1. Introduction
The years in childhood and adolescence are a foundation for the rest of your life. Health and well-being are important for development and factors, like good sleep habits and adequate levels of physical activity (PA), are important [
1,
2]. PA is associated with physical [
3], mental [
3], social and cognitive health benefits [
4], and physical inactivity increases the risk for ill-health [
3]. The benefits include lower adiposity, improved cardio-metabolic biomarker profile, increased physical fitness, improved bone health, and improved motor skill development [
4]. The PA recommendations from the World Health Organization (WHO) for children and adolescents are to spend an average of 60 min/day in moderate-to-vigorous PA (MVPA), conduct musculoskeletal strengthening exercises at least three days/week, and limit sedentary time [
3,
5]. PA can be divided into chronic PA (regular PA) and acute PA (sporadic occurrences). As opposed to chronic PA, which has long-term effects, the effects of acute PA on sleep are detectable only on the night following the acute PA [
6]. For instance, a meta-analysis including adolescents and adults found that the effects of acute PA resulted in 10 min of significantly increased sleep length, a deeper sleep, and falling asleep faster on nights following a day with acute PA [
6].
Around the globe, physical fitness muscle power and cardiovascular fitness decreased in children and adolescents between the year 1986 to 2015 [
7]. Nowadays, a majority (81%) of the children and adolescents spend less than 60 min in MVPA every day [
8].
It is common that PA declines during adolescence to early adulthood [
2]. Girls spend less time in PA than boys and since the year 2001, the prevalence of insufficient PA has decreased for boys but not for girls around the globe [
8]. In Sweden, a majority of children and adolescents do not meet the PA recommendations [
8]. In Sweden, the prevalence of children and adolescents that meet the PA recommendations have not increased during the previous decades [
3] and a majority spends less than 60 min every day in PA (82.2% boys and 87.3% girls) [
8].
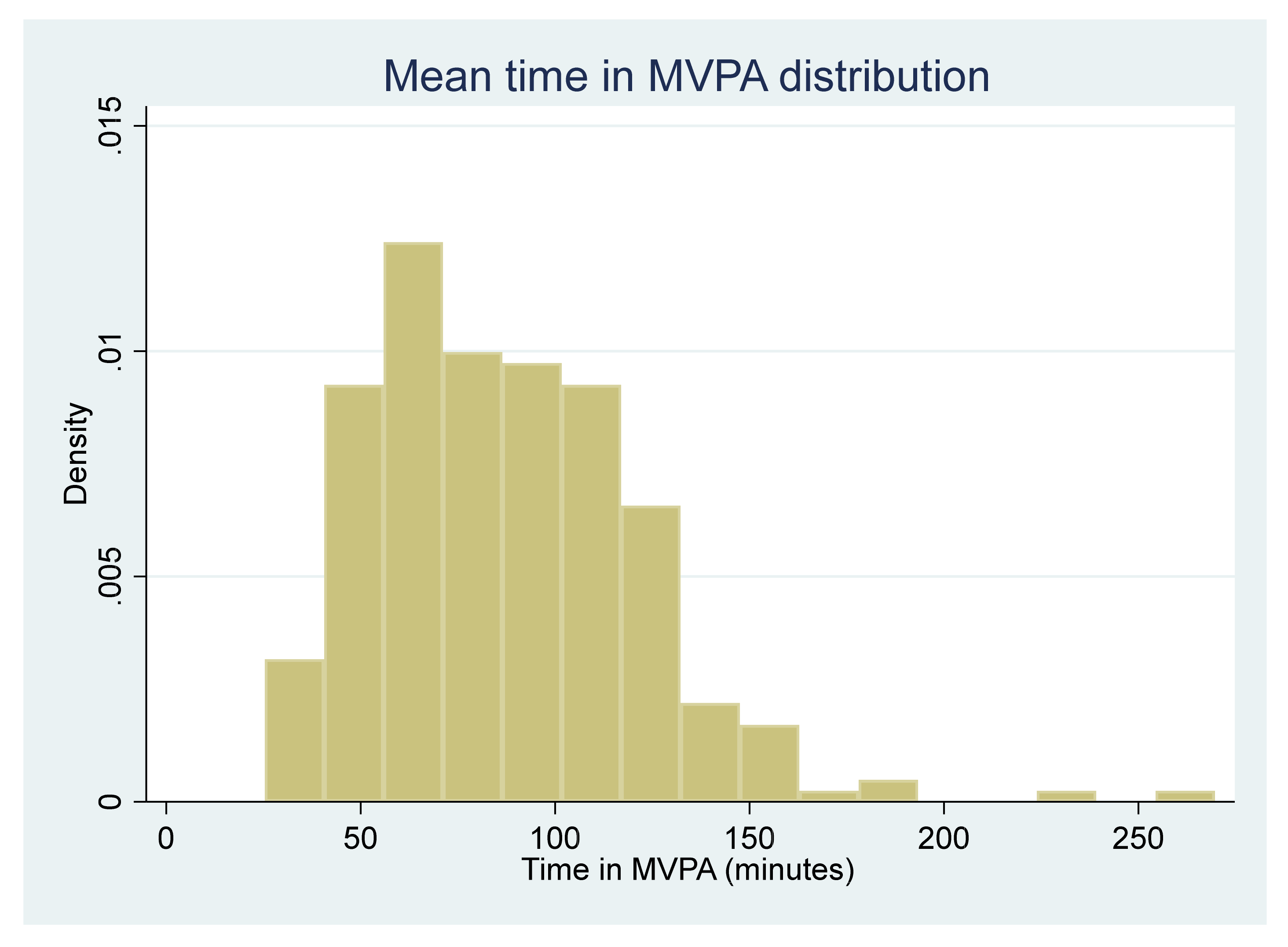
PA can be measured both with subjective measurements like questionnaires and other self-reported measures and via objective measures like doubly labeled water and accelerometers [
2]. The most common method for measuring PA is via objective measures with accelerometers, and accelerometers provide more robust and precise measures of the PA than subjective measures [
2,
9].
Sleep is important for children and adolescents’ physical, psychological, and academic functioning [
2], and insufficient sleep have been associated with ill-health [
4,
10,
11]. In addition, insufficient sleep could increase psychological ill health and threaten academic success [
4,
11]. A previous systematic review found that children and adolescents with longer sleep durations had lower adiposity indicators, better emotional regulation, higher academic achievements, and better life quality than children with shorter sleep duration [
4]. While there are no sleep recommendations in Sweden, The National Sleep Foundation in the United States has developed national sleep recommendations for children and adolescents; between 9–11 h of nocturnal sleep for children aged 6–13 years and 8–10 h for 14–17-year-olds [
12]. It is common that the sleep patterns shift during adolescence and this shift might be caused by psychological, social, behavioral, and pubertal changes [
2]. The physical changes during adolescence and puberty include changes in the circadian rhythm and the homeostatic sleep components, which influence the sleep-wake cycle, sleep timing, sleep duration, and sleep architecture [
2].
During the past decades, there has been a trend of declining sleep length in children and adolescents around the globe, and sleep deprivation has increased [
4,
13]. The decline can be seen in most countries (also in Sweden), age groups, and both sexes [
13,
14]. In addition, it is more common that boys have later nocturnal sleep times and do not meet the recommendations than girls [
14].
Previous studies that have examined the association between PA and sleep have resulted in mixed findings and potential mechanisms are still mainly unknown [
11,
15]. A previous systematic review with children and adolescents resulted in contradictory findings regarding sleep length and time in MVPA [
15]. However, the authors concluded that sleep length might be associated with sedentary behavior rather than time in MVPA [
15]. Furthermore, previous studies have examined if and how PA could affect sleep length, but the studies have been unable to detect statistically significant findings [
2,
10,
11]. A common belief is that conducting PA shortly before sleep could disrupt sleep. A prior study found mixed results regarding this belief; PA had potentially negative effects on sleep in adults but positive effects on children [
2]. Despite this, the existing literature implies that PA probably is beneficial for sleep in children, adolescents, and young adults [
2,
10,
16]. For instance, a systematic review found that children and adolescents with more PA were more likely to experience better nocturnal sleep [
2]. In addition, an intervention study found that increased time in MVPA improved sleep duration, sleep depth, sleep efficiency, increased rapid eye movement (REM) sleep latency, and decreased sleep onset latency in children and adolescents [
2,
10,
17]. However, due to the age-related decline in both PA and sleep during adolescence [
1,
2] less than 20% of the children and adolescents meet both the PA and sleep recommendations [
1]. In addition, those with low socioeconomic positions and poor economies are less active and have a higher risk of short sleep length [
5,
18]. Screen time has also been associated with a shorter sleep length [
14] and increased time in physical inactivity [
19]. The theoretical concepts consist of hypotheses for how PA could affect sleep and includes physical [
2,
10,
20] and psychological [
20] changes. Physical changes include the facts that sleep serves energy conservation, body restoration, and thermoregulatory functions—which are factors that are reversely affected by PA [
2,
10]. The psychological changes from PA are decreased anxiety and stress, which could improve sleep [
20]. Opdal et al. aimed to examine the association between PA and mental distress with a longitudinal study design [
21]. However, Opdal et al. were unable to detect changes in the PA and mental distress during the follow-up period [
21]. Though additional studies are needed, it is possible that the relationship between PA and sleep is synergetic and works via multiple complex physiological and psychological pathways [
2].
In addition to the potential confounders of sex, age, mental health, socioeconomic position, and screen time that have been mentioned above, the association between PA and sleep might also be mediated or moderated by sleep quality, daylight length, and the PA characteristics [
2,
10].
The evidence of an association between PA and sleep in children and adolescents are limited and this depends partly on methodological differences [
2], poor designs [
2,
11], and limited populations in the reported studies [
4]. There is a need for additional studies which have the potential to examine an association and yield high-quality evidence [
1]. It is the first time that measurements on sleep have been included and analyzed using the Health Behavior in School aged Children (HBSC) survey questionnaire by the Public Health Agency of Sweden. To the knowledge of the authors, an association between PA and sleep has not previously been studied in children and adolescents living in Sweden.
Aim and Research Questions
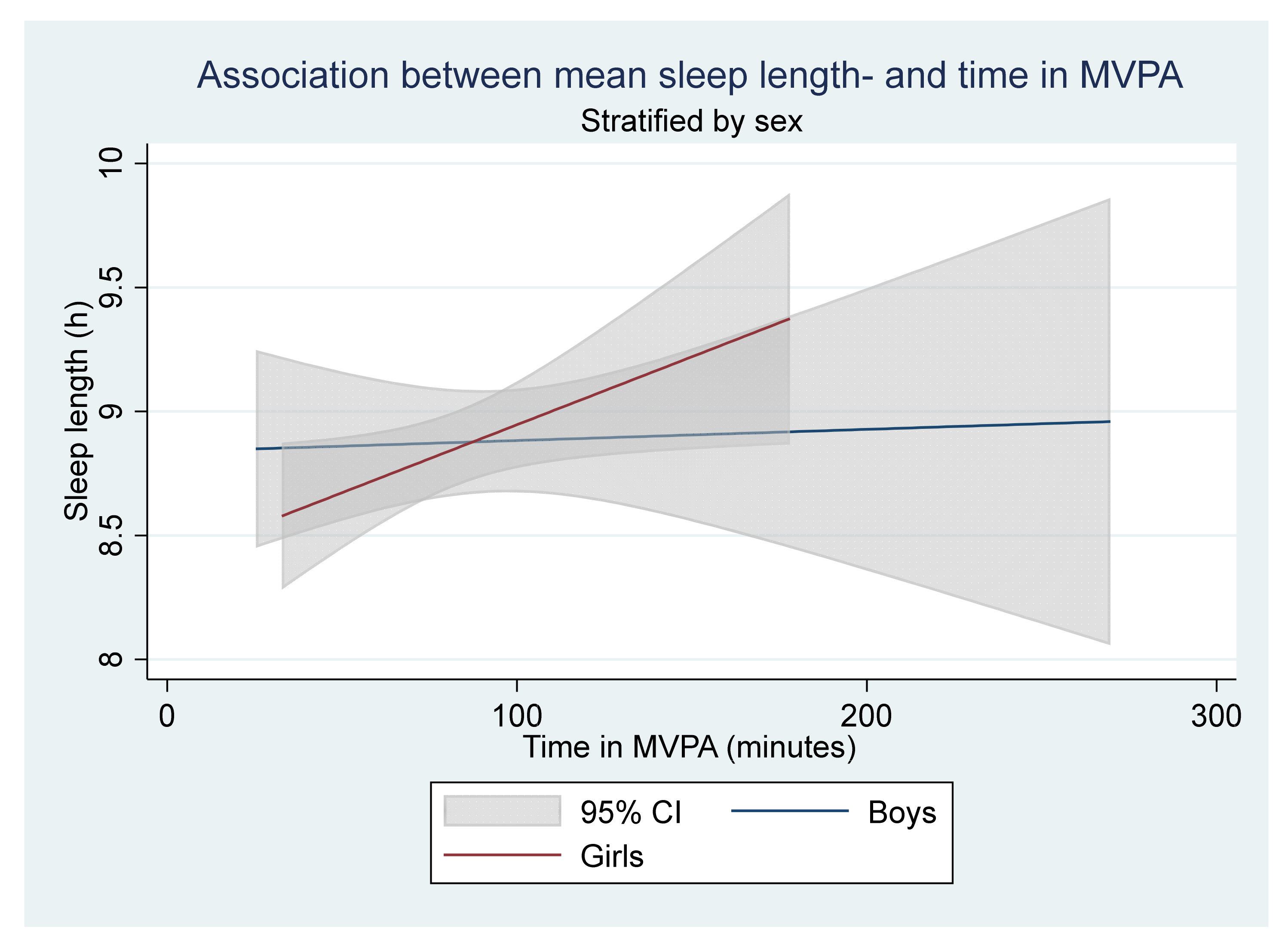
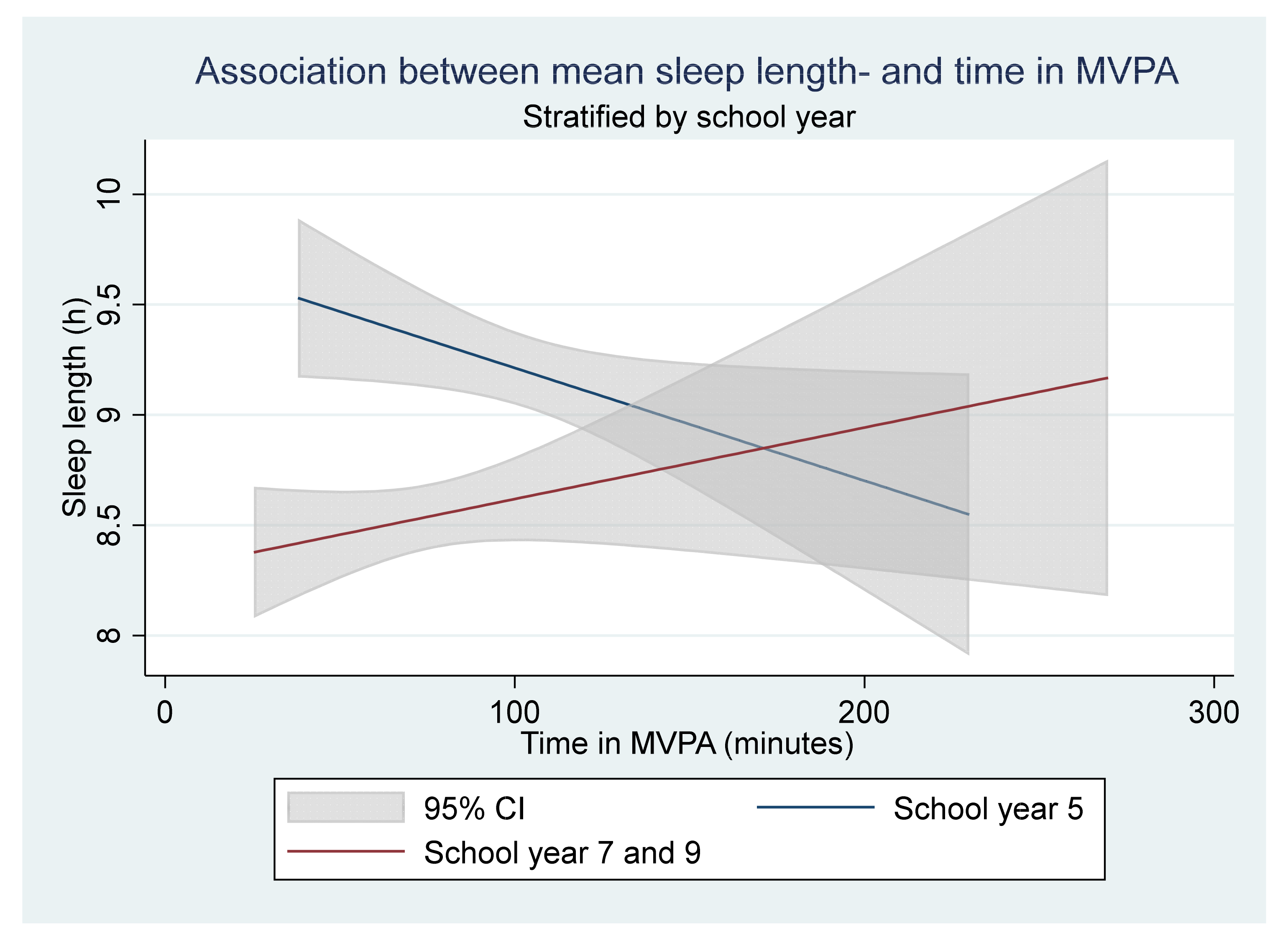
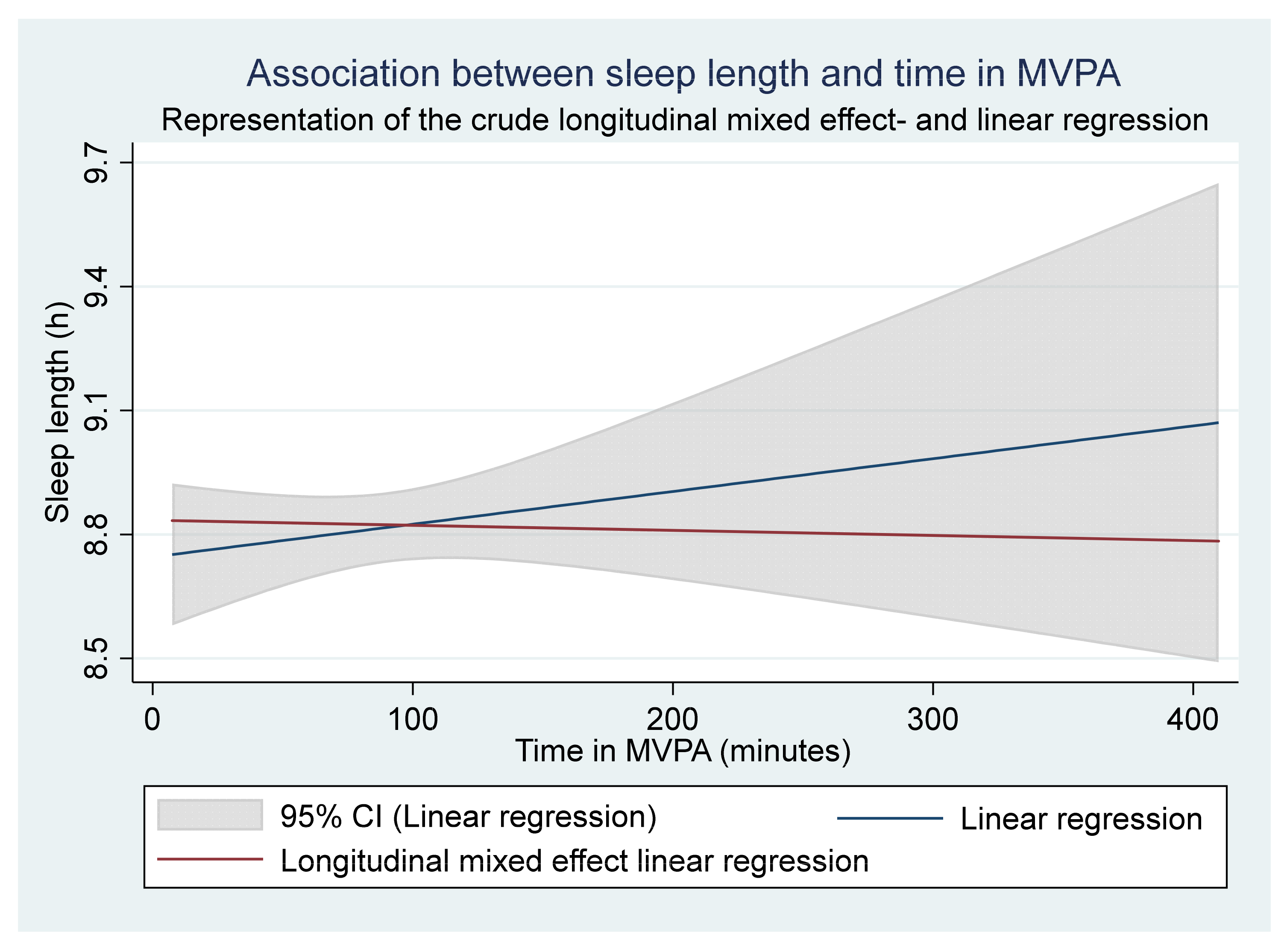
The primary aim was to examine if there is a dose-response relationship between time spent in acute MVPA and sleep length in children and adolescents. The secondary aim was to examine if the sleep length was higher for participants that spent an average of at least 60 min in MVPA/day. An additional aim was to distinguish differences in PA and sleep length between sex and school years.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








