
The Effect of Incorporating an Exergame Application in a Multidisciplinary Weight Management Program on Physical Activity and Fitness Indices in Children with Overweight and Obesity


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Procedure
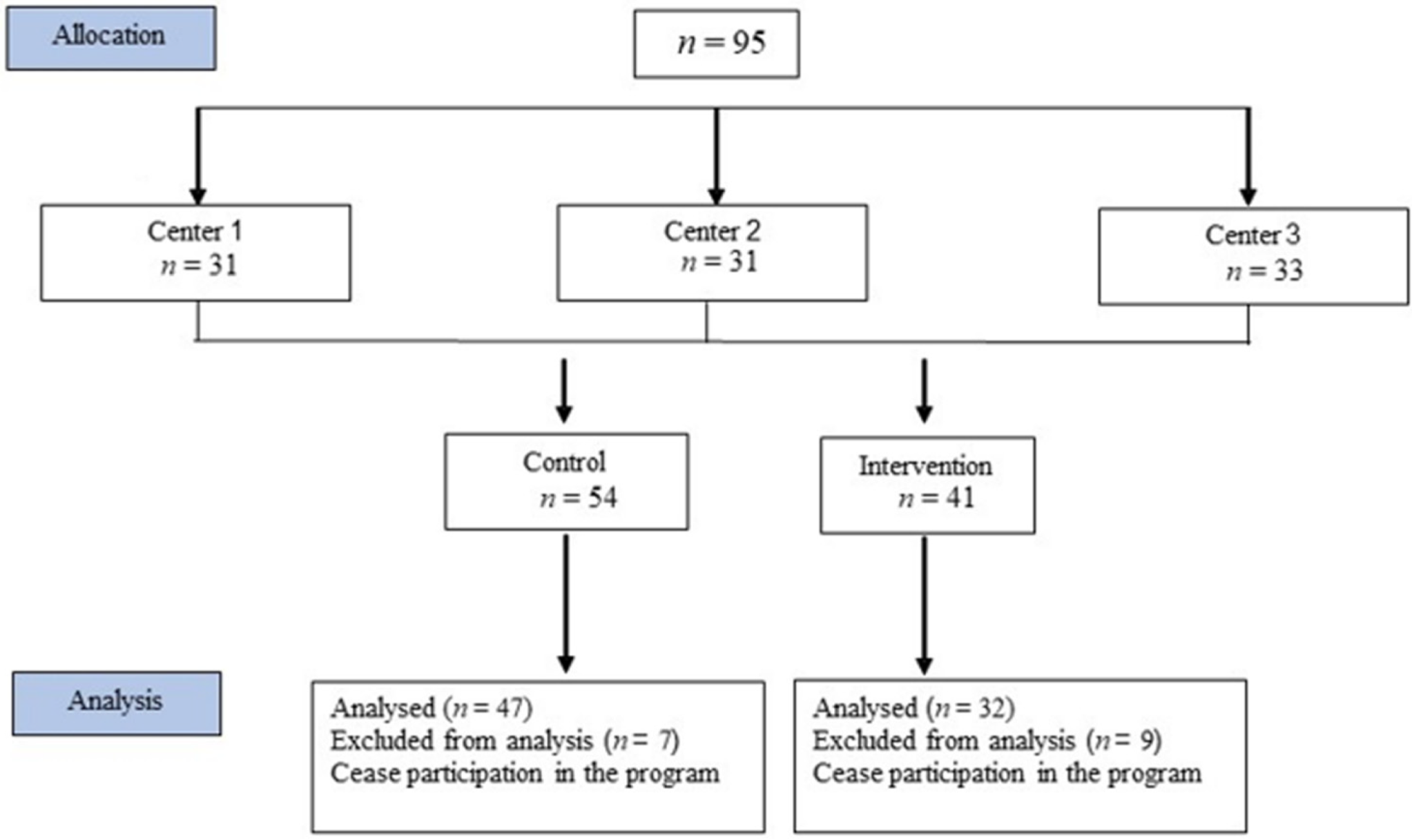
2.2. Participants
2.3. Interventions Protocol
2.4. Measurements
2.4.1. Anthropometric Measurements
2.4.2. Fitness Tests
2.4.3. Questionnaires
2.5. Statistical Analyses
3. Results
3.1. Anthropometric Measures
3.2. Fitness Components
3.3. Attitude toward Physical Activity
3.4. Program Compliance and Self-Reported Physical Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lobstein, T.; Jackson-Leach, R.; Moodie, M.L.; Hall, K.D.; Gortmaker, S.L.; Swinburn, B.A.; James, W.P.T.; Wang, Y.; McPherson, K. Child and adolescent obesity: Part of a bigger picture. Lancet 2015, 385, 2510–2520. [Google Scholar] [CrossRef] [Green Version]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Child-hood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- Barlow, S.E. the Expert Committee: Expert committee recommendations on the as-sessment, prevention, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120, s124–s192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietz, W.H. Reversing the tide of obesity. Lancet 2011, 378, 744–746. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Barnes, J.D.; González, S.A.; Katzmarzyk, P.T.; Onywera, V.O.; Reilly, J.J.; Tomkinson, G.R. Global Matrix 2.0: Report Card Grades on the Physical Activity of Children and Youth Comparing 38 Countries. J. Phys. Act. Health 2016, 13, S343–S366. [Google Scholar] [CrossRef] [Green Version]
- Health Behavior in School-Aged Children: WHO Collaborative Cross-National Survey/Study (HBSC) 2010–2011; WHO: Geneva, Switzerland, 2011.
- Ministry of Health. Prevention and Treatment of Obesity, A Subcommittee of the Health Behaviors Committee; Ministry of Health: Jerusalem, Israel, 2020.
- Content Source: Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion Control. Available online: https://www.cdc.gov/obesity/data/childhood.html (accessed on 14 December 2021).
- Ogden, C.; Carroll, M.D.; Curtin, L.R.; Lamb, M.M.; Flegal, K.M. About childhood obesity. JAMA 2010, 303, 242–249. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.; Hosking, J.; Woodward, A.; Witten, K.; MacMillan, A.; Field, A.; Baas, P.; Mackie, H. Systematic literature review of built environment effects on physical activity and active transport—An update and new findings on health equity. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 158. [Google Scholar] [CrossRef]
- Horodyska, K.; Boberska, M.; Knoll, N.; Scholz, U.; Radtke, T.; Liszewska, N.; Luszczynska, A. What matters, parental or child perceptions of physical activity facilities? A prospective parent-child study explaining physical activity and body fat among children. Psychol. Sport Exerc. 2018, 34, 39–46. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Waters, E.; de Silva-Sanigorski, A.; Hall, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, 7, CD001871. [Google Scholar] [CrossRef]
- Peirson, L.; Fitzpatrick-Lewis, D.; Morrison, K.; Ciliska, D.; Kenny, M.; Ali, M.U.; Raina, P. Prevention of overweight and obesity in children and youth: A systematic review and meta-analysis. CMAJ Open 2015, 3, E23–E33. [Google Scholar] [CrossRef] [Green Version]
- Visscher, T.L.S.; Kremers, S.P.J. How can we better prevent obesity in children? Curr. Obes. Rep. 2015, 4, 371–378. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Hermoso, A.; Cavero-Redondo, I.; Ramirez-Velez, R.; Ruiz, J.R.; Ortega, F.B.; Lee, D.C.; Martinez-Vizcaino, V. Muscular Strength as a Predictor of All-Cause Mortality in an Apparently Healthy Population: A Systematic Review and Meta-Analysis of Data From Approximately 2 Million Men and Women. Arch. Phys. Med. Rehabil. 2018, 99, 2100–2113. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Hermoso, A.; Esteban-Cornejo, I.; Olloquequi, J.; Ramirez-Velez, R. Cardi-orespiratory Fitness and Muscular Strength as Mediators of the Influence of Fatness on Academic Achievement. J. Pediatr. 2017, 187, 127–133. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjostrom, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karsten, L. It all used to be better? Different generations on continuity and change in urban children’s daily use of space. Child. Geogr. 2005, 3, 275–290. [Google Scholar] [CrossRef]
- Rideout, V.J.; Foehr, U.G.; Roberts, D.F. Generation M2: Media in the Lives of 8-to 18-Year-Olds; Henry J. Kaiser Family Foundation: Menlo Park, CA, USA, 2010. [Google Scholar]
- Davis, M.M.; Gance-Cleveland, B.; Hassink, S.; Johnson, R.; Paradis, G.; Resnicow, K. Recommendations for prevention of childhood obesity. Pediatrics 2007, 120 (Suppl. S4), 229–253. [Google Scholar] [CrossRef] [Green Version]
- Choi, D.J.; Kim, Y.S.; Um, N.R.; Kim, H.S. The Survey on Smartphone Overdependence [Internet]. In Annual Report; Report No.: NIA VI-RSE-C-18060; Ministry of Science and ICT, National Information Society Agency: Seoul, Korea, 2018; Available online: https://eng.nia.or.kr/site/nia_eng/ex/search/searchList.do (accessed on 14 December 2021).
- Park, J.H.; Park, M. Smartphone use patterns and problematic smartphone use among preschool children. PLoS ONE 2021, 16, e0244276. [Google Scholar] [CrossRef]
- Talbot, T.B. Virtual reality and interactive gaming technology for obese and diabetic children: Is military medical technology applicable? J. Diabetes Sci. Technol. 2011, 5, 234–238. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Sun, H. Effects of Active Videogame and Sports, Play, and Active Recrea-tion for Kids Physical Education on Children’s Health-Related Fitness and Enjoyment. Games Health J. 2017, 6, 312–318. [Google Scholar] [CrossRef]
- Valeriani, F.; Protano, C.; Marotta, D.; Liguori, G.; Romano Spica, V.; Valerio, G.; Vi-tali, M.; Galle, F. Exergames in Childhood Obesity Treatment: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4938. [Google Scholar] [CrossRef]
- Zeng, N.; Gao, Z. Exergaming and obesity in youth: Current perspectives. Int. J. Gen. Med. 2016, 9, 275–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, H.; Peng, W.; Lee, K.M. Promoting exercise self-efficacy with an exergame. J. Health Commun 2011, 16, 148–162. [Google Scholar] [CrossRef] [PubMed]
- Calvert, S.L.; Staiano, A.E.; Bond, B.J. Electronic gaming and the obesity crisis. New Dir. Child Adolesc. Dev. 2013, 2013, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Maddison, R.; Foley, L.; Ni Mhurchu, C.; Jiang, Y.; Jull, A.; Prapavessis, H.; Hohepa, M.; Rodgers, A. Effects of active video games on body composition: A randomized con-trolled trial. Am. J. Clin. Nutr. 2011, 94, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Trost, S.G.; Sundal, D.; Foster, G.D.; Lent, M.R.; Vojta, D. Effects of a pediatric weight management program with and without active video games: A randomized trial. JAMA Pediatrics 2014, 168, 407–413. [Google Scholar] [CrossRef] [Green Version]
- Gao, Z.; Chen, S. Are field-based exergames useful in preventing childhood obesity? A systematic review. Obes. Rev. 2014, 15, 676–691. [Google Scholar] [CrossRef]
- Christison, A.; Khan, H.A. Exergaming for Health: A Community-Based Pediatric Weight Management Program Using Active Video Gaming. Clin. Pediatr. 2012, 51, 382–388. [Google Scholar] [CrossRef]
- Guerra, P.H.; Nobre, M.R.; Silveira, J.A.; Taddei, J.A. The effect of school-based physical activity interventions on body mass index: A meta-analysis of randomized trials. Clinics 2013, 68, 1263–1273. [Google Scholar] [CrossRef]
- Metcalf, B.; Henley, W.; Wilkin, T. Republished research: Effectiveness of intervention on physical activity of children: Systematic review and meta-analysis of controlled trials with objectively measured outcomes (EarlyBird 54). Br. J. Sports Med. 2013, 47, e5888rep. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Zhang, T. Children’s Physical Activity Levels and Their Psychological Cor-relates in Interactive Dance Versus Aerobic Dance. Med. Sci. Sports Exerc. 2012, 44, 668. [Google Scholar]
- Staiano, A.E.; Calvert, S.L. Exergames for Physical Education Courses: Physical, Social, and Cognitive Benefits. Child Dev. Perspect. 2011, 5, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Wylie, C.G.; Coulton, P. Mobile exergaming. In Proceedings of the 2008 International Conference on Advances in Computer Entertainment Technology, Yokohama, Japan, 3–5 December 2008; pp. 338–341. [Google Scholar]
- Garde, A.; Umedaly, A.; Abulnaga, S.M.; Junker, A.; Chanoine, J.P.; Johnson, M.; An-sermino, J.M.; Dumont, G.A. Evaluation of a Novel Mobile Exergame in a School-Based Environment. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 186–192. [Google Scholar] [CrossRef]
- Macvean, A.; Robertson, J. iFitQuest: A school based study of a mobile location-aware exergame for adolescents. In Proceedings of the 14th International Conference on Human-Computer Interaction with Mobile Devices and Services, San Francisco, CA, USA, 21–24 September 2012; pp. 359–368. [Google Scholar] [CrossRef]
- Bochner, R.E.; Sorensen, K.M.; Belamarich, P.F. The impact of active video gaming on weight in youth: A meta-analysis. Clin. Pediatr. 2015, 54, 620–628. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, J.R.; Castro-Pinero, J.; Espana-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.M.; Jimenez-Pavon, D.; Chillon, P.; Girela-Rejon, M.J.; Mora, J.; et al. Field-based fitness assessment in young people: The ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef]
- Artero, E.G.; Espana-Romero, V.; Castro-Pinero, J.; Ruiz, J.; Jimenez-Pavon, D.; Apari-cio, V.; Gatto-Cardia, M.; Baena, P.; Vicente-Rodriguez, G.; Castillo, M.J.; et al. Criterion-related validity of field-based muscular fitness tests in youth. J. Sports Med. Phys. Fitness 2012, 52, 263–272. [Google Scholar] [PubMed]
- Thomas, E.; Petrigna, L.; Tabacchi, G.; Teixeira, E.; Pajaujiene, S.; Sturm, D.J.; Sahin, F.N.; Gomez-Lopez, M.; Pausic, J.; Paoli, A.; et al. Percentile values of the standing broad jump in children and adolescents aged 6-18 years old. Eur. J. Transl. Myol. 2020, 30, 9050. [Google Scholar] [CrossRef]
- Eather, N.; Morgan, P.J.; Lubans, D.R. Feasibility and preliminary efficacy of the Fit4Fun intervention for improving physical fitness in a sample of primary school chil-dren: A pilot study. Phys. Educ. Sport Pedagog. 2013, 18, 389–411. [Google Scholar] [CrossRef]
- Dirksen, T.; De Lussanet, M.H.; Zentgraf, K.; Slupinski, L.; Wagner, H. Increased Throwing Accuracy Improves Children’s Catching Performance in a Ball-Catching Task from the Movement Assessment Battery (MABC-2). Front. Psychol. 2016, 7, 1122. [Google Scholar] [CrossRef]
- Espana-Romero, V.; Artero, E.G.; Santaliestra-Pasias, A.M.; Gutierrez, A.; Castillo, M.J.; Ruiz, J.R. Hand span influences optimal grip span in boys and girls aged 6 to 12 years. J. Hand Surg. Am. 2008, 33, 378–384. [Google Scholar] [CrossRef]
- Leger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef]
- Ahler, T.; Bendiksen, M.; Krustrup, P.; Wedderkopp, N. Aerobic fitness testing in 6- to 9-year-old children: Reliability and validity of a modified Yo-Yo IR1 test and the Andersen test. Eur. J. Appl. Physiol. 2012, 112, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Benitez-Porres, J.; Lopez-Fernandez, I.; Raya, J.F.; Alvarez Carnero, S.; Alvero-Cruz, J.R.; Alvarez Carnero, E. Reliability and Validity of the PAQ-C Questionnaire to Assess Physical Activity in Children. J. Sch. Health 2016, 86, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Bervoets, L.; Van Noten, C.; Van Roosbroeck, S.; Hansen, D.; Van Hoorenbeeck, K.; Verheyen, E.; Van Hal, G.; Vankerckhoven, V. Reliability and Validity of the Dutch Physical Activity Questionnaires for Children (PAQ-C) and Adolescents (PAQ-A). Arch. Public Health 2014, 72, 47. [Google Scholar] [CrossRef] [Green Version]
- Murcia, J.A.; Gimeno, E.C.; Camacho, A.M. Measuring self-determination motivation in a physical fitness setting: Validation of the Behavioral Regulation in Exercise Question-naire-2 (BREQ-2) in a Spanish sample. J. Sports Med. Phys. Fit. 2007, 47, 366–374. [Google Scholar]
- Verloigne, M.; De Bourdeaudhuij, I.; Tanghe, A.; D’Hondt, E.; Theuwis, L.; Vansteen-kiste, M.; Deforche, B. Self-determined motivation towards physical activity in adolescents treated for obesity: An observational study. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 97. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.F.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B.D.; et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.; Frerichs, L.; Story, M.; Jones, J.; Gaskin, K.; Apple, A.; Skinner, A.; Arm-strong, S. An Integrated Clinic-Community Partnership for Child Obesity Treatment: A Randomized Pilot Trial. Pediatrics 2018, 141, e20171444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nemet, D.; Levi, L.; Pantanowitz, M.; Eliakim, A. A combined nutrition-al-behavioral-physical activity intervention for the treatment of childhood obesity–a 7-year summary. J. Pediatr. Endocrinol. Metab. 2014, 27, 445–451. [Google Scholar] [CrossRef]
- Valerio, G.; Maffeis, C.; Saggese, G.; Ambruzzi, M.A.; Balsamo, A.; Bellone, S.; Ber-gamini, M.; Bernasconi, S.; Bona, G.; Calcaterra, V.; et al. Diagnosis, treatment and preven-tion of pediatric obesity: Consensus position statement of the Italian Society for Pediatric Endocrinology and Diabetology and the Italian Society of Pediatrics. Ital. J. Pediatr. 2018, 44, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staiano, A.E.; Marker, A.M.; Beyl, R.A.; Hsia, D.S.; Katzmarzyk, P.T.; Newton, R.L. A randomized controlled trial of dance exergaming for exercise training in overweight and obese adolescent girls. Pediatr. Obes. 2017, 12, 120–128. [Google Scholar] [CrossRef] [Green Version]
- Staiano, A.E.; Beyl, R.A.; Guan, W.; Hendrick, C.A.; Hsia, D.S.; Newton, R.L., Jr. Home-based exergaming among children with overweight and obesity: A randomized clinical trial. Pediatr. Obes. 2018, 13, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.R.; Natvig, G.K.; Aadland, E.; Moe, V.F.; Kolotkin, R.L.; Anderssen, S.A.; Resaland, G.K. Associations between health-related quality of life, cardiorespiratory fitness, muscle strength, physical activity and waist circumference in 10-year-old children: The ASK study. Qual. Life Res. 2017, 26, 3421–3428. [Google Scholar] [CrossRef] [PubMed]
- Boreham, C.; Riddoch, C. The physical activity, fitness and health of children. J. Sports Sci. 2001, 19, 915–929. [Google Scholar] [CrossRef]
- Hills, A.P.; Andersen, L.B.; Byrne, N.M. Physical activity and obesity in children. Br. J. Sports Med. 2011, 45, 866–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voss, C.; Ogunleye, A.A.; Sandercock, G.R. Physical Activity Questionnaire for children and adolescents: English norms and cut-off points. Pediatr. Int. 2013, 55, 498–507. [Google Scholar] [CrossRef]
- Chen, S.R.; Lee, Y.J.; Chiu, H.W.; Jeng, C. Impact of physical activity on heart rate variability in children with type 1 diabetes. Childs Nerv. Syst. 2008, 24, 741–747. [Google Scholar] [CrossRef]
- Lewis, M.; Sutton, A. Understanding Exercise Behaviour: Examining the Interaction of Exercise Motivation and Personality in Predicting Exercise Frequency. J. Sport Behav. 2011, 34, 82–97. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68. [Google Scholar] [CrossRef]
- Hwang, J.; Kim, Y.H. Physical activity and its related motivational attributes in adolescents with different BMI. Int. J. Behav. Med. 2013, 20, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Abraham, A.A.; Calvert, S.L. Adolescent exergame play for weight loss and psychosocial improvement: A controlled physical activity intervention. Obesity 2013, 21, 598–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | APP (n = 32) | Control (n = 47) | ||||
|---|---|---|---|---|---|---|
| Pre Median (IQR) | Post Median (IQR) | Within-group p-value | Pre Median (IQR) | Post Median (IQR) | Within-group p-value * | |
| Height (cm) | 141.5 (18.50) | 142.0 (21.10) | <0.0001 | 147.0 (15.00) | 148.3 (14.40) | <0.0001 |
| Weight (kg) | 46.8 (18.20) | 47.5 (21.40) | NS | 55.5 (23.30) | 55.6 (23.50) | NS |
| BMI (kg/m²) | 25.4 (4.19) | 23.3 (5.24) | 0.009 | 26.0 (4.20) | 25.3 (4.44) | <0.0001 |
| BMI percentile | 99 (0.00) | 99 (2.00) | NS | 99 (0.00) | 99 (2.00) | NS |
| APP n = 32 | Control n = 44 | Between Group # | |||||
|---|---|---|---|---|---|---|---|
| Variable | Pre Median (IQR) | Post Median (IQR) | ∆ Median (IQR) | Pre Median (IQR) | Post Median (IQR) | ∆ Median (IQR) | ∆ p-value |
| Distance Yo-Yo Test (m) | 200.0 # (100.00) | 240 ** (110.0) | 60.0 (100.00) | 240.0 (160.00) | 240.0 (170.00) | 20.0 (160.00) | 0.038 |
| 4 × 10 m (sec) | 13.5 (3.60) | 12.6 ** (2.62) | −0.9 (1.13) | 14.1 (2.76) | 13.5 * (1.87) | 0.3 (1.44) | 0.010 |
| Wall Sit-Up (sec) | 24.2 (26.68) | 41.4 ** (26.61) | 14.9 (22.26) | 25.0 (19.35) | 29.3 (26.10) | 3.8 (17.04) | 0.050 |
| Standing Long Jump (cm) | 101.5 (21.00) | 100 (21.50) | −5.0 (21.50) | 111.0 (26.00) | 105.0 (21.00) | 4 (24.00) | 0.37 |
| Hand Grip (kg) | 12.5 # (11.75) | 13.8 * (12.75) | 1.0 (2.25) | 16.50 (7.00) | 17.0 (6.75) | 0.5 (3.00) | 0.40 |
| Hand Wall Toss Test (# catches) | 8 (8.00) | 12.5 ** (11.50) | 3.0 (7.50) | 7.0 (16.00) | 11.0 * (10.00) | 2.0 (5.00) | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kahana, R.; Kremer, S.; Dekel Dahari, M.; Kodesh, E. The Effect of Incorporating an Exergame Application in a Multidisciplinary Weight Management Program on Physical Activity and Fitness Indices in Children with Overweight and Obesity. Children 2022, 9, 18. https://0-doi-org.brum.beds.ac.uk/10.3390/children9010018
Kahana R, Kremer S, Dekel Dahari M, Kodesh E. The Effect of Incorporating an Exergame Application in a Multidisciplinary Weight Management Program on Physical Activity and Fitness Indices in Children with Overweight and Obesity. Children. 2022; 9(1):18. https://0-doi-org.brum.beds.ac.uk/10.3390/children9010018
Chicago/Turabian StyleKahana, Rotem, Shai Kremer, Merav Dekel Dahari, and Einat Kodesh. 2022. "The Effect of Incorporating an Exergame Application in a Multidisciplinary Weight Management Program on Physical Activity and Fitness Indices in Children with Overweight and Obesity" Children 9, no. 1: 18. https://0-doi-org.brum.beds.ac.uk/10.3390/children9010018