usual transformation techniques (logarithmic, etc.) or normalization algorithms (Blom or Tukey algorithms) were used to measure the interpretation of the results that resulted.
The statistical tests used were: The Student’s test or the non-parametric Mann–Whitney test for comparing means, the median test, Chi2 test or Fisher’s exact test for qualitative variables All tests were bilateral. The median and the mean were similar for all quantitative variables.
The number of subjects required was calculated for the main composite criterion: the number of apnea–bradycardias (with or without associated desaturations) and the number of desaturations. To highlight a decrease of at least two apnea–bradycardias or two desaturations during the four different times of autonomous feedings, it was evaluated with 21 patients per group with a risk of error of α = 0.05 and an expected power of 80%. The significance threshold was fixed at p = 0.05 in a bilateral situation.
The primary and secondary endpoint analyses were done on an intention-to-treat basis. The multivariate analyses consisted of modeling the primary and secondary endpoints, according to the two study groups, with parameters: gestational age, birth weight, and total ventilation time (invasive and non-invasive).
4. Results
4.1. Characteristic of Sample
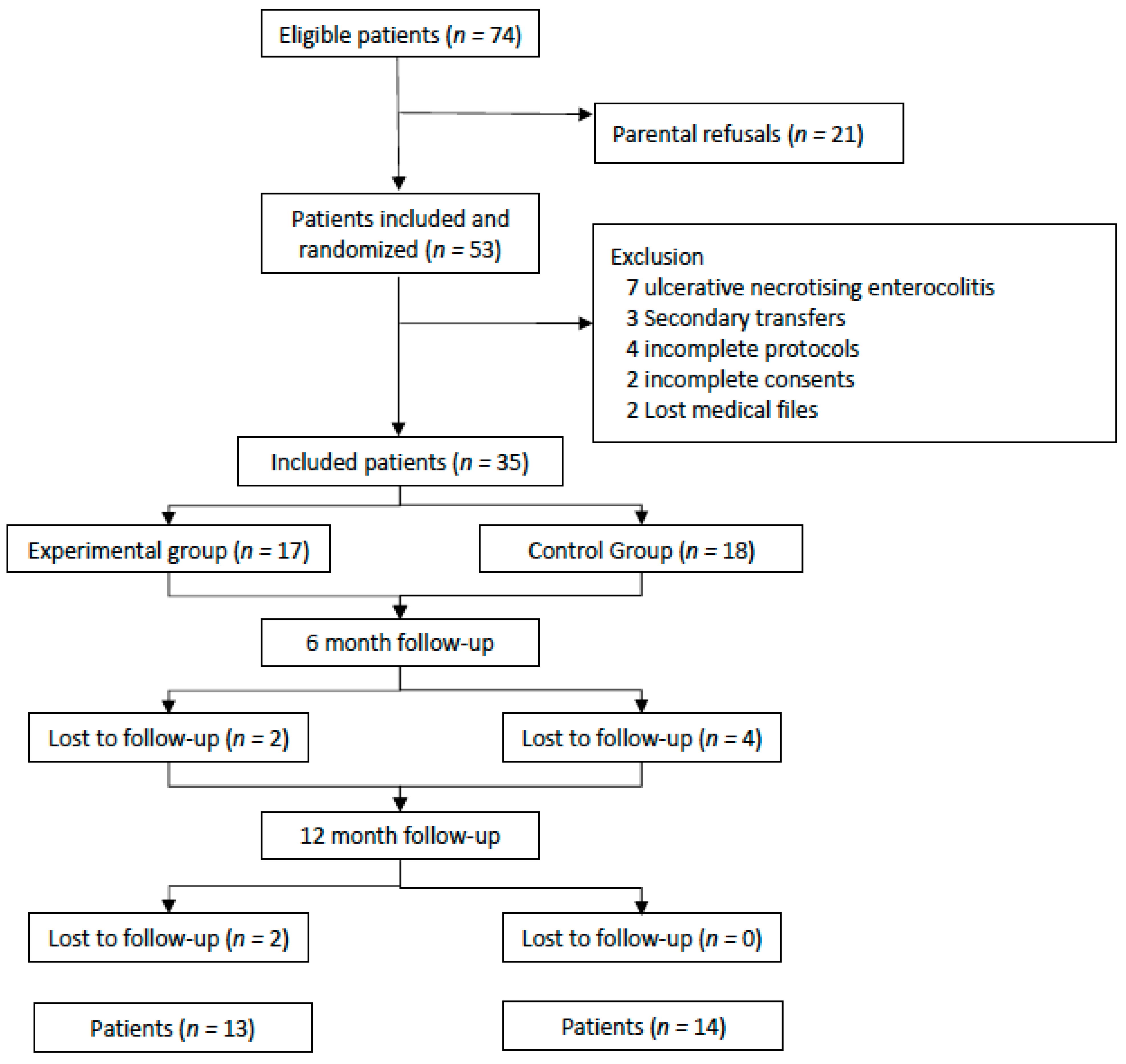
There were 53 patients included and they were randomized. Of the 35 who were not excluded, 17 were in the experimental group with OFS and 18 were in the control group without OFS.
During the 12-month follow-up, eight patients were lost to follow-up: four from the experimental group and four from the control group (
Figure 1).
There were 11 boys (64.7%) in the “with OFS” group and nine boys (50%) in the “without OFS” group. The mean term of birth was 28 weeks GA in the two groups. The average birth weight was 1101 g in the experimental group and 1047 g in the control group.
The baseline age at inclusion was 16.5 days (30 weeks GA and 2 days corrected age) in the experimental group, and 18 days, (30 weeks GA and 4 days corrected age) in the control group. There were no significant differences between the two groups, and both groups were comparable in terms of all their antenatal, neonatal, and postnatal characteristics (
Table 1).
4.2. Primary Objective
The cardio-respiratory manifestations were significantly lower in the experimental group compared with the control group (respectively
n = 102 vs.
n = 61,
p = 0.003) but the differences observed between the two groups were no longer significant (
p = 0.39) after adjustment for gestational age, birth weight, and total duration of ventilation. There were no statistically significant differences between the two groups when detailing apnea–bradycardia with or without associated desaturations (
Table 2).
4.3. Secondary Objectives
There were no statistically significant differences between the two groups concerning isolated desaturations during the four different times of the analysis (1, 4, and 8 autonomous feedings or all these feedings combined (
Table 2)).
There appeared to be no intolerance to the OFS protocol. The weight gain in both groups appeared similar.
Although not significant (
p = 0.70), the experimental group’s infants had a higher weight when discharged (2877 (±366) g) than the control group (2821 (±474) g). The total hospital stay length was shorter in the OFS group than the control group (respectively, 76.18 (±15.88) days vs. 78.72 (±17.67) days,
p = 0.66) (
Table 3).
The completion date for the eight autonomous feedings, continuing for 48 consecutive hours, which represented the date of acquisition of food autonomy, was earlier in the experimental group (corrected age of 36.41 (±1.06) weeks GA) than in the control group (36.78 (±1.44) weeks GA), but the difference was not significant (
p = 0.40) (
Figure 2).
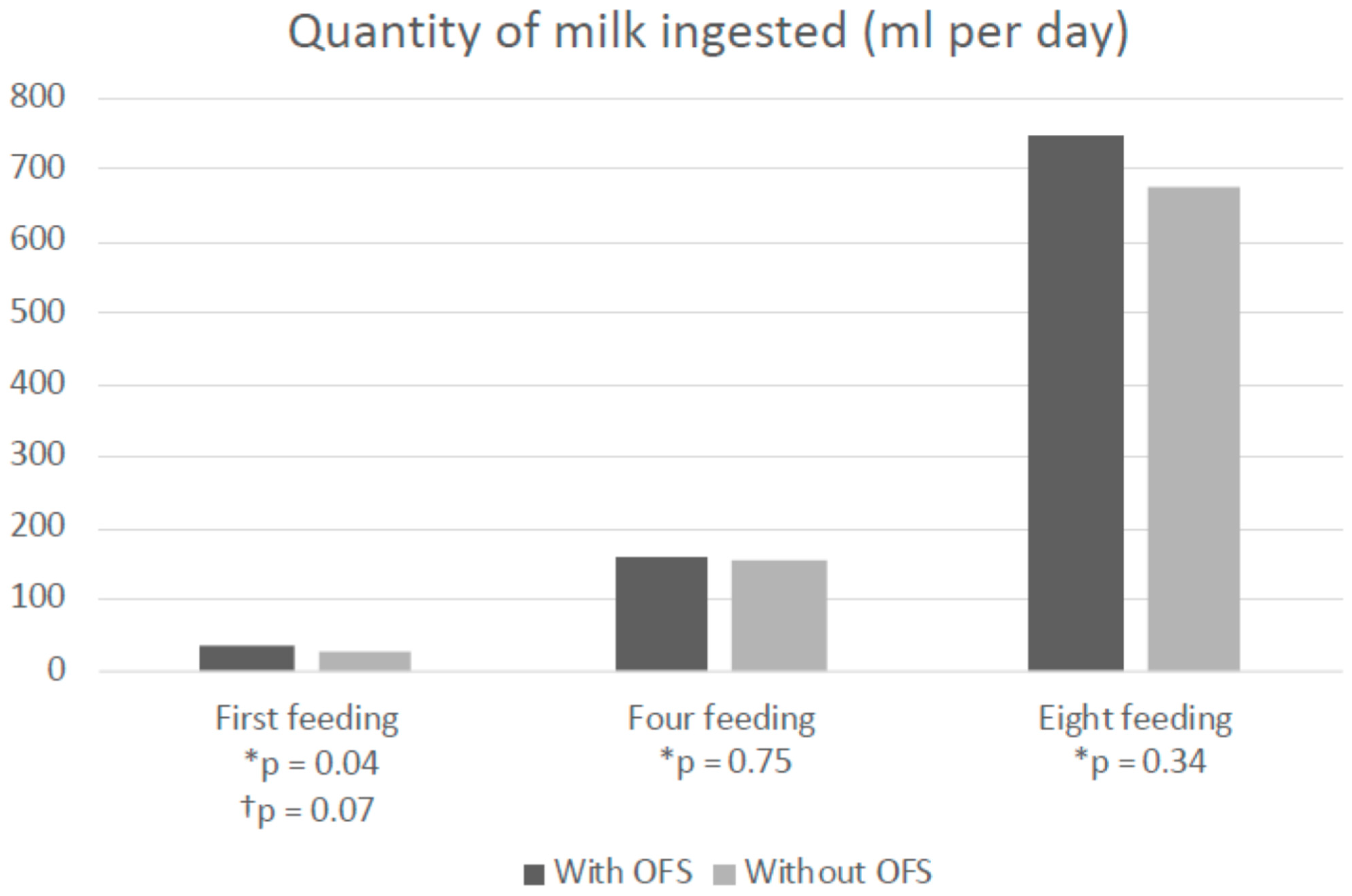
Only the quantity of milk ingested during the first autonomous feeding was significantly higher in the experimental group than in the control group (respectively 34.11 mL (+/− 6.60) vs. 29.50 mL (+/− 5, 94),
p = 0.04), in the univariate analysis. In the multivariate analysis with the adjustment for the parameters (gestational age, birth weight and total ventilation time), the observed difference between the two groups was no longer significant, however close to being significant (
p = 0.07) (
Supplemental Figure S1).
A six-month nutritional follow-up concerning the during of breast feedings, achievement of diversification and the presence of a normal gag reflex, was comparable in the two groups. The infant’s quality of life at 6 and 12 months was evaluated using the QUALIN questionnaire for the parents and showed no significant difference between the two groups (
Supplemental Table S1).
5. Discussion
Our study’s results suggest that early unimodal oral sensorimotor tactile stimulation does not significantly improve the cardio-respiratory stability or food autonomy of very premature babies.
No effect was found on the quantity of milk ingested (except at the first feeding), weight gain, or the length of hospital stay. The nutritional outcome at six months was unchanged, as was the quality of life of the child at 6 and 12 months, as assessed by the parents.
Similar to our study, a recent meta-analysis studied the effects of NNS in preterm infants under 37 weeks GA and found no significant effect on the decrease in cardio-respiratory events [
23].
On the other hand, our results concerning food autonomy are not consistent with most of the literature. Numerous studies have suggested that the duration between the transition from enteral feeding to autonomous oral feeding was reduced through oral stimulation [
24,
25,
26,
27,
28]. Our study showed a greater quantity of milk ingested during the first feeding which remained within the limits of significance. The average reduction time found in the different studies was 5 to 10 days. Rocha et al., in their randomized trial of 98 premature infants between 26 and 32 weeks GA found a more rapid 9-day acquisition of food autonomy [
29]. Tian et al., in their meta-analysis of 855 newborns between 27 and 33 weeks of age, found a similar result, with a decrease of around four days [
30]. Lessen et al. found that, for 20 premature newborns from 29 weeks GA, the decrease was five days [
31], as in our study, the correlation was even more marked when the protocols used combined sensorimotor oral stimulation with NNS [
32,
33].
Finally, the results concerning the effect of oral stimulation on the length of hospital stays are heterogeneous [
28,
34]. For Rocha et al., as well as Tian et al., the significant reduction in the length of the hospital stay was observed to be between four to ten days. For Lessen et al., an effect of oral stimulation on the length of hospital stay was not found.
Other studies did not find any significant differences either on food autonomy or on the length of the hospital stay [
34]. This is also the case in the study by Bache et al., which showed an increase in the rate of breastfeeding on discharge from the hospital, which was not the case in our study [
35].
Our study’s strengths included its randomized nature, the presence of a comparable control group, the analysis carried out with an intention-to-treat basis, and the analysis of multiple parameters (secondary criteria). Strengths also included the frequently used OFS oral protocols, which resulted from Bruwier’s and Fucile’s work, and for which no signs of intolerance were noted. The study’s paramedical staff received OFS training by qualified professional staff and the inclusion of a neonatology speech therapist was an additional asset. We were able to avoid confounding factors that can modify orality by using multivariate analyses with adjustment for gestational age, birth weight, and total ventilation time. Finally, we were able to take into account the quality of life of children as assessed by the parents in the medium term.
Our study’s limitations were represented by the absence of a blind methodology as well as the unicentric nature of the trial. The large number of people lost to follow-up minimized the number of necessary subjects, and certain parameters at the limit of significance could have been improved. When the infant received oral stimulation by different personnel such as childcare workers or childcare assistants, the reproducibility of the sessions may not have been similar. For hygienic reasons, the personnel’s gloved finger used might have been a source of discomfort for the child. We were unable to measure the quantitative parameters of the milk suction rate transfer, or the quantity of milk ingested during the first five minutes, on the total milk consumption or even the nutritional efficiency. Studies having analyzed the sucking measurement parameters [
36,
37,
38], note an improvement with oral stimulation, in particular the rate of milk transfer (quantity of milk ingested/duration of feeding in milliliters per minute), as well as the sucking frequency. This appears especially true since the quantity of milk ingested during first autonomous feed is at the limit of significance in multivariate analysis.
A major study weakness was the lack of details concerning OFS sessions which had no parent present. It can easily be assumed that when parents were present during the sessions, the newborn had conditions which enhanced their tolerance and well-being.
Finally, with improved developmental care for newborns, initiation to oral feeding should be done on the basis of personal observation for each newborn and not systematically according to their given gestational age. For individual adaptation, quantitative evaluation scores of nutritive suction make it possible to determine if the child is ready for this initiation to oral feeding [
39].
6. Conclusions
Early non-nutritive OFS does not reduce cardio-respiratory events during the period of acquisition of food autonomy, nor does it reduce the duration of acquisition of food autonomy, but it may improve nutritional efficiency. Results on this subject remain controversial in the literature. Continued studies on the subject with a more robust methodology, and with a dynamic analysis of sucking measurements, multimodal stimulation seem appropriate.
Supplementary Materials
The following are available online at
https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/children8121188/s1, Figure S1. Experimental and control group dates of first, 4th and 8th independent feeds, Week GA-adjusted. Table S1. Nutritional follow-up at 6 months, corrected age, and children’s QUALIN quality of life score at 6 and 12 months of age, as assessed by parents (experimental vs. control group).
Author Contributions
Contributors: S.M. participated in the data analysis and interpretation and writing of the manuscript. B.T., C.G. and V.B.-M. participated in the data collection, interpretation and writing of the manuscript. S.M., V.B.-M. and C.G. initiated and designed the protocol, and participated in the data interpretation and writing of the manuscript. G.S., A.G. and M.B. participated in writing the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by institutional grants from the French 2009 Appel d’Offre Recherche Clinique Assistance Publique, Hôpitaux de Marseille. The sponsor was represented by Assistance Publique, Hôpitaux de Marseille, France, whose role was to control the appropriateness of ethical and legal considerations.
Institutional Review Board Statement
The protocol was approved by the institutional ethics committee and by the French Protection Committee (N° IDRCB 2009-A01191-56, 1 January 2010), by the French national institution of pharmacovigilance (ANSM, Agence Nationale de Sécurité du Médicament et des produits de santé) (27 November 2009).
Informed Consent Statement
Informed consents were obtained once the information leaflet was reviewed with the parents or legal representatives of the children. Participants were advised they could withdraw their consent at any time, and that the data would be kept confidential.
Data Availability Statement
The datasets that generated and/or analyzed during the current study are not publicly available due to the data belongs to the Assistance Publique Hopitaux de Marseille. However, datasets are available from the sponsor (
[email protected]) on reasonable request and after sign a contract pertaining to the provision of data and/or results.
Acknowledgments
The authors wish to acknowledge the participation of all families of preterm infants in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Marret, S.; Chollat, C.; de Quelen, R.; Pinto Cardoso, G.; Abily-Donval, L.; Chadie, A.; Torre, S.; Vanhulle, C.; Mellier, D.; Charollais, A.; et al. Course and neurological/behavioral development of preterm children. Arch. Pediatrie 2015, 22, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.; Smith, E.; Schanler, R. Coordination of suck-swallow and swallow respiration in preterm infants. Acta Paediatr. 2007, 92, 721–727. [Google Scholar] [CrossRef]
- Lau, C.; Smith, E.O. A Novel Approach to Assess Oral Feeding Skills of Preterm Infants. Neonatology 2011, 100, 64–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinelli, J.; Symington, A.J. Non-nutritive sucking for promoting physiologic stability and nutrition in preterm infants. Cochrane Database Syst. Rev. 2005, 19, CD001071. [Google Scholar]
- Pineda, R.; Dewey, K.; Jacobsen, A.; Smith, J. Non-Nutritive Sucking in the Preterm Infant. Am. J. Perinatol. 2019, 36, 268–276. [Google Scholar]
- Fucile, S.; Gisel, E.; Lau, C. Oral stimulation accelerates the transition from tube to oral feeding in preterm infants. J. Pediatr. 2002, 141, 230–236. [Google Scholar] [CrossRef] [Green Version]
- Ashbaugh, J.B.; Leick-Rude, M.K.; Kilbride, H.W. Developmental care teams in the neonatal intensive care unit: Survey on current status. J. Perinatol. 1999, 19, 48–52. [Google Scholar] [CrossRef]
- Manificat, S.; Dazord, A.; Langue, J.; Danjou, G.; Bauche, P.; Bovet, F.; Cubells, J.; Luchelli, R.; Tockert, E.; Conway, K. Evaluation of the quality of life of infants and very young children: Validation of a questionnaire. Multicenter European study. Arch Pediatr. 2000, 7, 605–614. [Google Scholar] [CrossRef]
- Fontana, C.; Menis, C.; Pesenti, N.; Passera, S.; Liotto, N.; Mosca, F.; Roggero, P.; Fumagalli, M. Effects of early intervention on feeding behavior in preterm infants: A randomized controlled trial. Early Hum. Dev. 2018, 121, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Newnham, C.A.; Milgrom, J.; Skouteris, H. Effectiveness of a Modified Mother–Infant Transaction Program on Outcomes for Preterm Infants from 3 to 24 months of age. Infant Behav. Dev. 2009, 32, 17–26. [Google Scholar] [CrossRef]
- Vickers, A.; Ohlsson, A.; Lacy, J.; Horsley, A. Massage for promoting growth and development of preterm and/or low birth-weight infants. Cochrane Database Syst. Rev. 2004, 2004, CD000390. [Google Scholar] [CrossRef] [PubMed]
- Medoff-Cooper, B.; Rankin, K.; Li, Z.; Liu, L.; White-Traut, R. Multisensory Intervention for Preterm Infants Improves Sucking Organization. Adv. Neonatal Care 2015, 15, 142–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanagasabai, P.S.; Mohan, D.; Lewis, L.E.; Kamath, A.; Rao, B.K. Effect of Multisensory Stimulation on Neuromotor Development in Preterm Infants. Indian J. Pediatr. 2013, 80, 460–464. [Google Scholar] [CrossRef]
- Gaebler, C.P.; Hanzlik, J.R. The Effects of a Prefeeding Stimulation Program on Preterm Infants. Am. J. Occup. Ther. 1996, 50, 184–192. [Google Scholar] [CrossRef] [Green Version]
- Fucile, S.; Gisel, E.G.; Mcfarland, D.H.; Lau, C. Oral and non-oral sensorimotor interventions enhance oral feeding performance in preterm infants: Oral Feeding Following Sensorimotor Interventions. Dev. Med. Child Neurol. 2011, 53, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Standley, J.M.; Cassidy, J.; Grant, R.; Cevasco, A.; Szuch, C.; Nguyen, J.; Walworth, D.; Procelli, D.; Jarred, J.; Adams, K. The effect of music reinforcement for non-nutritive sucking on nipple feeding of premature infants. Pediatr. Nurs. 2010, 36, 138–145. [Google Scholar]
- Fucile, S.; Gisel, E.; Lau, C. Effect of an oral stimulation program on sucking skill maturation of preterm infants. Dev. Med. Child Neurol. 2005, 47, 158–162. [Google Scholar] [CrossRef]
- Greene, Z.; O’Donnell, C.P.; Walshe, M. Oral stimulation for promoting oral feeding in preterm infants. Cochrane Database Syst. Rev. 2016, 9, CD009720. [Google Scholar] [CrossRef] [Green Version]
- Papile, L.-A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Paneth, N. Classifying brain damage in preterm infants. J. Pediatr. 1999, 134, 527–529. [Google Scholar] [CrossRef]
- Als, H.; Tronick, E.; Lester, B.M.; Brazelton, T.B. The Brazelton Neonatal Behavioral Assessment Scale (BNBAS). J. Abnorm. Child Psychol. 1977, 5, 215–229. [Google Scholar] [CrossRef] [PubMed]
- Wallin, L.; Eriksson, M. Newborn Individual Development Care and Assessment Program (NIDCAP): A Systematic Review of the Literature. Worldviews Evid. Based Nurs. 2009, 6, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Foster, J.P.; Psaila, K.; Patterson, T. Non-nutritive sucking for increasing physiologic stability and nutrition in preterm infants. Cochrane Database Syst. Rev. 2016, 10, CD001071. [Google Scholar] [CrossRef]
- Ghomi, H.; Yadegari, F.; Soleimani, F.; Knoll, B.L.; Noroozi, M.; Mazouri, A. The effects of premature infant oral motor intervention (PIOMI) on oral feeding of preterm infants: A randomized clinical trial. Int. J. Pediatr. Otorhinolaryngol. 2019, 120, 202–209. [Google Scholar] [CrossRef]
- Fucile, S.; Milutinov, M.; Timmons, K.; Dow, K. Oral Sensorimotor Intervention Enhances Breastfeeding Establishment in Preterm Infants. Breastfeed. Med. 2018, 13, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Arora, K.; Goel, S.; Manerkar, S.; Konde, N.; Panchal, H.; Hegde, D.; Mondkar, J. Prefeeding Oromotor Stimulation Program for Improving Oromotor Function in Preterm Infants—A Randomized Controlled Trial. Indian Pediatr. 2018, 55, 675–678. [Google Scholar] [CrossRef]
- Bala, P.; Kaur, R.; Mukhopadhyay, K.; Kaur, S. Oromotor stimulation for transition from gavage to full oral feeding in preterm neonates: A Randomized controlled trial. Indian Pediatr. 2016, 53, 36–38. [Google Scholar] [CrossRef]
- Lima, A.H.; Côrtes, M.G.; Bouzada, M.C.F.; Friche, A.A.d.L. Preterm newborn readiness for oral feeding: Systematic review and meta-analysis. CoDAS 2015, 27, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Rocha, A.D.; Moreira, M.E.L.; Pimenta, H.P.; Ramos, J.R.M.; Lucena, S.L. A randomized study of the efficacy of sensory-motor-oral stimulation and non-nutritive sucking in very low birthweight infant. Early Hum. Dev. 2007, 83, 385–388. [Google Scholar] [CrossRef]
- Tian, X.; Yi, L.-J.; Zhang, L.; Zhou, J.-G.; Ma, L.; Ou, Y.-X.; Shuai, T.; Zeng, Z.; Song, G.M. Oral Motor Intervention Improved the Oral Feeding in Preterm Infants: Evidence Based on a Meta-Analysis with Trial Sequential Analysis. Medicine 2015, 94, e1310. [Google Scholar] [CrossRef] [PubMed]
- Lessen, B.S. Effect of the Premature Infant Oral Motor Intervention on Feeding Progression and Length of Stay in Preterm Infants. Adv. Neonatal Care 2011, 11, 129–139. [Google Scholar] [CrossRef]
- Zhang, Y.; Lyu, T.; Hu, X.; Shi, P.; Cao, Y.; Latour, J.M. Effect of Nonnutritive Sucking and Oral Stimulation on Feeding Performance in Preterm Infants: A Randomized Controlled Trial. Pediatr. Crit. Care Med. 2014, 15, 608–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arvedson, J.; Clark, H.; Lazarus, C.; Schooling, T.; Frymark, T. Evidence-Based Systematic Review: Effects of Oral Motor Interventions on Feeding and Swallowing in Preterm Infants. Am. J. Speech-Lang. Pathol. 2010, 19, 321–340. [Google Scholar] [CrossRef] [Green Version]
- Thakkar, P.A.; Rohit, H.R.; Ranjan, D.R.; Thakkar, U.P.; Singh, A. Effect of oral stimulation on feeding performance and weight gain in preterm neonates: A randomised controlled trial. Paediatr. Int. Child Health 2018, 38, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Bache, M.; Pizon, E.; Jacobs, J.; Vaillant, M.; Lecomte, A. Effects of pre-feeding oral stimulation on oral feeding in preterm infants: A randomized clinical trial. Early Hum. Dev. 2014, 90, 125–129. [Google Scholar] [CrossRef]
- Li, X.-L.; Liu, Y.; Liu, M.; Yang, C.-Y.; Yang, Q.-Z. Early Premature Infant Oral Motor Intervention Improved Oral Feeding and Prognosis by Promoting Neurodevelopment. Am. J. Perinatol. 2019, 37, 626–632. [Google Scholar] [CrossRef]
- Grassi, A.; Sgherri, G.; Chorna, O.; Marchi, V.; Gagliardi, L.; Cecchi, F.; Laschi, C.; Guzzetta, A. Early Intervention to Improve Sucking in Preterm Newborns: A Systematic Review of Quantitative Studies. Adv. Neonatal Care 2019, 19, 97–109. [Google Scholar] [CrossRef]
- Aguilar-Rodríguez, M.; León-Castro, J.C.; Álvarez-Cerezo, M.; Aledón-Andújar, N.; Escrig-Fernández, R.; Rodríguez de Dios-Benlloch, J.L.; Hervás-Marín, D.; Vento-Torres, M. The Effectiveness of an Oral Sensorimotor Stimulation Protocol for the Early Achievement of Exclusive Oral Feeding in Premature Infants. A Randomized, Controlled Trial. Phys. Occup. Ther. Pediatr. 2019, 40, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Neiva, F.; Leone, C.; Leone, C. Non-nutritive sucking scoring system for preterm newborns. Acta Paediatr. 2008, 97, 1370–1375. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}
{kind=link}