
The BabySaver: Design of a New Device for Neonatal Resuscitation at Birth with Intact Placental Circulation

 ,
, 
Abstract
:1. Introduction
The Rationale for the BabySaver Newborn Resuscitation Device
- prevents separation of the skilled birth attendant and mother, so that the care of the mother is not interrupted
- allows the mother to remain with the baby during its initial support, instead of removing it from her sight during these vital moments
- facilitates newborn resuscitation when only one skilled birth attendant is present.
2. Materials and Methods
2.1. Team
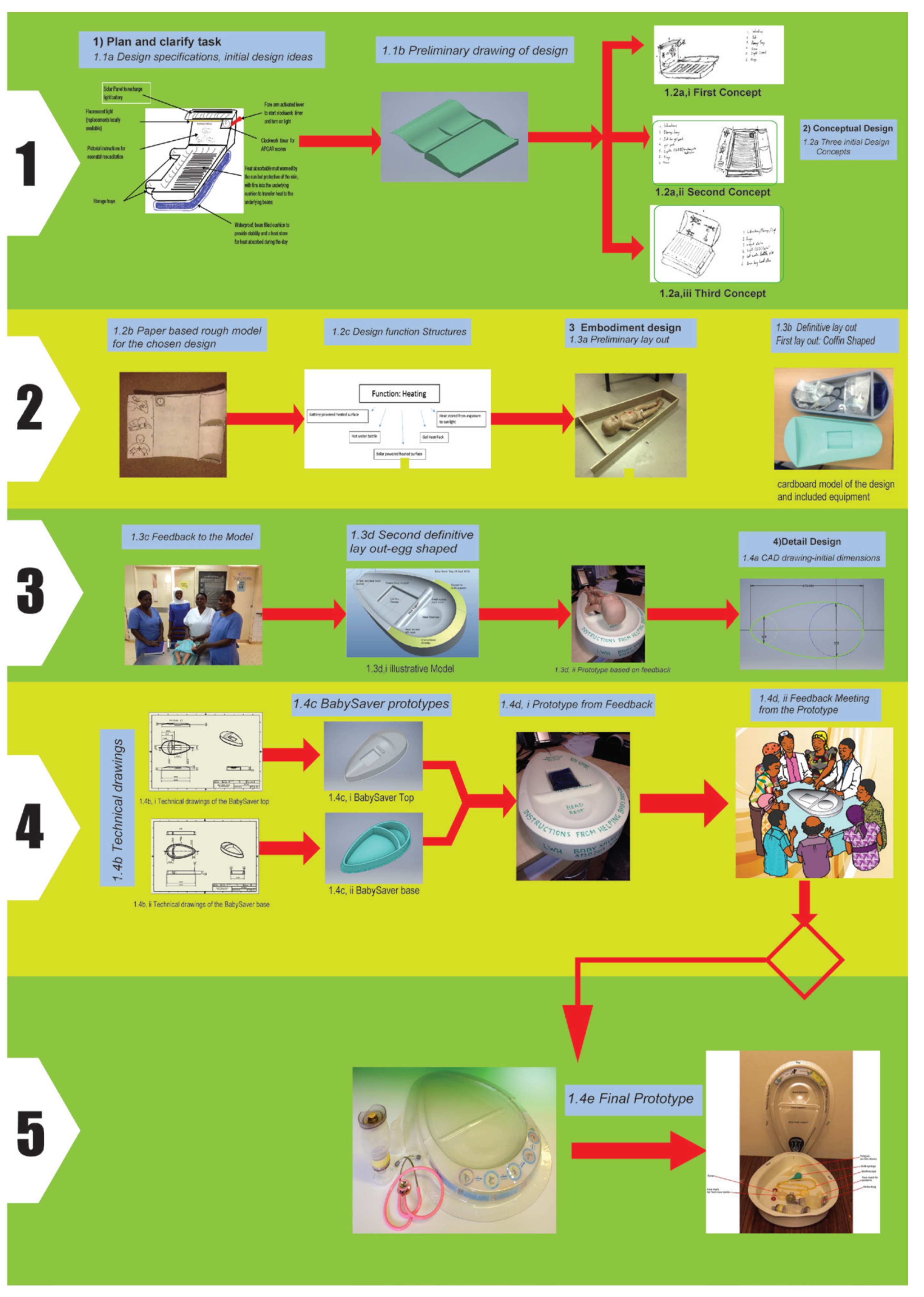
2.2. Design Process
2.3. Plan and Clarify the Task
2.3.1. Design Team Formation
2.3.2. Other Stakeholders
2.3.3. Problem Identification and Design Specification
2.4. Conceptual Design
2.4.1. Initial Design Concepts
Choice of a Design Concept
Heat Gel Pack
Methods for Design Production
Design Materials and Choices
2.4.2. Paper-Based Rough Design Model
2.4.3. Design Function Structures
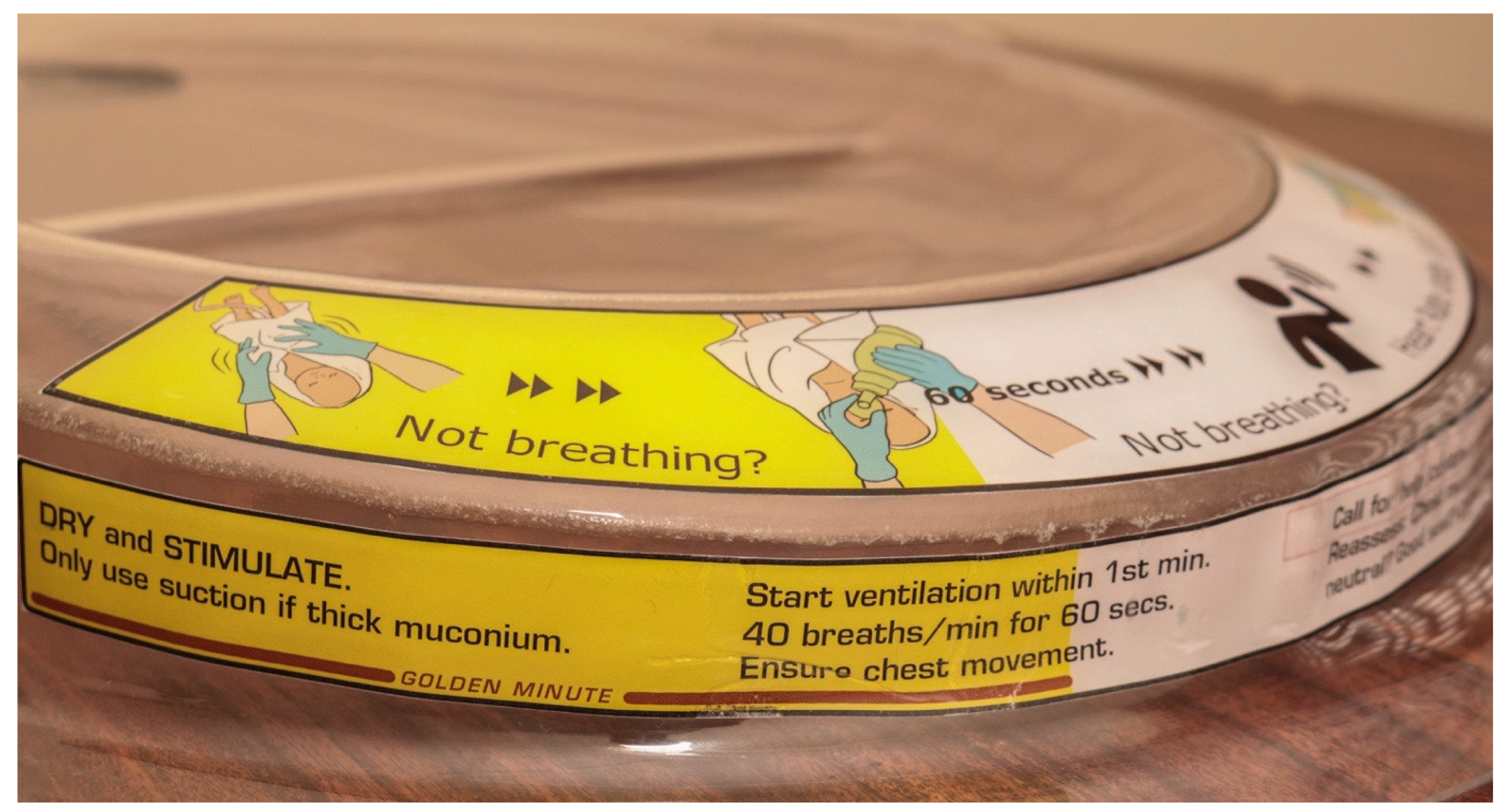
Choice of Helping Babies Breathe (HBB) Instructions
2.5. Embodiment Design
2.5.1. Preliminary Layout
Feedback Mbale Midwives
- (i)
- The rough model was not long enough for the baby and changes to the dimensions were proposed.
- (ii)
- The design required neck support as an add-in, to promote a natural neutral position during resuscitation.
- (iii)
- There were concerns that the timer could not sustain the bleaching effects of Sodium hypochlorite (Jik) solution following prolonged and frequent cleaning.
- (iv)
- They agreed with the need to include the storage tray for the pieces of equipment for resuscitation.
- (v)
- They proposed to add a valley on the top surface of the design as a slot for the gel pack. This would allow easier inserting and cleaning of the gel pack.
- (vi)
- Incorporating a light source in the tray would be incompatible with several specifications, especially “low cost and easy to sterilise using local methods”.
- (vii)
- Light and timer were henceforth decided to be removed from the list and made as separate components to store in the design when needed.
Commonwealth and FIGO Fellows
Positions of the Device at the Time of Resuscitation
Assembly of the Preliminary Layout
Cardboard Drawings
2.5.2. First Version of Definitive Layout
Feedback on the First Version of Definitive Layout
Feedback on the Contents of the BabySaver Design
2.5.3. Second Version of Definitive Layout
Feedback on the Second Version of Definitive Layout
2.6. Detailed Design
2.6.1. CAD Drawings
2.6.2. Technical Drawings
2.6.3. Prototype Initial Shape
2.6.4. Feedback from Users in Uganda
3. Results
3.1. Device Class
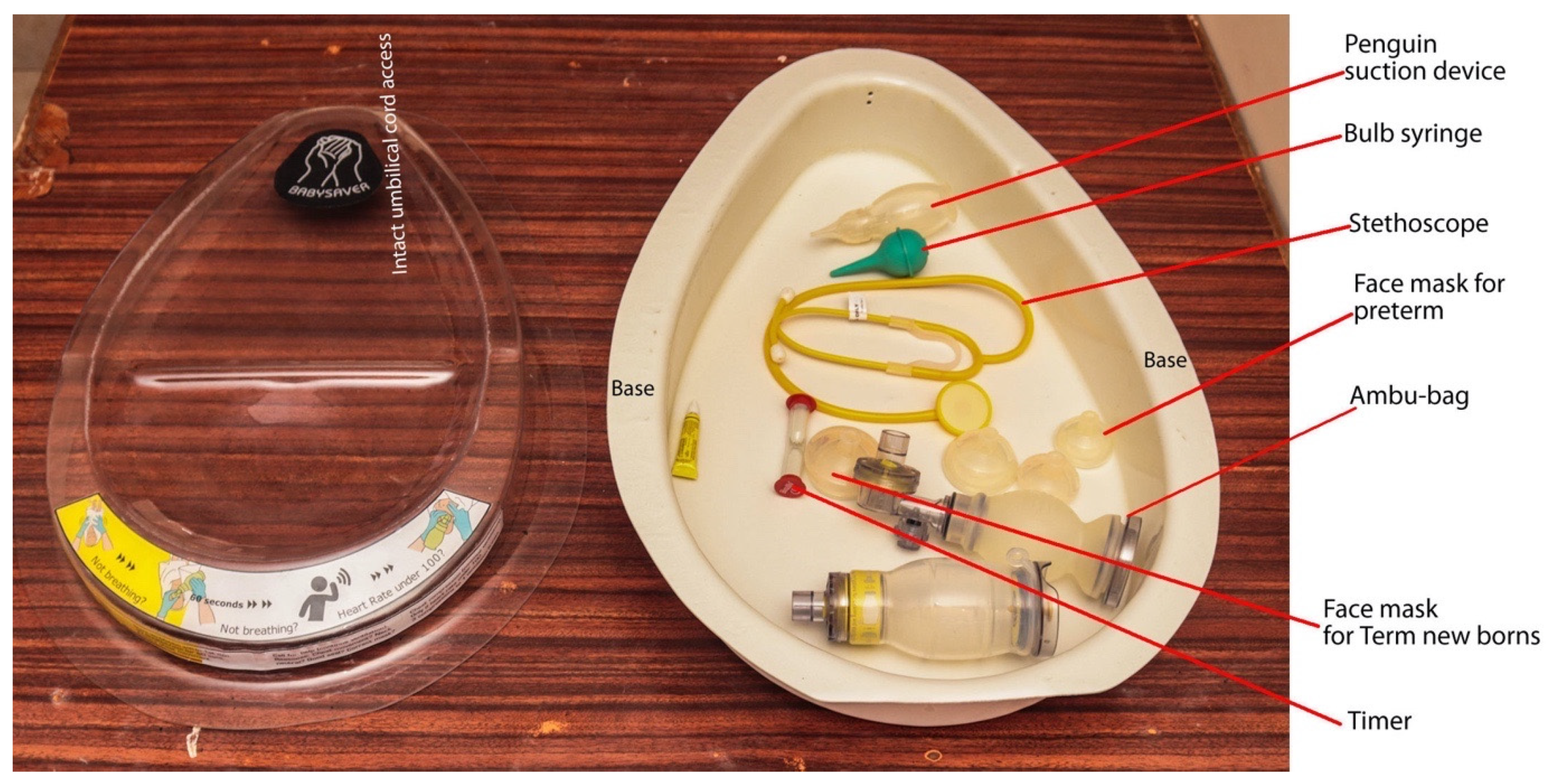
3.2. Device Description
3.2.1. The Tray
3.2.2. The Base
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ariff, S.; Lee, A.C.; Lawn, J.; Bhutta, Z.A. Global Burden, Epidemiologic Trends, and Prevention of Intrapartum-Related Deaths in Low-Resource Settings. Clin. Perinatol. 2016, 43, 593–608. [Google Scholar] [CrossRef]
- Hug, L.; Alexander, M.; You, D.; Alkema, L. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: A systematic analysis. Lancet Glob. Health 2019, 7, e710–e720. [Google Scholar] [CrossRef] [Green Version]
- United Nations Inter-Agency Group for Child Mortality Estimation (UNICEF, WHO, United Nations Population Division and the World Bank). Levels & Trends in Childhood Mortality: Report 2020. 2020. Available online: https://data.unicef.org/resources/levels-and-trends-in-child-mortality/last (accessed on 18 June 2021).
- Wall, S.N.; Lee, A.C.; Carlo, W.; Goldenberg, R.; Niermeyer, S.; Darmstadt, G.L.; Keenan, W.; Bhutta, Z.A.; Perlman, J.; Lawn, J. Reducing Intrapartum-Related Neonatal Deaths in Low- and Middle-Income Countries—What Works? Semin. Perinatol. 2010, 34, 395–407. [Google Scholar] [CrossRef]
- Sendeku, F.W.; Azeze, G.G.; Fenta, S.L. Perinatal asphyxia and its associated factors in Ethiopia: A systematic review and meta-analysis. BMC Pediatr. 2020, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gebreheat, G.; Tsegay, T.; Kiros, D.; Teame, H.; Etsay, N.; Welu, G.; Abraha, D. Prevalence and Associated Factors of Perinatal Asphyxia among Neonates in General Hospitals of Tigray, Ethiopia, 2018. BioMed Res. Int. 2018, 2018, 1–7. [Google Scholar] [CrossRef]
- Emechebe, G.; Ezeogu, J.; Odinaka, K.K. Birth Asphyxia in Nigeria: A Review. Trop. J. Med. Health Sci. Res. 2016, 5, 1. [Google Scholar]
- Wall, S.N.; Lee, A.C.C.; Niermeyer, S.; English, M.; Keenan, W.J.; Carlo, W.; Bhutta, Z.A.; Bang, A.; Narayanan, I.; Ariawan, I.; et al. Neonatal resuscitation in low-resource settings: What, who, and how to overcome challenges to scale up? Int. J. Gynecol. Obstet. 2009, 107, S47–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchon, D.; Bettles, N. Motherside care of the term neonate at birth. Matern. Health Neonatol. Perinatol. 2016, 2, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchon, D.; Pratesi, S.; Katheria, A. How to Provide Motherside Neonatal Resuscitation with Intact Placental Circulation? Child 2021, 8, 291. [Google Scholar] [CrossRef]
- Katheria, A.C.; Brown, M.K.; Rich, W.; Arnell, K. Providing a Placental Transfusion in Newborns Who Need Resuscitation. Front. Pediatr. 2017, 5, 1–8. [Google Scholar]
- Hutchon, D. Evolution of neonatal resuscitation with intact placental circulation. Infant 2014, 10, 58–61. [Google Scholar]
- Hutchon, D.J.R. Early versus delayed cord clamping at birth: In sickness and in health. Fetal Matern. Med. Rev. 2013, 24, 185–193. [Google Scholar] [CrossRef]
- Thomas, M.R.; Yoxall, C.W.; Weeks, A.D.; Duley, L. Providing newborn resuscitation at the mother’s bedside: Assessing the safety, usability and acceptability of a mobile trolley. BMC Pediatr. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Weeks, A.; Watt, P.; Yoxall, C.W.; Gallagher, A.; Burleigh, A.; Bewley, S.; Heuchan, A.M.; Duley, L. Innovation in immediate neonatal care: Development of the Bedside Assessment, Stabilisation and Initial Cardiorespiratory Support (BASICS) trolley. BMJ Innov. 2015, 1, 53–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwer, E.; Knol, R.; Vernooij, A.S.N.; Akker, T.V.D.; Vlasman, P.E.; Klumper, F.J.C.M.; Dekoninck, P.; Polglase, G.R.; Hooper, S.B.; Pas, A.B.T. Physiological-based cord clamping in preterm infants using a new purpose-built resuscitation table: A feasibility study. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 104, F396–F402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knol, R.; Brouwer, E.; Vernooij, A.S.N.; Klumper, F.J.C.M.; Dekoninck, P.; Hooper, S.B.; Pas, A.B.T. Clinical aspects of incorporating cord clamping into stabilisation of preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F493–F497. [Google Scholar] [CrossRef]
- Knol, R.; Brouwer, E.; Akker, T.V.D.; DeKoninck, P.; van Geloven, N.; Polglase, G.R.; Lopriore, E.; Herkert, E.; Reiss, I.K.; Hooper, S.B.; et al. Physiological-based cord clamping in very preterm infants Randomised controlled trial on effectiveness of stabilisation. Resuscitation 2020, 147, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Knol, R.; Brouwer, E.; Klumper, F.J.C.M.; Akker, T.V.D.; Dekoninck, P.; Hutten, G.J.; Lopriore, E.; Van Kaam, A.H.; Polglase, G.R.; Reiss, I.K.M.; et al. Effectiveness of Stabilization of Preterm Infants with Intact Umbilical Cord Using a Purpose-Built Resuscitation Table—Study Protocol for a Randomized Controlled Trial. Front. Pediatr. 2019, 7, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katheria, A.; Lee, H.C.; Knol, R.; Irvine, L.; Thomas, S. A review of different resuscitation platforms during delayed cord clamping. J. Perinatol. 2021, 13, 1–9. [Google Scholar]
- Niermeyer, S.; Robertson, N.J.; Ersdal, H.L. Beyond basic resuscitation: What are the next steps to improve the outcomes of resuscitation at birth when resources are limited? Semin. Fetal Neonatal Med. 2018, 23, 361–368. [Google Scholar] [CrossRef]
- Pahl, G.; Beitz, W.; Feldhusen, J.; Grote, K.-H. Engineering Design: A Systematic Approach, 3rd ed.; Springer: London, UK, 2007. [Google Scholar]
- Fogarty, M.; Osborn, D.A.; Askie, L.; Seidler, A.L.; Hunter, K.; Lui, K.; Simes, J.; Tarnow-Mordi, W. Delayed vs. early umbilical cord clamping for preterm infants: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2018, 218, 1–18. [Google Scholar] [CrossRef]
- Rabe, H.; Gyte, G.M.; Díaz-Rossello, J.L.; Duley, L. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst. Rev. 2019, 9, CD003248. [Google Scholar] [CrossRef]
- Rabe, H.; Reynolds, G.J.; Diaz-Rosello, J.L. Early versus delayed umbilical cord clamping in preterm infants. Cochrane Database Syst. Rev. 2004, 77, CD003248. [Google Scholar] [CrossRef]
- Matar, H.E.; Almerie, M.Q.; Alsabbagh, M.; Jawoosh, M.; Almerie, Y.; Abdulsalam, A.; Duley, L. Policies for care during the third stage of labour: A survey of maternity units in Syria. BMC Pregnancy Childbirth 2010, 10, 32. [Google Scholar] [CrossRef] [Green Version]
- Madar, J.; Roehr, C.C.; Ainsworth, S.; Ersdal, H.; Morley, C.; Rüdiger, M.; Skåre, C.; Szczapa, T.; Pas, A.T.; Trevisanuto, D.; et al. European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation 2021, 161, 291–326. [Google Scholar] [CrossRef]
- World Health Organisation. Guideline: Delayed Umbilical Cord Clamping for Improved Maternal and Infant Health and Nutrition Outcomes; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Ministry of Health. Uganda Clinical Guidelines 2016: National Guidelines for Management of Common Conditions, Revised; Ministry of Health Uganda: Kampala, Uganda, 2016.
- Mitchell, E.J.; Benjamin, S.; Ononge, S.; Ditai, J.; Qureshi, Z.; Masood, S.N.; Whitham, D.; Godolphin, P.J.; Duley, L. Identifying women giving birth preterm and care at the time of birth: A prospective audit of births at six hospitals in India, Kenya, Pakistan and Uganda. BMC Pregnancy Childbirth 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Niermeyer, S. From the Neonatal Resuscitation Program to Helping Babies Breathe: Global impact of educational programs in neonatal resuscitation. Semin. Fetal Neonatal Med. 2015, 20, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Ogrodnik, P.J. Class 1 Devices: Case Studies in Medical Devices Design; Elsevier: London, UK, 2015. [Google Scholar]
- Soth, M.; Piraino, T. Noninvasive Mechanical Ventilation: Theory, Equipment, and Clinical Applications, Second; Springer International Publishing: New York, NY, USA, 2016. [Google Scholar]
- Madar, J. Clinical risk management in newborn and neonatal resuscitation. Semin. Fetal Neonatal Med. 2005, 10, 45–61. [Google Scholar] [CrossRef]
- Uganda National Council for Science and Technology (UNCST). National Guidelines for Conduct of Research during Corona Virus Disease 2019 (COVID-19) Pandemic, July; Uganda National Council for Science and Technology: Kampala, Uganda, 2020.
- Bang, A.; Bellad, R.; Gisore, P.; Hibberd, P.; Patel, A.; Goudar, S.; Esamai, F.; Goco, N.; Meleth, S.; Derman, R.J.; et al. Implementation and evaluation of the Helping Babies Breathe curriculum in three resource limited settings: Does Helping Babies Breathe save lives? A study protocol. BMC Pregnancy Childbirth 2014, 14, 116. [Google Scholar] [CrossRef] [Green Version]
- Kamath-Rayne, B.D.; Thukral, A.; Visick, M.K.; Schoen, E.; Amick, E.; Deorari, A.; Cain, C.J.; Keenan, W.J.; Singhal, N.; Little, G.A.; et al. Helping Babies Breathe, Second Edition: A Model for Strengthening Educational Programs to Increase Global Newborn Survival. Glob. Health Sci. Pract. 2018, 6, 538–551. [Google Scholar] [CrossRef] [Green Version]
- Singhal, N.; Lockyer, J.; Fidler, H.; Keenan, W.; Little, G.; Bucher, S.; Qadir, M.; Niermeyer, S. Helping Babies Breathe: Global neonatal resuscitation program development and formative educational evaluation. Resuscitation 2012, 83, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Mann, C.; Chilcott, S.; Plumb, K.; Brooks, E.; Man, M.-S. Reporting and appraising the context, process and impact of PPI on contributors, researchers and the trial during a randomised controlled trial—the 3D study. Res. Involv. Engag. 2018, 4, 1–12. [Google Scholar] [CrossRef] [PubMed]
- INVOLVE. Public Involvement in Clinical Trials: Supplement to the Briefing Notes for Researchers; Eastleigh: Hampshire, UK, 2012. [Google Scholar]
- Martin, J.L.; Murphy, E.; Crowe, J.; Norris, B.J. Capturing user requirements in medical device development: The role of ergonomics. Physiol. Meas. 2006, 27, R49–R62. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S/No | Resuscitation Procedure in Delivery Rooms | Problems with the Current Method of Resuscitation at Birth | Mechanism of Action | Outcome |
|---|---|---|---|---|
| 1 | The baby is delivered by attending skilled birth attendant or student in the labour suite or operating theatre | |||
| 2 | The baby’s cord is clamped, or tied immediately and cut by the skilled birth attendant or student | Lack of a system to perform delayed cord clamping | Leads to decreased blood volume, haemoglobin and iron stores | An effect on baby’s neurological development |
| 3 | The baby is dried and kept warm by the attending skilled birth attendant or student | Transfer of baby to a separate resuscitation station | Maternal-baby separation leading to fear of babies being swapped | Maternal distress |
| 4 | The baby is transferred to a resuscitaire/resuscitation station if it does not cry | Resuscitaire is not functional or broken | Resuscitation may be performed inadequately on available surfaces | Unnecessary death |
| 5 | The baby’s airways are checked for any secretions and cleared if needed by wiping with a cloth or suctioning | Lack of constant electricity in delivery rooms | Absence of a heating option for the baby on the resuscitaire | Risk of hypothermia during resuscitation on the resuscitaire |
| 6 | The baby’s back is rubbed 2−3 times, or feet slapped to stimulate breathing | Inconsistent or unavailable in-service training programme on helping babies breathe | Midwives not up to date with resuscitation guidelines or steps | Inability to follow guidelines for resuscitation |
| 7 | The baby is positioned in neutral position and ventilation initiated with bag and mask | Missing equipment for resuscitation | Inability to perform all the necessary steps of resuscitation | Unsuccessful resuscitation |
| 8 | If available, a mixture of oxygen and air is recommended for premature babies | Equipment is not in one place at time of resuscitation | Delays to initiate suctioning, bag and mask ventilation | Wasting of golden minute |
| 9 | If required after bag and mask ventilation, chest compressions are performed on the baby by a midwife | |||
| 10 | If these are unsuccessful and drugs are available, drugs are administered by attending skilled birth attendant | |||
| 11 | If resuscitation is successful, the baby is transferred to the neonatal unit | |||
| 12 | The equipment used in the birth is taken for cleaning by the attending midwife | The equipment is cleaned in the same buckets as those for delivery | ||
| 13 | The resuscitation equipment is maintained by the local engineering department |
| S/No. | Requirement | Comments | Rank |
|---|---|---|---|
| 1 | The design must warm the baby to prevent hypothermia. | The heating should not harm the baby | 1 |
| 2 | The design must work with resuscitation protocols in place. | The systems may vary from hospital to hospital, but the tray should fit into standard practice in Mulago and Mbale hospitals | 2 |
| 3 | The design must be made of non-slip, cleanable materials. | The materials used must be able to be sterilised using current local cleaning practices | 2 |
| 4 | The design must provide pictorial instructions on how to deliver neonatal resuscitation. | This must agree with up-to-date standards of practice | 3 |
| 5 | The design must have storage capabilities for auxiliary equipment. | 4 | |
| 6 | The design must be able to be moved safely. | This includes when in use | 5 |
| 7 | The design should be cheap to manufacture | Aim for manufacture price under $10 | 6 |
| 8 | The design should have a light. | This should be independent from hospital utilities | 7 |
| 9 | The design should have a timer. | 8 | |
| 10 | The design should be theft proof. | If possible, the design should discourage theft, or theft of parts. | 9 |
| 11 | The design should be able to be used on a variety of surfaces. |
| Equipment and Supplies for the Care of Every Newborn at Birth in the BabySaver | ||
|---|---|---|
| Essential equipment | Optional equipment | Optional Supplies |
| Suction device | NeoBeat newborn heart rate monitor | Surgical gloves |
| Neonatal Ambu Bag | Laryngoscope | Cord ties |
| Neonatal face mask size 1 | Timer | |
| Neonatal face mask size 0 | Tetracycline eye ointment | |
| Neonatal stethoscope | Vitamin K | |
| Intravenous fluids | ||
| Adrenaline | ||
| Oxytocin | ||
| Key Process | Potential Failure Mode (FM) | Potential Failure Effects | SEV | Potential Causes | OCC | Current Controls | DET | RPN | Recommendations | Responsible Person |
|---|---|---|---|---|---|---|---|---|---|---|
| What is the process step or input? | In what ways can the process step or input fail? | What is the impact on the key output variables once it fails (customer or internal requirements)? | How severe is the effect on the customer? | What causes the key input to go wrong? | How often does cause or FM OCC occur? | What are the existing controls and procedures that prevent either the cause or the failure mode? | How well can you detect the cause or the failure mode? | What are the actions for reducing the occurrence of the cause, or improving detection? | Who is responsible for the recommended action? | |
| Organise resuscitation equipment in the BabySaver | The bag and mask are non-functional | The baby receives inadequate ventilation | 1 | Defects in the pieces of equipment and limited user ability to detect early | 1 | All resuscitation equipment included in BabySaver should be checked before handing over to the hospital staff | 1 | 4 | User training | supplier/SAfRI/Laerdal Global |
| BabySaver is brought close to the delivery bed | BabySaver falls | Midwife is injured | 2 | BabySaver held with slippery hands and in a rush | 2 | There is usually a delivery trolley in the labour suite, on which the BabySaver can be placed and moved | 1 | 4 | The users are trained on handling the BabySaver unit in a real clinical setting | Skilled birth attendant |
| Explain BabySaver to the mother and attendant | Mother scared of the device | Mother refuses the BabySaver use | 2 | Deliveries occurring before the explanation. Many deliveries under 1 midwife | 2 | All women are admitted to labour at a central station | 1 | 4 | Explanation of the device at any opportunity a midwife is in contact with the mother in labour during admission, examinations, etc. | Skilled birth attendant |
| Place the tray in between mother’s legs | Tray slips | Mother and Baby are injured | 2 | A tray placed on an incompatible surface, no space in between legs. The tray is positioned wrongly with the broad end closet to the buttocks instead | 2 | Some delivery beds are long enough in the labour suite. For the surface material of the delivery beds, tests need to be performed to see how feasible this is. | 1 | 4 | User training on the positioning of the BabySaver, feasibility testing | Skilled birth attendant |
| Activates gel pack | The heat gel pack is not present | Baby’s temperature drops | 1 | Equipment not replaced after use | 3 | The tray will have a checklist of equipment that should be included | 1 | 3 | Equipment included will be detailed in the instructions | Manufacturer |
| Heat pack ruptures | Baby is injured | 2 | Heat pack has weak point due to incorrect care or manufacturing flaw | 1 | Pack contents non-toxic, pack contents not hot enough to injure | 1 | 2 | Instructions on pack care (not having the plastic on a hot surface, wrapping with a cloth while boiling, etc.) included | Manufacturer | |
| Heat pack overheats | Baby is injured | 3 | The pack is placed directly on neonate skin instead of through cloth | 1 | The heat gel pack has been tested to ensure it does not reach harmful heat levels | 1 | 3 | Instructions to regularly check the infant for erythema included | Manufacturer | |
| Heat pack underheats | Baby’s temperature drops | 1 | Manufacturing error | 1 | Spare heat pack provided | 2 | 2 | Batch testing required | Manufacturer | |
| Gently place the baby onto the tray | The baby is placed incorrectly | Resuscitation is incorrectly performed | 1 | Insufficient training | 3 | Neck support and pictorial instructions included | 1 | 3 | User training | Supplier/SAfRI/manufacturer |
| Position the baby in a neutral position | The baby is positioned incorrectly | Resuscitation is incorrectly performed | 1 | The neck support is too elevated, or the neck support groove is too shallow | 3 | Minimum elevation of the neck support included | 1 | 3 | User training | Manufacturer |
| Keep the baby warm | The baby loses heat on the tray | Baby develops hypothermia | 1 | The baby is not covered in enough clothes, cotton dry clothes. Wet clothes not changed | 3 | The baby is dried and changed into a second warm cotton cloth before starting resuscitation | 1 | 3 | User training | Skilled birth attendant |
| Resuscitation is performed | Instructions are unclear | Resuscitation is incorrectly performed | 3 | Insufficient user training | 1 | Instructions are standard internationally agreed guidelines, checked with experienced practitioners for content. | 2 | 6 | User training, instructions also checked with inexperienced users for clarity | Supplier |
| Tray fails mechanically | Mother and baby are injured | 2 | Too much force on the tray; sharp edges can cause discomfort | 1 | Durable material that does not degrade, smooth surface edges | 2 | 4 | Product lifecycle and surfaces of the edges advised in instructions | Manufacturer | |
| Mother kicks the tray during use | Midwife is injured | 2 | Maternal distress | 1 | Instructions for the user | 2 | 4 | User training and explaining to the mother early about the use of the BabySaver | Skilled birth attendant | |
| Withdraw the tray from between mother’s legs | The tray slips or is transferred to the ground | Midwife and mother injured | 1 | user oversight and fatigue, slippery gloves soiled in liquor and blood | 3 | The tray has a flat flap for firm handling | 1 | 3 | The users must be trained on proper handling of the tray with both hands where possible | Users/skilled birth attendants |
| Withdraw the equipment from the delivery field | Equipment is not replaced | Resuscitation is incorrectly performed | 1 | Replacement is not available, user oversight, pieces of equipment for resuscitation remain in mother’s clothes | 3 | The tray has a checklist of equipment that should be included | 1 | 3 | Equipment included will be detailed on the instructions, as well as care instructions for the auxiliary components | Manufacturer |
| Reprocess the BabySaver and equipment | BabySaver is not disinfected fully | Baby contracts infection | 2 | Cleaning protocol not followed | 3 | The product has no crevasses; is compatible with local cleaning products | 2 | 12 | User training | Supplier |
| BabySaver is not disinfected immediately | Baby contracts infection | 2 | Cleaning protocol not followed | 3 | The product has no crevasses; is compatible with local cleaning products | 2 | 12 | User training | Supplier | |
| Baby’s pieces of equipment for resuscitation are mixed with maternal delivery pieces of equipment | Baby contracts infection | 2 | Cleaning protocol not followed | 3 | The product has no crevasses; is compatible with local cleaning products | 2 | 12 | User training | Supplier | |
| The tray is returned to storage | Equipment is not replaced | Resuscitation is incorrectly performed | 1 | Replacement s not available, user oversight | 3 | The tray has a checklist of equipment that should be included | 1 | 3 | Equipment included will be detailed on the instructions, as well as care instructions for the auxiliary components | Manufacturer |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ditai, J.; Barry, A.; Burgoine, K.; Mbonye, A.K.; Wandabwa, J.N.; Watt, P.; Weeks, A.D. The BabySaver: Design of a New Device for Neonatal Resuscitation at Birth with Intact Placental Circulation. Children 2021, 8, 526. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060526
Ditai J, Barry A, Burgoine K, Mbonye AK, Wandabwa JN, Watt P, Weeks AD. The BabySaver: Design of a New Device for Neonatal Resuscitation at Birth with Intact Placental Circulation. Children. 2021; 8(6):526. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060526
Chicago/Turabian StyleDitai, James, Aisling Barry, Kathy Burgoine, Anthony K. Mbonye, Julius N. Wandabwa, Peter Watt, and Andrew D. Weeks. 2021. "The BabySaver: Design of a New Device for Neonatal Resuscitation at Birth with Intact Placental Circulation" Children 8, no. 6: 526. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060526