
Under-Vaccination in Pediatric Liver Transplant Candidates with Acute and Chronic Liver Disease—A Retrospective Observational Study of the European Reference Network TransplantChild

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Acquisition
2.2. Statistical Analysis
2.3. Immunization Recommendations
2.3.1. Diphtheria, Tetanus, Pertussis, Poliomyelitis and Haemophilus Influenzae Type B
2.3.2. Hepatitis B
2.3.3. Pneumococcal Conjugate Vaccine
2.3.4. Pneumococcal Polysaccharide Vaccine
2.3.5. Rotavirus Vaccine
2.3.6. Meningococcal Vaccine Serogroup C (MenC)
2.3.7. Meningococcal Vaccine Serogroup B (MenB)
2.3.8. Meningococcal Vaccine Serogroup ACWY (MenACWY)
2.3.9. Measles, Mumps, and Rubella (MMR)
2.3.10. Varicella/Chickenpox Vaccine (VZV)
2.3.11. Human Papillomavirus (HPV) Vaccines
3. Results
3.1. Study Population
3.2. Analysis of Age-Appropriate Vaccination Coverage
3.3. Country-Specific Vaccination Coverage between Healthy Children and Those with Chronic Liver Disease
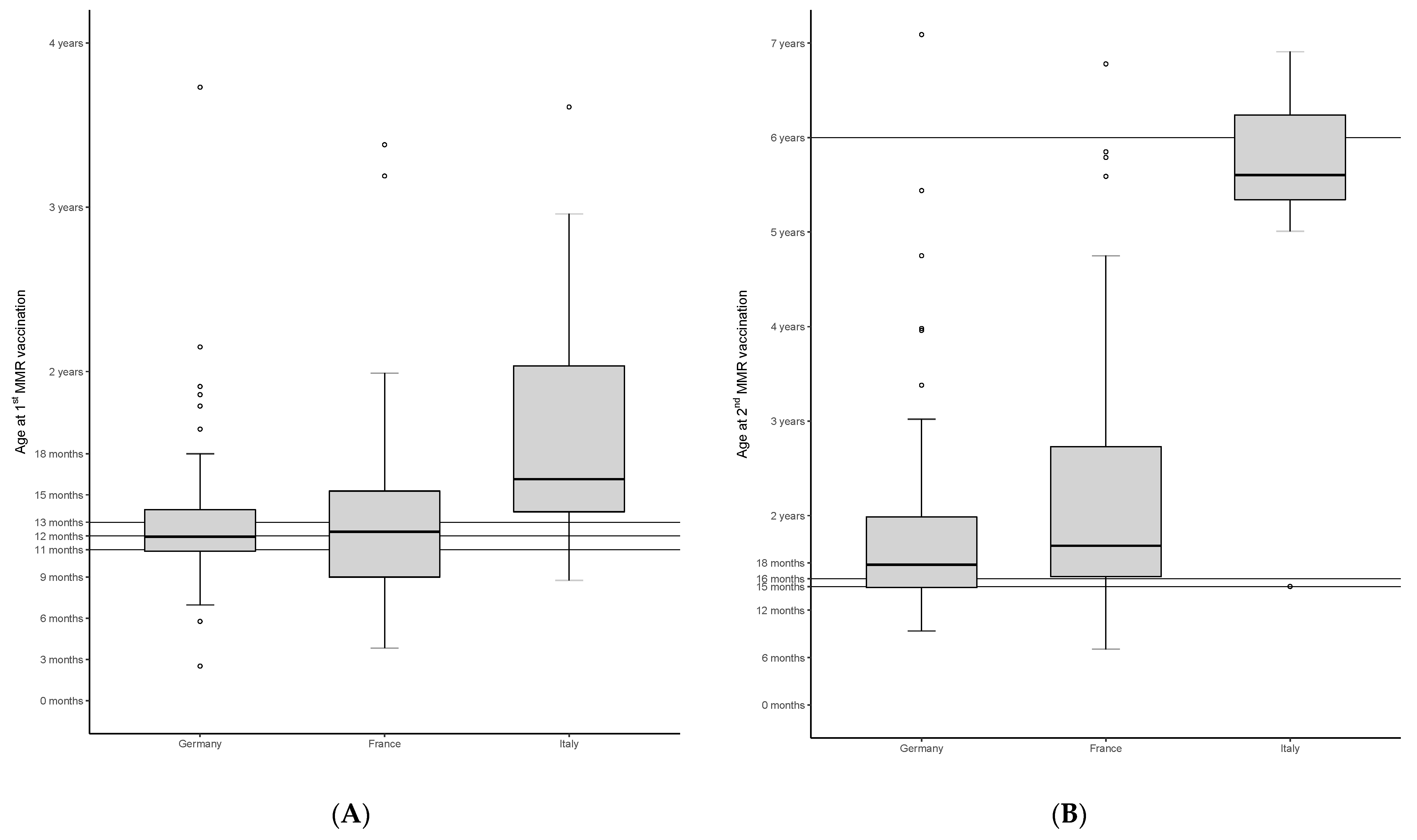
3.4. Age at Vaccination for 1st and 2nd Dose with MMR in Children with Chronic Liver Disease in Germany, France and Italy
3.5. Prevalence of Protective Antibody Levels against Hepatitis A and B, Measles and VZV Prior to Transplantation
3.6. Prevalence of Protective Antibody Levels in Infants with Age-Appropriate Vaccination
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Farmer, D.G.; Venick, R.S.; McDiarmid, S.V.; Ghobrial, R.M.; Gordon, S.A.; Yersiz, H.; Hong, J.; Candell, L.; Cholakians, A.; Wozniak, L.; et al. Predictors of Outcomes after Pediatric Liver Transplantation: An Analysis of More Than 800 Cases Performed at a Single Institution. J. Am. Coll. Surg. 2007, 204, 904–914. [Google Scholar] [CrossRef] [PubMed]
- Wallot, M.; Mathot, M.; Janssen, M.; Hölter, T.; Paul, K.; Buts, J.P.; Reding, R.; Otte, J.B.; Sokal, E.M. Long-term survival and late graft loss in pediatric liver transplant recipients—A 15-year single-center experience. Liver Transpl. 2002, 8, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Elisofon, S.A.; Magee, J.C.; Ng, V.L.; Horslen, S.P.; Fioravanti, V.; Economides, J.; Erinjeri, J.; Anand, R.; Mazariegos, G.V. Society of Pediatric Liver Transplantation Research Group Society of pediatric liver transplantation: Current registry status 2011–2018. Pediatr. Transplant. 2020, 24, e13605. [Google Scholar] [CrossRef] [PubMed]
- Dohna Schwake, C.; Guiddir, T.; Cuzon, G.; Benissa, M.R.; Dubois, C.; Miatello, J.; Merchaoui, Z.; Durand, P.; Tissieres, P. Bicêtre Pediatric Liver Transplant Group Bacterial infections in children after liver transplantation: A single-center surveillance study of 345 consecutive transplantations. Transpl. Infect. Dis. 2020, 22, e13208. [Google Scholar] [CrossRef] [PubMed]
- Feldman, A.G.; Beaty, B.L.; Curtis, D.; Juarez-Colunga, E.; Kempe, A. Incidence of Hospitalization for Vaccine-Preventable Infections in Children Following Solid Organ Transplant and Associated Morbidity, Mortality, and Costs. JAMA Pediatr. 2019, 173, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Feldman, A.G.; Sundaram, S.S.; Beaty, B.L.; Torres, R.; Curtis, D.J.; Kempe, A. Immunization Status at the Time of Liver Transplant in Children and Adolescents. JAMA 2019, 322, 1822–1824. [Google Scholar] [CrossRef]
- L’Huillier, A.G.; Wildhaber, B.; Belli, D.C.; Diana, A.; Rodriguez, M.I.; Siegrist, C.-A.; Barbe, K.M.P. Successful serology-based intervention to increase protection against vaccine-preventable diseases in liver-transplanted children: A 19-yr review of the Swiss national reference center. Pediatr. Transplant. 2011, 16, 50–57. [Google Scholar] [CrossRef] [PubMed]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Signorelli, C.; Odone, A.; Cella, P.; Iannazzo, S.; D’Ancona, F.; Guerra, R. Infant immunization coverage in Italy (2000–2016). Ann. Ist. Super Sanita 2017, 53, 231–237. [Google Scholar]
- Vaccine Schedules in All Countries in the EU/EEA. Available online: https://vaccine-schedule.ecdc.europa.eu/ (accessed on 31 May 2021).
- Rieck, T.; Feig, M.; Wichmann, O.; Siedler, A. Impfquoten von Kinderschutzimpfungen in Deutschland—Aktuelle Ergebnisse aus der RKI-Impfsurveillance. Epid Bull 2020, 32/33, 9–27. [Google Scholar] [CrossRef]
- Données de Couverture Vaccinale Rougeole, Rubéole, Oreillons par Groupe D’âge. Available online: https://www.santepubliquefrance.fr/determinants-de-sante/vaccination/articles/donnees-de-couverture-vaccinale-rougeole-rubeole-oreillons-par-groupe-d-age (accessed on 31 May 2021).
- D’Ancona, F.; D’Amario, C.; Maraglino, F.; Rezza, G.; Iannazzo, S. The law on compulsory vaccination in Italy: An update 2 years after the introduction. Eurosurveillance 2019, 24, 1900371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaudelus, J.; Cohen, R.; Leboucher, B.; Stahl, J.; Denis, F.; Pujol, P.; Longfier, L.; Martinot, A. Meningococcal C vaccine coverage in France in infants, children, and adolescents. Med. Mal. Infect. 2019, 49, 180–186. [Google Scholar] [CrossRef]
- Leung, D.H.; Economides, J.M.; Healy, C.M.; Ton-That, M. High Prevalence of Hepatitis B Nonimmunity in Vaccinated Pediatric Liver Transplant Recipients. Arab. Archaeol. Epigr. 2015, 15, 535–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sintusek, P.; Posuwan, N.; Wanawongsawad, P.; Jitraruch, S.; Poovorawan, Y.; Chongsrisawat, V. High prevalence of hepatitis B-antibody loss and a case report of de novo hepatitis B virus infection in a child after living-donor liver transplantation. World J. Gastroenterol. 2018, 24, 752–762. [Google Scholar] [CrossRef]
- Hartley, J.L.; Davenport, M.; Kelly, D.A. Biliary atresia. Lancet 2009, 374, 1704–1713. [Google Scholar] [CrossRef]
- Feldman, A.G.; Kempe, A.; Beaty, B.L.; Sundaram, S.S.; Studies of Pediatric Liver Transplantation (SPLIT) Research Group. Immunization practices among pediatric transplant hepatologists. Pediatr. Transplant. 2016, 20, 1038–1044. [Google Scholar] [CrossRef]
- McCashland, T.M.; Preheim, L.C.; Gentry-Nielsen, M.J. Pneumococcal Vaccine Response in Cirrhosis and Liver Transplantation. J. Infect. Dis. 2000, 181, 757–760. [Google Scholar] [CrossRef] [Green Version]
- Levitsky, J.; Kalil, A.C.; Meza, J.L.; Hurst, G.E.; Freifeld, A. Chicken pox after pediatric liver transplantation. Liver Transplant. 2005, 11, 1563–1566. [Google Scholar] [CrossRef] [PubMed]
- Feldhoff, C.M.; Balfour, H.H.; Simmons, R.L.; Najarian, J.S.; Mauer, S.M. Varicella in children with renal transplants. J. Pediatr. 1981, 98, 25–31. [Google Scholar] [CrossRef]
- Rubin, L.G.; Levin, M.J.; Ljungman, P.; Davies, E.G.; Avery, R.; Tomblyn, M.; Bousvaros, A.; Dhanireddy, S.; Sung, L.; Keyserling, H.; et al. Infectious Diseases Society of America 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin. Infect. Dis. 2014, 58, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.; Colgrove, J.; Verger, P. Why France is making eight new vaccines mandatory. Vaccine 2018, 36, 1801–1803. [Google Scholar] [CrossRef]
- Di Pietro, A.; Visalli, G.; Antonuccio, G.M.; Facciolà, A. Today’s vaccination policies in Italy: The National Plan for Vaccine Prevention 2017-2019 and the Law 119/2017 on the mandatory vaccinations. Ann. Ig. 2019, 31, 54–64. [Google Scholar] [PubMed]
- Robert Koch-Institut. Gesetz für den Schutz vor Masern und zur Stärkung der Impfprävention (Masernschutzgesetz). Bulletin 2020, 3–5. [Google Scholar] [CrossRef]
- Fadda, M.; Galimberti, E.; Fiordelli, M.; Schulz, P.J.; De La Torre, I.; Christiansen, M.; Zapata, F.S. Evaluation of a Mobile Phone–Based Intervention to Increase Parents’ Knowledge About the Measles-Mumps-Rubella Vaccination and Their Psychological Empowerment: Mixed-Method Approach. JMIR mHealth uHealth 2018, 6, e59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vann, J.C.J.; Jacobson, R.M.; Coyne-Beasley, T.; Asafu-Adjei, J.K.; Szilagyi, P.G. Patient reminder and recall interventions to improve immunization rates. Cochrane Database Syst. Rev. 2018, 1, CD003941. [Google Scholar] [CrossRef]
- Wu, J.-F.; Ni, Y.-H.; Chen, H.-L.; Hsu, H.-Y.; Lai, H.-S.; Chang, M.H. Humoral immunogenicity to measles, rubella, and varicella-zoster vaccines in biliary atresia children. Vaccine 2009, 27, 2812–2815. [Google Scholar] [CrossRef] [PubMed]
- Yoeli, J.K.; Yoeli, D.; Miloh, T.A.; Rana, A.; Goss, J.A.; Munoz-Rivas, F. Measles, mumps, rubella (vaccine) and varicella vaccines in pediatric liver transplant: An initial analysis of post-transplant immunity. Pediatr. Transplant. 2019, 23, e13490. [Google Scholar] [CrossRef] [PubMed]
- Barbe, K.M.P.; Pittet, L.; Sottas, C.E.; Grillet, S.; Wildhaber, B.; Rodriguez, M.I.; Kaiser, L.; Belli, D.C.; McLin, V.A.; Siegrist, C.-A. Varicella-Zoster Immunization in Pediatric Liver Transplant Recipients: Safe and Immunogenic. Arab. Archaeol. Epigr. 2012, 12, 2974–2985. [Google Scholar] [CrossRef]


{kind=link}
| Chronic Liver Disease (n = 363) | Control Group/Acute Liver Disease (n = 67) | p | |
|---|---|---|---|
| Gender, male (%) | 179 (49.3%) | 39 (58.2%) | 0.181 |
| Diagnosis | BA: 221 (60.9%) Metabolic: 35 (9.6%) PFIC: 25 (6.9%) Cryptogenic cirrhosis: 23 (6.3%) Alagille: 13 (3.6%) CF: 12 (3.3%) Other: 34 (9.3%) | Malignancy: 34 (50.7%) Acute liver failure: 26 (38.8%) Neonatal onset: 6 (9.0%) Amanita phalloides poisoning: 1 (1.5%) | |
| Country distribution of patients | Germany: 163 (44.9%) France: 106 (29.2%) Italy: 84 (23.1%) Lithuania: 10 (2.8%) | Germany: 42 (62.7%) France: 8 (11.9%) Italy: 16 (23.9%) Lithuania: 1 (1.5%) | |
| Age at time of transplant, median (IQR) | 1.6 (0.7–4.8) | 2.2 (1.3–4.7) | 0.314 |
| Year of birth, median (IQR) | 2011 (2007–2015) | 2011 (2007–2015) | 0.849 |
| Vaccine | Chronic Liver Disease | Control Group | p |
|---|---|---|---|
| DTP-PV-Hib | 80.2% (291/363) | 85.5% (53/62) | 0.324 |
| Hepatitis B | 74.1% (269/363) | 79.0% (49/62) | 0.409 |
| Hepatitis A | 42.0% (100/238) | 7.7% (4/52) | <0.00001 |
| Pneumococcal conjugate vaccine | 66.5% (230/346) | 79.3% (46/58) | 0.052 |
| Pneumococcal polysaccharide vaccine | 20.1% (30/149) | 2.9% (1/34) | 0.016 |
| Rotavirus (since 2006) | 16.6% (46/277) | 30.6% (15/49) | 0.020 |
| MenC | 65.7% (134/204) | 59.2% (29/49) | 0.393 |
| MenB (since 2013) | 22.0% (40/182) | 16.1% (5/31) | 0.461 |
| MenACWY (since 2010) | 8.1% (19/236) | 6.7% (3/45) | 0.751 |
| HPV | 20.0% (3/15) | 0.0% (0/2) | Ø |
| MMR | 81.1% (198/244) | 62.3% (33/53) | 0.003 |
| VZV | 65.2% (144/221) | 54.9% (28/51) | 0.171 |
| Germany | France | Italy | ||||
|---|---|---|---|---|---|---|
| Chronic Transplant Candidates | Healthy Children [12] | Chronic Transplant Candidates | Healthy Children | Chronic Transplant Candidates | Healthy Children [14] | |
| MenC received in % up to 24 months of age | 44.8% | 77.8% | 40.5% | 65.3% [15] | 43.6% | 87.8% |
| 1st MMR received in % up to 24 months of age | 86.5% | 89.8% | 90.2% | 90.9% [13] | 60.4% | 94.1% |
| 2nd MMR received in % up to 24 months of age | 65.8% | 69.9% | 50.7% | 83.4% [13] | 57.9% up to 84 months | 90.1% up to 84 months |
| 1st VZV received in % up to 24 months of age | 81.1% | 83.7% | 46.7% | % | 46.8% | 46.7% |
| 2nd VZV received in % up to 24 months of age | 46.2% | 66.0% | 10.5% | % | 26.3% up to 72 months | % |
| Vaccine | Chronic Liver Disease | Control Group | p |
|---|---|---|---|
| Hepatitis B | 63.3% (195/308) | 80.0% (40/50) | 0.021 |
| Hepatitis A | 60.1% (169/281) | 39.5% (17/43) | 0.011 |
| Measles | 62.9% (163/259) | 70.7% (29/41) | 0.334 |
| VZV | 53.1% (163/307) | 68.8% (33/48) | 0.042 |
| Vaccine | Chronic Liver Disease | Control Group | p |
|---|---|---|---|
| Hepatitis B | 68.6% (131/191) | 81.1% (30/37) | 0.127 |
| Hepatitis A | 88.9% (80/90) | 100.0% (4/4) | 1.00 |
| Measles | 80.6% (125/155) | 72.7% (16/22) | 0.388 |
| VZV | 67.4% (91/135) | 80.8% (21/26) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laue, T.; Demir, Z.; Debray, D.; Cananzi, M.; Gaio, P.; Casotti, V.; D’Antiga, L.; Urbonas, V.; Baumann, U. Under-Vaccination in Pediatric Liver Transplant Candidates with Acute and Chronic Liver Disease—A Retrospective Observational Study of the European Reference Network TransplantChild. Children 2021, 8, 675. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080675
Laue T, Demir Z, Debray D, Cananzi M, Gaio P, Casotti V, D’Antiga L, Urbonas V, Baumann U. Under-Vaccination in Pediatric Liver Transplant Candidates with Acute and Chronic Liver Disease—A Retrospective Observational Study of the European Reference Network TransplantChild. Children. 2021; 8(8):675. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080675
Chicago/Turabian StyleLaue, Tobias, Zeynep Demir, Dominique Debray, Mara Cananzi, Paola Gaio, Valeria Casotti, Lorenzo D’Antiga, Vaidotas Urbonas, and Ulrich Baumann. 2021. "Under-Vaccination in Pediatric Liver Transplant Candidates with Acute and Chronic Liver Disease—A Retrospective Observational Study of the European Reference Network TransplantChild" Children 8, no. 8: 675. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080675