
Cross-Sectional Survey on Long Term Sequelae of Pediatric COVID-19 among Italian Pediatricians

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence, Practitioners RC of G, Scotland HI. COVID-19 rapid guideline: Managing the longterm effects of COVID-19. NICE Guidel. 2020, 1–35. [Google Scholar]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11. [Google Scholar] [CrossRef]
- Ludvigsson, J.F. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020, 109, 1088–1095. [Google Scholar] [CrossRef]
- Parisi, G.F.; Brindisi, G.; Indolfi, C.; Diaferio, L.; Marchese, G.; Ghiglioni, D.G.; Zicari, A.M.; Del Giudice, M.M. Upper airway involvement in pediatric COVID-19. Pediatr. Allergy Immunol. 2020, 31, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Parisi, G.F.; Indolfi, C.; Decimo, F.; Leonardi, S.; del Giudice, M.M. COVID-19 Pneumonia in Children: From Etiology to Management. Front. Pediatr. 2020, 8, 616622. [Google Scholar] [CrossRef]
- Ludvigsson, J.F. Case report and systematic review suggest that children may experience similar long-term effects to adults after clinical COVID-19. Acta Paediatr. 2021, 110, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Munblit, D.; De Rose, C.; Sinatti, D.; Ricchiuto, A.; Carfi, A.; Valentini, P. Preliminary evidence on long COVID in children. Acta Paediatr. 2021, 110, 2208–2211. [Google Scholar] [CrossRef] [PubMed]
- Brackel, C.L.H.; Lap, C.R.; Buddingh, E.P.; Houten, M.A.; van der Sande, L.J.T.M.; Langereis, E.J.; Bannier, M.A.G.E.; Pijnenburg, M.W.H.; Hashimoto, S.; Terheggen-Lagro, S.W.J. Pediatric long-COVID: An overlooked phenomenon? Pediatr. Pulmonol. 2021. [Google Scholar] [CrossRef]
- Ludvigsson, J.F. Reporting suspicions of long COVID in children is justified during this global emergency. Acta Paediatr. 2021, 110, 1373. [Google Scholar] [CrossRef]
- Diaferio, L.; Parisi, G.F.; Brindisi, G.; Indolfi, C.; Marchese, G.; Ghiglioni, D.G.; Zicari, A.M.; Marseglia, G.L.; Del Giudice, M.M. Cross-sectional survey on impact of paediatric COVID-19 among Italian paediatricians: Report from the SIAIP rhino-sinusitis and conjunctivitis committee. Ital. J. Pediatr. 2020, 46, 1–6. [Google Scholar] [CrossRef]
- Molteni, E.; Sudre, C.H.; Canas, L.S.; Bhopal, S.S.; Hughes, R.C.; Antonelli, M.; Murray, B.; Kläser, K.; Kerfoot, E.; Chen, L.; et al. Illness duration and symptom profile in symptomatic UK school-aged children tested for SARS-CoV-2. Lancet Child Adolesc. Health 2021, 3. [Google Scholar] [CrossRef]
- Ashkenazi-Hoffnung, L.; Shmueli, E.; Ehrlich, S.; Ziv, A.; Bar-On, O.; Birk, E.; Lowenthal, A.; Prais, D. long COVID in Children: Ob-servations From A Designated Pediatric Clinic. Pediatr. Infect. Dis. J. 2021. EPUB Ahead of Print. [Google Scholar] [CrossRef]
- Wostyn, P. COVID-19 and chronic fatigue syndrome: Is the worst yet to come? Med. Hypotheses 2021, 146, 110469. [Google Scholar] [CrossRef] [PubMed]
- Rivera, M.C.; Mastronardi, C.; Silva-Aldana, C.T.; Arcos-Burgos, M.; Lidbury, B.A. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Comprehensive Review. Diagnostics 2019, 9, 91. [Google Scholar] [CrossRef] [Green Version]
- Clayton, E.W. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. JAMA 2015, 313, 1101–1102. [Google Scholar] [CrossRef]
- Proal, A.; Marshall, T. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome in the Era of the Human Microbiome: Persistent Pathogens Drive Chronic Symptoms by Interfering With Host Metabolism, Gene Expression, and Immunity. Front. Pediatr. 2018, 6. [Google Scholar] [CrossRef]
- Lam, M.H.-B.; Wing, Y.-K.; Yu, M.W.-M.; Leung, C.-M.; Ma, R.C.W.; Kong, A.P.S.; So, W.; Fong, S.Y.-Y.; Lam, S.-P. Mental Morbidities and Chronic Fatigue in Severe Acute Respiratory Syndrome Survivors: Long-term Follow-up. Arch. Intern. Med. 2009, 169, 2142–2147. [Google Scholar] [CrossRef] [Green Version]
- Moldofsky, H.; Patcai, J. Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol. 2011, 11, 37. [Google Scholar] [CrossRef] [Green Version]
- Lidbury, B.A. Ross River Virus Immune Evasion Strategies and the Relevance to Post-viral Fatigue, and Myalgic Encephalomyelitis Onset. Front. Med. 2021, 8. [Google Scholar] [CrossRef]
- Lipton, J.O.; Sahin, M. The Neurology of mTOR. Neuron 2014, 84, 275–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, B.; Lamming, D.W. The Mechanistic Target of Rapamycin: The Grand ConducTOR of Metabolism and Aging. Cell Metab. 2016, 23, 990–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| QUESTION | POSSIBLE ANSWERS |
|---|---|
| When the swab was negative, how many patients were still symptomatic? | a. 0–20% b. 20–40% c. 40–60% d. 60–80% e. >80% |
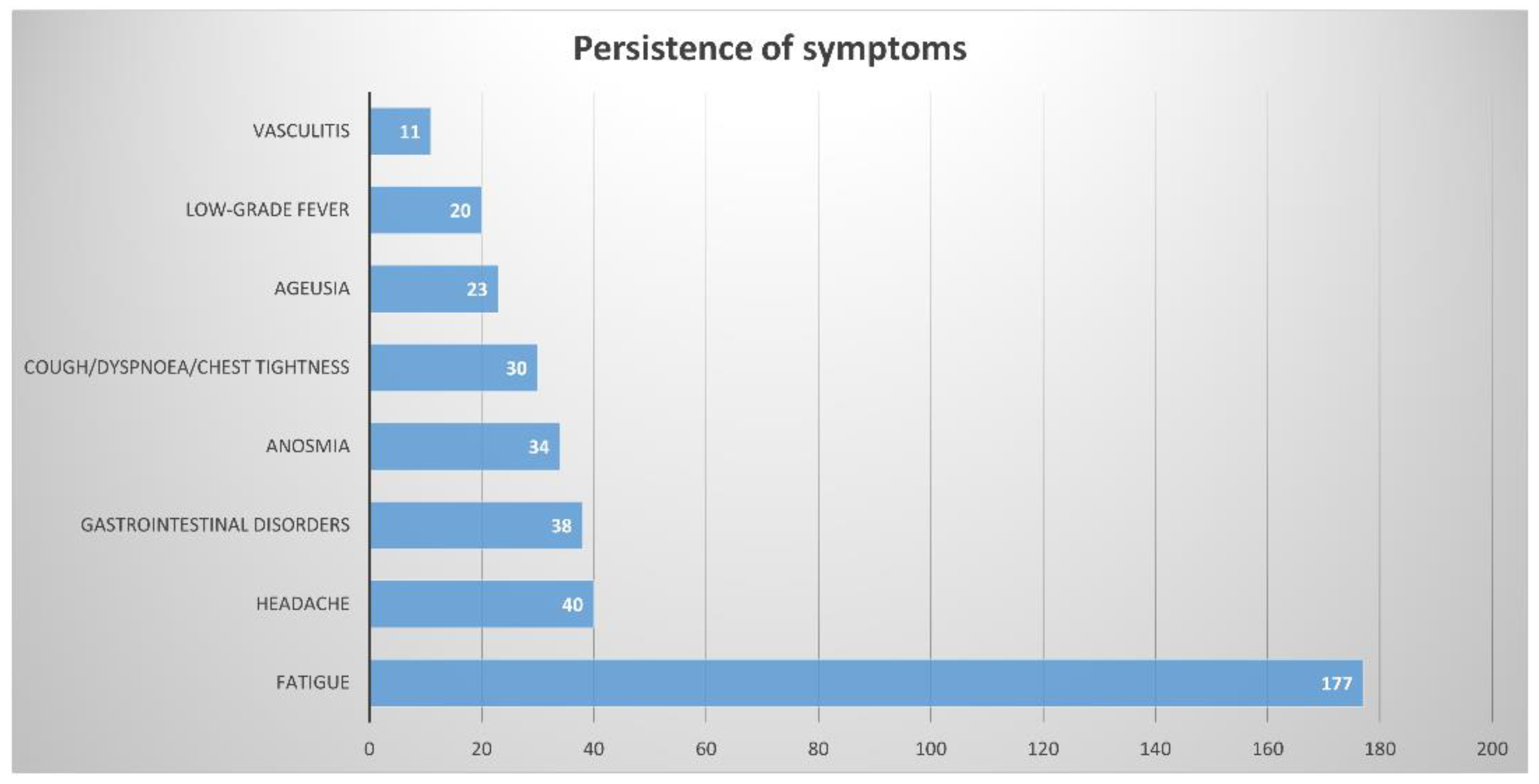
| Which of the following symptoms seem to persist even after the swab negativization (one or more responses allowed)? | a. low-grade fever b. cough/dyspnea/chest tightness c. fatigue d. anosmia e. ageusia f. headache g. vasculitis h. gastrointestinal disorders |
| Is it your habit to evaluate the antibody response with a serological test after clinical recovery? | a. Yes b. No c. It depends on the cases |
| In your reality, is there a clinic dedicated to the management of children recovered from covid-19? | a. Yes b. No |
| Total of Participants | 267 |
|---|---|
| Sex (male versus female) | 92 (34.4%) versus 175 (65.6%) |
| Age (years old): | |
| I. 20–30 | I. 0 (0%) |
| II. 31–40 | II. 11 (4.2%) |
| III. 41–50 | III. 40 (14.9%) |
| IV. 51–60 | IV. 84 (31.3%) |
| V. >60 | V. 132 (49.6%) |
| Types of pediatricians: | |
| i. Primary care | I. 202 (75.5%) |
| ii. Pediatric hospital medicine | II. 42 (16.3%) |
| iii. Pediatric emergency medicine | III. 5 (1.9%) |
| iv. Specialized outpatient healthcare | IV. 14 (5.4%) |
| v. Pediatric critical care medicine | V. 2 (0.9%) |
| vi. Pediatric infectious disease | VI. 0% |
| vii. no answer | VII. 2 |
| Territorial subdivisions (South and Islands versus Center of Italy versus Northern Italy) | 52 (19.4%) versus 73 (27.4%) versus 142 (53.2%). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parisi, G.F.; Diaferio, L.; Brindisi, G.; Indolfi, C.; Umano, G.R.; Klain, A.; Marchese, G.; Ghiglioni, D.G.; Zicari, A.M.; Marseglia, G.L.; et al. Cross-Sectional Survey on Long Term Sequelae of Pediatric COVID-19 among Italian Pediatricians. Children 2021, 8, 769. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090769
Parisi GF, Diaferio L, Brindisi G, Indolfi C, Umano GR, Klain A, Marchese G, Ghiglioni DG, Zicari AM, Marseglia GL, et al. Cross-Sectional Survey on Long Term Sequelae of Pediatric COVID-19 among Italian Pediatricians. Children. 2021; 8(9):769. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090769
Chicago/Turabian StyleParisi, Giuseppe Fabio, Lucia Diaferio, Giulia Brindisi, Cristiana Indolfi, Giuseppina Rosaria Umano, Angela Klain, Giuseppe Marchese, Daniele Giovanni Ghiglioni, Anna Maria Zicari, Gian Luigi Marseglia, and et al. 2021. "Cross-Sectional Survey on Long Term Sequelae of Pediatric COVID-19 among Italian Pediatricians" Children 8, no. 9: 769. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090769