
Heterogeneous Condition of Asthmatic Children Patients: A Narrative Review

 , , and
, , and 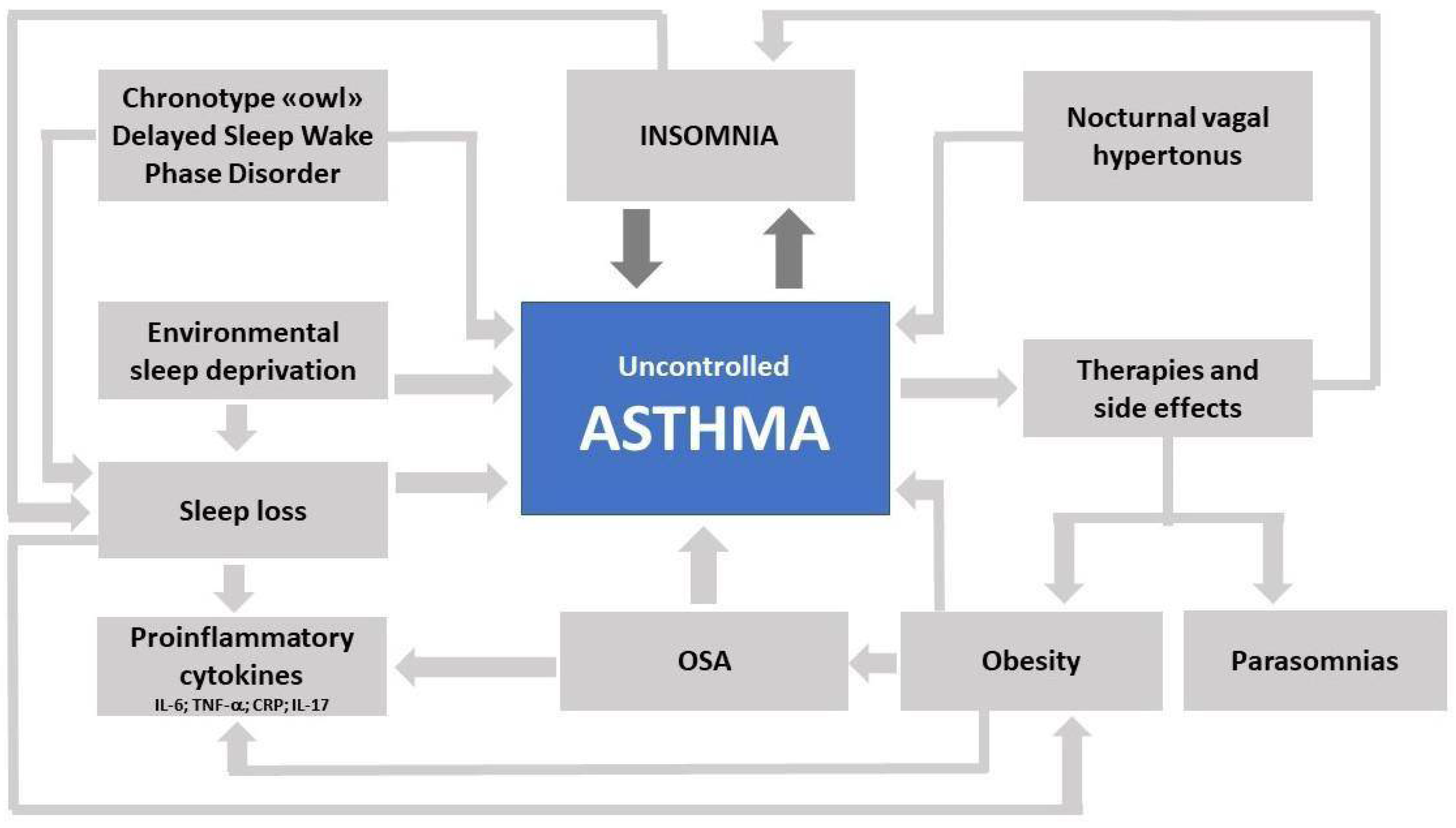{kind=link}
Abstract
:1. Introduction
Overview on Pediatric Asthma
2. Diagnostic Tools
Biomarker for Diagnosis and Follow-Up
3. Transitional Care
4. Specific Current Challenges
5. Preventive Strategies
5.1. Preventive Allergy Immunotherapy
5.2. Microbiome and Airway Inflammation
6. Therapeutic Approach to Asthma and Severe Asthma in Childhood and Adolescence
7. Adolescents, Asthma, and Sleep Disorders
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Caruso, C.; Colantuono, S.; Nicoletti, A.; Arasi, S.; Firinu, D.; Gasbarrini, A.; Coppola, A.; Di Michele, L. Metabolomics, Microbiota, and In Vivo and In Vitro Biomarkers in Type 2 Severe Asthma: A Perspective Review. Metabolites 2021, 11, 647. [Google Scholar] [CrossRef] [PubMed]
- Caruso, C.; Colantuono, S.; Tolusso, B.; Di Mario, C.; Pentassuglia, A.; Rumi, G.; Gremese, E.; Romano, A.; Gasbarrini, A. Basophil activation and serum IL-5 levels as possible monitor biomarkers in severe eosinophilic asthma patients treated with anti-IL-5 drugs. Allergy 2021, 76, 1569–1571. [Google Scholar] [CrossRef] [PubMed]
- Rusconi, F.; Fernandes, R.M.; Pijnenburg, M.W.H.; Grigg, J. The Severe Paediatric Asthma Collaborative in Europe (SPACE) ERS Clinical Research Collaboration: Enhancing participation of children with asthma in therapeutic trials of new biologics and receptor blockers. Eur. Respir. J. 2018, 52, 1801665. [Google Scholar] [CrossRef] [PubMed]
- Kolmert, J.; Gómez, C.; Balgoma, D.; Sjödin, M.; Bood, J.; Konradsen, J.R.; Ericsson, M.; Thörngren, J.-O.; James, A.; Mikus, M.; et al. Urinary Leukotriene E4 and Prostaglandin D2 Metabolites Increase in Adult and Childhood Severe Asthma Characterized by Type 2 Inflammation. A Clinical Observational Study. Am. J. Respir. Crit. Care Med. 2021, 203, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Nejman-Gryz, P.; Górska, K.; Krenke, K.; Peradzyńska, J.; Paplińska-Goryca, M.; Kulus, M.; Krenke, R. Periostin concentration in exhaled breath condensate in children with mild asthma. J. Asthma 2021, 58, 60–68. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Scioscia, G.; Lacedonia, D.; Soccio, P.; Lepore, G.; Saetta, M.; Barbaro, M.P.F.; Barnes, P.J. Looking for Airways Periostin in Severe Asthma: Could It Be Useful for Clustering Type 2 Endotype? Chest 2018, 154, 1083–1090. [Google Scholar] [CrossRef]
- Vezir, E.; Civelek, E.; Misirlioglu, E.D.; Toyran, M.; Capanoglu, M.; Karakus, E.; Kahraman, T.; Ozguner, M.; Demirel, F.; Gursel, I.; et al. Effects of Obesity on Airway and Systemic Inflammation in Asthmatic Children. Int. Arch. Allergy Immunol. 2021, 182, 679–689. [Google Scholar] [CrossRef]
- Shah, S.N.; Grunwell, J.R.; Mohammad, A.F.; Stephenson, S.T.; Lee, G.B.; Vickery, B.P.; Fitzpatrick, A.M. Performance of Eosinophil Cationic Protein as a Biomarker in Asthmatic Children. J. Allergy Clin. Immunol. Pract. 2021, 9, 2761–2769.e2. [Google Scholar] [CrossRef]
- Roberts, G.; Vazquez-Ortiz, M.; Knibb, R.; Khaleva, E.; Alviani, C.; Angier, E.; Blumchen, K.; Comberiati, P.; Duca, B.; DunnGalvin, A.; et al. EAACI Guidelines on the effective transition of adolescents and young adults with allergy and asthma. Allergy 2020, 75, 2734–2752. [Google Scholar] [CrossRef]
- Khaleva, E.; Knibb, R.; DunnGalvin, A.; Vazquez-Ortiz, M.; Comberiati, P.; Alviani, C.; Garriga-Baraut, T.; Gowland, M.H.; Gore, C.; Angier, E.; et al. Perceptions of adolescents and young adults with allergy and/or asthma and their parents on EAACI guideline recommendations about transitional care: A European survey. Allergy 2021, 1–11. [Google Scholar] [CrossRef]
- Center for Disease Control. National Center for Environmental Health: Climate Effects on Health. 2021. Available online: http://www.cdc.gov/climateandhealth/effects/default.htm (accessed on 10 February 2022).
- Environmental Protection Agency. Climate Change. 2021. Available online: http://www.epa.gov/climatechange/basics/ (accessed on 10 February 2022).
- Amato, G.; Cecchi, L.; Amato, M.; Annesi-Maesano, I. Climate change and respiratory diseases. Eur. Respir. Rev. 2014, 23, 161–169. [Google Scholar] [CrossRef]
- Environmental Protection Agency. Research and Development: Allergies Getting Worse? 2021. Available online: http://www.epa.gov/research/gems/scinews_aeroallergens.htm (accessed on 10 February 2022).
- Global Strategy for the Diagnosis. Management and Prevention of Chronic Obstructive Pulmonary Disease, Global Initiative for Chronic Obstructive Lung Disease (GOLD). 2021. Available online: http://www.goldcopd.org/ (accessed on 20 November 2021).
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention; Global Initiative for Asthma: Fontana, WI, USA, 2020; Available online: www.ginasthma.org (accessed on 10 May 2021).
- Mustafa, S.S.; Shaker, M.S.; Munblit, D.; Greenhawt, M. Paediatric allergy practice in the era of coronavirus disease 2019. Curr. Opin. Allergy Clin. Immunol. 2021, 21, 159–165. [Google Scholar] [CrossRef]
- Gupta, A.; Bush, A.; Nagakumar, P. Asthma in children during the COVID-19 pandemic: Lessons from lockdown and future directions for management. Lancet Respir. Med. 2020, 8, 1070–1071. [Google Scholar] [CrossRef]
- Halken, S.; Larenas-Linnemann, D.; Roberts, G.; Calderón, M.A.; Angier, E.; Pfaar, O.; Ryan, D.; Agache, I.; Ansotegui, I.J.; Arasi, S.; et al. EAACI guidelines on allergen immunotherapy: Prevention of allergy. Pediatr. Allergy Immunol. 2017, 28, 728–745. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, M.; Dhami, S.; Netuveli, G.; Halken, S.; Muraro, A.; Roberts, G.; Larenas-Linnemann, D.; Calderón, M.A.; Penagos, M.; Du Toit, G.; et al. Allergen immunotherapy for the prevention of allergy: A systematic review and Meta-Analysis. Pediatr. Allergy Immunol. 2017, 28, 18–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gradman, J.; Halken, S. Preventive Effect of Allergen Immunotherapy on Asthma and New Sensitizations. J. Allergy Clin. Immunol. Pract. 2021, 9, 1813–1817. [Google Scholar] [CrossRef] [PubMed]
- Thorsen, J.; Rasmussen, M.A.; Waage, J.; Mortensen, M.; Brejnrod, A.; Bønnelykke, K.; Chawes, B.L.; Brix, S.; Sørensen, S.J.; Stokholm, J.; et al. Infant airway microbiota and topical immune perturbations in the origins of childhood asthma. Nat. Commun. 2019, 10, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Tang, H.H.F.; Lang, A.; Teo, S.M.; Judd, L.M.; Gangnon, R.; Evans, M.D.; Lee, K.E.; Vrtis, R.; Holt, P.G.; Lemanske, R.F.; et al. Developmental patterns in the nasopharyngeal microbiome during infancy are associated with asthma risk. J. Allergy Clin. Immunol. 2021, 147, 1683–1691. [Google Scholar] [CrossRef]
- Zhou, Y.; Jackson, D.; Bacharier, L.B.; Mauger, D.; Boushey, H.; Castro, M.; Durack, J.; Huang, Y.; Lemanske, R.F., Jr.; Storch, G.A.; et al. The Upper-Airway microbiota and loss of asthma control among asthmatic children. Nat. Commun. 2019, 10, 5714. [Google Scholar] [CrossRef] [Green Version]
- Abrahamsson, T.; Jakobsson, H.E.; Andersson, A.; Björkstén, B.; Engstrand, L.; Jenmalm, M.C. Low gut microbiota diversity in early infancy precedes asthma at school age. Clin. Exp. Allergy 2014, 44, 842–850. [Google Scholar] [CrossRef] [Green Version]
- McNagny, K.M.; Sears, M.R.; Kollmann, T.; CHILD Study Investigators; Mohn, W.W.; Turvey, S.E.; Finlay, B.B.; Subbarao, P.; Mandhane, P.; Becker, A.; et al. Early infancy microbial and metabolic alterations affect risk of childhood asthma. Sci. Transl. Med. 2015, 7, 307ra152. [Google Scholar] [CrossRef]
- Bannier, M.A.G.E.; van Best, N.; Bervoets, L.; Savelkoul, P.H.M.; Hornef, M.W.; van de Kant, K.D.G.; Jöbsis, Q.; Dompeling, E.; Penders, J. Gut microbiota in wheezing preschool children and the association with childhood asthma. Allergy 2020, 75, 1473–1476. [Google Scholar] [CrossRef] [PubMed]
- Birzele, L.T.; Depner, M.; Ege, M.J.; Engel, M.; Kublik, S.; Bernau, C.; Loss, G.J.; Genuneit, J.; Horak, E.; Schloter, M.; et al. Environmental and mucosal microbiota and their role in childhood asthma. Allergy 2017, 72, 109–119. [Google Scholar] [CrossRef]
- Asher, I.; Pearce, N. Global burden of asthma among children. Int. J. Tuberc. Lung Dis. 2014, 18, 1269–1278. [Google Scholar] [CrossRef]
- Pijnenburg, M.W.; Szefler, S. Personalized medicine in children with asthma. Paediatr. Respir. Rev. 2014, 16, 101–107. [Google Scholar] [CrossRef]
- Trivedi, M.; Denton, E. Asthma in Children and Adults—What Are the Differences and What Can They Tell us About Asthma? Front. Pediatr. 2019, 7, 256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jat, K.R. Spirometry in children. Prim. Care Respir. J. 2013, 22, 221–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, N.; Gallagher, R.; Fowler, C.; Wales, S. The role of parents in managing asthma in middle childhood: An important consideration in chronic care. Collegian 2010, 17, 71–76. [Google Scholar] [CrossRef]
- Bacharier, L.B.; Guilbert, T.W. New Directions in Pediatric Asthma. Immunol. Allergy Clin. N. Am. 2019, 39, 283–295. [Google Scholar] [CrossRef]
- Asher, M.I.; Montefort, S.; Bjorksten, B.; Lai, C.K.; Strachan, D.P.; Weiland, S.K.; Williams, H. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry Cross-Sectional surveys. Lancet 2006, 368, 733–743. [Google Scholar] [CrossRef]
- Voorend-van Bergen, S.; Vaessen-Verberne, A.A.; Landstra, A.M.; Brackel, H.J.; van den Berg, N.J.; Caudri, D.; de Jongste, J.C.; Merkus, P.J.; Pijnenburg, M.W. Monitoring childhood asthma: Web-Based diaries and the asthma control test. J. Allergy Clin. Immunol. 2014, 133, 1599–1605.e92. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, P.M.; Watson, L.; Davis, K.J.; Rabe, K.F. Poor asthma control in children: Evidence from epidemiological surveys and implications for clinical practice. Int. J. Clin. Pract. 2006, 60, 321–334. [Google Scholar] [CrossRef]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention; Global Initiative for Asthma: Fontana, WI, USA, 2021; Available online: https://ginasthma.org/wp-content/uploads/2021/05/GINA-Main-Report-2021-V2-WMS.pdf (accessed on 3 June 2021).
- Santamaria, F.; Borrelli, M.; Baraldi, E. GINA 2021: The missing pieces in the childhood asthma puzzle. Lancet Respir. Med. 2021, 9, e98. [Google Scholar] [CrossRef]
- Forno, E.; Lescher, R.; Strunk, R.; Childhood Asthma Management Program Research Group; Weiss, S.T.; Fuhlbrigge, A.; Celedón, J.C. Decreased Response To Inhaled Steroids In Overweight And Obese Asthmatic Children. J. Allergy Clin. Immunol. 2011, 127, 741–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vajro, P.; Fischler, B.; Burra, P.; Debray, D.; Dezsofi, A.; Nuzio, S.G.; Hadzic, N.; Hierro, L.; Jahnel, J.; Lamireau, T.; et al. The Health Care Transition of Youth With Liver Disease Into the Adult Health System: Position Paper From ESPGHAN and EASL. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 976–990. [Google Scholar] [CrossRef] [PubMed]
- Tantisira, K.G.; Lake, S.; Silverman, E.S.; Palmer, L.; Lazarus, R.; Silverman, E.K.; Liggett, S.B.; Gelfand, E.W.; Rosenwasser, L.J.; Richter, B.; et al. Corticosteroid pharmacogenetics: Association of sequence variants in CRHR1 with improved lung function in asthmatics treated with inhaled corticosteroids. Hum. Mol. Genet. 2004, 13, 1353–1359. [Google Scholar] [CrossRef] [Green Version]
- Tantisira, K.G.; Hwang, E.S.; Raby, B.A.; Silverman, E.S.; Lake, S.L.; Richter, B.G.; Peng, S.L.; Drazen, J.M.; Glimcher, L.H.; Weiss, S.T. TBX21: A functional variant predicts improvement in asthma with the use of inhaled corticosteroids. Proc. Natl. Acad. Sci. USA 2004, 101, 18099–18104. [Google Scholar] [CrossRef] [Green Version]
- Tantisira, K.G.; Lasky-Su, J.; Harada, M.; Murphy, A.; Litonjua, A.A.; Himes, B.E.; Lange, C.; Lazarus, R.; Sylvia, J.; Klanderman, B.; et al. Genomewide association between GLCCI1 and response to glucocorticoid therapy in asthma. N. Engl. J. Med. 2011, 365, 1173–1183. [Google Scholar] [CrossRef] [Green Version]
- Koster, E.S.; van der Zee, A.H.M.; Tavendale, R.; Mukhopadhyay, S.; Vijverberg, S.J.; Raaijmakers, J.A.; Palmer, C.N.A. FCER2 T2206C variant associated with chronic symptoms and exacerbations in steroid-treated asthmatic children. Allergy 2011, 66, 1546–1552. [Google Scholar] [CrossRef]
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; Fitzgerald, J.M.; et al. Global Initiative for Asthma Strategy 2021: Executive Summary and Rationale for Key Changes. Am. J. Respir. Crit. Care Med. 2022, 205, 17–35. [Google Scholar] [CrossRef]
- Lawless, C.; Turner, E.M.; LeFave, E.; Koinis-Mitchell, D.; Fedele, D.A. Sleep hygiene in adolescents with asthma. J. Asthma 2020, 57, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Lunsford-Avery, J.R.; Bidopia, T.; Jackson, L.; Sloan, J. Behavioral Treatment of Insomnia and Sleep Disturbances in School-Aged Children and Adolescents. Child Adolesc. Psychiatr. Clin. N. Am. 2021, 30, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Csonka, P.; Tapiainen, T.; Mäkelä, M.J.; Lehtimäki, L. Optimal administration of bronchodilators with valved holding chambers in preschool children: A review of literature. Eur. J. Pediatr. 2021, 180, 3101–3109. [Google Scholar] [CrossRef] [PubMed]
- Custovic, A.; Bhattacharjee, R.; Choi, B.H.; Gozal, D.; Mokhlesi, B. Association of adenotonsillectomy with asthma outcomes in children: A longitudinal database analysis. PLoS Med. 2014, 11, e1001753. [Google Scholar] [CrossRef] [Green Version]
- Valvo, L.; Leonardi, S.; Marseglia, G.L.; Del Giudice, M.M.; Salpietro, C.; Ciprandi, G.; La Rosa, M. Inhalation Therapy in Asthmatic and Not Asthmatic Children. Int. J. Immunopathol. Pharmacol. 2011, 24 (Suppl. S4), 61–67. [Google Scholar] [CrossRef]
- Toraldo, D.M.; Di Michele, L.; Ralli, M.; Arigliani, M.; Passali, G.C.; De Benedetto, M.; Passali, D. Obstructive sleep apnea syndrome in the pediatric age: The role of the pneumologist. Eur. Rev. Med. Pharmacol. Sci. 2019, 23 (Suppl. S1), 15–18. [Google Scholar] [CrossRef]
- Kamps, A.W.; van Ewijk, B.; Roorda, R.J.; Brand, P.L. Poor inhalation technique, even after inhalation instructions, in children with asthma. Pediatr. Pulmonol. 2000, 29, 39–42. [Google Scholar] [CrossRef]
- Han, J.; Nguyen, J.; Kim, Y.; Geng, B.; Romanowski, G.; Alejandro, L.; Proudfoot, J.; Xu, R.; Leibel, S. Effect of inhaled corticosteroid use on weight (BMI) in pediatric patients with Moderate-Severe asthma. J. Asthma 2019, 56, 263–269. [Google Scholar] [CrossRef]
- Denton, E.; Price, D.B.; Tran, T.N.; Canonica, G.W.; Menzies-Gow, A.; Fitzgerald, J.M.; Sadatsafavi, M.; de Llano, L.P.; Christoff, G.; Quinton, A.; et al. Cluster Analysis of Inflammatory Biomarker Expression in the International Severe Asthma Registry. J. Allergy Clin. Immunol. Pract. 2021, 9, 2680–2688.e7. [Google Scholar] [CrossRef]
- Fleming, L.; Murray, C.; Bansal, A.T.; Hashimoto, S.; Bisgaard, H.; Bush, A.; Frey, U.; Hedlin, G.; Singer, F.; van AAlderen, W.M.; et al. The burden of severe asthma in childhood and adolescence: Results from the paediatric U-BIOPRED cohorts. Eur. Respir. J. 2015, 46, 1322–1333. [Google Scholar] [CrossRef] [Green Version]
- Ross, K.R.; Gupta, R.; DeBoer, M.D.; Zein, J.; Phillips, B.R.; Mauger, D.T.; Li, C.; Myers, R.E.; Phipatanakul, W.; Fitzpatrick, A.M.; et al. Severe asthma during childhood and adolescence: A longitudinal study. J. Allergy Clin. Immunol. 2020, 145, 140–146.e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarokh, L.; Saletin, J.M.; Carskadon, M.A. Sleep in adolescence: Physiology, cognition and mental health. Neurosci. Biobehav. Rev. 2016, 70, 182–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curcio, G.; Ferrara, M.; De Gennaro, L. Sleep loss, learning capacity and academic performance. Sleep Med. Rev. 2006, 10, 323–337. [Google Scholar] [CrossRef]
- World Health Organization. Factsheet on Asthma. 2020. Available online: http://www.who.int/news-room/fact-sheets/detail/asthma (accessed on 10 February 2022).
- Jonson, E.O.; Roth, T.; Schultz, L.; Breslau, N. Epidemiology of DSM-IV Insomnia in Adolescence: Lifetime Prevalence, Chronicity, and an Emergent Gender Difference. Pediatrics 2006, 117, e247–e256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, R.E.; Roberts, C.R.; Duong, H.T. Chronic Insomnia and Its Negative Consequences for Health and Functioning of Adolescents: A 12-Month Prospective Study. J. Adolesc. Health 2008, 42, 294–302. [Google Scholar] [CrossRef] [Green Version]
- Alanazi, T.M.; Alghamdi, H.S.; Alberreet, M.S.; Alkewaibeen, A.M.; Alkhalefah, A.M.; Omair, A.; Al-Jahdali, H.; Al-Harbi, A. The prevalence of sleep disturbance among asthmatic patients in a tertiary care center. Sci. Rep. 2021, 11, 2457. [Google Scholar] [CrossRef]
- de Zambotti, M.; Goldstone, A.; Colrain, I.M.; Baker, C.B. Insomnia disorder in adolescence: Diagnosis, impact, and treatment. Sleep Med. Rev. 2018, 39, 12–24. [Google Scholar] [CrossRef]
- Reiter, J.; Ramagopal, M.; Gileles-Hillel, A.; Forno, E. Sleep disorders in children with asthma. Pediatr. Pulmonol. 2021, 1–9. [Google Scholar] [CrossRef]
- Durrington, H.J.; Farrow, S.N.; Loudon, A.S.; Ray, D.W. The circadian clock and asthma. Thorax 2014, 69, 90–92. [Google Scholar] [CrossRef] [Green Version]
- Haarman, M.G.; van Hunsel, F.; de Vries, T.W. Adverse drug reactions of montelukast in children and adults. Pharmacol. Res. Perspect. 2017, 5, e00341. [Google Scholar] [CrossRef]
- Martin, R.J.; Cicutto, L.C.; Ballard, R.D. Factors Related to the Nocturnal Worsening of Asthma. Am. Rev. Respir. Dis. 1990, 141, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Sundbom, F.; Malinovschi, A.; Lindberg, E.; Almqvist, C.; Janson, C. Insomnia symptoms and asthma control. Interrelations and importance of comorbidities. Clin. Exp. Allergy 2020, 50, 170–177. [Google Scholar] [CrossRef]
- Meltzer, L.; Beebe, D.W.; Jump, S.; Flewelling, K.; Sundström, D.; White, M.; Zeitlin, P.L.; Strand, M.J. Impact of sleep opportunity on asthma outcomes in adolescents. Sleep Med. 2020, 65, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Bakour, C.; Schwartz, S.W.; Wang, W.; Sappenfield, W.M.; Couluris, M.; Chen, H.; O’Rourke, K. Sleep duration patterns from adolescence to young adulthood and the risk of asthma. Ann. Epidemiol. 2020, 49, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Hanson, M.D.; Chen, E. The Temporal Relationships Between Sleep, Cortisol, and Lung Functioning in Youth with Asthma. J. Pediatr. Psychol. 2008, 33, 312–316. [Google Scholar] [CrossRef] [Green Version]
- Meltzer, L.J.; Ullrich, M.; Szefle, S. Sleep Duration, Sleep Hygiene, and Insomnia in Adolescents with Asthma. J. Allergy Clin. Immunol. Pract. 2014, 2, 562–569. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caruso, C.; Colantuono, S.; Arasi, S.; Nicoletti, A.; Gasbarrini, A.; Coppola, A.; Di Michele, L. Heterogeneous Condition of Asthmatic Children Patients: A Narrative Review. Children 2022, 9, 332. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030332
Caruso C, Colantuono S, Arasi S, Nicoletti A, Gasbarrini A, Coppola A, Di Michele L. Heterogeneous Condition of Asthmatic Children Patients: A Narrative Review. Children. 2022; 9(3):332. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030332
Chicago/Turabian StyleCaruso, Cristiano, Stefania Colantuono, Stefania Arasi, Alberto Nicoletti, Antonio Gasbarrini, Angelo Coppola, and Loreta Di Michele. 2022. "Heterogeneous Condition of Asthmatic Children Patients: A Narrative Review" Children 9, no. 3: 332. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030332