
Health Literacy in Schools? A Systematic Review of Health-Related Interventions Aimed at Disadvantaged Adolescents


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection Criteria
- Included typical adolescents with a reported mean age between 12 and 16 years;
- Self-reported that the participants were from a socioeconomically disadvantaged (or equivalent) background;
- Included the implementation of an intervention related to health literacy (increases health knowledge, understanding, awareness, motivation, confidence) in at least one of the following areas: physical activity, sedentary behaviour, dietary habits, sleeping habits, mental health or substance abuse;
- Included school-based interventions, interventions that could be feasibly implemented in a school setting or interventions that could be linked to a school curriculum;
- Aimed to increase health knowledge/comprehension, understanding, behaviour, value, well-being, motivation, self-efficacy or self-monitoring in relation to any of the following domains: physical activity, sedentary behaviour, dietary habits, sleeping habits, mental health or substance abuse.
- 6.
- They included special populations (e.g., children with learning difficulties, pregnant adolescents, exclusively obese individuals, or those with a specific health condition);
- 7.
- The intervention did not include an educational element or a component targeting health literacy (increases health knowledge, understanding, awareness, motivation, confidence);
- 8.
- They were book chapters, case studies, student dissertations, conference abstracts, review articles, meta-analyses, editorials, protocol papers or systematic reviews;
- 9.
- They were not published in English or in a peer-reviewed journal;
- 10.
- The full-text article was not available.
2.2. Information Sources, Search Strategy and Study Selection
2.3. Data Collection
2.4. Quality Appraisal
3. Results
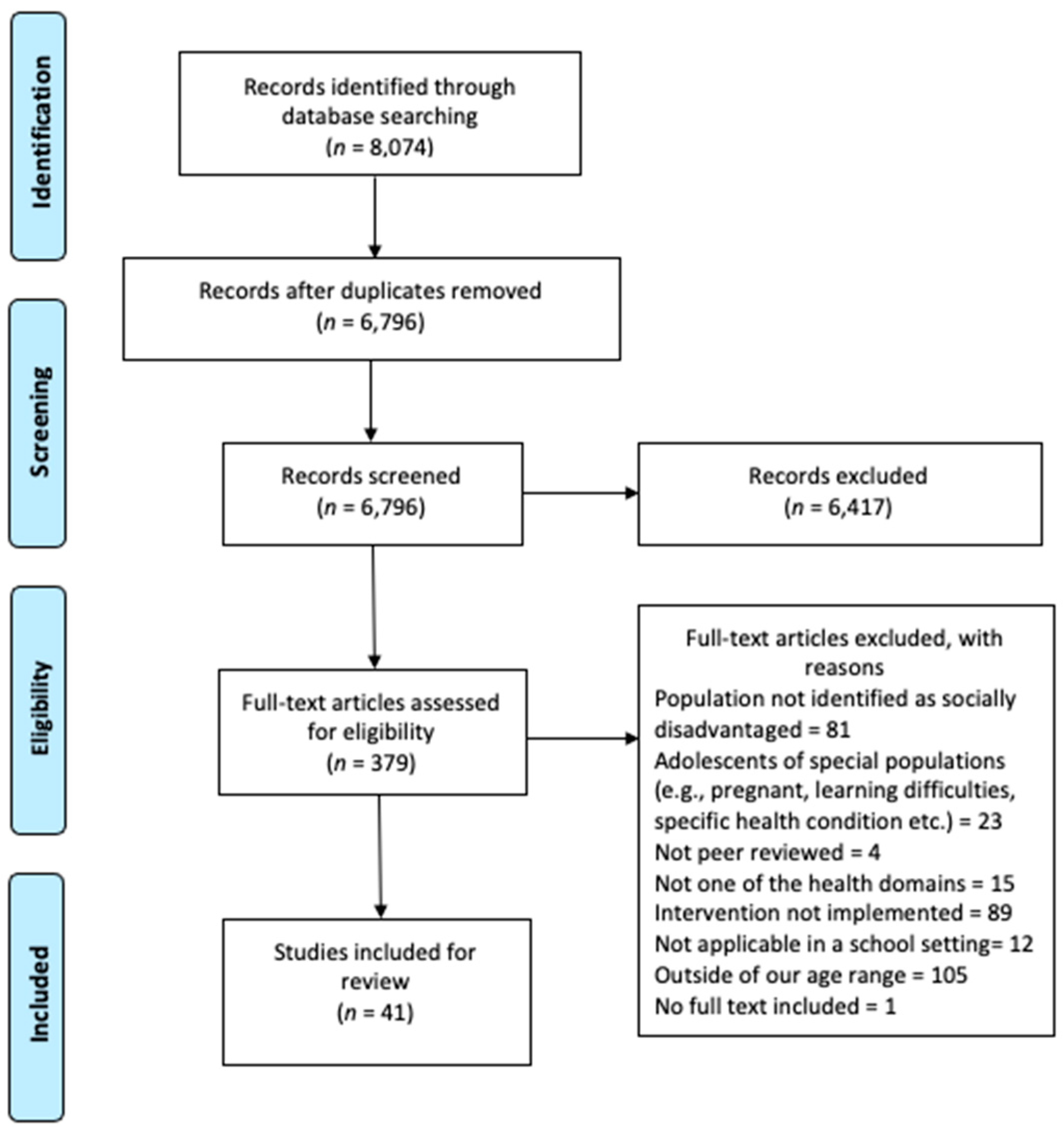
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Appraisal
3.4. Intervention Characteristics
3.5. Intervention Results
3.6. Effective Intervention Strategies
3.6.1. ‘Hands-On’ or Practical Learning
3.6.2. Peer Support
3.6.3. Holistic Approaches
4. Discussion
4.1. Effective Intervention Strategies
4.2. Implications of the Identified Interventions Strategies for Socioeconomically Disadvantaged Adolescents
4.3. The Intervention Strategies and Health Literacy
4.4. Applying Effective Intervention Strategies
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. PICO Table

{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Adolescents with a reported mean age between 12 and 16 years from a socioeconomically disadvantaged (or equivalent) background. | Mean age not between 12 and 16 or special populations (e.g., children with learning difficulties, pregnant adolescents, exclusively obese individuals, or those with a specific health condition). |
| Intervention | The implementation of an intervention related to health literacy (increases health knowledge, understanding, awareness, motivation, confidence) in at least one of the following areas physical activity, sedentary behaviour, dietary habits, sleeping habits, mental health or substance abuse. | The intervention did not include an educational element or a component targeting health literacy (increases health knowledge, understanding, awareness, motivation, confidence). |
| Context | School-based interventions, interventions that could be feasibly implemented in a school setting, or interventions that could be linked to a school curriculum. | Book chapters, case studies, student dissertations, conference abstracts, review articles, meta-analyses, editorials, protocol papers or systematic reviews. |
| Outcome | Aimed to increase health knowledge/comprehension, understanding, behaviour, value, well-being, motivation, self-efficacy or self-monitoring in relation any of the following domains: physical activity, sedentary behaviour, dietary habits, sleeping habits, mental health or substance abuse. | Outside of the targeted health domains. |
| Study Design | Published in English and in a peer-reviewed journal. | Systematic review, meta-analysis or full text not available. |
Appendix B. Search Strategy (For PubMed)
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; Coggeshall, M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Chattu, V.K.; Sakhamuri, S.M.; Kumar, R.; Spence, D.W.; Bahammam, A.S.; Pandi-Perumal, S.R. Insufficient Sleep Syndrome: Is it time to classify it as a major noncommunicable disease? Sleep Sci. 2018, 11, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Ngo, V.K.; Rubinstein, A.; Ganju, V.; Kanellis, P.; Loza, N.; Rabadan-Diehl, C.; Daar, A.S. Grand Challenges: Integrating Mental Health Care into the Non-Communicable Disease Agenda. PLoS Med. 2013, 10, e1001443. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.; Lopez, A.D. Measuring the Global Burden of Disease. N. Engl. J. Med. 2013, 369, 448–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarborough, P.; Bhatnagar, P.; Wickramasinghe, K.K.; Allender, S.; Foster, C.; Rayner, M. The economic burden of ill health due to diet, physical inactivity, smoking, alcohol and obesity in the UK: An update to 2006-07 NHS costs. J. Public Heal. 2011, 33, 527–535. [Google Scholar] [CrossRef] [Green Version]
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic Disparities in Health Behaviors. Annu. Rev. Sociol. 2010, 36, 349–370. [Google Scholar] [CrossRef] [Green Version]
- Miranda, J.J.; Kinra, S.; Casas, J.P.; Smith, G.D.; Ebrahim, S. Non-communicable diseases in low- and middle-income countries: Context, determinants and health policy. Trop. Med. Int. Heal. 2008, 13, 1225–1234. [Google Scholar] [CrossRef] [Green Version]
- Bull, E.R.; Dombrowski, S.U.; McCleary, N.; Johnston, M. Are interventions for low-income groups effective in changing healthy eating, physical activity and smoking behaviours? A systematic review and meta-analysis. BMJ Open 2014, 4, e006046. [Google Scholar] [CrossRef]
- Nutbeam, D. Health Promotion Glossary. Heal. Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Nutbeam, D.; McGill, B.; Premkumar, P. Improving health literacy in community populations: A review of progress. Heal. Promot. Int. 2018, 33, 901–911. [Google Scholar] [CrossRef]
- Batterham, R.; Hawkins, M.; Collins, P.; Buchbinder, R.; Osborne, R. Health literacy: Applying current concepts to improve health services and reduce health inequalities. Public Heal. 2016, 132, 3–12. [Google Scholar] [CrossRef]
- WHO. World Health Organization Shanghai declaration on promoting health in the 2030 Agenda for Sustainable Development. Heal. Promot. Int. 2017, 32, 7–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bröder, J.; Chang, P.; Kickbusch, I.; Levin-Zamir, D.; McElhinney, E.; Nutbeam, D.; Okan, O.; Osborne, R.; Pelikan, J.; Rootman, I.; et al. IUHPE Position Statement on Health Literacy: A practical vision for a health literate world. Glob. Heal. Promot. 2018, 25, 79–88. [Google Scholar] [CrossRef]
- Fleary, S.A.; Joseph, P.; Pappagianopoulos, J.E. Adolescent health literacy and health behaviors: A systematic review. J. Adolesc. 2018, 62, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Paakkari, L.; Kokko, S.; Villberg, J.; Paakkari, O.; Tynjälä, J. Health literacy and participation in sports club activities among adolescents. Scand. J. Public Heal. 2017, 45, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Paakkari, L.; Torppa, M.; Mazur, J.; Boberova, Z.; Sudeck, G.; Kalman, M.; Paakkari, O. A Comparative Study on Adolescents’ Health Literacy in Europe: Findings from the HBSC Study. Int. J. Environ. Res. Public Heal. 2020, 17, 3543. [Google Scholar] [CrossRef]
- Paakkari, L.T.; Torppa, M.P.; Paakkari, O.-P.; Välimaa, R.S.; A Ojala, K.S.; A Tynjälä, J. Does health literacy explain the link between structural stratifiers and adolescent health? Eur. J. Public Heal. 2019, 29, 919–924. [Google Scholar] [CrossRef]
- Stormacq, C.; Broucke, S.V.D.; Wosinski, J. Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Heal. Promot. Int. 2019, 34, e1–e17. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Regional Office for Europe. Health 2020 A European Policy Framework and Strategy for the 21st Century. 2013. Available online: http://www.euro.who.int/pubrequest (accessed on 27 January 2021).
- Steinberg, L. Cognitive and affective development in adolescence. Trends Cogn. Sci. 2005, 9, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; A Afifi, R.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Patton, G.C.; Sawyer, S.M.; Santelli, J.S.; Ross, D.A.; Afifi, R.; Allen, N.B.; Arora, M.; Azzopardi, P.; Baldwin, W.; Bonell, C.; et al. Our future: A Lancet commission on adolescent health and wellbeing. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef] [Green Version]
- Woods-Townsend, K.; Leat, H.; Bay, J.; Bagust, L.; Davey, H.; Lovelock, D.; Christodoulou, A.; Griffiths, J.; Grace, M.; Godfrey, K.; et al. LifeLab Southampton: A programme to engage adolescents with DOHaD concepts as a tool for increasing health literacy in teenagers –a pilot cluster-randomized control trial. J. Dev. Orig. Heal. Dis. 2018, 9, 475–480. [Google Scholar] [CrossRef] [Green Version]
- Baird, J.; Cooper, C.; Margetts, B.M.; Barker, M.; Inskip, H.M. Changing health behaviour of young women from disadvantaged backgrounds: Evidence from systematic reviews. In Proceedings of the Nutrition Society; Amsterdam University Press: Amsterdam, The Netherlands, 2009; Volume 68, pp. 195–204. [Google Scholar]
- Borzekowski, D.L. Considering Children and Health Literacy: A Theoretical Approach. Pediatrics 2009, 124, S282–S288. [Google Scholar] [CrossRef]
- Nutbeam, D. Getting evidence into policy and practice to address health inequalities. Heal. Promot. Int. 2004, 19, 137–140. [Google Scholar] [CrossRef] [Green Version]
- Bay, J.L.; Vickers, M.H.; Mora, H.A.; Sloboda, D.M.; Morton, S.M. Adolescents as agents of healthful change through scientific literacy development: A school-university partnership program in New Zealand. Int. J. STEM Educ. 2017, 4, 15. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.-C.; Nutbeam, D.; Aldinger, C.; Leger, L.S.; Bundy, D.; Hoffmann, A.M.; Yankah, E.; McCall, D.; Buijs, G.; Arnaout, S.; et al. Schools for health, education and development: A call for action. Heal. Promot. Int. 2008, 24, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearson, M.L.; Chilton, R.; Wyatt, K.; Abraham, C.; Ford, T.; Woods, H.B.; Anderson, R.H. Implementing health promotion programmes in schools: A realist systematic review of research and experience in the United Kingdom. Implement. Sci. 2015, 10, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Bonell, C.; Humphrey, N.; Fletcher, A.; Moore, L.; Anderson, R.; Campbell, R. Why schools should promote students’ health and wellbeing. BMJ 2014, 348, g3078. [Google Scholar] [CrossRef] [Green Version]
- Bradley, B.J.; Greene, A.C. Do Health and Education Agencies in the United States Share Responsibility for Academic Achievement and Health? A Review of 25 Years of Evidence About the Relationship of Adolescents’ Academic Achievement and Health Behaviors. J. Adolesc. Heal. 2013, 52, 523–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suhrcke, M. The impact of health and health behaviours on educati onal outcomes in high-income countries: A review of the evidence. 2011. [Google Scholar]
- Langford, R.; Bonnell, C.P.; E Jones, H.; Pouliou, T.; Murphy, S.M.; Waters, E.; A Komro, K.; Gibbs, L.F.; Magnus, D.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst. Rev. 2014, CD008958. [Google Scholar] [CrossRef] [PubMed]
- Khambalia, A.Z.; Dickinson, S.; Hardy, L.L.; Gill, T.; Baur, L.A. A synthesis of existing systematic reviews and meta-analyses of school-based behavioural interventions for controlling and preventing obesity. Obes. Rev. 2011, 13, 214–233. [Google Scholar] [CrossRef] [PubMed]
- Waters, E.; De Silva-Sanigorski, A.; Burford, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, CD001871. [Google Scholar] [CrossRef]
- Hall, W.J.; Zeveloff, A.; Steckler, A.; Schneider, M.; Thompson, D.; Pham, T.; Volpe, S.L.; Hindes, K.; Sleigh, A.; McMurray, R.G.; et al. Process evaluation results from the HEALTHY physical education intervention. Heal. Educ. Res. 2011, 27, 307–318. [Google Scholar] [CrossRef] [Green Version]
- Nash, R.; Elmer, S.; Thomas, K.; Osborne, R.; MacIntyre, K.; Shelley, B.; Murray, L.; Harpur, S.; Webb, D. HealthLit4Kids study protocol; crossing boundaries for positive health literacy outcomes. BMC Public Heal. 2018, 18, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coupe, N.; Cotterill, S.; Peters, S. Tailoring lifestyle interventions to low socio-economic populations: A qualitative study. BMC Public Heal. 2018, 18, 967. [Google Scholar] [CrossRef] [Green Version]
- Hiscock, R.; Judge, K.; Bauld, L. Social inequalities in quitting smoking: What factors mediate the relationship between socioeconomic position and smoking cessation? J. Public Heal. 2010, 33, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Buck, D.; Frosini, F. Clustering of unhealthy behaviours over time: Implications for policy and practice. 2012. [Google Scholar]
- White, M.; Adams, J.; Heywood, P. How and why do interventions that increase health overall widen inequalities within populations? Soc. Inequal. Public Health 2009, 64–81. [Google Scholar] [CrossRef] [Green Version]
- Ockene, I.S.; Tellez, T.L.; Rosal, M.C.; Reed, G.W.; Mordes, J.P.; Merriam, P.A.; Olendzki, B.C.; Handelman, G.; Nicolosi, R.J.; Ma, Y. Outcomes of a Latino Community-Based Intervention for the Prevention of Diabetes: The Lawrence Latino Diabetes Prevention Project. Am. J. Public Heal. 2012, 102, 336–342. [Google Scholar] [CrossRef]
- Brown, J.; Michie, S.; A Geraghty, A.W.; Yardley, L.; Gardner, B.; Shahab, L.; A Stapleton, J.; West, R. Internet-based intervention for smoking cessation (StopAdvisor) in people with low and high socioeconomic status: A randomised controlled trial. Lancet Respir. Med. 2014, 2, 997–1006. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfeiffer, K.A.; Robbins, L.B.; Ling, J.; Sharma, D.B.; Dalimonte-Merckling, D.M.; Voskuil, V.R.; Kaciroti, N.; Resnicow, K. Effects of the Girls on the Move randomized trial on adiposity and aerobic performance (secondary outcomes) in low-income adolescent girls. Pediatr. Obes. 2019, 14, e12559. [Google Scholar] [CrossRef] [PubMed]
- Robbins, L.B.; Ling, J.; Toruner, E.K.; Bourne, K.A.; Pfeiffer, K.A. Examining reach, dose, and fidelity of the “Girls on the Move” after-school physical activity club: A process evaluation. BMC Public Heal. 2016, 16, 671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, A.D.; Gilley, J.; James, J.; Kimani, M. “High Five to Healthy Living”: A Health Intervention Program for Youth at an Inner City Community Center. J. Community Heal. 2011, 37, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Robinson, W.L. Reducing Substance Use Among African American Adolescents: Effectiveness of School-Based Health Centers. Clin. Psychol. Sci. Pr. 2003, 10, 491–504. [Google Scholar] [CrossRef]
- Schleider, J.L.; Burnette, J.L.; Widman, L.; Hoyt, C.; Prinstein, M.J. Randomized Trial of a Single-Session Growth Mind-Set Intervention for Rural Adolescents’ Internalizing and Externalizing Problems. J. Clin. Child Adolesc. Psychol. 2020, 49, 660–672. [Google Scholar] [CrossRef]
- Kerr, J.C.; Valois, R.F.; Farber, N.B.; Vanable, P.A.; DiClemente, R.J.; Salazar, L.; Brown, L.K.; Carey, M.P.; Romer, D.; Stanton, B.; et al. Effects of Promoting Health Among Teens on Dietary, Physical Activity, and Substance Use Knowledge and Behaviors for African American Adolescents. Am. J. Heal. Educ. 2013, 44, 191–202. [Google Scholar] [CrossRef] [Green Version]
- Mendelson, T.; Tandon, S.D.; Obrennan, L.M.; Leaf, P.J.; Ialongo, N.S. Brief report: Moving prevention into schools: The impact of a trauma-informed school-based intervention. J. Adolesc. 2015, 43, 142–147. [Google Scholar] [CrossRef]
- Luesse, H.B.; Luesse, J.E.; Lawson, J.; Koch, P.A.; Contento, I.R. In Defense of Food Curriculum: A Mixed Methods Outcome Evaluation in Afterschool. Heal. Educ. Behav. 2019, 46, 612–625. [Google Scholar] [CrossRef] [PubMed]
- Issner, J.H.; Mucka, L.E.; Barnett, D. Increasing Positive Health Behaviors in Adolescents with Nutritional Goals and Exercise. J. Child Fam. Stud. 2016, 26, 548–558. [Google Scholar] [CrossRef]
- Frazier, S.L.; Dinizulu, S.M.; Rusch, D.; Boustani, M.M.; Mehta, T.G.; Reitz, K. Building Resilience After School for Early Adolescents in Urban Poverty: Open Trial of Leaders @ Play. Adm. Policy Ment. Heal. Ment. Heal. Serv. Res. 2014, 42, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Quante, M.; Khandpur, N.; Kontos, E.Z.; Bakker, J.P.; Owens, J.A.; Redline, S. A Qualitative Assessment of the Acceptability of Smartphone Applications for Improving Sleep Behaviors in Low-Income and Minority Adolescents. Behav. Sleep Med. 2019, 17, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Roth, S.E.; Gill, M.; Chan-Golston, A.M.; Rice, L.N.; Crespi, C.M.; Koniak-Griffin, D.; Prelip, M.L. The Effects of a 2-Year Middle School Physical Education Program on Physical Activity and Its Determinants. J. Phys. Act. Heal. 2019, 16, 608–615. [Google Scholar] [CrossRef]
- Fardy, P.S.; White, R.E.; Haltiwanger-Schmitz, K.; Magel, J.R.; McDermott, K.J.; Clark, L.T.; Hurster, M.M. Coronary disease risk factor reduction and behavior modification in minority adolescents: The PATH program. J. Adolesc. Heal. 1996, 18, 247–253. [Google Scholar] [CrossRef]
- Knapp, M.B.; Hall, M.T.; Mundorf, A.R.; Partridge, K.L.; Johnson, C.C. Perceptions of School-Based Kitchen Garden Programs in Low-Income, African American Communities. Heal. Promot. Pr. 2018, 20, 667–674. [Google Scholar] [CrossRef]
- Romero, A.J. A Pilot Test of the Latin Active Hip Hop Intervention to Increase Physical Activity among Low-Income Mexican-American Adolescents. Am. J. Heal. Promot. 2012, 26, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Alaimo, K.; Oleksyk, S.; Golzynski, D.; Drzal, N.; Lucarelli, J.; Reznar, M.; Wen, Y.; Yoder, K.K. The Michigan Healthy School Action Tools Process Generates Improvements in School Nutrition Policies and Practices, and Student Dietary Intake. Heal. Promot. Pr. 2015, 16, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Sibinga, E.M.; Perry-Parrish, C.; Chung, S.-E.; Johnson, S.B.; Smith, M.; Ellen, J.M. School-based mindfulness instruction for urban male youth: A small randomized controlled trial. Prev. Med. 2013, 57, 799–801. [Google Scholar] [CrossRef]
- Frenn, M.; Malin, S.; Bansal, N.; Delgado, M.; Greer, Y.; Havice, M.; Ho, M.; Schweizer, H. Addressing Health Disparities in Middle School Students’ Nutrition and Exercise. J. Community Heal. Nurs. 2003, 20, 1–14. [Google Scholar] [CrossRef]
- Frenn, M.; Malin, S.; Brown, R.L.; Greer, Y.; Fox, J.; Greer, J.; Smyczek, S. Changing the tide: An Internet/video exercise and low-fat diet intervention with middle-school students. Appl. Nurs. Res. 2005, 18, 13–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frenn, M.; Malin, S.; Bansal, N.K. Stage-based interventions for low-fat diet with middle school students. J. Pediatr. Nurs. 2003, 18, 36–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, M.M.; Hager, E.R.; Le, K.; Anliker, J.; Arteaga, S.S.; DiClemente, C.; Gittelsohn, J.; Magder, L.; Papas, M.; Snitker, S.; et al. Challenge! Health Promotion/Obesity Prevention Mentorship Model Among Urban, Black Adolescents. Pediatrics 2010, 126, 280–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicary, J.R.; Henry, K.L.; Bechtel, L.J.; Swisher, J.D.; Smith, E.A.; Wylie, R.; Hopkins, A.M. Life Skills Training Effects for High and Low Risk Rural Junior High School Females. J. Prim. Prev. 2004, 25, 399–416. [Google Scholar] [CrossRef]
- Jackson, C.J.; Mullis, R.M.; Hughes, M. Development of a theater-based nutrition and physical activity intervention for low-income, urban, African American adolescents. Prog. Community Heal. Partnerships: Res. Educ. Action 2010, 4, 89–98. [Google Scholar] [CrossRef]
- Dewar, D.L.; Morgan, P.J.; Plotnikoff, R.C.; Okely, A.D.; Collins, C.E.; Batterham, M.; Callister, R.; Lubans, D.R. The Nutrition and Enjoyable Activity for Teen Girls Study: A cluster randomized controlled trial. Am. J. Prev. Med. 2013, 45, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Morgan, P.J.; Okely, A.D.; Dewar, D.; Collins, C.E.; Batterham, M.; Callister, R.; Plotnikoff, R.C. Preventing Obesity Among Adolescent Girls. Arch. Pediatr. Adolesc. Med. 2012, 166, 821–827. [Google Scholar] [CrossRef] [Green Version]
- Dray, J.; Bowman, J.; Campbell, E.; Freund, M.; Hodder, R.; Wolfenden, L.; Richards, J.; Leane, C.; Green, S.; Lecathelinais, C.; et al. Effectiveness of a pragmatic school-based universal intervention targeting student resilience protective factors in reducing mental health problems in adolescents. J. Adolesc. 2017, 57, 74–89. [Google Scholar] [CrossRef]
- Smith, J.J.; Morgan, P.J.; Plotnikoff, R.C.; Stodden, D.F.; Lubans, D.R. Mediating effects of resistance training skill competency on health-related fitness and physical activity: The ATLAS cluster randomised controlled trial. J. Sports Sci. 2015, 34, 772–779. [Google Scholar] [CrossRef]
- Casey, M.M.; Harvey, J.T.; Telford, A.; Eime, R.M.; Mooney, A.; Payne, W.R. Effectiveness of a school-community linked program on physical activity levels and health-related quality of life for adolescent girls. BMC Public Heal. 2014, 14, 649. [Google Scholar] [CrossRef] [Green Version]
- Hollis, J.L.; Sutherland, R.; Campbell, L.; Morgan, P.J.; Lubans, D.R.; Nathan, N.; Wolfenden, L.; Okely, A.D.; Davies, L.; Williams, A.; et al. Effects of a ‘school-based’ physical activity intervention on adiposity in adolescents from economically disadvantaged communities: Secondary outcomes of the ‘Physical Activity 4 Everyone’ RCT. Int. J. Obes. 2016, 40, 1486–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandeira, A.D.S.; Silva, K.S.; Bastos, J.L.D.; Silva, D.A.S.; Lopes, A.D.S.; Filho, V.C.B. Psychosocial mediators of screen time reduction after an intervention for students from schools in vulnerable areas: A cluster-randomized controlled trial. J. Sci. Med. Sport 2020, 23, 264–269. [Google Scholar] [CrossRef]
- Leme, A.C.B.; Baranowski, T.; Thompson, D.; Nicklas, T.; Philippi, S.T. Sustained impact of the “Healthy Habits, Healthy Girls – Brazil” school-based randomized controlled trial for adolescents living in low-income communities. Prev. Med. Rep. 2018, 10, 346–352. [Google Scholar] [CrossRef]
- Da Silva, K.B.B.; Fiaccone, R.L.; Couto, R.D.; Ribeiro-Silva, R.D.C. Evaluation of the effects of a programme promoting adequate and healthy eating on adolescent health markers: An interventional study. Nutr. Hosp. 2015, 32, 1582–1590. [Google Scholar]
- Berria, J.; Minatto, G.; A Lima, L.R.; Martins, C.R.; Petroski, E.L. Predictors of dropout in the school-based multi-component intervention, ‘Mexa-se’. Heal. Educ. Res. 2018, 33, 280–291. [Google Scholar] [CrossRef]
- Fröberg, A.; Jonsson, L.; Berg, C.; Lindgren, E.-C.; Korp, P.; Lindwall, M.; Raustorp, A.; Larsson, C. Effects of an Empowerment-Based Health-Promotion School Intervention on Physical Activity and Sedentary Time among Adolescents in a Multicultural Area. Int. J. Environ. Res. Public Heal. 2018, 15, 2542. [Google Scholar] [CrossRef] [Green Version]
- Holmberg, C.; Larsson, C.; Korp, P.; Lindgren, E.-C.; Jonsson, L.; Fröberg, A.; E Chaplin, J.; Berg, C. Empowering aspects for healthy food and physical activity habits: Adolescents’ experiences of a school-based intervention in a disadvantaged urban community. Int. J. Qual. Stud. Heal. Well-being 2018, 13, 1487759. [Google Scholar] [CrossRef]
- Shinde, S.; A Weiss, H.; Varghese, B.; Khandeparkar, P.; Pereira, B.; Sharma, A.; Gupta, R.; A Ross, D.; Patton, G.; Patel, V. Promoting school climate and health outcomes with the SEHER multi-component secondary school intervention in Bihar, India: A cluster-randomised controlled trial. Lancet 2018, 392, 2465–2477. [Google Scholar] [CrossRef]
- Ganpat, T.S.; Sethi, J.K.; Nagendra, H.R. Yoga improves attention and self-esteem in underprivileged girl student. J. Educ. Heal. Promot. 2013, 2, 55. [Google Scholar] [CrossRef] [PubMed]
- Dubuy, V.; De Cocker, K.; De Bourdeaudhuij, I.; Maes, L.; Seghers, J.; Lefevre, J.; De Martelaer, K.; Brooke, H.; Cardon, G. Evaluation of a real world intervention using professional football players to promote a healthy diet and physical activity in children and adolescents from a lower socio-economic background: A controlled pretest-posttest design. BMC Public Heal. 2014, 14, 457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Araya, R.; Fritsch, R.; Spears, M.; Rojas, G.; Martinez, V.; Barroilhet, S.; Vöhringer, P.; Gunnell, D.; Stallard, P.; Guajardo, V.; et al. School Intervention to Improve Mental Health of Students in Santiago, Chile. JAMA Pediatr. 2013, 167, 1004–1010. [Google Scholar] [CrossRef] [Green Version]
- Aceves-Martins, M.; Llauradó, E.; Tarro, L.; Moriña, D.; Papell-Garcia, I.; Prades-Tena, J.; Kettner-Høeberg, H.; Puiggròs, F.; Arola, L.; Davies, A.; et al. A School-Based, Peer-Led, Social Marketing Intervention To Engage Spanish Adolescents in a Healthy Lifestyle (“We Are Cool”—Som la Pera Study): A Parallel-Cluster Randomized Controlled Study. Child. Obes. 2017, 13, 300–313. [Google Scholar] [CrossRef]
- Beaulac, J.; Kristjansson, E.; Calhoun, M. ‘Bigger than hip-hop?’ Impact of a community-based physical activity program on youth living in a disadvantaged neighborhood in Canada. J. Youth Stud. 2011, 14, 961–974. [Google Scholar] [CrossRef]
- Shackleton, N.; Jamal, F.; Viner, R.M.; Dickson, K.; Patton, G.; Bonell, C. School-Based Interventions Going Beyond Health Education to Promote Adolescent Health: Systematic Review of Reviews. J. Adolesc. Heal. 2016, 58, 382–396. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, R.L.; Campbell, E.M.; Lubans, D.R.; Morgan, P.J.; Nathan, N.K.; Wolfenden, L.; Okely, A.D.; Gillham, K.E.; Hollis, J.L.; Oldmeadow, C.J.; et al. The Physical Activity 4 Everyone Cluster Randomized Trial: 2-Year Outcomes of a School Physical Activity Intervention Among Adolescents. Am. J. Prev. Med. 2016, 51, 195–205. [Google Scholar] [CrossRef] [Green Version]
- Sussman, S.; Skara, S.; Ames, S.L. Substance Abuse Among Adolescents. Subst. Use Misuse 2008, 43, 1802–1828. [Google Scholar] [CrossRef]
- Urrila, A.S.; Artiges, E.; Massicotte, J.; Miranda, R.; Vulser, H.; Bézivin-Frere, P.; Lapidaire, W.; Lemaître, H.; Penttilä, J.; The IMAGEN Consortium; et al. Sleep habits, academic performance, and the adolescent brain structure. Sci. Rep. 2017, 7, 41678. [Google Scholar] [CrossRef] [Green Version]
- Das, J.K.; Salam, R.A.; Arshad, A.; Finkelstein, Y.; Bhutta, Z.A. Interventions for Adolescent Substance Abuse: An Overview of Systematic Reviews. J. Adolesc. Heal. 2016, 59, S61–S75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griggs, S.; Conley, S.; Batten, J.; Grey, M. A systematic review and meta-analysis of behavioral sleep interventions for adolescents and emerging adults. Sleep Med. Rev. 2020, 54, 101356. [Google Scholar] [CrossRef] [PubMed]
- Durlak, J.A.; Dupre, E.P. Implementation Matters: A Review of Research on the Influence of Implementation on Program Outcomes and the Factors Affecting Implementation. Am. J. Community Psychol. 2008, 41, 327–350. [Google Scholar] [CrossRef] [PubMed]
- Schaap, R.; Bessems, K.; Otten, R.; Kremers, S.; van Nassau, F. Measuring implementation fidelity of school-based obesity prevention programmes: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.; Lubben, F.; Hogarth, S. Bringing science to life: A synthesis of the research evidence on the effects of context-based and STS approaches to science teaching. Sci. Educ. 2007, 91, 347–370. [Google Scholar] [CrossRef]
- Grace, M.; Woods-Townsend, K.; Griffiths, J.; Godfrey, K.; Hanson, M.; Galloway, I.; Azaola, M.C.; Harman, K.; Byrne, J.; Inskip, H. Developing teenagers’ views on their health and the health of their future children. Heal. Educ. 2012, 112, 543–559. [Google Scholar] [CrossRef]
- Jaccard, J.; Blanton, H.; Dodge, T. Peer Influences on Risk Behavior: An Analysis of the Effects of a Close Friend. Dev. Psychol. 2005, 41, 135–147. [Google Scholar] [CrossRef] [Green Version]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Vesely, S.K.; Wyatt, V.H.; Oman, R.F.; Aspy, C.B.; Kegler, M.C.; Rodine, S.; Marshall, L.; McLeroy, K.R. The potential protective effects of youth assets from adolescent sexual risk behaviors. J. Adolesc. Heal. 2004, 34, 356–365. [Google Scholar] [CrossRef]
- Donovan, J.E. Adolescent alcohol initiation: A review of psychosocial risk factors. J. Adolesc. Heal. 2004, 35, 529.e7–529.e18. [Google Scholar] [CrossRef]
- Michie, S.; Jochelson, K.; Markham, W.A.; Bridle, C. Low-income groups and behaviour change interventions: A review of intervention content, effectiveness and theoretical frameworks. J. Epidemiol. Community Heal. 2009, 63, 610–622. [Google Scholar] [CrossRef] [Green Version]
- Resnicow, K.; Yaroch, A.L.; Davis, A.; Wang, D.T.; Carter, S.; Slaughter, L.; Coleman, D.; Baranowski, T. Go Girls!: Results from a Nutrition and Physical Activity Program for Low-Income, Overweight African American Adolescent Females. Heal. Educ. Behav. 2000, 27, 616–631. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Morgan, P.J.; Aguiar, E.J.; Callister, R. Randomized controlled trial of the Physical Activity Leaders (PALs) program for adolescent boys from disadvantaged secondary schools☆. Prev. Med. 2011, 52, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Der Aa, D.A.K.-V.; Altenburg, T.M.; Zee, C.H.V.R.-V.D.; Chinapaw, M.J.M. The effectiveness and promising strategies of obesity prevention and treatment programmes among adolescents from disadvantaged backgrounds: A systematic review. Obes. Rev. 2017, 18, 581–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization, Regional Office for Europe. Physical Activity Promotion in Socially Disadvantaged grouPs: PrinciPles for action Policy summary. 2013. Available online: http://www.euro.who.int/pubrequest (accessed on 26 January 2021).
- Ventura, A.K.; Birch, L.L. Does parenting affect children’s eating and weight status? Int. J. Behav. Nutr. Phys. Act. 2008, 5, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamath, C.C.; Vickers, K.S.; Ehrlich, A.; McGovern, L.; Johnson, J.; Singhal, V.; Paulo, R.; Hettinger, A.; Erwin, P.J.; Montori, V.M. Behavioral Interventions to Prevent Childhood Obesity: A Systematic Review and Metaanalyses of Randomized Trials. J. Clin. Endocrinol. Metab. 2008, 93, 4606–4615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golley, R.K.; Hendrie, G.A.; Slater, A.; Corsini, N. Interventions that involve parents to improve children’s weight-related nutrition intake and activity patterns—What nutrition and activity targets and behaviour change techniques are associated with intervention effectiveness? Obes. Rev. 2011, 12, 114–130. [Google Scholar] [CrossRef]
- Zarychta, K.; Mullan, B.; Luszczynska, A. It doesn’t matter what they say, it matters how they behave: Parental influences and changes in body mass among overweight and obese adolescents. Appetite 2016, 96, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D.; Lloyd, J.E. Understanding and Responding to Health Literacy as a Social Determinant of Health. Annu. Rev. Public Heal. 2021, 42. [Google Scholar] [CrossRef] [PubMed]
- Peralta, L.R.; Rowling, L. Implementation of school health literacy in Australia: A systematic review. Heal. Educ. J. 2018, 77, 363–376. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Heal. Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Elmer, S.; Nash, R.; Kemp, N.; Coleman, C.; Wyss, M.; Roach, J. HealthLit4Kids: Supporting schools to be health literacy responsive organisations. Heal. Promot. J. Aust. 2021, 32, 17–28. [Google Scholar] [CrossRef]
- McCuaig, L.; Coore, S.; Carroll, K.; Macdonald, D.; Rossi, A.; Bush, R.; Ostini, R.; Hay, P.; Johnson, R. Developing Health Literacy through School Based Health Education: Can Reality Match Rhetoric? 2012. Available online: http://www.hms.uq.edu.au/media/194975/reality_matching_rhetoric_report.pdf (accessed on 13 November 2020).
- Massey, P.M.; Prelip, M.; Calimlim, B.M.; Quiter, E.S.; Glik, D.C. Contextualizing an expanded definition of health literacy among adolescents in the health care setting. Heal. Educ. Res. 2012, 27, 961–974. [Google Scholar] [CrossRef] [Green Version]
- Paakkari, O.; Torppa, M.; Boberova, Z.; Välimaa, R.; Maier, G.; Mazur, J.; Kannas, L.; Paakkari, L. The cross-national measurement invariance of the health literacy for school-aged children (HLSAC) instrument. Eur. J. Public Heal. 2019, 29, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Spillane, A.; Belton, S.; McDermott, C.; Issartel, J.; Osborne, R.H.; Elmer, S.; Murrin, C. Development and validity testing of the Adolescent Health Literacy Questionnaire (AHLQ): Protocol for a mixed methods study within the Irish school setting. BMJ Open 2020, 10, e039920. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.J.; Hay, P.J.; Macdonald, D. The outsourcing of health, sport and physical educational work: A state of play. Phys. Educ. Sport Pedagog. 2011, 16, 399–415. [Google Scholar] [CrossRef] [Green Version]
- McCuaig, L.A. Teaching the Art of Healthy Living: A Genealogical Study of h-pe and the Moral Governance of Apprentice Citizens. Ph.D. Thesis, School of Human Movement Studies, The University of Queensland, Queensland, Australia, 2008. [Google Scholar]
- Beauchamp, A.; Batterham, R.W.; Dodson, S.; Astbury, B.; Elsworth, G.R.; McPhee, C.; Jacobson, J.; Buchbinder, R.; Osborne, R.H. Systematic development and implementation of interventions to OPtimise Health Literacy and Access (Ophelia). BMC Public Heal. 2017, 17, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batterham, R.W.; Buchbinder, R.; Beauchamp, A.; Dodson, S.; Elsworth, G.R.; Osborne, R.H. The OPtimising HEalth LIterAcy (Ophelia) process: Study protocol for using health literacy profiling and community engagement to create and implement health reform. BMC Public Heal. 2014, 14, 694. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Authors (year) | Country | Study Design | Research Type | Sample | Gender |
|---|---|---|---|---|---|
| Aceves-Martins et al. (2017) [86] | Spain | RCT | MM | 393 | M&F |
| Alaimo et al. (2015) [62] | US | Pre-test-post-test design (quasi-experimental) | QT | 1176 | M&F |
| Araya et al. (2013) [85] | Chile | RCT | QT | 2512 | M&F |
| Baker et al. (2011) [49] | US | Pre-test-post-test design (quasi-experimental) | MM | 46 | M&F |
| Bandeira et al. (2020) [76] | Brazil | RCT | QT | 1085 | M&F |
| Beaulac et al. (2011) [87] | Canada | Post-test evaluation | MM | 67 | M&F |
| Berria et al. (2018) [79] | Brazil | Pre-test-post-test design (quasi-experimental) | QT | 546 | M&F |
| Black et al. (2010) [67] | US | RCT | QT | 235 | M |
| Brito Beck da Silva et al. (2015) [78] | Brazil | RCT | QT | 833 | M&F |
| Casey et al. (2014) [74] | Australia | RCT | QT | 621 | F |
| Dewar et al. (2013) [70] | Australia | RCT | QT | 357 | F |
| Dray et al. (2017) [72] | Australia | RCT | QT | 3115 | M&F |
| Dubuy et al. (2014) [84] | Belgium | Pre-test-post-test design (quasi-experimental design) | QT | 414 | M |
| Fardy et al. (1996) [59] | US | RCT | QT | 346 | M&F |
| Frazier et al. (2015) [56] | US | (Single group) Pre-test-post-test design | QT | 46 | M&F |
| Frenn et al. (2003) [66] | US | Pre-test-post-test design (quasi-experimental) | QT | 117 | M&F |
| Frenn et al. (2003) [64] | US | Pre-test-post-test design (quasi-experimental) | QT | 130 | M&F |
| Frenn et al. (2005) [65] | US | Pre-test-post-test design (quasi-experimental) | QT | 103 | M&F |
| Fróberg et al. (2018) [80] | Sweden | Pre-test-post-test design (quasi-experimental) | QT | 114 | M&F |
| Hollis et al. (2016) [75] | Australia | RCT | QT | 1150 | M&F |
| Holmberg et al. (2018) [81] | Sweden | Post-test evaluation | QL | 49 | M&F |
| Issner et al. (2017) [55] | US | RCT | QT | 100 | M&F |
| Jackson et al. (2010) [69] | US | Pre-test-post-test design (quasi-experimental) | MM | 15 | M&F |
| Kerr et al. (2013) [52] | US | RCT | QT | 1654 | M&F |
| Knapp et al. (2019) [60] | US | Cross sectional | QL | 27 | M&F |
| Leme et al. (2018) [77] | Brazil | RCT | QT | 253 | F |
| Lubans et al. (2012) [71] | Australia | RCT | QT | 357 | F |
| Luesse et al. (2019) [54] | US | (Single group) Pre-test-post-test design | MM | 32 | M&F |
| Mendelson et al. (2015) [53] | US | Pre-test-post-test design (quasi-experimental) | QT | 49 | M&F |
| Quante et al. (2019) [57] | US | Post-test qualitative evaluation | QL | 27 | M&F |
| Robbins et al. (2016) [48] | US | RCT | QT | 1519 | F |
| Robbins et al. (2019) [47] | US | RCT | QT | 1519 | F |
| Robinson et al. (2003) [50] | US | Cross sectional | QT | 1196 | M&F |
| Romero (2012) [61] | US | (Single group) Pre-test post-test design | QT | 73 | M&F |
| Roth et al. (2019) [58] | US | RCT | QT | 3763 | M&F |
| Schleider et al. (2019) [51] | US | RCT | QT | 222 | F |
| Sethi et al. (2013) [83] | India | (Single group) Pre-test-post-test design | QT | 60 | F |
| Shinde et al. (2018) [82] | India | RCT | QT | 13,035 | M&F |
| Sibinga et al. (2013) [63] | US | RCT | QT | 41 | M |
| Smith et al. (2016) [73] | Australia | RCT | QT | 361 | M |
| Vicary et al. (2016) [68] | US | RCT | QT | 319 | F |
| Authors | Selection Bias | Detection Bias | Attrition Bias | Reporting Bias | |
|---|---|---|---|---|---|
| Random Sequence Generation | Allocation Concealment | Blinding of Outcome data | Incomplete Outcome Reporting | Selective Outcome Reporting | |
| Aceves-Martins et al. [86] | Low risk | High Risk | Unclear Risk | Low risk | Low risk |
| Alaimo et al. [62] | n/a | n/a | Unclear Risk | High Risk | Low Risk |
| Araya et al. [85] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk |
| Baker et al. [49] | n/a | n/a | Unclear Risk | Low Risk | Low Risk |
| Bandeira et al. [76] | Unclear Risk | Unclear Risk | High Risk | Low Risk | Low Risk |
| Beaulac et al. [87] | n/a | n/a | Low Risk | Low Risk | Low Risk |
| Berria et al. [79] | n/a | n/a | Unclear Risk | Low Risk | Low Risk |
| Black et al. [67] | Low Risk | Unclear Risk | Low Risk | Low Risk | Low Risk |
| Brito Beck da Silva et al. [78] | Unclear Risk | Unclear Risk | Unclear Risk | Low Risk | Low Risk |
| Casey et al. [74] | Low Risk | Unclear Risk | Unclear Risk | High Risk | Low Risk |
| Dewar et al. [70] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk |
| Dray et al. [72] | Low Risk | High Risk | Unclear Risk | Low Risk | Low Risk |
| Dubuy et al. [84] | n/a | n/a | High Risk | Low Risk | Low Risk |
| Fardy et al. [59] | Unclear Risk | Unclear Risk | Unclear Risk | Low Risk | Low Risk |
| Frazier et al. [56] | n/a | n/a | High Risk | Unclear Risk | Low Risk |
| Frenn et al. [66] | n/a | n/a | Low Risk | Unclear Risk | Low Risk |
| Frenn et al. [64] | n/a | n/a | Unclear Risk | Low Risk | Low Risk |
| Frenn et al. [65] | n/a | n/a | Low Risk | Low Risk | Low Risk |
| Fróberg et al. [80] | n/a | n/a | Unclear Risk | Low Risk | Low Risk |
| Hollis et al. [75] | Low Risk | Low risk | Low Risk | Low Risk | Low Risk |
| Holmberg et al. [81] | n/a | n/a | Low Risk | Low Risk | n/a |
| Issner et al. [55] | Low Risk | Unclear Risk | High Risk | High Risk | Low Risk |
| Jackson et al. [69] | n/a | n/a | Unclear Risk | Low Risk | Low Risk |
| Kerr et al. [52] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk |
| Knapp et al. [60] | n/a | n/a | High Risk | Low Risk | Low Risk |
| Leme et al. [77] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk |
| Lubans et al. [71] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk |
| Luesse et al. [54] | n/a | n/a | High Risk | Low Risk | Low Risk |
| Mendelson et al. [53] | High Risk | High Risk | High Risk | Unclear Risk | Low Risk |
| Quante et al. [57] | n/a | n/a | Unclear Risk | Low Risk | Low Risk |
| Robbins et al. [48] | Low Risk | High Risk | Low Risk | Low Risk | Low Risk |
| Robbins et al. [47] | Low Risk | High Risk | Low Risk | Low Risk | Low Risk |
| Robinson et al. [50] | n/a | n/a | Unclear Risk | Low Risk | Low Risk |
| Romero [61] | n/a | n/a | Low Risk | Low Risk | Low Risk |
| Roth et al. [58] | Unclear Risk | Unclear Risk | High Risk | Low Risk | Low Risk |
| Schleider et al. [51] | Low Risk | Low Risk | Unclear Risk | Low Risk | Low Risk |
| Sethi et al. [83] | n/a | n/a | Low Risk | Low Risk | Low Risk |
| Shinde et al. [82] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk |
| Sibinga et al. [63] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk |
| Smith et al. [73] | Low Risk | Low Risk | Low Risk | Low Risk | Low Risk |
| Vicary et al. [68] | Unclear Risk | Unclear Risk | Unclear Risk | Low Risk | Low Risk |
| Author | Purpose of the Intervention | Key Features of the Intervention | Delivered by | Duration | Theory | Study Outcome(s) Measured | Effectiveness (in Relation to the Outcome Measures) | Fidelity Measure | |
|---|---|---|---|---|---|---|---|---|---|
| Diet and PA Interventions (n = 13) | |||||||||
| Aceves-Martins et al. [86] | To increase fruit and vegetable intake and PA, while reducing screen time | (a) Adolescent challenge creator (ACC) training: An initial training session on social media principles and healthy lifestyle theory led by a university specialist in health and communication. (b) Design and implementation of 10 activities: ACCs attended activity design sessions. The themes of the activities were based on the primary and secondary objectives of the study, which would stimulate the interest of their peers and were designed to be attractive. The ACCs presented the intervention in classrooms at the two intervention schools, in which they explained the study, provided social media information, and invited their peers to provide suggestions for activities. The ACCs disseminated the activities using social media platforms, posters and flyers. Information, photographs, and videos pertaining to each activity were uploaded to the campaign’s social media platforms. Number of participants = 170. | ACCs, (trained by university specialists) | 12 months | None reported |
| The percentage of adolescents in the intervention group who consumed ≥1 portion of fruit/day increased by 23.5% (p < 0.01). Vegetable consumption differed only in males. The percentage of males consuming ≥1 portion of vegetables/day increased by 27.9% (p < 0.01) in the intervention group. The percentage of adolescents in the intervention group who engaged in ≥6 h of PA/week participation increased by 21.2% (p < 0.01). The percentage of male adolescents who engaged in ≤2 h of screen time/week increased by 27.9% (p < 0.01) in the intervention group and 12.3% in the control group (p = 0.01). | No | |
| Baker et al. [49] | To promote a healthylifestyle and improve healthy behaviours* (oral hygiene, hand washing techniques, PA, personal hygiene, and nutrition and food safety) *information reported in this review relates to PA and nutrition components | Medical students presented a lecture, followed by an exercise session (circuit training), healthy smoothie preparation, and nutritional value of food analysis. The lecture topics were broken down into modules (Physical Health and Healthy Eating Habits), and included methods for achieving optimal fitness, types of exercise, proper weight gaining/loss techniques and nutrition/food safety. The intervention was linked to the NFL Youth Education Town community centre. Number of participants = 46. | Medical students | 5 weeks | None reported |
| Physical Health Module: 17% of the participants passed the pre-test (60% or higher). 67% percent of all participants passed their post-test (60% or higher, achieving that objective). 75% of these participants improved their test scores by at least 10%, also achieving that objective. Following the end of the intervention program, the survey showed a positive change in behaviour in 75% of the participants. Healthy Eating Habits Module: 29% of the participants passed the pre-test (60% or higher) .50% of the participants passed the post-test (60% or higher), failing to achieve that objective. 86% of all the participants improved their scores by at least 10%, successfully achieving that objective. The survey following the intervention showed that 50% of the participants positively changed their personal eating habits. | No | |
| Black et al. [67] | Health promotion and obesity prevention program | A manualised 12-session intervention (“Challenge”) included a rap music video promoting healthy eating and PA principles of mentorship (role modelling and support), participatory learning, goal setting. In addition to setting dietary and PA goals, tracking and evaluating progress, and revising goals as necessary, intervention adolescents prepared and tasted healthy snacks and engaged in PA. Number of participants = 121. | Specially trained, college-enrolled, African American mentors | (Approx.) 10 months | Social Cognitive Theory and Motivational Interviewing |
| The percentage of overweight/obese adolescents declined from 54% to 36% in the intervention group, while the percentage declined from 36% to 32% among the control group. The percentage overweight/obese adolescents further declined to 35% in the intervention group, but increased to 38% among the control group at delayed follow up, resulting in a significant difference between groups (χ2 = 5.8, p = 0.02, GEE). There were no statistically significant interactions between intervention and time in either post-intervention or delayed follow up for total percent body fat, fat mass or fat free mass in the multi-level modelling with the whole sample. | No | |
| Dewar et al. [70] | To promote PA and healthy eating and prevent obesity among inactive adolescent girls | The Nutrition and Enjoyable Activity for Teen (NEAT) Girls combined a range of strategies to promote lifestyle (e.g., walking to school) and lifetime PA (e.g., resistance training), improve dietary intake, and reduce sedentary behaviours. Intervention components included enhanced school sport sessions and lunchtime PA, nutrition workshops, interactive educational seminars, pedometers for self-monitoring, student handbooks, parent newsletters, text messages to reinforce and encourage health behaviours.Number of participants = 179. | Teachers, researchers, dieticians | 12 months | Social Cognitive Theory |
| There were no changes in BMI, but there was a group-by-time interaction effect for percentage body fat (–1.96%, p = 0.006) | Yes | |
| Dubuy et al. [84] | To promote a healthy diet and PA | 3 components (start clinic, school program, end clinic). Clinics (ran by players): eating healthy breakfast, warm up session with players and signing a lifestyle contract. School element: providing free fruit to all pupils, fruit and vegetable quiz, lessons on importance of drinking enough water, activity breaks and active playgrounds. Number of participants = 268. | Professional soccer players, health workers and teachers | 4 months | None reported |
| No intervention effects were found for consumption of breakfast, fruit, soft drinks or sweet and savoury snacks. Positive intervention effects were found for self-efficacy for having a daily breakfast (p < 0.01), positive attitude towards vegetables consumption (p < 0.01) and towards lower soft drink consumption (p < 0.001). A trend towards significance (p < 0.10) was found for self-efficacy for reaching the PA guidelines. For sports participation, no significant intervention effect was found. 92 students completed the process evaluation questionnaire, the feedback was largely positive. | Yes | |
| Frenn et al. [66] | To improve the adoption of a diet lower in fat and duration of PA | The primary classroom strategy for the sessions was consciousness raising and self-re-evaluation.Separate smaller group sessions were held for students in the preparation, action, and maintenance stages of change Examples of content used include food pyramids, food diaries, peer leadership, planning exercise sessions. (Specific strategies detailed in the paper.)Number of participants = 60. | Paediatric nursing students | 4 classroom intervention sessions (duration of intervention not reported) | Transtheoretical Model and Health Promotion model |
| When the Health Promotion/Transtheoretical Model interventions were used in 4 classroom sessions, students had a significantly (p <.05) reduced trend toward choosing a diet higher in fat and increased duration of PA, as compared with a control group. | No | |
| Frenn et al. [64] | To examine improvement related to Healthy People 2010 Objectives (U.S. Department of Health & Human Services, 2000) for low-fat diets and MVPA | Internet and video sessions for students in the precontemplation and contemplation stages of change focused on raising awareness of current eating and exercise, identifying pros (or benefits) of both low-fat diet and exercise, and overcoming cons (or barriers) to consuming low-fat diets and participating in exercise. Those in the precontemplation, action, and maintenance stages of change were prepared as “peer models” and led the healthy snack and exercise labs with the assistance of senior nursing students and faculty. Online feedback was given to all students in the intervention for each internet session. (Specific strategies detailed in the paper.)Number of participants = 67. | Peer models (students), nursing students and other faculty members | Academic year | Transtheoretical Model and Health Promotion model |
| The difference in percentage of dietary fat intake between the intervention and control groups as a whole was not significant. Both control and intervention groups decreased their amount of MVPA, but the level of decrease in MVPA was less among the intervention group (–8.58 min) as compared to the control (–37.61 min; p = 0.024) | No | |
| Frenn et al. [65] | To increase PA and reduce dietary fat among low-income, culturally diverse, 7th-grade students | Eight-session Blackboard platform-delivered internet approach with four 2 to 3 min videos. Sessions included preparing snacks, raising awareness for food early in the day/night-time binging, consciousness raising for PA and caloric balance. Computer-generated tailored feedback based on stage of behaviour change was provided to individual subjects for both PA and dietary fat. (Specific strategies detailed in the paper.)Number of participants = 43. | Blackboard platform delivery (internet and computer based).Previously delivered by paediatric nursing students | 1 month | Transtheoretical Model and Health Promotion Model |
| Intervention students who completed more than half of sessions increased MVPA by an average of 22 min, compared with a decrease of 46 min for the control group, t 103 = −1.99, p = 0.05. Those who completed all three sessions increased PA by 33 min. Those participating more than half the sessions decreased percentage of dietary fat from 30.7 to 29.9, t 87 = 2.73, p = 0.008, whereas those in the control had 31.5% dietary fat in pre-test and 31.6% in post-test. Those participating in less than half the diet sessions were not significantly different than students in the control group classes, t 16.6 = −1.843, p = 0.08. | None reported | |
| Holmberg et al. [81] | To improve MVPA, sedentary time, exercise training frequency and duration | The intervention was developed and implemented, as a result of cooperation and shared decision making among the researchers and the participants. Components included health coaching, health promotion sessions and a closed Facebook group. Number of participants = 49. | PhD students and the research team | 2 years | None reported |
| The adolescents appreciated influencing the components of the intervention and collaborating with peers in active learning activities such as practicing sports and preparing meals. They also reported acquiring new health information, that trying new activities was inspiring, and the use of pedometers and photo-food diaries helped them reflect on their health behaviours. This was echoed by teachers. | No | |
| Issner et al. [55] | To motivate urban, minority youth to make healthy changes in diet and PA | All participants engaged in goal discussion with a health coach that lasted 3–5 min. The enhanced intervention group continued the intervention after the goalsetting portion wherein facilitators used probes to discuss previous experience, elicit positive change talk, discussion of benefits, and ideas for potential solutions.Number of participants = 51. | “Health coaches” (first and second author and research assistants) | 20 min–1 session | Self-Determination Theory and Motivational Interviewing |
| There was no significant interaction between the impact of the two intervention conditions on participants’ reports of fruit and vegetable intake across two time periods Wilks Lambda = 1.00, F(2, 52) = 0.19, p = 0.66, partial eta squared = 0.004. A main effect of time trended toward significance, Wilks Lambda = 0.95, F(2, 52) = 2.88, p = 0.09, partial eta squared = 0.054, with both groups showing an increase in fruit and vegetable intake. There was no significant interaction between participants’ reports of PA across two time periods, Wilks Lambda = 0.99, F(2, 49) = 0.58, p = 0.45, partial eta squared = 0.012. Time significantly affected outcomes, Wilks Lambda = 0.90, F(2, 49) = 4.99, p = 0.03, partial eta squared = 0.096, with both groups showing an increase in PA at time 2. In the goals only condition, from baseline to follow up, PA significantly increased, t(22) = −2.27, p < 0.05 (effect size d = 0.46) and autonomous motivation for PA significantly increased, t(22) = −2.45, p < 0.05 (effect size d = 0.56). In the enhanced intervention condition, from baseline to follow up, PA significantly increased, t(22) = −2.17, p < 0.05 (effect size d = 0.40), autonomous motivation for diet significantly increased, t(22) = −3.59, p < 0.001 (effect size d = 0.67), and self-efficacy for diet significantly increased t(22) = −3.91, p < 0.001 (effect size d = 0.67). | Yes | |
| Jackson et al. [69] | To engage low-income, urban, African American adolescents and their families in learning ways to adopt a healthy lifestyle | Interventions components included nutrition and PA information education, preparation and performance of their own “healthy” skits, team building exercises designed to introduce theatre dynamics, which progressed into script-writing activities, making healthy recipes or snacks. Each session ended with some form of PA (circuit training or a dance routine). At the end of the 6 week program, students performed ‘Getting on Track’ for family and friends. Parents were engaged in three ways: (1) participating in a health information and recipe session, (2) completing home-based activities, and (3) attending the intervention’s culminating event, the Champions of Health Dinner Theatre.Number of participants = 15. | Registered dietitian with a background in theatre and a program assistant | 6 weeks | None reported |
| Increases in the number of participants who knew the daily recommended number of servings of fruits and vegetables as well as the recommended amount of time healthy children should be active. When given a choice between specific food item and activity pairs, participants chose healthier food items and PA over sedentary activity at post-test.An increase in students who responded “sometimes” when asked about healthy behaviour (eating fruits and vegetables instead of sweets and participating in PA instead of watching television) The participants experience of the intervention was positive and identified methods to improve future interventions. | No | |
| Leme et al. [77] | To help achieve healthy food choices, promote lifestyle and lifetime PA, and reduce screen time activities | Intervention components included enhanced PE classes, PA leadership book, recess PA, weekly nutrition and PA messages delivered by teachers during recess, three interactive seminars led by dietitians, nutrition and PA handbook, nutrition workshops, dietary and PA diaries, parents’ newsletters, text messages to students twice a week to encourage them to be physically active and eat healthily. Number of participants = 142. | Dieticians and teachers | 6 months | Social-Cognitive Theory |
| No significant effect for BMI (F = 2.120, p = 0.135). | Yes | |
| Lubans et al. [71] | To promote PA and healthy eating and prevent obesity among inactive adolescent girls | The Nutrition and Enjoyable Activity for Teen (NEAT) Girls combined a range of strategies to promote lifestyle (e.g., walking to school) and lifetime PA (e.g., resistance training), improve dietary intake, and reduce sedentary behaviours. Intervention components included enhanced school sport sessions and lunchtime PA, nutrition workshops, interactive educational seminars, pedometers for self-monitoring, student handbooks, parent newsletters, text messages to reinforce and encourage health behaviours. Number of participants = 179. | Teachers, researchers, dieticians | 12 months | Social Cognitive Theory |
| After 12 months, changes in BMI (adjusted mean difference, −0.19; 95% CI, −0.70 to 0.33), BMI z score (mean, −0.08; 95% CI, −0.20 to 0.04), and body fat percentage (mean, −1.09; 95% CI, −2.88 to 0.70) were in favour of the intervention, but they were not statistically different from those in the control group. | Yes | |
| PA (only) Interventions (n = 9) | |||||||||
| Bandeira et al. [76] | To promote PA and reduce the screen time | Teacher training, which was focused on lifestyle behaviours, including excessive screen time, and its implications for health support material, was delivered to teachers to assist them in organising classes on the topic. Component opportunities were created to encourage PA and decrease screen time in the school environment so that adolescents could play games/sports during free time at school. Supervised sessions of 10–15 min (“Gymnastics at School”) were performed twice a week. Health education messages were spread across the schools, and pamphlets were handed over to students/parents. The messages were also addressed to the psychosocial (self-efficacy, attitude, and social support) and environmental aspects of the practice of PA and reducing sedentary behaviour, especially screen time. Number of participants = 548. | Teachers and school staff, undergraduate PE students | 4 months (one semester) | Socio-Ecological Model, Health-Promoting Schools and Social Cognitive Theory |
| There were no significant differences between intervention and control groups for reduction on screen time, in both sexes (boys: 0.105 h/day, 95% CI: −0.184 to 0.393, p = 0.477; girls: −0.065 h/day, 95% CI: −0.383 to 0.252, p = 0.686) and age groups (11–13 years: −0.046 h/day, 95% CI: −0.630 to0.538, p = 0.878; 14–17 years: 0.193 h/day, 95% CI: −0.077 to 0.464, p = 0.162). | Yes | |
| Casey et al. [74] | To improve health-related quality of life (HRQoL), levels of PA, and a range of potential mediators of PA (e.g., self-efficacy, perceived sport competence). | School PE component which incorporated student-centred teaching approaches and behavioural skill development. The PE component involved students participating in two 6-session units, each designed as one session per week during their ‘normal’ PE class time. The two units were a sport unit (tennis or football) and a recreational unit. The curriculum and teaching approach drew on the principles of Game Sense, an Australian derivative of the Teaching Games for Understanding approach, and productive pedagogies in curriculum development. Number of participants = 362. | PE teachers, community fitness instructors and sports coaches | One academic year | Socio-Ecological Model and Social Cognitive Theory |
| After adjustment for baseline levels of PedsQL, the intervention group had significantly higher scores on all three PedsQL scores: physical functioning (adjusted M ± SE = 83.9 ± 0.7, p = 0.005), psychosocial (79.9 ± 0.8, p = 0.001) and total score (81.3 ± 0.7, p = 0.001)—than the control group (80.9 ± 0.8; 76.1 ± 0.9 and 77.8 ± 0.8, respectively), suggesting that the program positively influenced HRQoL. Differences in PedsQL were also present in the 3-group analysis (intervention completers, intervention non-completers and control), whereby the intervention non-completers had significantly higher scores (84.0 ± 0.8, p = 0.021; 80.4 ± 0.9, p = 0.003; and 81.7 ± 0.8, p = 0.002, respectively) than the control group (80.9 ± 0.8, 76.1 ± 0.9 and 77.8 ± 0.8, respectively). There was no statistically significant difference in either the 2-group or 3-group analysis for mins of leisure time (LT) MVPA, MET-mins of LTMVPA, or in the proportion meeting PA guidelines. | Yes | |
| Fróberg et al. [80] | To improve MVPA, sedentary time, exercise training frequency and duration | The intervention was developed and implemented as a result of cooperation and shared decision making among the researchers and the participants.Components included health coaching, health promotion sessions and a closed Facebook group. Number of participants = 54. | PhD students | 2 years | None reported |
| There were no significant effects on changes in the accelerometer-measured MVPA (β = 0.26, 95% CI = [0.08; 0.43]) and sedentary time (β = −0.19, 95% CI = [−0.55; 0.15]), or the self-reported ET frequency (β = 0.03, 95% CI = [−0.25; 0.33]) and duration (β = 0.27 [95% CI = 0.01;0.60]), among the adolescents | No | |
| Hollis et al. [75] | To reduce the decline in PA typically observed during adolescence | The intervention components targeted the school curriculum, school environment, and broader community and parental support. School curriculum included teaching strategies to maximise student PA in health and PE lessons, development and monitoring of student PA plans within PE lessons and the implementation of a 10 week enhanced school sports programme.School environment included the development and modification of school policies, PA programmes during school breaks and promotion of community PA providers. Additional interventions strategies included an in-school PA consultant 1 day per week, establishing leadership and support, teacher training resources, teacher prompts and intervention implementation performance feedback to schools. Parent engagement: information was regularly sent to the parents via school newsletters, the school website and newsletters on PA recommendations, school-based PA strategies, promotion of community PA providers and strategies to support their child’s PA. Number of participants = 645. | Teachers | 19–24 months (7–9 school terms) | Social-Cognitive Theory and Socio-Ecological Model |
| At 12 months, there were group-by-time effects for weight (mean difference (95% CI) =−0.90 kg (−1.50; −0.30), p < 0.01) and BMI (−0.28 kg m−2 (−0.50; −0.06), p = 0.01) in favour of the intervention group, but not for BMI z-score (−0.05 (−0.11; 0.01), p = 0.13). These findings were consistent for weight (−0.62 kg (−1.21; −0.03), p = 0.01) and BMI (−0.28 kg m−2 (−0.49; −0.06), p = 0.01) at 24 months, with group-by-time effects also found for BMI z-score (−0.08 (−0.14; −0.02), p = 0.02) favouring the intervention group. Intervention effects were significant for all adiposity outcomes at 12 and 24 months in both the complete cases and multiple imputation analyses. There was weak evidence of a differential treatment on effect on weight in males compared with females (three-way interaction p = 0.22). Among males there, was a statistically significant treatment effect at 24 months in favour of the intervention group (−1.26 kg (−2.11; −0.41), p = 0.01). There were no significant effects on weight, BMI and BMI z-score at either 12 or 24 months for females. There was weak evidence of a differential treatment on effect on weight in males compared with females (three-way interaction p = 0.22). Among males, there was a statistically significant treatment effect at 24 months in favour of the intervention group (−1.26 kg (−2.11; −0.41), p = 0.01). There were no significant effects on weight, BMI and BMI z-score at either 12 or 24 months for females. Weight status at baseline: minimal evidence of differential treatment effects depending on baseline weight for weight (p = 0.50), BMI (p = 0.57) or BMI z-score (p = 0.64). PA level at baseline: no evidence of differential treatment effects depending on activity status at baseline for weight (p = 0.94), BMI (p = 0.95) or BMI z-score (p = 0.31). There was no significant effect on weight, BMI or BMI z-score for either active or inactive students at 12 or 24 months. | Yes | |
| Robbins et al. [48] | To facilitate long-term attainment of adequate MVPA by enhancing girls’ perceptions of perceived benefits, self-efficacy, enjoyment, social support, role models, autonomy, relatedness, competence and reducing barriers relative to PA | A 90 min PA club included organisational tasks (recording attendance and putting equipment away), healthy snacks, warm up activities, encouragement of MVPA, incorporation of information from the Health Promotion Model and Self-Determination Theory and varying forms of PA. Number of participants = 752 | PA club manager and 3–4 PA club instructors | 17 weeks | Health Promotion Model and Self-Determination Theory |
| Reach: Across the 3 years, the total mean attendance at the PA club was 20.54 ± 16.50 days, equivalent to 41% attendance. 93 evaluations were used to measure dose. Dose Received (exposure): The mean accelerometer measured MVPA time was 21.85 ± 6.16 min, and the average number of steps was 2826 ± 820. Dose Received (satisfaction): 88 of the 93 (95.7%) observations by the process evaluators indicated that the girls liked the PAs conducted in the club, and all agreed that girls liked their club instructors. 451 girls completed the satisfaction questionnaire after the 17-week intervention. On average, 87.8% (n = 396) liked the activities offered in the club, and 85.4% (n = 385) liked the club coaches/managers. Fidelity: process evaluators perceived that the PA club was well received by the girls and delivered with high quality by the coaches/managers. In addition, girls perceived the club was successful in increasing their PA. | Yes | |
| Robbins et al. [47] | To facilitate long-term attainment of adequate MVPA by enhancing girls’ perceptions of perceived benefits, self-efficacy, enjoyment, social support, role models, autonomy, relatedness, competence and reducing barriers relative to PA | A 90 min PA club included organisational tasks (recording attendance and putting equipment away), healthy snacks, warm up activities, encouragement of MVPA, incorporation of information from the Health Promotion Model and Self-Determination Theory and varying forms of PA. Number of participants = 752. | PA club manager and 3–4 PA club instructors | 17 weeks | Health Promotion Model and Self-Determination Theory |
| No significant between-group differences in BMI-z existed at post-intervention, but % body fat increased less among intervention than control group girls (Mchange = 0.43% vs. 0.73%). Aerobic performance decreased less in intervention vs. control (Mchange = −0.39 vs. −0.57). | Yes | |
| Romero [61] | To increase frequency of vigorous PA | The first 20 min of lessons were interactive sessions focused on lesson content followed by 30 min break dancing sessions. Lessons were created in collaboration with key stakeholders (middle school students, middle school teachers, health educators, and local break dancers). Key components of the intervention were based on Social Cognitive Theory and included the following: self-efficacy, culturally similar social role models, positive specific feedback on behaviour by teachers and peers, regular logs of PA, setting measurable goals, and identifying neighbourhood resources for PA. Number of participants = 71. | Bilingual/bicultural female university students | 5 weeks | Social Cognitive Theory |
| For girls, a significant increase in vigorous exercise was found from pre-test to post-test, but this was not significant for boys. No significant differences were found in dance frequency. | No | |
| Roth et al. [58] | Predisposing, enabling, and reinforcing factors for PA as well as self-reported PA | Intervention schools were provided a middle school PE curriculum, $2500 in equipment vouchers for use in PE classes, and a $200 stipend for completing all 12 h of the training. Number of participants = 3763. | PE teachers | 2 years | Social Learning Theory |
| While there were no detectable intervention effects on daily PA, there was a negative intervention effect detected for weekly muscle strengthening PA. | No | |
| Smith et al. [73] | To examine the mediating effect of resistance training skill competency on percentage of body fat, muscular fitness and PA | Intervention components included researcher-led seminars for students, provision of fitness equipment to schools, smartphone application and website, pedometers for self-monitoring, parental strategies for reducing screen time (i.e., newsletters), lunch-time PA mentoring sessions and face-to-face activity sessions run by teachers during the timetabled school sport period. Number of participants = 181. | Teachers | 20 weeks | Self-Determination Theory and Social Cognitive Theory |
| The mediated effect was statistically significant for percentage of body fat (B [SE] = −0.95 [.26]; 95% CI = −1.49 to −0.47) and muscular fitness (B [SE] = 0.16 [.07]; 95%CI = 0.03 to 0.31). The mediated effect was not significant for MVPA (B [SE] = 0.50 [2.1]; 95%CI = −3.6 to 4.6). | Yes | |
| Mental Health Interventions (n = 7) | |||||||||
| Araya et al. [85] | To reduce depressive symptoms among low-income secondary school students | The intervention consisted of 11 weekly and 2 booster sessions, each lasting approximately 1 h. There was an introductory session, 6 sessions dealing with thought restructuring and emotions, 3 sessions of problem-solving strategies, and 1 closing session to revise and integrate all previous work. Two booster sessions delivered at months 2 and 7 reviewed challenging negative thoughts and problem-solving strategies. Number of participants = 1221. | Psychologists, occupational therapists, and social workers) | 3 months | Cognitive Behavioural Model |
| There was no evidence of any clinically important differences between the intervention and control arms in depressive symptoms scores at 3 months (adjusted difference in means, −0.19; 95% CI, −1.22 to 0.84; p = 0.72) or at 12 months. The adjusted difference in the primary outcome at 3 months between trial arms was −0.15 (95% CI, −1.12 to 0.81; p = 0.75) with 20 imputed full data sets. | Yes | |
| Dray et al. [72] | To increase the provision of universal strategies targeting multiple internal and external resilience protective factors | A framework of sixteen intervention strategies. Each strategy was designed to address one or more internal or external resilience protective factor. Intervention schools were asked to meet the prescribed set of strategies; however, schools were given the flexibility to select which specific programs or resources to implement to address each of the strategies. (The 16 strategies are detailed in the paper.)Number of participants = 1909. | Teachers | 3 years | None reported |
| There was no significant difference between intervention and control groups for the outcomes of total SDQ, internalising problems and prosocial behaviour There was a significant difference for the outcome of externalising problems in favour of the control group, though the magnitude of effect was small (b¼0.43, 95% CI: 0.04 to 0.83, p¼0.02) | Yes | |
| Frazier et al. [56] | To leverage recreational activities for social emotional learning | Leaders @ play: The program included didactic instruction, skills demonstration and discussion, role plays, and sports and recreation to provide practice with feedback. The first two sessions included team building activities; introduction to the Good Behaviour Game; and orientation to the junior camp counsellor internship. Intervention content emphasised social problem solving, emotion regulation, and effective communication. The last two sessions included review, celebration, and preparation for summer camp. Families @ Play: Multi-family groups comprised of youth, parents, and extended family were designed to meet twice per month for 90 min. The format and content mirrored those of Leaders @ Play. The primary goal was to introduce a targeted skill (problem solving, emotion regulation, or effective communication), accompanied by specific strategies by which families could model and reinforce them at home. Number of participants = 46. | Physical instructor, park recreation leaders, park supervisors, mental health providers | Leaders @ play = 10 weeks. Parents @ play = 10 weeks | None reported |
| There were no significant changes in parent report of Social Skills over time: baseline to post-test: t 62 = −0.23, n.s., post-test to follow up: t 50 = 1.19, n.s, and baseline to follow up: t 64 = 1.08, n.s. Despite a trended increase in parent-reported Problem Behaviours from baseline to post-test, t 65 = −1.84, p = 0.56 (Cohen’s d = −0.46), these ratings returned to baseline levels by follow up, t 50 = 1.83, p = 0.07 (post-test to follow up) and t 65 = 0.26, n.s. (baseline to follow up). Staff-reported Problem Behaviours for the total sample across sites showed no change from baseline to post-test, t 49 = 1.64, n.s., but declined significantly by follow up, t 61 = 2.04, p < 0.05 (post-test to follow up) and t 60 = 3.75, p < 0.0001 (baseline to follow up). Staff-reported Social Skills improved from baseline to post-test, t 51 = −2.56, p = 0.01 and follow up, t 63 = −2.11, p < 0.05, and gains were maintained from post-test to follow up, t 62 = 1.49, n.s. Effect sizes based on overall means from the total sample showed staff-reported reductions in Problem Behaviours (d = 0.46 at post-test and 0.88 at follow up) and gains in Social Skills (d = −0.72 and −0.53, respectively). | Yes | |
| Mendelson et al. [53] | To enhance social, emotional, and academic functioning | RAP Club incorporates psychoeducation, cognitive behavioural, and mindfulness strategies from three evidence-supported treatments: Dialectical Behaviour Therapy for Adolescents, Trauma Adaptive Recovery Group Education and Therapy and School-Based Trauma/Grief Group Psychotherapy. Number of participants = 29. | Co-facilitated by a mental health counsellor and young adult community member | 6 weeks | None reported |
| Compared with controls, intervention students improved on teacher rated dysregulation (F(1,43) = 7.94, p < 0.01, d = 0.85), social competence (F(1,43) = 8.32, p < 0.01, d = 0.87), academic competence (F(1,45) = 6.65, p < 0.05, d = 0.76), and authority acceptance (F(1,43) = 5.43, p < 0.05, d = 0.69). The pattern of scores was in the predicted direction for all the other teacher-reported outcomes, except attention. Student-reported outcomes did not differ by study condition. 17% of intervention students had elevated baseline depression; all displayed a pattern of reduced post-test symptoms. 83% of intervention participants reported low baseline depression; compared with control participants with low baseline depression, these students showed improved teacher-rated dysregulation (t(39) = 2.9, p < 0.01), social competence (t(38) = −2.57, p < 0.05), academic competence (t(40) = −2.27, p < 0.05), authority acceptance (t(39) = 2.53, p < 0.05), and disciplinary sanctions ((t(39) = 2.28, p < 0.05) Higher program dose was associated with greater improvement than low dose on teacher-rated academic comparison (t(1,25) = 2.93, p < 0.01), discipline (t(1,25) = 2.24, p < 0.05), and conduct problems (t(1,25) = 2.4, p < 0.05). | No | |
| Schleider et al. [51] | To reduce depressive symptoms, social anxiety symptoms, and conduct problems | Growing Minds (GM): A self-administered, computerised single-session intervention (SSI) which includes content related to multiple types of mind-sets (personality, intelligence, self-regulation) across four interactive modules. Number of participants = 115. | Self-administered on a computer. Research assistance was available for assistance if needed | 1 session | None reported |
| Relative to girls in the control group, girls receiving the GM-SSI reported modest but significantly greater reductions in depressive symptoms (d = 0.23) and likelihood of reporting elevated depressive symptoms (d = 0.29) from baseline to follow up. GM-SSI effects were non-significant for social anxiety symptoms, although a small effect size emerged in the hypothesised direction (d = 0.21), and non-significant for change in conduct problems (d = 0.01). | No | |
| Sethi et al. [83] | To improve attention and self-efficacy | All the students participated in the yoga course for 5 days. The module was selected from Integrated Approach of Yoga Therapy for positive health. Number of participants = 60. | Not reported | 5 days | None reported |
| The intervention resulted in a significant increase in self-efficacy (p = 0.001) and attention scores (p < 0.001). | No | |
| Shinde et al. [82] | To improve school climate and health-related outcomes | The intervention identifies four priority areas for action: promoting social skills among adolescents; engaging the school community in school-level decision-making processes; providing access to factual knowledge about health and risk behaviours to the school community; and enhancing problem-solving skills among adolescents. The intervention strategies were organised at three levels—whole school, group, and individual levels—and include school health committee, awareness generation fun activities, speak out box (letterbox), wall magazine, competitions (debates, poster making, quizzes, etc.), health policies, peer groups, workshops, individual counselling. Number of participants in the teacher-led intervention = 4046. Number of participants in the lay counsellor-led intervention = 4524. | Lay counsellor (SM) or teacher (TSM) | One academic year | None reported |
| Participants in the SM-delivered intervention schools had substantially higher school climate scores at endpoint survey than those in the control group (BBSCQ baseline-adjusted mean difference [aMD] 7·57 [95% CI 6·11–9·03]; effect size 1·88 [95% CI 1·44–2·32], p < 0·0001) and the TSM-delivered intervention (aMD 7·57 [95% CI 6·06–9·08]; effect size 1·88 [95% CI 1·43–2·34], p < 0·0001). There was no effect of the TSM-delivered intervention compared with control (aMD −0·009 [95% CI −1·53 to 1·51], effect size 0·00 [95% CI −0·45 to 0·44], p = 0·99). | Yes | |
| Diet Interventions (n = 4) | |||||||||
| Luesse et al. [54] | To increase intake of whole/minimally processed foods, operationalised as fruit and vegetables, and decrease intake of highly processed foods, operationalised as sugar-sweetened beverages, fast foods, and processed-packaged snacks | In ’Defence of Food’ is a health education curriculum of 10 sequential 2 h educational lessons. The lessons were structured into three units, consisting of three lessons each, followed by a final celebration lesson. Key aspects of lessons included food rules, film clips, food preparation/tasting, goal setting.(Detailed curriculum components within the paper.) Number of participants = 32. | After-school program teachers | 10 weeks | Social Cognitive Theory and Self-Determination Theory |
| There was a significant increase in mean frequency of fruit and vegetable intake at post-test compared with pre-test (t = 3.359, p < 0.01)—an effect size that is considered to be large (d = 0.59). Small effect sizes (d = 0.34) were seen for mean intakes of highly processed foods but change in score was not statistically significant (p = 0.06). Statistically significant increases in outcome expectations and self-efficacy for fruit and vegetable intake occurred from pre-test to post-test; all other mediators showed no statistically significant changes. Youth discussed supports for eating fruit and vegetable intake, including social support and modelling, the application of self-regulation skills to increase intake, and their expressed preferences for fruit and vegetable. Youth were also preoccupied with the negative physical outcome expectations of eating highly processed foods, such as developing diabetes. | No | |
| Brito Beck da Silva et al. [78] | To promote adequate and healthy eating | Eight meetings lasting 50 min each were provided to promote healthy eating and PA. The topics covered were: 1) healthy eating; 2) PA and sports; 3) fats, sugars and salt: effects of a poor diet; 4) nutritional evaluation: The basics; 5) use of supplements in PA: A critical approach; 6) food labelling: food and nutritional safety; 7) role of nutrients in health promotion: functional foods with a focus on fruits, vegetables and legumes; 8) good food handling practices. A webpage was created in a social network used by the adolescents, in which videos, trivia and general guidelines on healthy eating were posted.For parents and/or guardians, didactic-educational materials were sent through adolescents to encourage them to maintain a healthy lifestyle. Number of participants = 387. | Nutritionists | 9 months | None reported |
| The intervention group exhibited decreases of 7.64 mg/dL (2.94 mg/dL) in mean TC (p = 0.009) and 7.77 mg/dL (2.60 mg/dL) in mean LDLc (p = 0.003) and increases of 18% in legume consumption (OR = 1.18; 95% CI 1.03–1.37) and 17% in vegetable consumption (OR = 1.17, 95% CI 1.01–1.35) compared with those who did not undergo intervention at the end of the 9-month follow up. No differences were noted in the anthropometric parameters studied. | No | |
| Knapp et al. [60] | To address individual, social, and environmental factors that affect dietary behaviours | Interactive, garden and kitchen-based curriculum classes during school hours as well as afterschool programming for students. Students were involved in growing, harvesting, preparing, and eating food. Programming also extends beyond the classroom to involve families, school staff, and community members in activities and events, such as family food nights, open garden days, and parent cooking classes. Number of participants = 27. | Program teachers | Not reported | None reported |
| Four primary themes emerged from the focus group data: (1) development of life skills, (2) food and health, (3) family and community, and (4) experiential and participatory learning environment. These core themes and subcategories of the themes were organised into levels of the socioecological model. | No | |
| Alaimo et al. [62] | To improve school nutrition practices (including nutrition education) and policies, and to improve student dietary intake | Schools were asked to convene a Coordinated School Health Team (CSHT) with representatives from various sectors of the school (administration, faculty, food service, health care, and students).Schools were provided with a trained facilitator to meet with their CSHT on one time to complete the healthy School Action Tool (HSAT) healthy eating and nutrition topic area (questions on the following topics: school nutrition policies, school nutrition environment, school health education programs including nutrition education, and school food service programs). At the end of each module, schools were to identify several “bright ideas” they could implement. Schools were asked to prioritise their goals and received $1000 to implement nutrition education or nutrition marketing activities in their action plans.Number of students unknown (40 schools). | Not reported | 2 years | None reported |
| Schools that completed the HSAT prior to but not during the School Nutrition Advances Kids (SNAK) project reported adopting more nutrition policies than schools that never completed the HSAT or a similar program (2.2 vs. 0.4 nutrition policies).Schools that completed the HSAT at any time (prior to but not during the SNAK, during but not prior to, and both prior and during the SNAK project) reported adopting significantly more nutrition practices than schools that never completed the HSAT or a similar program (6.8, 5.8, 7.0, vs. 1.6 nutrition practices, respectively). Schools that completed a similar assessment or grant program before or after the SNAK project also reported adopting significantly more nutrition practices than schools that never completed the HSAT (4.3 vs. 1.6 nutrition practices). Students in schools that were randomised to complete the HSAT reported consuming significantly more fruit (17.5%) and fibre (4.9%) and less cholesterol (4.2%) than students in the control schools. Students in schools that completed the HSAT during the intervention reported consuming significantly more fruit (20.1%) and fibre (5.1%) and less cholesterol (8.4%) than students in schools that had never completed the HSAT. | No | |
| Substance Abuse (n = 2) | |||||||||
| Vicary et al. [68] | To reduce the risk for initiation of substance abuse or reduce increased use in high-risk females | The life skills training (LST) condition, which is usually taught by a limited number of teachers in a series of classes dedicated to substance abuse prevention. The infused (I)-LST condition integrates life skills training and alcohol, tobacco or other drugs (ATOD) information into a variety of the existing grade level subject curricula by the teachers for these subject areas. The goal of such an approach is to make prevention an integral part of the total curriculum. I-LST teachers were trained by university/project staff. Number of participants (LST) = 234. Number of participants (I-LST) = 297. | Teachers | 2 years | None reported | Students’ self-report of:
| The LST low-risk females reported a significantly lower frequency of alcohol use, less binge-drinking, and less marijuana use, while the I-LST low-risk females reported significantly less cigarette smoking. However, the only significant substance use effect that remained for the low-risk females by the end of 8th grade was [less] cigarette smoking for I-LST.Both LST and I-LST positively affected knowledge of alcohol, tobacco, and other drugs. The I-LST program demonstrated a desirable effect on the normative beliefs of the low-risk females at the end of year two. Among skill variables, treatment effects were found for LST low-risk females for decision making, communication, and coping skills at the end of year one, although, at the end of year two, these effects had disappeared. LST females demonstrated significantly worse media resistance skills at the end of year two. Two skill treatment effects existed for the low-risk I-LST females. At the end of year one, I-LST positively affected decision-making skill; however, this effect was reduced to a non-significant level by the end of year two. The I-LST program resulted in greater coping skills by the end of year two for the low- risk females. More positive results were observed, however, for the females at higher risk, with significant treatment effects found in a number of substance use categories. After the first year of programming, high-risk females in the LST program were less likely to use alcohol (both for any drinking and for binge drinking), marijuana, and inhalants. A significant treatment effect was also shown among high-risk females in the I-LST program for drinking, binge drinking, and marijuana use at the end of the first year. The LST program significantly affected pro drug attitudes, normative beliefs, and knowledge of ATOD myths and realities although the effects did not remain at a significant level by the end of year two.The LST program resulted in two treatment effects for the high-risk females, assertiveness and refusal skills. A significant treatment effect was observed for the high-risk females in the I-LST for normative beliefs by the end of year one, although the effect did not remain through year two. A significant I-LST treatment effect was observed for attitudes toward ATOD and refusal skills at year two among the high-risk females. | No | |
| Robinson et al. [50] | To reduce substance use within a sample of low-income, inner-city African American adolescents | School-based health centre (SBHC) social workers and health educators conduct schoolwide prevention/education groups during regular scheduled classes, as well as schoolwide special assemblies and health fairs. The SBHCs operate similarly to a typical physician’s office. A student’s initial visit to the SBHC includes a comprehensive physical and mental health assessment. Alcohol and drug prevention and rehabilitation services are provided in the form of classroom-based preventative health education and individual counselling. Number of participants = 598. | A physician specialising inadolescent medicine, a nurse practitioner, a social worker, a medical assistant, and a health educator | 6 months for 7th graders and 2 years and 6 months for 9th graders | None reported |
| For the analysis of cigarette smoking, a significant grade 3 SBHC interaction effect was found, F(1, 585) 5 3.83, p 5 0.05. The SBHC students smoked slightly less than non-SBHC students in the 9th grade; but, by 11th grade, SBHC students were smoking significantly less than non-SBHC students.The SBHC 3 grade interaction effect for alcohol use was non-significant, F(1, 586) 5 0.39, p 0.50, although students from SBHC schools (M 5 1.32, SD 5 3.24) reported drinking slightly less frequently than students from non-SBHC schools (M 5 1.60, SD 5 3.75), this difference was not significant, F(1586) 5 2.45, p 5 0.12 For marijuana, a significant grade 3 SBHC interaction effect was found, F(1, 587) 5 12.72, p, 0.001. By 11th grade, marijuana use had significantly decreased among SBHC students while marijuana use among non-SBHC students dramatically increased. | No | |
| PA, Diet, Substance Abuse and Mental Health Interventions | |||||||||
| Fardy et al. [59] | To promote health knowledge and behaviour, coronary risk factors, and cardiovascular (CV) fitness | 20–25 min circuit training classes followed by 5 min of health behaviours lecture/discussion (topics included exercise, nutrition, smoking cessation, stress management, heart disease, cancer, and motivation). Student workbook from Stanford Adolescent Heart Health Program and the PA and Teenage Health pilot study. Number of participants = 181. | PE teacher and assisted by undergraduate and graduate PE majors | 11 weeks | None reported |
| Cardiovascular health knowledge scores significancy increased in the intervention group, whereas they decreased in the control group. Significant changes in self-reported dietary behaviour were observed in female subjects. Significant changes in risk factors were restricted to lowered total cholesterol in girls. Mean cholesterol values in female subjects decreased from 165 to 149 mg/dl in the treatment group, whereas female controls decreased from 154 to 150 mg/dl. There were no significant differences in blood pressure, obesity, and self-reported PA. Estimated mean CV improved in females from 33 to 38 mL/kg per min (p < 0.0001), at heart rates of 176 and 152, respectively, whereas control subjects increased only from 33 to 34 mL/kg per min at heart rates of 178 and 172, respectively. In male subjects, treatment and control groups improved from 43 to 52 mL/kg per min and 41 to 49 mL/kg per min, respectively, although the differences between groups were not significant. | No | |
| Mental Health and Sleep Interventions | |||||||||
| Sibinga et al. [63] | To improve mental health and reduce stress | Mindfulness-based stress reduction (MBSR) programs consist of three components: didactic material related to mindfulness, meditation, yoga, and the mind–body connection; experiential practice of various mindfulness meditations, mindful yoga, and the “body scan” during group meetings and encouragement of home practice; group discussion focused on the application of mindfulness to everyday situations and problem solving related to barriers to effective practice. Number of participants = 22. | A mindfulness instructor | 12 weeks | None reported |
| MBSR participants had less anxiety and a reduction in negative coping approaches (p = 0.06). MBSR participants showed an increase in self-reported anger (p =0.06). Otherwise, there were no significant differences between groups. Among all participants, there was an association between the mindfulness subscale “act with awareness” and lower anxiety (p < 0.01). Among MBSR participants, mindfulness subscales were associated with less self-reported angry temperament (pb0.02) and less anger reactivity (p = 0.05). Total cortisol output was not statistically significantly different between groups at baseline or follow up. Overall, cortisol output was higher post-program (p = 0.05). There was a trend towards increasing cortisol over time among ‘healthy-topic’ participants (113.6 to 167.5, p = 0.07); but not among MBSR participants (128.3 to 138.5, p = 0.33).Regression analyses of actigraphy data showed no differences between groups in sleep latency (p = 0.29), WASO (p = 0.42), or sleep efficiency (p = 0.97); also, sleep diaries showed no differences in sleep quality (0.67). | No | |
| PA, Diet and Substance Abuse | |||||||||
| Kerr et al. [52] | To improve dietary behaviours, PA, and substance use knowledge and behaviours | Promoting Health Among Teens (PHAT) is a culturally tailored intervention for African American adolescents, focusing on 3 dimensions of health behaviour (diet, PA and substance abuse) for premature cancer and cardiovascular disease prevention.The intervention interactive learning activities to increase health knowledge, develop health behaviour skills, change attitudes, increase self-efficacy, and explore beliefs regarding personal health behaviours. PHAT utilised cultural pride, goal setting, and instruction in dietary behaviours, PA, nutrition cognition. PHAT was conducted using group facilitation, role playing, games, and classroom multimedia messages. (Specific strategies detailed in the paper.) Number of participants = 834. | Trained interventionists | 2 weeks | Social Cognitive Theory |
| PHAT participants had significantly higher knowledge scores than FOY (control) participants (p ≤ 0.0001), and the rate of increase in condition was significantly higher among PHAT participants than FOY participants (p ≤ 0.0001). Participants with greater general health knowledge for the centred health knowledge variable had significantly higher intercepts for past week fruit consumption (p ≤ 0.01), past week vegetable consumption (p ≤ 0.0001), past month vegetable consumption (p ≤ 0.0001) past week moderate PA (p ≤ 0.0001), past week PA to strengthen or tone muscles (p ≤ 0.01) lifetime alcohol use (p ≤ 0.01), and lifetime marijuana use (p ≤ 0.05). Participants with lower general health knowledge had higher intercepts for past month alcohol use (p ≤ 0.01) and past month marijuana use (p ≤ 0.0001).Participants with lower general health knowledge scores had significantly greater slopes for lifetime alcohol use (p ≤ 0.01). The growth curves for moderate PA and PA to strengthen and tone muscles were not significantly different between PHAT and FOY participants. The level of engagement of vigorous PA was not significantly different between experimental conditions; however, the rates of increase for participants in PHAT were higher than those in FOY. There were no significant differences in growth curve results between experimental conditions for all past month substance abuse behaviour variables, lifetime alcohol use, and lifetime tobacco use. There were significantly higher rates of increase for PHAT participants in lifetime marijuana use (p < 0.0001). Growth curve modelling indicated that participants in PHAT had significantly more gains in health knowledge than participants in FOY, but the effects on behaviour were modest. | Yes | |
| Sleep Interventions | |||||||||
| Quante et al. [57] | To assess the acceptability of sleep apps | Sleep app use to monitor sleep hygiene. Participants could choose between two commercially available sleep apps: ‘SleepBot’© and ‘SleepTime’©. Number of participants = 12. | App based | 2 weeks | None reported |
| There were several barriers identified in relation to the adoption of sleep hygiene interventions, namely reluctance to follow scheduled sleep routines on weekends and concern about “parting” with electronics at bedtime. Participants were intrigued by the idea of adopting an app-based sleep intervention but were sceptical that they could successfully adopt sleep hygiene practices and were more interested in making changes on school days than on weekends. The overall feedback on two commercial sleep apps was positive, with a good adherence and engagement rate, and perceived health benefits. | No | |
| Mental Health and PA | |||||||||
| Beaulac et al. [87] | To promote psychological, social, and physical well-being | The intervention was developed from a thorough literature review, consultation with youth and parents, and ongoing dialogue with community partners. Emphasis was placed on improving dance skills and on fostering positive relationships with peers and adult role model. Number of participants = 67. | Dance instructors (Culture Shock Canada) | 13 weeks | Socio-Ecological Model |
| The findings suggested that the community-based intervention was a promising program for the promotion of youth psychological, social, and physical well-being. The adolescents, parents, and/or personnel described benefits across seven main areas, including dancing and related skills, behaviours (e.g., reduced television viewing), physical well-being, psychological well-being, relationships, respect for others and for diversity, and school performance. | Yes | |
| PA, Diet and Mental Health | |||||||||
| Berria et al. [79] | To improve components of fitness and body image | MVPA, strength and flexibility exercises were increased in PE classes Students were encouraged to use recess time actively with the availability of balls and ropes. Educational sessions were provided on PA, health, nutrition and body image Educational resources used included movie, lectures, confection of posters and music, and cooking workshops Parents were invited to a night-time healthy eating meeting. Number of participants = 328. | PE teachers and a nutritionist | 13 weeks | None reported |
| In the crude analysis for the entire sample and among students with adequate BMI at baseline, there was a greater probability of dropping out with increasing age and BMI. Students classified as overweight were more likely to drop out with increasing age. In the adjusted analysis, the association with age remained for the entire sample, including students with adequate BMI and with overweight. In addition, for the overweight students, participation in the intervention during the afternoon period and the higher socioeconomic status were associated with dropping out of the intervention. | No | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, C.; Goss, H.R.; Issartel, J.; Belton, S. Health Literacy in Schools? A Systematic Review of Health-Related Interventions Aimed at Disadvantaged Adolescents. Children 2021, 8, 176. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030176
Smith C, Goss HR, Issartel J, Belton S. Health Literacy in Schools? A Systematic Review of Health-Related Interventions Aimed at Disadvantaged Adolescents. Children. 2021; 8(3):176. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030176
Chicago/Turabian StyleSmith, Craig, Hannah R. Goss, Johann Issartel, and Sarahjane Belton. 2021. "Health Literacy in Schools? A Systematic Review of Health-Related Interventions Aimed at Disadvantaged Adolescents" Children 8, no. 3: 176. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030176