
Obsessive-Compulsive Disorder in PANS/PANDAS in Children: In Search of a Qualified Treatment—A Systematic Review and Metanalysis

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Data Extraction and Outcomes
2.1.1. Electronic Database Search
2.1.2. Statistical Analysis
3. Results
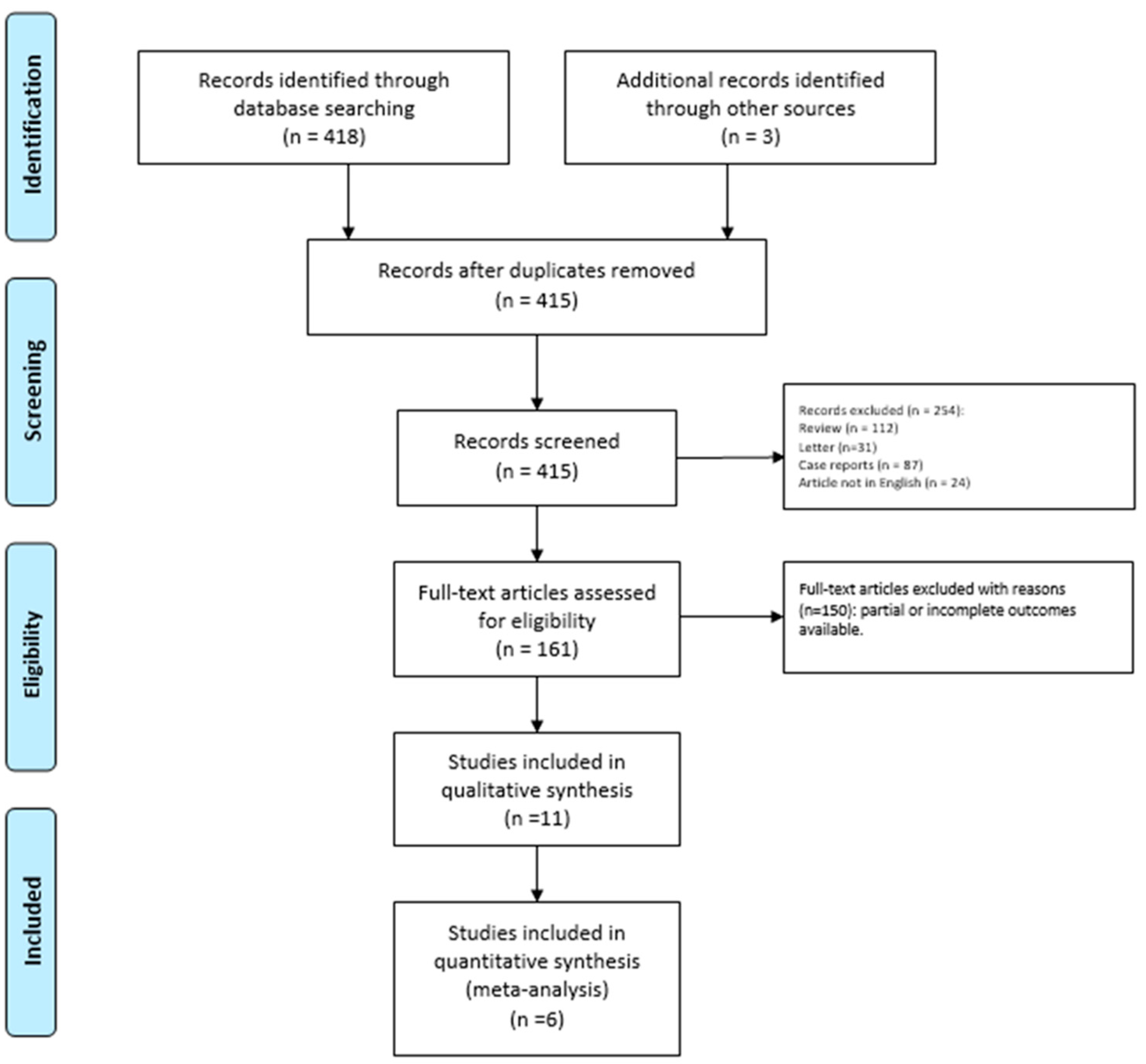
3.1. Retrieving Researches
3.2. Patients Features
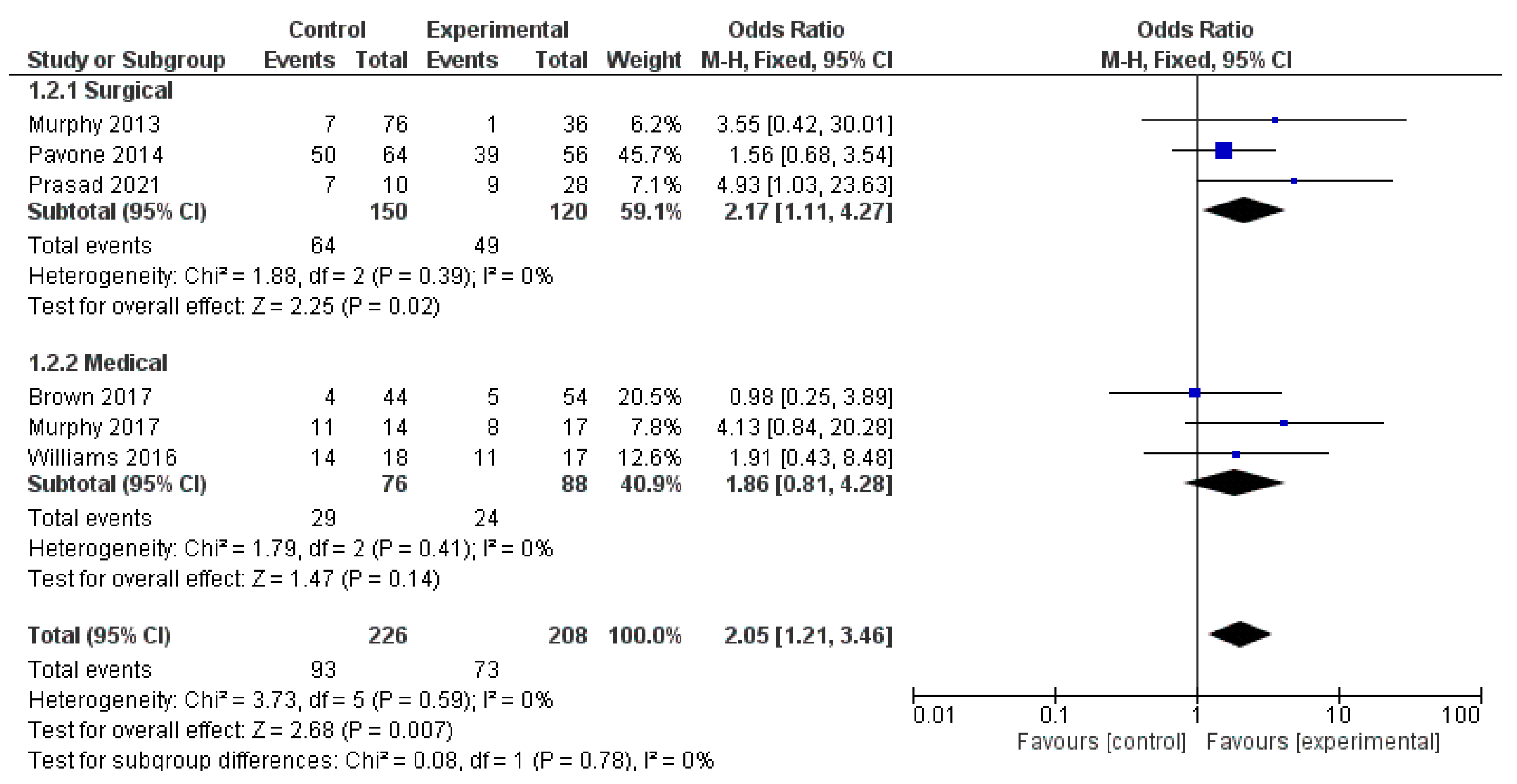
4. Surgical Treatment
5. Medical Treatment
6. Discussion
Study Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swedo, S.E.; Leonard, H.L.; Garvey, M.; Mittleman, B.; Allen, A.J.; Perlmutter, S.; Lougee, L.; Dow, S.; Zamkoff, J.; Dubbert, B.K. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: Clinical description of the first 50 cases. Am. J. Psychiatry 1998, 155, 264–271. [Google Scholar] [CrossRef]
- Swedo, S.E.; Leckman, J.F.; Rose, N.R. From Research Subgroup to Clinical Syndrome: Modifying the PANDAS Criteria to Describe PANS (Pediatric Acute-onset Neuropsychiatric Syndrome). Pediatr. Ther. 2012, 2, 113. [Google Scholar] [CrossRef]
- Chang, K.; Frankovich, J.; Cooperstock, M.; Cunningham, M.W.; Latimer, M.E.; Murphy, T.K.; Pasternack, M.; Thienemann, M.; Williams, K.; Walter, J.; et al. Clinical Evaluation of Youth with Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS): Recommendations from the 2013 PANS Consensus Conference. J. Child Adolesc. Psychopharmacol. 2015, 25, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Pavone, P.; Ceccarelli, M.; Marino, S.; Caruso, D.; Falsaperla, R.; Berretta, M.; Rullo, E.V.; Nunnari, G. SARS-CoV-2 related paediatric acute-onset neuropsychiatric syndrome. Lancet Child Adolesc. Heal. 2021, 5, e19–e21. [Google Scholar] [CrossRef]
- Thienemann, M.; Murphy, T.; Leckman, J.; Shaw, R.; Williams, K.; Kapphahn, C.; Frankovich, J.; Geller, D.; Bernstein, G.; Chang, K.; et al. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part I-Psychiatric and Behavioral Interventions. J. Child Adolesc. Psychopharmacol. 2017, 27, 566–573. [Google Scholar] [CrossRef]
- Ercan, T.E.; Ercan, G.; Severge, B.; Arpaozu, M.; Karasu, G. Mycoplasma pneumoniae Infection and Obsessive-Compulsive Disease: A Case Report. J. Child Neurol. 2008, 23, 338–340. [Google Scholar] [CrossRef]
- Caruso, J.M.; Tung, G.A.; Gascon, G.G.; Rogg, J.; Davis, L.; Brown, W.D. Persistent Preceding Focal Neurologic Deficits in Children With Chronic Epstein-Barr Virus Encephalitis. J. Child Neurol. 2000, 15, 791–796. [Google Scholar] [CrossRef]
- Fallon, B.A.; Kochevar, J.M.; Gaito, A.; Nields, J.A. The underdiagnosis of neuropsychiatric Lyme disease in children and adults. Psychiatr. Clin. N. Am. 1998, 21, 693–703. [Google Scholar] [CrossRef]
- Gamucci, A.; Uccella, S.; Sciarretta, L.; D’Apruzzo, M.; Calevo, M.G.; Mancardi, M.M.; Veneselli, E.; De Grandis, E. PANDAS and PANS: Clinical, Neuropsychological, and Biological Characterization of a Monocentric Series of Patients and Proposal for a Diagnostic Protocol. J. Child Adolesc. Psychopharmacol. 2019, 29, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Sigra, S.; Hesselmark, E.; Bejerot, S. Treatment of PANDAS and PANS: A systematic review. Neurosci. Biobehav. Rev. 2018, 86, 51–65. [Google Scholar] [CrossRef]
- Wilbur, C.; Bitnun, A.; Kronenberg, S.; Laxer, R.M.; Levy, D.M.; Logan, W.J.; Shouldice, M.; Yeh, E.A. PANDAS/PANS in childhood: Controversies and evidence. Paediatr. Child Heal. 2018, 24, 85–91. [Google Scholar] [CrossRef]
- Tipton, P.W. Searching for tics. Neurol. Neurochir. Polska 2019, 53, 315–316. [Google Scholar] [CrossRef]
- Pavone, P.; Rapisarda, V.; Serra, A.; Nicita, F.; Spalice, A.; Parano, E.; Rizzo, R.; Maiolino, L.; Di Mauro, P.; Vitaliti, G.; et al. Pediatric Autoimmune Neuropsychiatry Disorder Associated with Group a Streptococcal Infection: The Role of Surgical Treatment. Int. J. Immunopathol. Pharmacol. 2014, 27, 371–378. [Google Scholar] [CrossRef]
- Brown, K.D.; Farmer, C.; Freeman, G.M.; Spartz, E.; Farhadian, B.; Thienemann, M.; Frankovich, J. Effect of Early and Prophylactic Nonsteroidal Anti-Inflammatory Drugs on Flare Duration in Pediatric Acute-Onset Neuropsychiatric Syndrome: An Observational Study of Patients Followed by an Academic Community-Based Pediatric Acute-Onset Neuropsychiatric Syndrome Clinic. J. Child Adolesc. Psychopharmacol. 2017, 27, 619–628. [Google Scholar] [CrossRef]
- Snider, L.A.; Lougee, L.; Slattery, M.; Grant, P.; Swedo, S.E. Antibiotic prophylaxis with azithromycin or penicillin for childhood-onset neuropsychiatric disorders. Biol. Psychiatry 2005, 57, 788–792. [Google Scholar] [CrossRef]
- Murphy, T.K.; Brennan, E.M.; Johnco, C.; Parker-Athill, E.C.; Miladinovic, B.; Storch, E.A.; Lewin, A.B. A Double-Blind Randomized Placebo-Controlled Pilot Study of Azithromycin in Youth with Acute-Onset Obsessive–Compulsive Disorder. J. Child Adolesc. Psychopharmacol. 2017, 27, 640–651. [Google Scholar] [CrossRef]
- Spartz, E.J.; Freeman, G.M., Jr.; Brown, K.; Farhadian, B.; Thienemann, M.; Frankovich, J. Course of Neuropsychiatric Symptoms After Introduction and Removal of Nonsteroidal Anti-Inflammatory Drugs: A Pediatric Observational Study. J Child Adolesc. Psychopharmacol. 2017, 27, 652–659. [Google Scholar] [CrossRef]
- Brown, K.; Farmer, C.; Farhadian, B.; Hernandez, J.; Thienemann, M.; Frankovich, J. Pediatric Acute-Onset Neuropsychiatric Syndrome Response to Oral Corticosteroid Bursts: An Observational Study of Patients in an Academic Community-Based PANS Clinic. J. Child Adolesc. Psychopharmacol. 2017, 27, 629–639. [Google Scholar] [CrossRef]
- Williams, K.A.; Swedo, S.E.; Farmer, C.; Grantz, H.; Grant, P.J.; D’Souza, P.; Hommer, R.; Katsovich, L.; King, R.A.; Leckman, J.F. Randomized, Controlled Trial of Intravenous Immunoglobulin for Pediatric Autoimmune Neuropsychiatric Disorders Associated With Streptococcal Infections. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 860–867.e2. [Google Scholar] [CrossRef]
- Hesselmark, E.; Bejerot, S. Patient Satisfaction and Treatments Offered to Swedish Patients with Suspected Pediatric Acute-Onset Neuropsychiatric Syndrome and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections. J. Child Adolesc. Psychopharmacol. 2019, 29, 634–641. [Google Scholar] [CrossRef] [Green Version]
- Murphy, M.L.; Pichichero, M.E. Prospective Identification and Treatment of Children With Pediatric Autoimmune Neuropsychiatric Disorder Associated With Group A Streptococcal Infection (PANDAS). Arch. Pediatr. Adolesc. Med. 2002, 156, 356–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demesh, D.; Virbalas, J.M.; Bent, J.P. The Role of Tonsillectomy in the Treatment of Pediatric Autoimmune Neuropsychiatric Disorders Associated With Streptococcal Infections (PANDAS). JAMA Otolaryngol. Neck Surg. 2015, 141, 272–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, N.; Johng, S.; Powell, D.; Williams, M.; Latimer, E.; Harley, E. Role of tonsillectomy and adenoidectomy in parental satisfaction of treatments for PANDAS. Am. J. Otolaryngol. 2021, 42, 102963. [Google Scholar] [CrossRef] [PubMed]
- Perlmutter, S.J.; Leitman, S.F.; Garvey, M.A.; Hamburger, S.; Feldman, E.; Leonard, H.L.; Swedo, S.E. Therapeutic plasma exchange and intravenous immunoglobulin for obsessive-compulsive disorder and tic disorders in childhood. Lancet 1999, 354, 1153–1158. [Google Scholar] [CrossRef]
- Storch, E.A.; Murphy, T.K.; Geffken, G.R.; Mann, G.; Adkins, J.; Merlo, L.J.; Duke, D.; Munson, M.; Swaine, Z.; Goodman, W.K. Cognitive-Behavioral Therapy for PANDAS-Related Obsessive-Compulsive Disorder: Findings From a Preliminary Waitlist Controlled Open Trial. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1171–1178. [Google Scholar] [CrossRef] [Green Version]
- Nadeau, J.M.; Jordan, C.; Selles, R.R.; Wu, M.S.; King, M.A.; Patel, P.D.; Hanks, C.E.; Arnold, E.B.; Lewin, A.B.; Murphy, T.K.; et al. A Pilot Trial of Cognitive-Behavioral Therapy Augmentation of Antibiotic Treatment in Youth with Pediatric Acute-Onset Neuropsychiatric Syndrome-Related Obsessive-Compulsive Disorder. J. Child Adolesc. Psychopharmacol. 2015, 25, 337–343. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Riva, J.J.; Malik, K.M.; Burnie, S.J.; Endicott, A.R.; Busse, J. What is your research question? An introduction to the PICOT format for clinicians. J. Can. Chiropr. Assoc. 2012, 56, 167–171. [Google Scholar]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. Rev. Man Joanna Briggs Inst. 2017. [Google Scholar] [CrossRef]
- Zhou, Y.; Dendukuri, N. Statistics for quantifying heterogeneity in univariate and bivariate meta-analyses of binary data: The case of meta-analyses of diagnostic accuracy. Stat. Med. 2014, 33, 2701–2717. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.K.; Lewin, A.B.; Parker-Athill, E.C.; Storch, E.A.; Mutch, P.J. Tonsillectomies and Adenoidectomies Do Not Prevent the Onset of Pediatric Autoimmune Neuropsychiatric Disorder Associated With Group A Streptococcus. Pediatr. Infect. Dis. J. 2013, 32, 834–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farhood, Z.; Ong, A.A.; Discolo, C.M. PANDAS: A systematic review oftreatment options. Int. J. Pediatr Otorhinolaryngol. 2016, 89, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Kirvan, C.A.; Swedo, S.E.; Snider, L.A.; Cunningham, M.W. Antibody-mediated neuronal cell signaling in behavior and movement disorders. J. Neuroimmunol. 2006, 179, 173–179. [Google Scholar] [CrossRef]
- Kirvan, C.A.; Cox, C.; Swedo, S.E.; Cunningham, M. Tubulin Is a Neuronal Target of Autoantibodies in Sydenham’s Chorea. J. Immunol. 2007, 178, 7412–7421. [Google Scholar] [CrossRef]
- Hallett, J.J.; Harling-Berg, C.J.; Knopf, P.M.; Stopa, E.G.; Kiessling, L.S. Anti-striatal antibodies in Tourette syndrome cause neuronal dysfunction. J. Neuroimmunol. 2000, 111, 195–202. [Google Scholar] [CrossRef]
- Dileepan, T.; Smith, E.; Knowland, D.; Hsu, M.; Platt, M.; Bittner-Eddy, P.; Cohen, B.; Southern, P.; Latimer, E.; Harley, E.; et al. Group A Streptococcus intranasal infection promotes CNS infiltration by streptococcal-specific Th17 cells. J. Clin. Investig. 2015, 126, 303–317. [Google Scholar] [CrossRef] [Green Version]
- Latimer, M.E.; L’Etoile, N.; Seidlitz, J.; Swedo, S.E. Therapeutic Plasma Apheresis as a Treatment for 35 Severely Ill Children and Adolescents with Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections. J. Child Adolesc. Psychopharmacol. 2015, 25, 70–75. [Google Scholar] [CrossRef] [Green Version]
- Jonasson, G.; Wilkinson, S.R. Prednisolone-induced obsessive-compulsive behavior in a child. Tidsskr. Den Nor. Legeforen. 1993, 113, 3162–3163. [Google Scholar]
- Blankenship, P.; Kurek, K. Azithromycin Prophylaxis in an AdolescentWithPANDAS. J. Pediatr. Pharmacol. Ther. 2020, 25, 6163. [Google Scholar] [CrossRef]
- Rajgor, A.D.; Hakim, N.A.; Ali, S.; Darr, A. Paediatric Autoimmune Neuropsychiatric Disorder Associated with Group A Beta-Haemolytic Streptococcal Infection: An Indication for Tonsillectomy? A Review of the Literature. Int. J. Otolaryngol. 2018, 2018, 2681304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocuzza, S.; Marino, S.; Gulino, A.; Pustorino, E.; Murabito, P.; Maniaci, A.; Sabino, L.; Taibi, R.; Di Luca, M.; Falsaperla, R.; et al. ENT involvement and orobuccal movements’ disorders in Pandas patients: As-sessment and rehabilitations tools. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 4110–4117. [Google Scholar] [CrossRef] [PubMed]
- Calaprice, D.; Tona, J.; Murphy, T.K. Treatment of Pediatric Acute-Onset Neuropsychiatric Disorder in a Large Survey Population. J. Child Adolesc. Psychopharmacol. 2018, 28, 92–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgical | |||||||
|---|---|---|---|---|---|---|---|
| Authors, Year, Reference | Study Design | Patients | Age (Mean ± SD/Range) | Gender | Treatment | OCD Treatment Group | OCD Control Group |
| Murphy et al., 2013 [32] | Prospective controlled study | 43 PANDAS vs. 69 Healthy | 9.18 ± 2.38 | 68M vs. 44F | 36 Surgery vs. 76 N-Surgery | 35/36 (OCD) | 69/76 (OCD) |
| Pavone et al., 2014 [13] | Prospective study controlled | 120 PANDAS | 11.05 ± 1.2 | 63M vs. 57F | 56 Surgery vs. 64 N-Surgery | 17/56 (OCD) | 14/64 (OCD) |
| Prasad et al., 2021 [20] | Retrospective study controlled | 60 PANDAS | - | - | 28 Surgery vs. 10 N-Surgery | 19/28 (OCD) | 3/10 (OCD) |
| Demesh et al., 2015 [22] | Retrospective study controlled | 10 PANDAS | 6.5 | 8 M vs. 2 F | 9 Surgery & N-Surgery (Antibiotics) vs. 1 N-Surgery | 9/9 (OCD) | 5/10 (OCD) |
| NonSurgical | |||||||
| Murphy et al., 2017 [16] | Prospective randomized controlled study | 31 | 8.26 ± 2.78 | 20M vs. 11 F | 17 Azithromycin vs. 14 Placebo | 9/17 (OCD) | 3/14 (OCD) |
| Snider et al., 2005 [15] | Prospective randomized controlled study | 23 | 7.9 ± 1.3 | 15 M vs. 8F | 11 Penicillin vs. 12 Azithromycin | 6/11 (OCD) | 11/12 (OCD) |
| Spartz et al., 2017 [17] | Retrospective study | 77 | 8.3 ± 3.6 | 42 M vs. 35 F | 77 NSAID | 32/77 (OCD) | - |
| Hesselmark et al., 2019 [20] | Retrospective controlled study | 53 | 7.9 (1–20) | 33 M vs. 20 F | 46 Antibiotics vs. 17 IVIG | 19/46 (OCD) | 12/17 (OCD) |
| Brown et al., 2017 [14] | Retrospective controlled study | 95 | 7.8 ± 3.8 Treatment vs. 8.6 ± 3.2 Placebo | - | 54 Corticosteroids vs. 44 Placebo | 49/54 (OCD) | 40/44 (OCD) |
| Murphy et al., 2002 [21] | Prospective controlled study | 12 | 7 (range 5.4–10.11) | 7 M vs. 5 F | 5 Penicillin vs. 1 Amoxicillina/Clavulanic vs. 6 Cephalosporin | 6/12 (OCD) | - |
| Williams et al., 2016 [19] | Prospective randomized controlled study | 35 | placebo 9.61 ± 2.32 IVIG 8.99 ± 2.37 | 23 M vs. 12 F | 17 IVIG vs. 18 Placebo | 6/17 (OCD) | 4/18 (OCD) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cocuzza, S.; Maniaci, A.; La Mantia, I.; Nocera, F.; Caruso, D.; Caruso, S.; Iannella, G.; Vicini, C.; Privitera, E.; Lechien, J.R.; et al. Obsessive-Compulsive Disorder in PANS/PANDAS in Children: In Search of a Qualified Treatment—A Systematic Review and Metanalysis. Children 2022, 9, 155. https://0-doi-org.brum.beds.ac.uk/10.3390/children9020155
Cocuzza S, Maniaci A, La Mantia I, Nocera F, Caruso D, Caruso S, Iannella G, Vicini C, Privitera E, Lechien JR, et al. Obsessive-Compulsive Disorder in PANS/PANDAS in Children: In Search of a Qualified Treatment—A Systematic Review and Metanalysis. Children. 2022; 9(2):155. https://0-doi-org.brum.beds.ac.uk/10.3390/children9020155
Chicago/Turabian StyleCocuzza, Salvatore, Antonino Maniaci, Ignazio La Mantia, Francesco Nocera, Daniela Caruso, Sebastiano Caruso, Giannicola Iannella, Claudio Vicini, Elio Privitera, Jerome Rene Lechien, and et al. 2022. "Obsessive-Compulsive Disorder in PANS/PANDAS in Children: In Search of a Qualified Treatment—A Systematic Review and Metanalysis" Children 9, no. 2: 155. https://0-doi-org.brum.beds.ac.uk/10.3390/children9020155