
Diagnostic Process for Autism Spectrum Disorder: A Meta-Analysis of Worldwide Clinical Practice Guidelines for the Initial Somatic Assessment
 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Literature Review
2.2. Quality Appraisal
2.3. Data Extraction
3. Results
3.1. Synthesis of Somatic Disorders Guidelines for Initial Somatic Assessment
3.1.1. Chromosome and Gene Abnormalities, Metabolic Diseases, and Mitochondrial Abnormalities
3.1.2. Neurological Diseases
3.1.3. Hearing Impairments and Visual Deficiencies
3.1.4. Sleep Disorders
3.1.5. Eating Disorders
3.1.6. Gastrointestinal Disorders
3.1.7. Endocrine Diseases
3.1.8. Auto-Immune Disorders
3.1.9. Toxins
3.1.10. General Health Issues
3.2. Synthesis of the Recommended Disciplines Involved
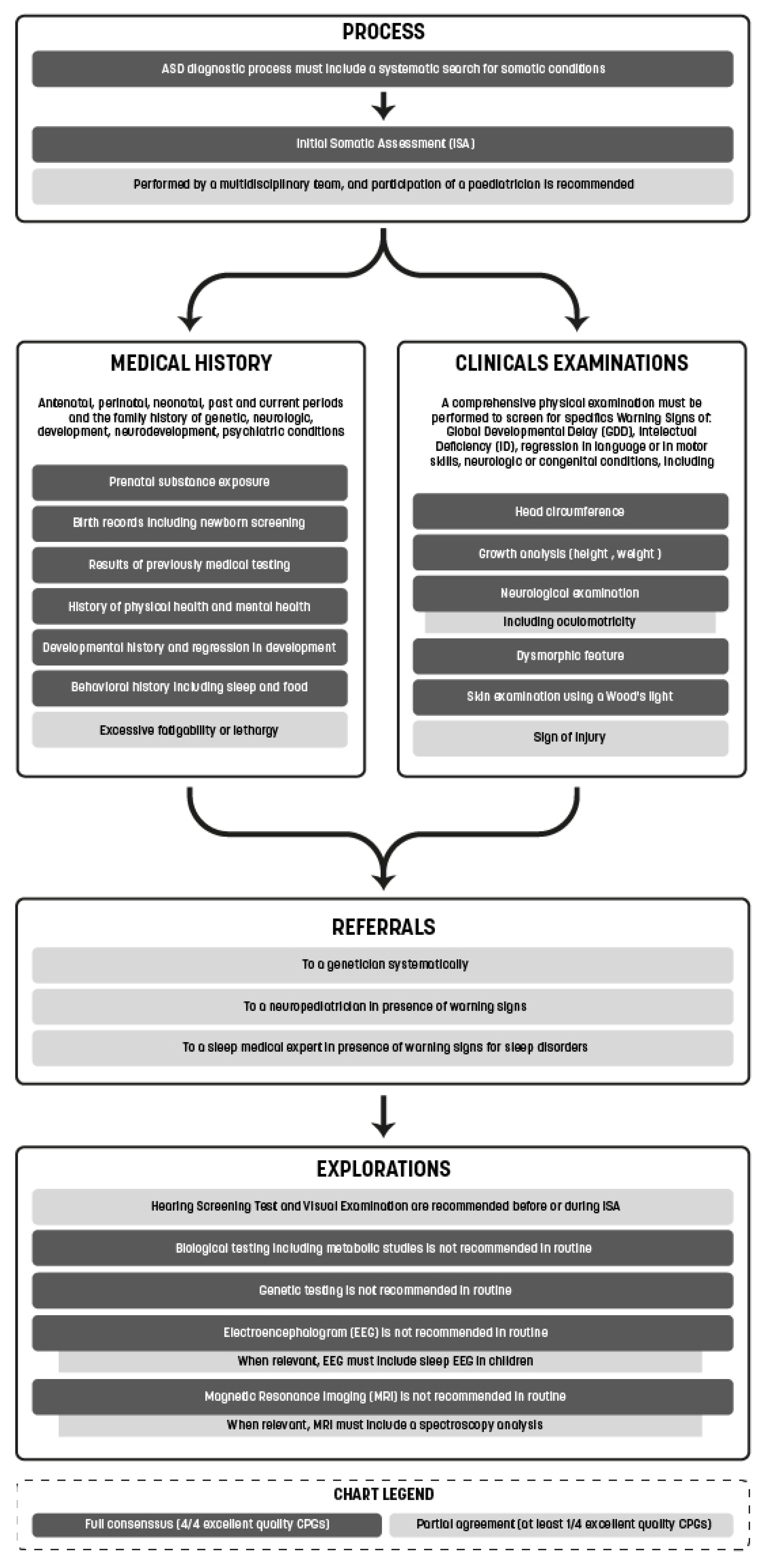
3.2.1. Medical Questioning and Investigations
3.2.2. Physical Examination
3.2.3. Warning Signs
3.2.4. Hearing Tests and Visual Examinations
3.2.5. Biological Testing including Metabolic Studies
3.2.6. Genetic Testing
3.2.7. Electroencephalogram
3.2.8. Magnetic Resonance Imaging
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- ICD-11—Mortality and Morbidity Statistics. Available online: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/437815624 (accessed on 23 January 2021).
- Lai, M.C.; Lombardo, M.V.; Baron-Cohen, S. Search strategy and selection criteria. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Tick, B.; Bolton, P.; Happé, F.; Rutter, M.; Rijsdijk, F. Heritability of autism spectrum disorders: A meta-analysis of twin studies. J. Child Psychol. Psychiatry 2016, 57, 585–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campisi, L.; Imran, N.; Nazeer, A.; Skokauskas, N.; Azeem, M.W. Autism spectrum disorder. Br. Med. Bull. 2018, 127, 91–100. [Google Scholar] [CrossRef] [Green Version]
- Maenner, M.J.; Shaw, K.A.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Esler, A.; Furnier, S.M.; Hallas, L.; Hall-Lande, J.; Hudson, A.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2018. MMWR. Surveill. Summ. 2021, 70, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Loomes, R.; Hull, L.; Mandy, W.P.L. What Is the Male-to-Female Ratio in Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 466–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haute Autorité de Santé. Trouble du Spectre de l’Autisme: Signes d’Alerte, Repérage, Diagnostic et Evaluation Chez l’Enfant et l’Adolescent; HAS, Service des Bonnes Pratiques Professionnelles: Saint-Denis La Plaine, France, 2018. [Google Scholar]
- National Institute for Health and Clinical Excellence. Autism Spectrum Disorder in under 19s: Recognition, Referral and Diagnosis. NICE, Clinical Guideline CG128, September 2011. Available online: http://nice.org.uk/guidance/cg128 (accessed on 13 July 2022).
- Lukmanji, S.; Manji, S.A.; Kadhim, S.; Sauro, K.M.; Wirrell, E.C.; Kwon, C.-S.; Jetté, N. The co-occurrence of epilepsy and autism: A systematic review. Epilepsy Behav. 2019, 98, 238–248. [Google Scholar] [CrossRef]
- Woolfenden, S.; Sarkozy, V.; Ridley, G.; Coorey, M.; Williams, K. A systematic review of two outcomes in autism spectrum disorder—Epilepsy and mortality. Dev. Med. Child Neurol. 2012, 54, 306–312. [Google Scholar] [CrossRef]
- Shavelle, R.M.; Strauss, D.J.; Pickett, J. Causes of death in autism. J. Autism. Dev. Disord. 2001, 31, 569–576. [Google Scholar] [CrossRef]
- Bilder, D.; Botts, E.L.; Smith, K.R.; Pimentel, R.; Farley, M.; Viskochil, J.; McMahon, W.M.; Block, H.; Ritvo, E.; Ritvo, R.-A.; et al. Excess Mortality and Causes of Death in Autism Spectrum Disorders: A Follow up of the 1980s Utah/UCLA Autism Epidemiologic Study. J. Autism Dev. Disord. 2013, 43, 1196–1204. [Google Scholar] [CrossRef] [Green Version]
- Prado, C. Le coût économique et social de l’autisme. Droit Déontologie Soin 2013, 13, 46–50. [Google Scholar] [CrossRef]
- Whitney, D.G.; Shapiro, D.N. National Prevalence of Pain Among Children and Adolescents With Autism Spectrum Disorders. JAMA Pediatr. 2019, 173, 1203–1205. [Google Scholar] [CrossRef] [PubMed]
- Baeza-Velasco, C.; Cohen, D.; Hamonet, C.; Vlamynck, E.; Diaz, L.; Cravero, C.; Cappe, E.; Guinchat, V. Autism, Joint Hypermobility-Related Disorders and Pain. Front. Psychiatry 2018, 9, 656. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Pivina, L.; Dadar, M.; Meguid, N.A.; Semenova, Y.; Anwar, M.; Chirumbolo, S. Gastrointestinal alterations in autism spectrum disorder: What do we know? Neurosci. Biobehav. Rev. 2020, 118, 111–120. [Google Scholar] [CrossRef] [PubMed]
- MTudor, E.; Walsh, C.E.; Mulder, E.C.; Lerner, M.D. Pain as a predictor of sleep problems in youth with autism spectrum disorders. Autism 2015, 19, 292–300. [Google Scholar] [CrossRef]
- Hirvikoski, T.; Mittendorfer-Rutz, E.; Boman, M.; Larsson, H.; Lichtenstein, P.; Bölte, S. Premature mortality in autism spectrum disorder. Br. J. Psychiatry 2016, 208, 232–238. [Google Scholar] [CrossRef] [Green Version]
- Hawkes, N. People with autism die 16 years earlier on average, says charity. BMJ 2016, 352, i1615. [Google Scholar] [CrossRef]
- Cashin, A.; Buckley, T.; Trollor, J.; Lennox, N. A scoping review of what is known of the physical health of adults with autism spectrum disorder. J. Intellect. Disabil. 2018, 22, 96–108. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US). Committee on Standards for Developing Trustworthy Clinical Practice Guidelines. In Clinical Practice Guidelines We Can Trust; National Academies Press: Washington, DC, USA, 2011. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK209539/ (accessed on 3 September 2022).
- Welcome to G-I-N—Guidelines International Network. Available online: http://www.g-i-n.net/ (accessed on 6 January 2018).
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. Can. Med. Assoc. J. 2010, 182, E839–E842. [Google Scholar] [CrossRef] [Green Version]
- Penner, M.; Anagnostou, E.; Andoni, L.Y.; Ungar, W.J. Systematic review of clinical guidance documents for autism spectrum disorder diagnostic assessment in select regions. Autism 2017, 22, 517–527. [Google Scholar] [CrossRef] [Green Version]
- Whitehouse, A.J.O.; Evans, K.; Eapen, V.; Wray, J. A National Guideline for the Assessment and Diagnosis of Autism Spectrum Disorders in Australia; Cooperative Research Centre for Living with Autism (Autism CRC): Brisbane, Australia, 2018; Available online: https://www.autismcrc.com.au/knowledge-centre/resource/national-guideline (accessed on 3 September 2022).
- Scottish Intercollegiate Guidelines Network. SIGN 145: Assessment, Diagnosis and Interventions for Autism Spectrum Disorders; SIGN, A National Clinical Guideline; SIGN: Edinburgh, Scotland, 2016; p. 145. Available online: http://www.sign.ac.uk (accessed on 12 January 2020).
- Whitehouse, A.; Evans, K.; Eapen, V.; Wray, J. A National Guideline for the Assessment and Diagnosis of Autism Spectrum Disorders in Australia—Administrative and Technical Report; Cooperative Research Centre for Living with Autism: Brisbane, Australia, 2018. [Google Scholar]
- Johnson, C.P.; Myers, S.M.; The Council on Children with Disabilities. Identification and Evaluation of Children with Autism Spectrum Disorders. Pediatrics 2007, 120, 1183–1215. [Google Scholar] [CrossRef]
- Nachshen, J.; Garcin, N.; Moxness, K.; Tremblay, Y.; Hutchinson, P.; Lachance, A.; Beaurivage, M.; Breitenbach, M.; Bryson, S.; Burack, J.; et al. Screening, Assessment, and Diagnosis of Autism Spectrum Disorders in Young Children: Canadian Best Practice Guidelines; Miriam Foundation: Montreal, QC, USA, 2008. [Google Scholar]
- Volkmar, F.; Siegel, M.; Woodbury-Smith, M.; King, B.; McCracken, J.; State, M. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Autism Spectrum Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 237–257. [Google Scholar] [CrossRef] [Green Version]
- Missouri Autism Guidelines Initiative. Autism Spectrum Disorders: Missouri Best Practice Guidelines for Screening, Diagnosis, and Assessment. 2010.
- University of Connecticut School of Medicine and Dentistry. Connecticut Guidelines for a Clinical Diagnosis of Autism Spectrum Disorder. Available online: http://digitalcommons.uconn.edu/pcare_articles/45 (accessed on 12 January 2020).
- Ministries of Health and Education. New Zealand Autism Spectrum Disorder Guideline, 2nd ed.; Ministry of Health: Wellington, New Zealand, 2016. Available online: http://www.health.govt.nz/autismspectrumdisorder (accessed on 12 January 2020).
- Hunter, J.; Rivero-Arias, O.; Angelov, A.; Kim, E.; Fotheringham, I.; Leal, J. Epidemiology of fragile X syndrome: A systematic review and meta-analysis. Am. J. Med. Genet. Part A 2014, 164, 1648–1658. [Google Scholar] [CrossRef]
- Kyle, S.M.; Vashi, N.; Justice, M.J. Rett syndrome: A neurological disorder with metabolic components. Open Biol. 2018, 8, 170216. [Google Scholar] [CrossRef] [Green Version]
- Kaur, S.; Christodoulou, J. MECP2 Disorders. In GeneReviews®; Adam, M.P., Everman, D.B., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK1497/ (accessed on 6 November 2022).
- Tatton-Brown, K.; Cole, T.R.; Rahman, N. Sotos Syndrome. In GeneReviews®; Adam, M.P., Everman, D.B., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK1479/ (accessed on 6 November 2022).
- Smith, A.C.; Boyd, K.E.; Brennan, C.; Charles, J.; Elsea, S.H.; Finucane, B.M.; Foster, R.; Gropman, A.; Girirajan, S.; Haas-Givler, B. Smith-Magenis Syndrome. In GeneReviews®; Adam, M.P., Everman, D.B., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK1310/ (accessed on 6 November 2022).
- Bahl, S.; Cordeiro, D.; MacNeil, L.; Schulze, A.; Mercimek-Andrews, S. Urine creatine metabolite panel as a screening test in neurodevelopmental disorders. Orphanet. J. Rare Dis. 2020, 15, 339. [Google Scholar] [CrossRef]
- DesRoches, C.-L.; Patel, J.; Wang, P.; Minassian, B.; Salomons, G.S.; Marshall, C.R.; Mercimek-Mahmutoglu, S. Estimated carrier frequency of creatine transporter deficiency in females in the general population using functional characterization of novel missense variants in the SLC6A8 gene. Gene 2015, 565, 187–191. [Google Scholar] [CrossRef]
- Mercimek-Mahmutoglu, S.; Pop, A.; Kanhai, W.; Ojeda, M.F.; Holwerda, U.; Smith, D.; Loeber, J.; Schielen, P.; Salomons, G. A pilot study to estimate incidence of guanidinoacetate methyltransferase deficiency in newborns by direct sequencing of the GAMT gene. Gene 2016, 575, 127–131. [Google Scholar] [CrossRef]
- Berg, A.T.; Plioplys, S. Epilepsy and autism: Is there a special relationship? Epilepsy Behav. 2012, 23, 193–198. [Google Scholar] [CrossRef] [Green Version]
- Houghton, R.; Liu, C.; Bolognani, F. Psychiatric Comorbidities and Psychotropic Medication Use in Autism: A Matched Cohort Study with ADHD and General Population Comparator Groups in the United Kingdom. Autism Res. 2018, 11, 1690–1700. [Google Scholar] [CrossRef]
- Camfield, C.S.; Camfield, P.R.; Gordon, K.; Wirrell, E.; Dooley, J.M. Incidence of Epilepsy in Childhood and Adolescence: A Population-Based Study in Nova Scotia from 1977 to 1985. Epilepsia 1996, 37, 19–23. [Google Scholar] [CrossRef]
- Sacco, R.; Gabriele, S.; Persico, A.M. Head circumference and brain size in autism spectrum disorder: A systematic review and meta-analysis. Psychiatry Res. 2015, 234, 239–251. [Google Scholar] [CrossRef]
- Schaefer, G.B.; Mendelsohn, N.J. Clinical genetics evaluation in identifying the etiology of autism spectrum disorders: 2013 guideline revisions. Genet. Med. 2013, 15, 399–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brian, J.A.; Zwaigenbaum, L.; Ip, A. Standards of diagnostic assessment for autism spectrum disorder. Paediatr. Child Health 2019, 24, 444–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bougeard, C.; Picarel-Blanchot, F.; Schmid, R.; Campbell, R.; Buitelaar, J. Prevalence of Autism Spectrum Disorder and Co-morbidities in Children and Adolescents: A Systematic Literature Review. Front. Psychiatry 2021, 12, 744709. [Google Scholar] [CrossRef] [PubMed]
- Elrod, M.G.; Nylund, C.M.; Susi, A.L.; Gorman, G.H.; Hisle-Gorman, E.; Rogers, D.J.; Erdie-Lalena, C. Prevalence of Diagnosed Sleep Disorders and Related Diagnostic and Surgical Procedures in Children with Autism Spectrum Disorders. J. Dev. Behav. Pediatr. 2016, 37, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Kinnell, H.G. Pica as a Feature of Autism. Br. J. Psychiatry 1985, 147, 80–82. [Google Scholar] [CrossRef]
- Mayes, S.D.; Zickgraf, H. Atypical eating behaviors in children and adolescents with autism, ADHD, other disorders, and typical development. Res. Autism Spectr. Disord. 2019, 64, 76–83. [Google Scholar] [CrossRef]
- Buie, T.; Campbell, D.B.; Fuchs, G.J., 3rd; Furuta, G.T.; Levy, J.; Vandewater, J.; Whitaker, A.H.; Atkins, D.; Bauman, M.L.; Beaudet, A.L.; et al. Evaluation, Diagnosis, and Treatment of Gastrointestinal Disorders in Individuals With ASDs: A Consensus Report. Pediatrics 2010, 125 (Suppl. 1), S1–S18. [Google Scholar] [CrossRef] [Green Version]
- New York State Department of Health and Bureau of Early Intervention. New York State Department of Health Clinical Practice Guideline on Assessment and Intervention Services for Young Children (Age 0–3) with Autism Spectrum Disorders (ASD): 2017; New York State Department of Health and Bureau of Early Intervention: New York, NY, USA, 2017. [Google Scholar]
- Hyman, S.L.; Levy, S.E.; Myers, S.M.; Council on Children with Disabilities, Section on Developmental and Behavioral Pediatrics. Identification, Evaluation, and Management of Children With Autism Spectrum Disorder. Pediatrics 2020, 145, e20193447. [Google Scholar] [CrossRef] [Green Version]
- Zerbo, O.; Leong, A.; Barcellos, L.; Bernal, P.; Fireman, B.; Croen, L.A. Immune mediated conditions in autism spectrum disorders. Brain, Behav. Immun. 2015, 46, 232–236. [Google Scholar] [CrossRef]
- Singapore Ministry of Health. Autism Spectrum Disorders in Pre-School Children. In AMS-MOH Clinical Practice Guidelines; Singapore Ministry of Health: Singapore, 2010. [Google Scholar]
- FDA. FDA Drug Safety Communication: FDA Approves Label Changes for Use of General Anesthetic and Sedation Drugs in Young Children. Available online: https://www.fda.gov/Drugs/DrugSafety/ucm554634.htm (accessed on 27 January 2018).




{kind=link}
{kind=link}
{kind=link}
| AGREE II Criteria | Quality Appraisal Used Criteria |
|---|---|
| Domain 1. Scope and Purpose | Domain 1. Scope and Purpose: all criteria |
| Domain 2. Stakeholder involvement | Domain 2. Stakeholder involvement: all criteria |
| Domain 3. Rigour of development | Domain 3. Rigour of development: all criteria except for the “updating procedure” criterion |
| Domain 4. Clarity of presentation | Not evaluated |
| Domain 5. Applicability | Not evaluated |
| Domain 6. Editorial independence | Domain 4. Editorial independence: all criteria |
| CPG | Domain 1 | Domain 2 | Domain 3 | Domain 4 | Overall | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Score | Rank | Score | Rank | Score | Rank | Score | Rank | Score | Rank | |
| MIR | 88.9 | 5 | 83.3 | 4 | 52.4 | 7 | 27.8 | 12 | 62.6 | 6 |
| SIN | 85.2 | 6 | 57.4 | 9 | 30.2 | 9 | 13.9 | 14 | 44.4 | 9 |
| MISS | 83.3 | 8 | 63 | 8 | 22.2 | 10 | 30.6 | 11 | 43.7 | 10 |
| NICE | 100 | 1 | 92.6 | 3 | 87.3 | 2 | 94.4 | 1 | 91.9 | 1 |
| ACMG | 72.2 | 10 | 40.7 | 12 | 11.9 | 13 | 55.6 | 6 | 35.6 | 12 |
| CONN | 57.4 | 14 | 57.4 | 9 | 14.3 | 12 | 19.4 | 13 | 32.2 | 14 |
| AACAP | 72.2 | 10 | 33.3 | 14 | 58.7 | 5 | 50 | 8 | 55.2 | 8 |
| NZ | 85.2 | 6 | 81.5 | 5 | 51.6 | 8 | 55.6 | 6 | 64.8 | 5 |
| SIGN | 98.2 | 2 | 94.4 | 1 | 84.1 | 3 | 91.7 | 3 | 90 | 3 |
| NY | 74.1 | 9 | 72.2 | 7 | 54 | 6 | 47.2 | 10 | 60.7 | 7 |
| CRC | 94.4 | 4 | 94.4 | 1 | 88.9 | 1 | 94.4 | 1 | 91.9 | 1 |
| HAS | 96.3 | 3 | 79.6 | 6 | 74.6 | 4 | 77.8 | 4 | 80.4 | 4 |
| CPS | 66.7 | 13 | 33.3 | 14 | 7.1 | 14 | 66.7 | 5 | 33.2 | 13 |
| AAP | 72.2 | 10 | 44.4 | 11 | 21.4 | 11 | 50 | 8 | 40 | 11 |
| Excellent quality | Good quality | Poor quality | ||||||||
| Chromosome and Gene Abnormalities |
|---|
| Tuberous sclerosis complex (TSC1-TSC2): all CPGs |
| Rett syndrome (MECP2): all CPGs |
| Fragile X syndrome: all CPGs |
| Neurofibromatosis: 8/14 |
| Down syndrome (trisomy 21): 7/14 |
| Prader-Willi syndrome, Angelman syndrome and Dup15q syndrome (15q11-q13): 7/14 |
| Phosphatase and tensin homolog (PTEN) gene mutation associated disorders (Cowden syndrome, Bannayan–Riley–Ruvalcaba syndrome): 7/14 |
| Williams–Beuren syndrome (7q11.23): 5/14 |
| Higher rates of Copy-number variations: 5/14 |
| Phelan–MacDermid syndrome or 22q13.3 deletion syndrome (SHANK3): 4/14 |
| Turner syndrome (45, X): 4/14 |
| Cornelia de Lange syndrome (5p13.1-Xp11.22-p11.21): 4/14 |
| Smith–Magenis syndrome (17p11.2): 4/14 |
| Möbius syndrome (13q12.2-q13): 4/14 |
| Muscular Dystrophy including Duchenne Muscular Dystrophy: 4/14 |
| 22q11.2 deletion syndrome (DiGeorge and Shprintzen syndromes): 4/14 |
| CHARGE syndrome (8q12.1): 3/14 |
| Sotos syndrome (5q35): 3/14 |
| Metabolic diseases |
| Untreated Phenylketonuria: 7/14 |
| Smith–Lemli–Opitz syndrome (3β-Hydroxycholesterol-7-reductase deficiency): 4/14 |
| Disorders of creatine transport or metabolism: 4/14 |
| Disorders of carnitine biosynthesis: 3/14 |
| Mucopolysaccharidosis including mucopolysaccharidosis III: 3/14 |
| Disorders of γ-aminobutyric acid metabolism: 2/14 |
| Phosphoribosylpyrophosphate synthetase superactivity 2/14 |
| Disorders associated with cerebral folate deficiency 2/14 |
| Homocystinuria: 2/14 |
| Warning Signs | Conditions That May Be Suspected | Referral, Further Examinations |
| GDD and ID, dysmorphic features, congenital abnormalities | Chromosome and gene abnormalities | Referral for clinical genetics evaluation; could require oriented genetic tests |
| Microcephaly | Rett syndrome | |
| Male gender with drooling, recurrent respiratory infections, hypotonic facies | ||
| Male gender | FXS | |
| Female gender with family history of X-linked compatible NDD, premature ovarian insufficiency, ataxia, or tremors | ||
| Macrocephaly (>2.5 SD) | PTEN gene mutation, FXS | |
| Macrocephaly and excessive growth | Sotos syndrome | |
| Seizures or symptoms suggesting sub-clinical seizures | Epilepsy, epileptic encephalopathy | Pediatric neurologist or neurologist referral; could require EEG |
| Language regression | Epilepsy, epileptic encephalopathy including Landau-Kleffner syndrome | |
| Abnormalities on neurological examination including head circumference abnormalities | Neurological diseases | Pediatric neurologist or neurologist referral; could require EEG, MRI |
| Skin pigmentation abnormalities | TSC, NF1 | Geneticist and pediatric neurologist or neurologist referral; could require genetic testing, EEG, MRI |
| Seizures, cyclic vomiting, lethargy, ataxia, hypotonia, dystonia, muscle weakness, dysmorphic features, skin abnormalities, poor growth, regression (particularly if associated fever, illnesses, or unusual odors), deafness, oculomotor abnormalities, metabolic acidosis, anemia, multi-organ system involvement, inadequate or absence of newborn screening | Metabolic and mitochondrial diseases | Pediatric neurologist or neurologist, specialists, geneticist referral; could require EEG, MRI, metabolic studies, genetic testing |
| Resistant sleep disorder, loud snoring, choking or periodic apnea during sleep | Obstructive sleep apnea, sleep disordered breathing | Pediatrician, otorhinolaryngologist, and sleep medicine services referral |
| Difficulties with sleep onset, night awakening, and parasomnias | Obstructive sleep apnea, restless legs syndrome, nocturnal seizures, medication side effects, circadian rhythm abnormalities | |
| Pica | Intoxications (e.g., lead poisoning) | Biological testing |
| Behavioural manifestations | General health issues, pain | Pediatrician or general practitioner referral |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dauchez, T.; Camelot, G.; Levy, C.; Rajerison, T.; Briot, K.; Pizano, A.; Geoffray, M.-M.; Landrieu, L.; Bouvard, M.; Amestoy, A. Diagnostic Process for Autism Spectrum Disorder: A Meta-Analysis of Worldwide Clinical Practice Guidelines for the Initial Somatic Assessment. Children 2022, 9, 1886. https://0-doi-org.brum.beds.ac.uk/10.3390/children9121886
Dauchez T, Camelot G, Levy C, Rajerison T, Briot K, Pizano A, Geoffray M-M, Landrieu L, Bouvard M, Amestoy A. Diagnostic Process for Autism Spectrum Disorder: A Meta-Analysis of Worldwide Clinical Practice Guidelines for the Initial Somatic Assessment. Children. 2022; 9(12):1886. https://0-doi-org.brum.beds.ac.uk/10.3390/children9121886
Chicago/Turabian StyleDauchez, Tom, Guillaume Camelot, Charlotte Levy, Toky Rajerison, Kellen Briot, Adrien Pizano, Marie-Maude Geoffray, Loic Landrieu, Manuel Bouvard, and Anouck Amestoy. 2022. "Diagnostic Process for Autism Spectrum Disorder: A Meta-Analysis of Worldwide Clinical Practice Guidelines for the Initial Somatic Assessment" Children 9, no. 12: 1886. https://0-doi-org.brum.beds.ac.uk/10.3390/children9121886