Orthodontic Treatment of a Patient with Dentin Dysplasia Type I and Bilateral Maxillary Canine Impaction: Case Presentation and a Family-Based Genetic Analysis

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
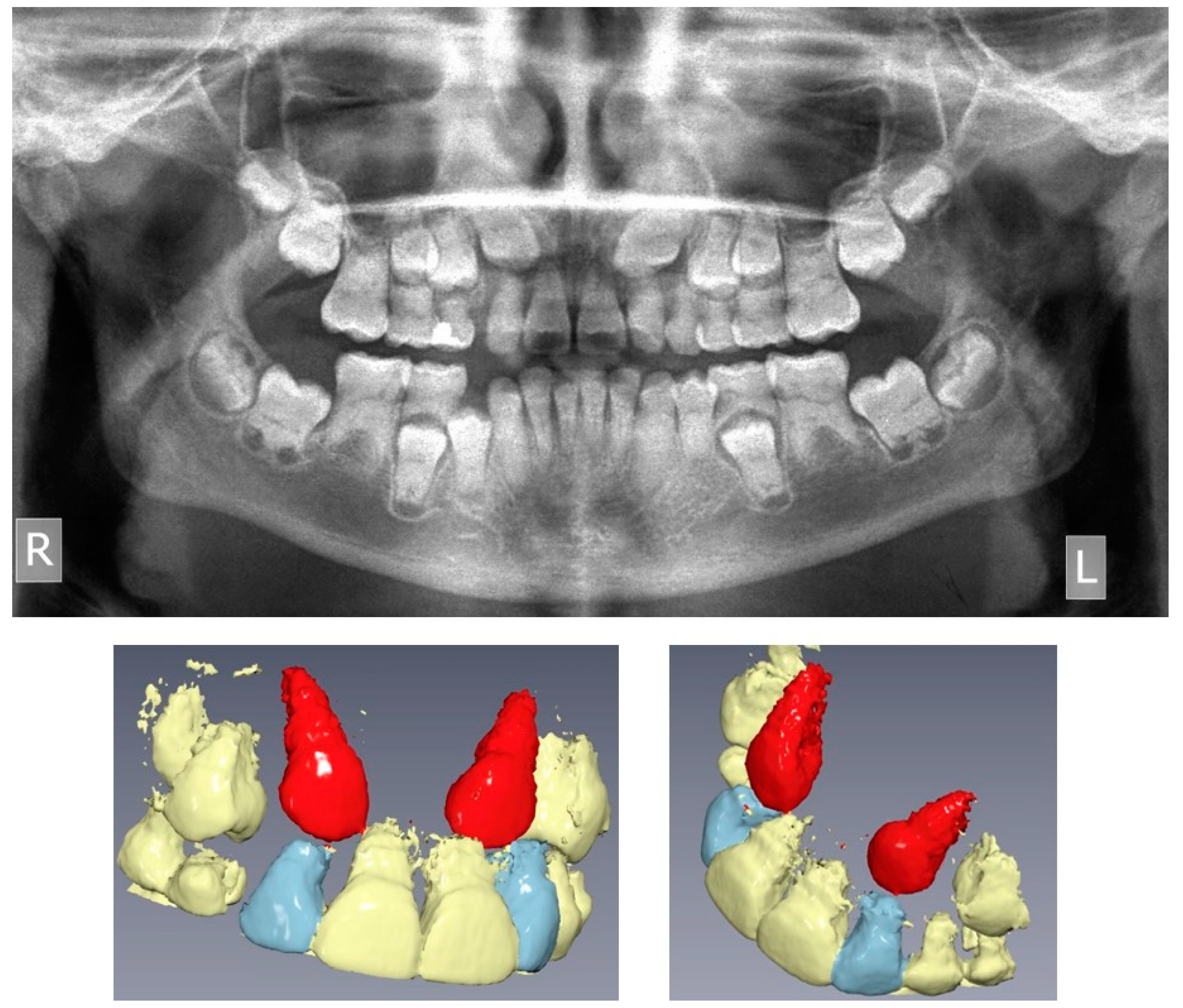
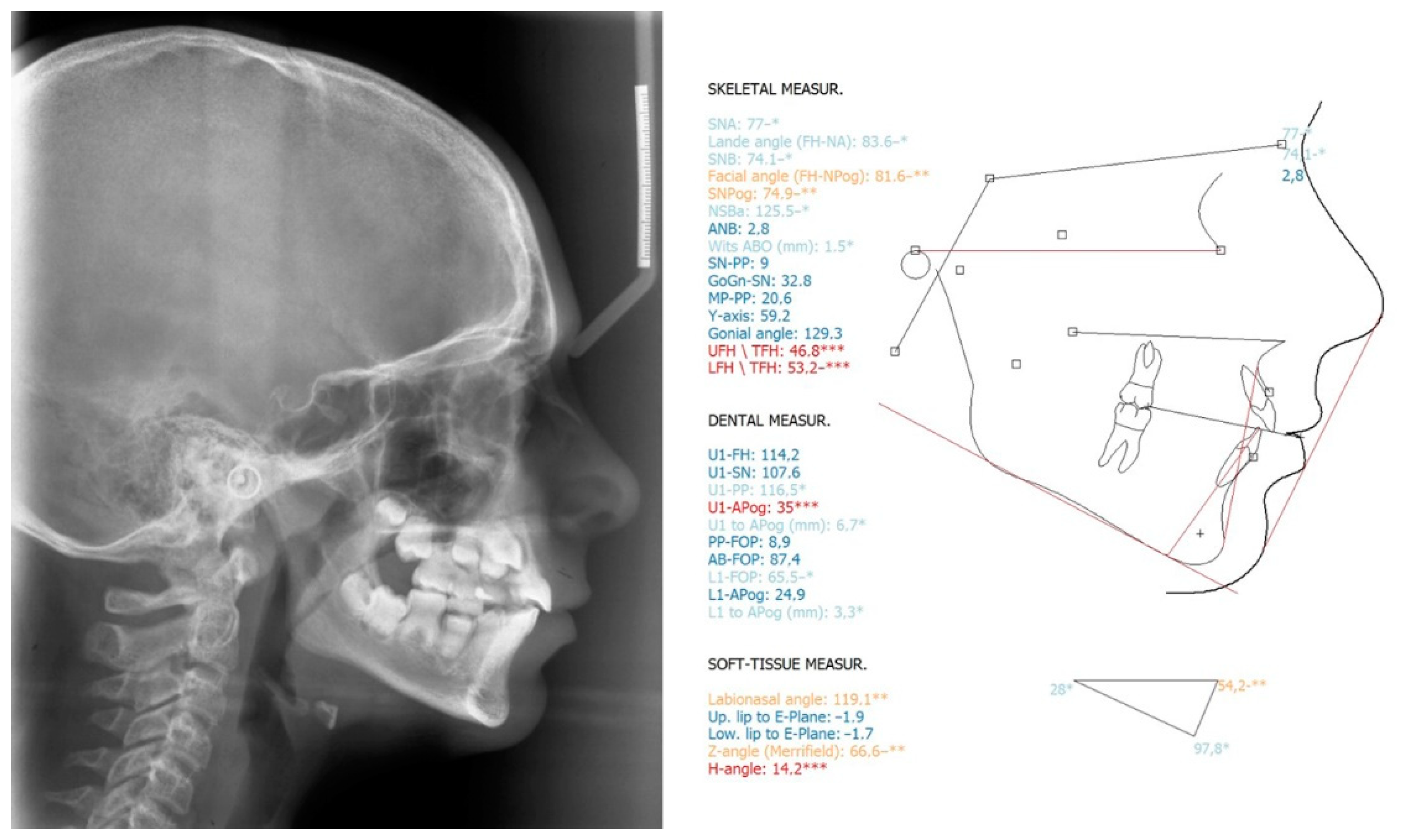
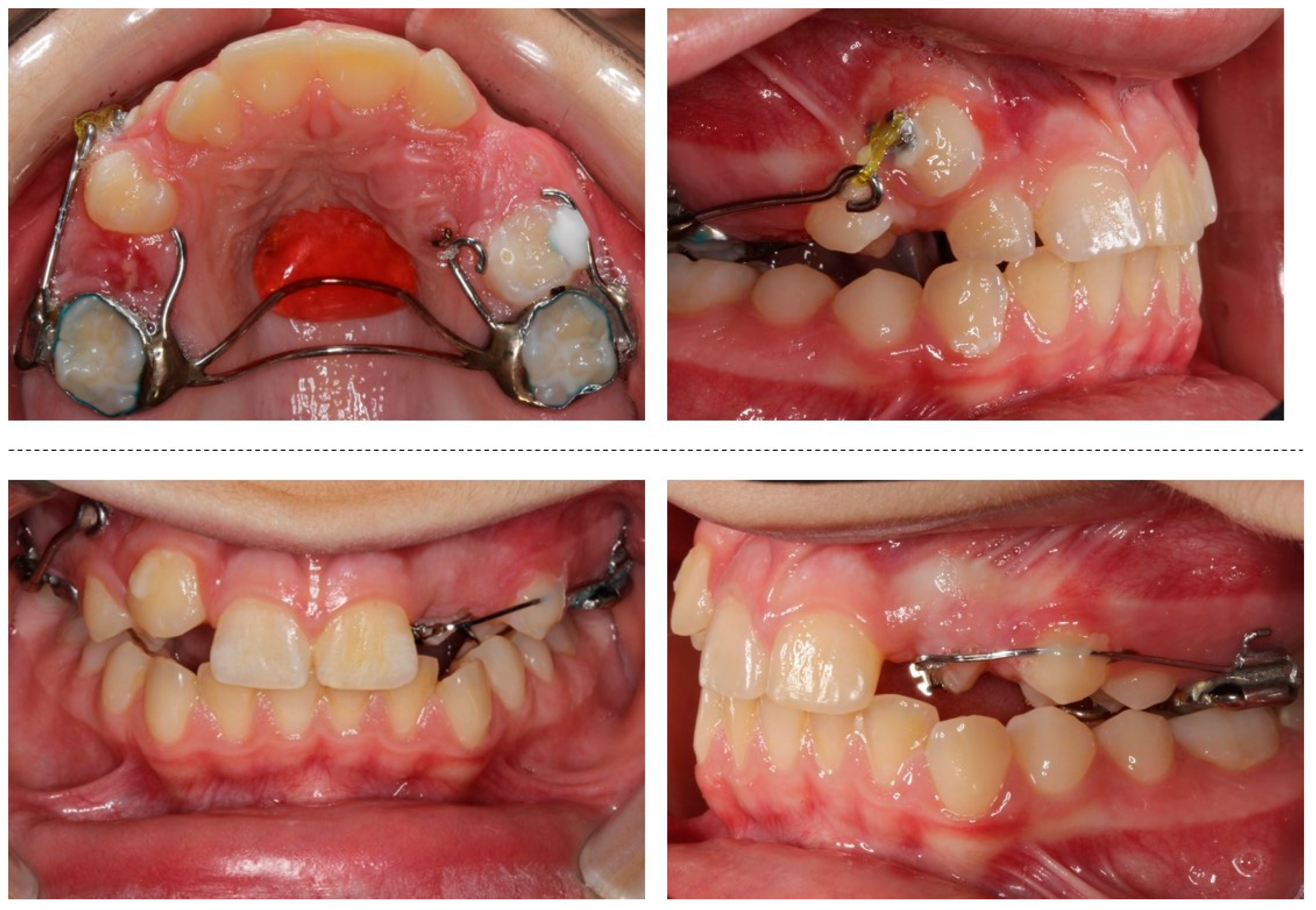
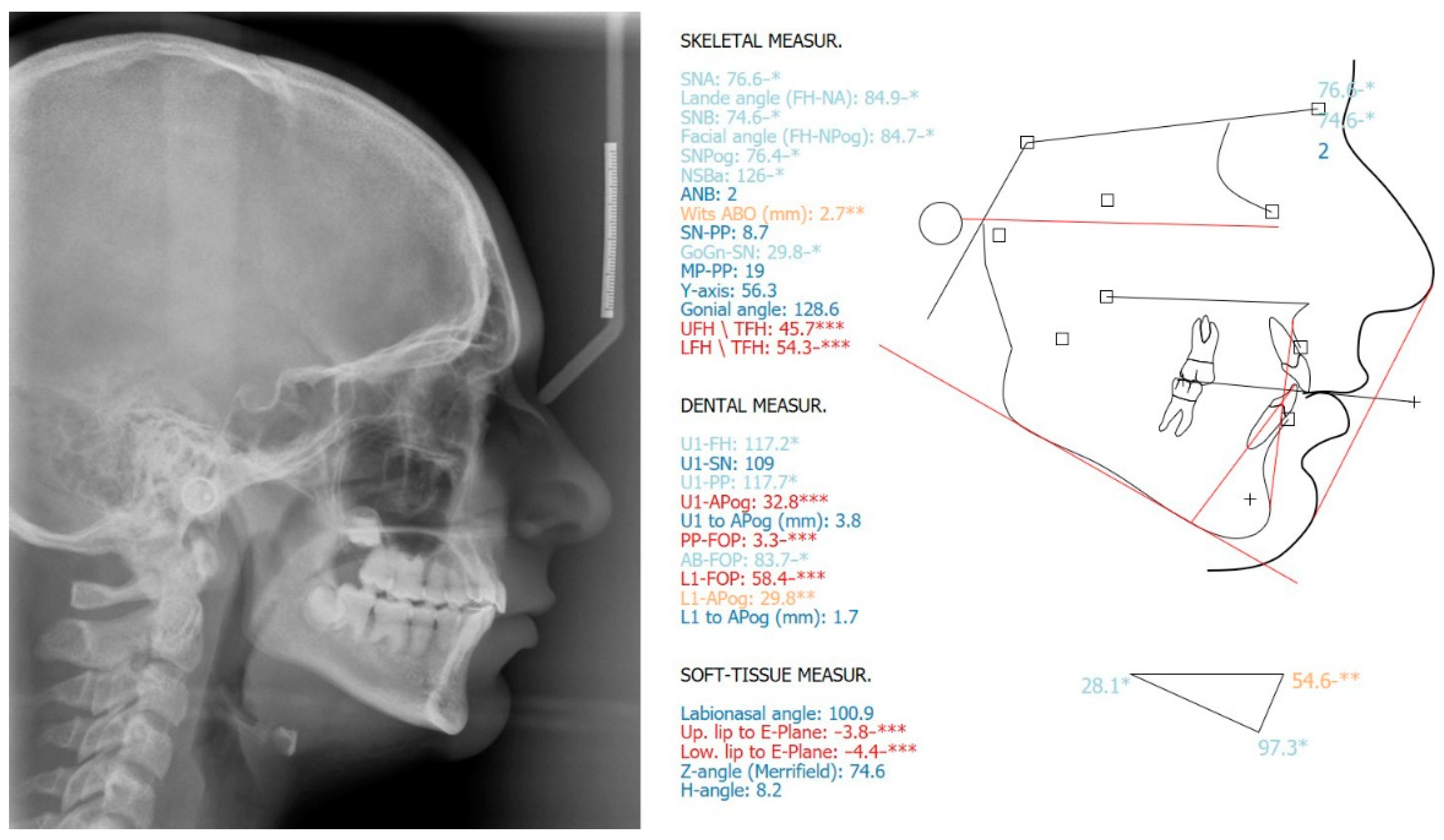
2.1. Clinical Findings and Diagnosis
2.2. Treatment Objectives
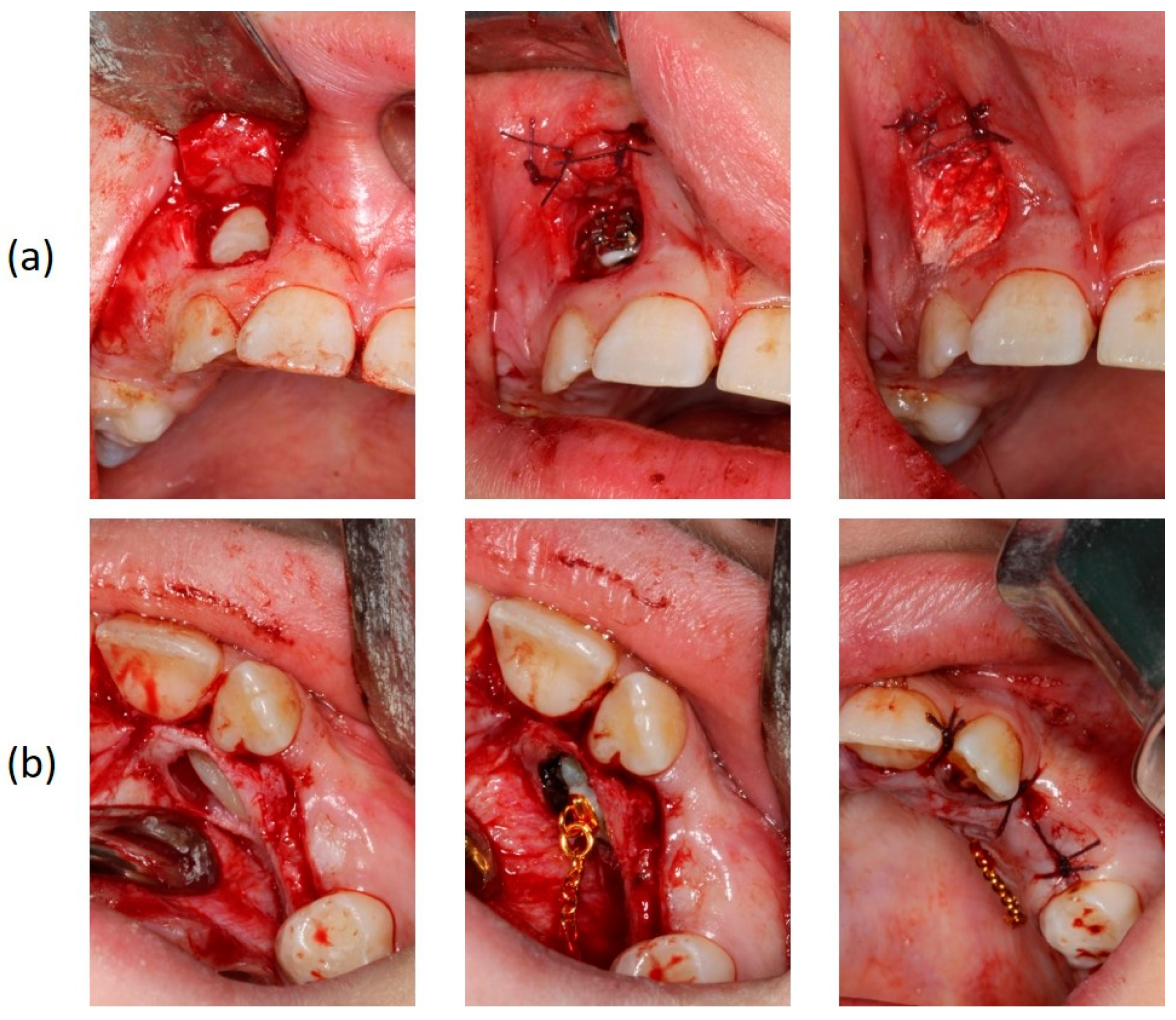
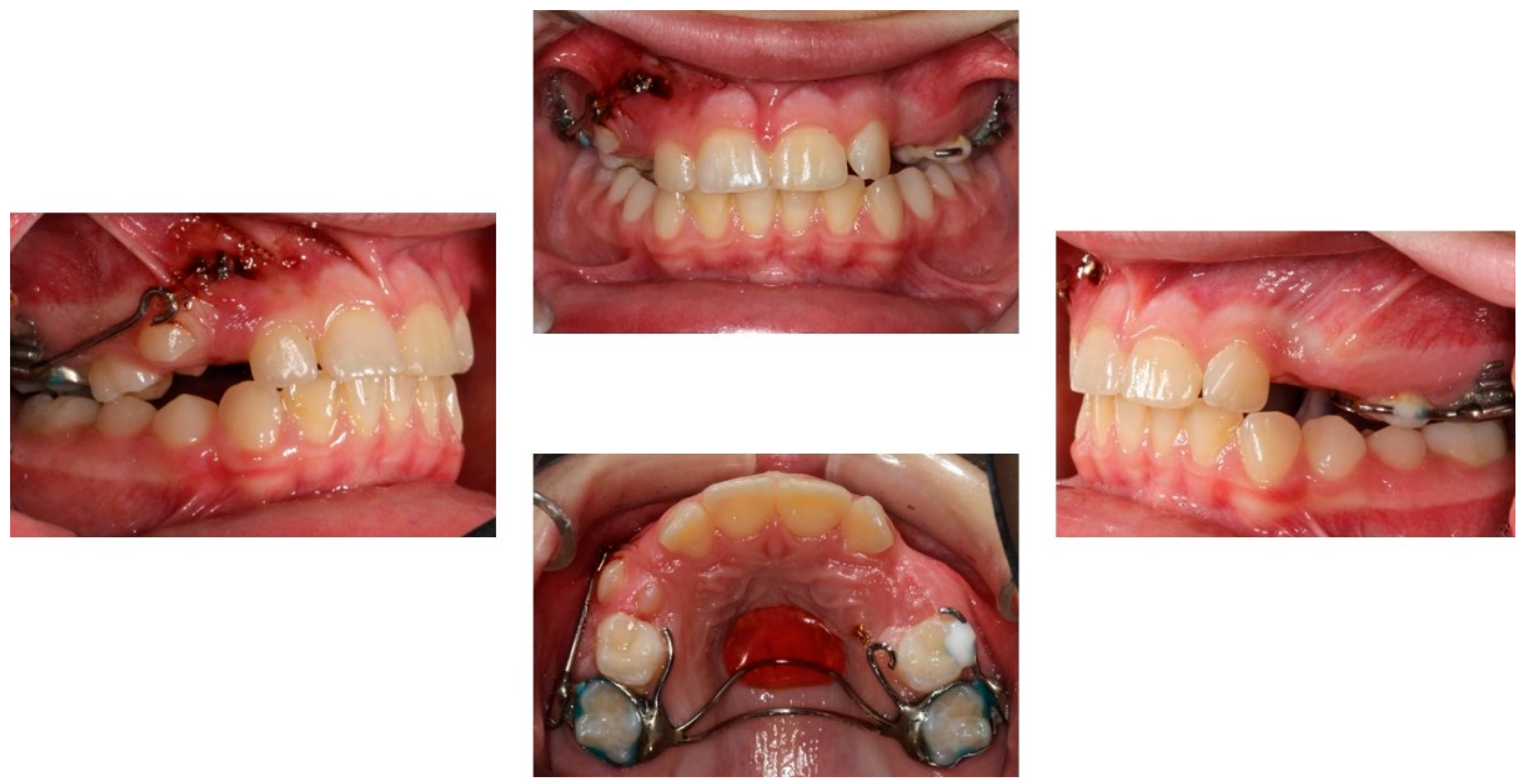
2.3. Treatment Planning
2.4. Treatment Results
2.5. Retention
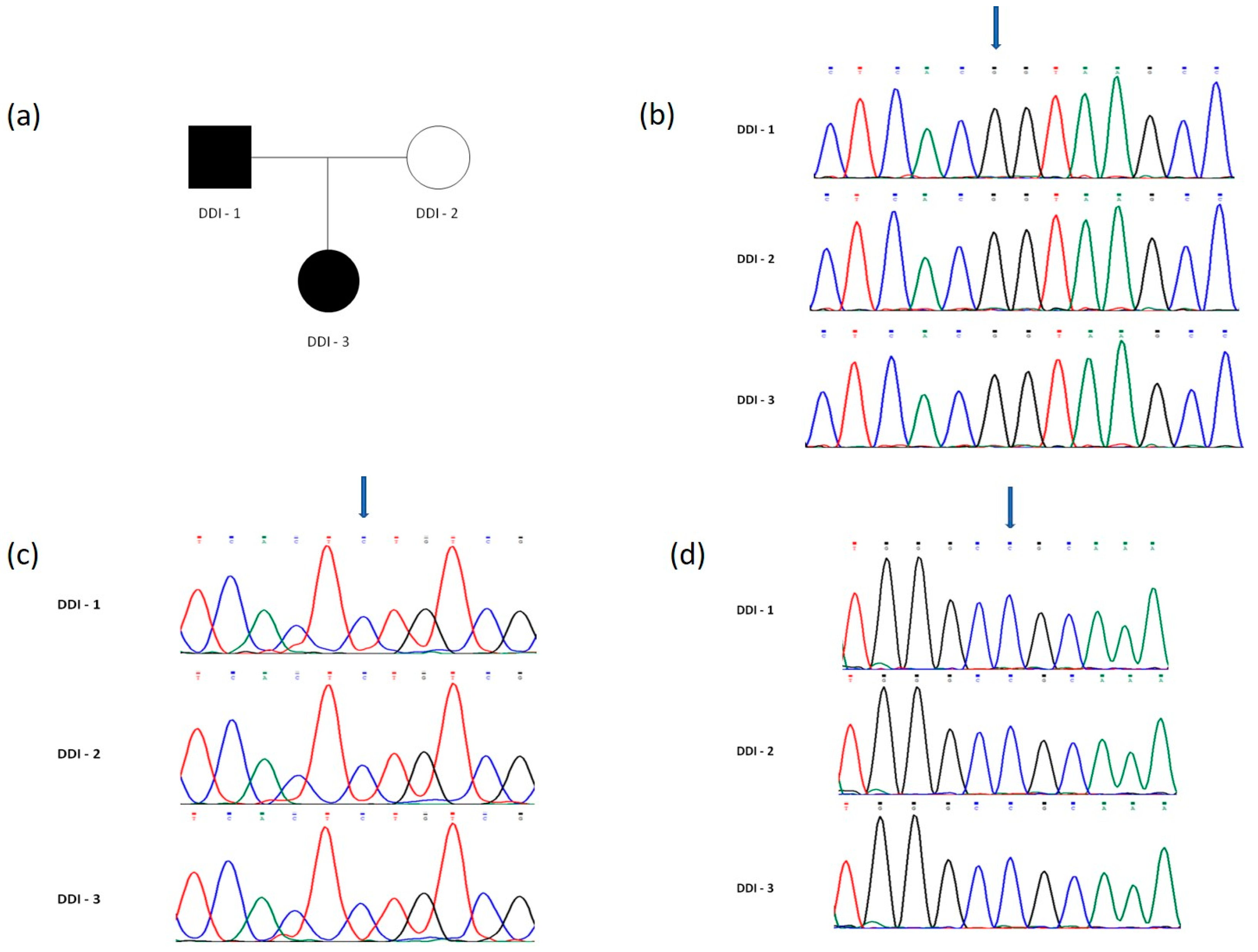
3. Genetic Analysis of the Family
3.1. Saliva Sampling, DNA Isolation, PCR and Sanger Sequencing
3.2. Results of the Genetic Analysis
4. Discussion
4.1. Orthodontic Treatment
4.2. Differential Diagnosis
4.3. Genetic Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, J.W.; Simmer, J.P. Hereditary dentin defects. J. Dent. Res. 2007, 86, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Witkop, C.J., Jr. Hereditary defects of dentin. Dent. Clin. N. Am. 1975, 19, 25–45. [Google Scholar] [PubMed]
- Van Dis, M.L.; Allen, C.M. Dentinal dysplasia type I: A report of four cases. Dentomaxillofac. Radiol. 1989, 18, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.; Würfel, F.; Mundt, T. Dentin dysplasia type I—A case report. Ann. Anat. 1999, 181, 138–140. [Google Scholar] [CrossRef]
- Shanky, P.E.; Mackie, I.C.; Sloan, P. Dentinal dysplasia type I: Report of a case. Int. J. Paediatr. Dent. 1999, 9, 37–42. [Google Scholar] [CrossRef]
- Kalk, W.W.; Batenburg, R.H.; Vissink, A. Dentin dysplasia type I: Five cases within one family. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1998, 86, 175–178. [Google Scholar] [CrossRef]
- Özer, L.; Karasu, H.; Aras, K.; Tokman, B.; Ersoy, E. Dentin dysplasia type I: Report of atypical cases in the permanent and mixed dentitions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2004, 98, 85–90. [Google Scholar] [CrossRef]
- Ye, X.; Li, K.; Liu, L.; Yu, F.; Xiong, F.; Fan, Y.; Xu, X.; Zuo, C.; Chen, D. Dentin dysplasia type I—Novel findings in deciduous and permanent teeth. BMC Oral Health 2015, 15, 163. [Google Scholar] [CrossRef] [Green Version]
- Shields, E.D.; Bixler, D.; el-Kafrawy, A.M. A proposed classification for heritable human dentin defects with a description of a new entity. Arch. Oral Biol. 1973, 18, 543–553. [Google Scholar] [CrossRef]
- Carroll, M.K.O.; Duncan, W.K.; Perkins, T.M. Dentin dysplasia: Review of the literature and a proposed subclassification based on radiographic findings. Oral Surg. Oral Med. Oral Pathol. 1991, 72, 119–125. [Google Scholar] [CrossRef]
- Bloch-Zupan, A.; Jamet, X.; Etard, C.; Laugel, V.; Muller, J.; Geoffroy, V.; Strauss, J.P.; Pelletier, V.; Marion, V.; Poch, O.; et al. Homozygosity mapping and candidate prioritization identify mutations, missed by whole-exome sequencing, in SMOC2, causing major dental developmental defects. Am. J. Hum. Genet. 2011, 89, 773–781. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Chen, D.; Xiong, F.; Chen, D.; Liu, C.; Liu, Y.; Yu, Q.; Xiong, J.; Liu, J.; Li, K.; et al. A splicing mutation in VPS4B causes dentin dysplasia I. J. Med. Genet. 2016, 53, 624–633. [Google Scholar] [CrossRef]
- Xiong, F.; Ji, Z.; Liu, Y.; Zhang, Y.; Hu, L.; Yang, Q.; Qiu, Q.; Zhao, L.; Chen, D.; Tian, Z.; et al. Mutation in SSUH2 causes autosomal-dominant dentin dysplasia type I. Hum. Mutat. 2017, 38, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Li, X.; Lu, F.; Wang, Y.; Xiong, F.; Li, Q. Dentin dysplasia type I—A dental disease with genetic heterogeneity. Oral Dis. 2019, 25, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Rocha, C.T.; Nelson-Filho, P.; Da Silva, L.A.B.; Assed, S.; De Queiroz, A.M. Variation of dentin dysplasia type I: Report of atypical findings in the permanent dentition. Braz. Dent. J. 2011, 22, 74–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Depprich, R.A.; Ommerborn, M.A.; Handschel, J.G.; Naujoks, C.D.; Meyer, U.; Kübler, N.R. Dentin dysplasia type I: A challenge for treatment with dental implants. Head Face Med. 2007, 3, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khandelwal, S.; Gupta, D.; Likhyani, L. A case of dentin dysplasia with full mouth rehabilitation: A 3-year longitudinal study. Int. J. Clin. Pediatr. Dent. 2014, 7, 119–124. [Google Scholar] [PubMed]
- Bespalez-Filho, R.; De Azambuja Berti Couto, S.; Souza, P.H.C.; Westphalen, F.H.; Jacobs, R.; Willems, G.; Tanaka, O.M. Orthodontic treatment of a patient with dentin dysplasia type I. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Ericson, S.; Kurol, J. Incisor root resorptions due to ectopic maxillary canines imaged by computerized tomography: A comparative study in extracted teeth. Angle Orthod. 2000, 70, 276–283. [Google Scholar]
- Ericson, S.; Bjerklin, K.; Falahat, B. Does the canine dental follicle cause resorption of permanent incisor roots? A computed tomographic study of erupting maxillary canines. Angle Orthod. 2002, 72, 95–104. [Google Scholar]
- Milberg, D.J. Labially impacted maxillary canines causing severe root resorption of maxillary central incisors. Angle Orthod. 2006, 76, 173–176. [Google Scholar]
- Alqerban, A.; Jacobs, R.; Lambrechts, P.; Loozen, G.; Willems, G. Root resorption of the maxillary lateral incisor caused by impacted canine: A literature review. Clin. Oral Investig. 2009, 13, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Lai, C.S.; Bornstein, M.M.; Mock, L.; Heuberger, B.M.; Dietrich, T.; Katsaros, C. Impacted maxillary canines and root resorptions of neighboring teeth: A radiographic analysis using cone-beam computed tomography. Eur. J. Orthod. 2013, 35, 529–538. [Google Scholar] [CrossRef] [Green Version]
- Walker, S. Root resorption during orthodontic treatment. Evid.-Based Dent. 2010, 11, 88. [Google Scholar] [CrossRef]
- Weltman, B.; Vig, K.W.; Fields, H.W.; Shanker, S.; Kaizar, E.E. Root resorption associated with orthodontic tooth movement: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 462–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, J.; Chen, J.; Weinkamer, R.; Darendeliler, M.A.; Swain, M.V.; Sue, A.; Zheng, K.; Li, Q. In vivo effects of different orthodontic loading on root resorption and correlation with mechanobiological stimulus in periodontal ligament. J. R. Soc. Interface 2019, 16, 20190108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, P.S.; Hart, T.C. Disorders of human dentin. Cells Tissues Organs 2007, 186, 70–77. [Google Scholar] [CrossRef] [Green Version]
- de La Dure-Molla, M.; Philippe Fournier, B.; Berdal, A. Isolated dentinogenesis imperfecta and dentin dysplasia: A revision of the classification. Eur. J. Hum. Genet. 2015, 23, 445–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Chen, L.; Liu, J.; Zhao, Z.; Qu, E.; Wang, X.; Chang, W.; Xu, C.; Wang, Q.K.; Liu, M. A novel DSPP mutation is associated with type II dentinogenesis Imperfecta in a chinese family. BMC Med. Genet. 2007, 8, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.-K.; Lee, K.-E.; Jeon, D.; Lee, G.; Lee, H.; Shin, C.-U.; Jung, Y.-J.; Lee, S.-H.; Hahn, S.-H.; Kim, J.-W. A novel mutation in the DSPP gene associated with dentinogenesis imperfecta Type II. J. Dent. Res. 2009, 88, 51–55. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, J.; Ma, Y.; Du, W.; Zhao, S.; Zhang, Z.; Zhang, X.; Liu, Y.; Xiao, H.; Wang, H.; et al. A novel splicing mutation alters DSPP transcription and leads to dentinogenesis imperfecta Type II. PLoS ONE 2011, 6, e27982. [Google Scholar] [CrossRef]
- Auguściak-Duma, A.; Witecka, J.; Sieroń, A.L.; Janeczko, M.; Pietrzyk, J.J.; Ochman, K.; Galicka, A.; Borszewska-Kornacka, M.K.; Pilch, J.; Jakubowska-Pietkiewicz, E. Mutations in the COL1A1 and COL1A2 genes associated with osteogenesis imperfecta (OI) types I or III. Acta Biochim. Pol. 2018, 65, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.-K.; Seymen, F.; Kang, H.-Y.; Lee, K.-E.; Gencay, K.; Tuna, B.; Kim, J.-W. MMP20 hemopexin domain mutation in amelogenesis imperfecta. J. Dent. Res. 2010, 89, 46–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nalbant, D.; Youn, H.; Nalbant, S.I.; Sharma, S.; Cobos, E.; Beale, E.G.; Du, Y.; Williams, S.C. FAM20: An evolutionarily conserved family of secreted proteins expressedin hematopoietic cells. BMC Genom. 2005, 6, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Wang, W.; Qin, M.; Zhao, Y. Novel FAM83H mutations in patients with amelogenesis imperfecta. Sci. Rep. 2017, 7, 6075. [Google Scholar] [CrossRef]













Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papagiannis, A.; Fanourakis, G.; Mitsea, A.; Karayianni, K.; Vastardis, H.; Sifakakis, I. Orthodontic Treatment of a Patient with Dentin Dysplasia Type I and Bilateral Maxillary Canine Impaction: Case Presentation and a Family-Based Genetic Analysis. Children 2021, 8, 519. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060519
Papagiannis A, Fanourakis G, Mitsea A, Karayianni K, Vastardis H, Sifakakis I. Orthodontic Treatment of a Patient with Dentin Dysplasia Type I and Bilateral Maxillary Canine Impaction: Case Presentation and a Family-Based Genetic Analysis. Children. 2021; 8(6):519. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060519
Chicago/Turabian StylePapagiannis, Alexandros, Galinos Fanourakis, Anastasia Mitsea, Kety Karayianni, Heleni Vastardis, and Iosif Sifakakis. 2021. "Orthodontic Treatment of a Patient with Dentin Dysplasia Type I and Bilateral Maxillary Canine Impaction: Case Presentation and a Family-Based Genetic Analysis" Children 8, no. 6: 519. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060519