
Combined Use of Three-Dimensional Construction and Indocyanine Green-Fluorescent Imaging for Resection of Multiple Lung Metastases in Hepatoblastoma

 , ,
, ,
Abstract
:1. Introduction
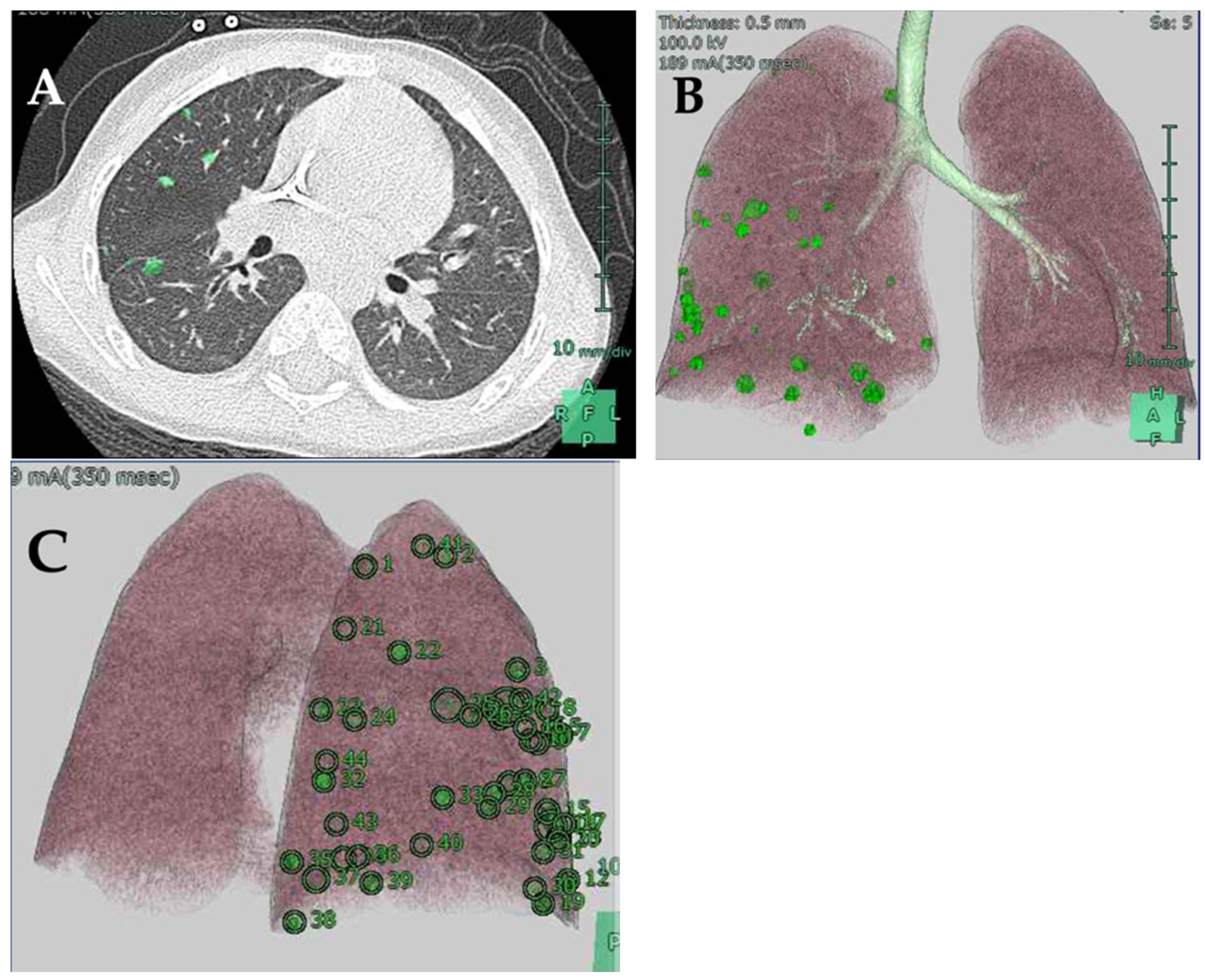
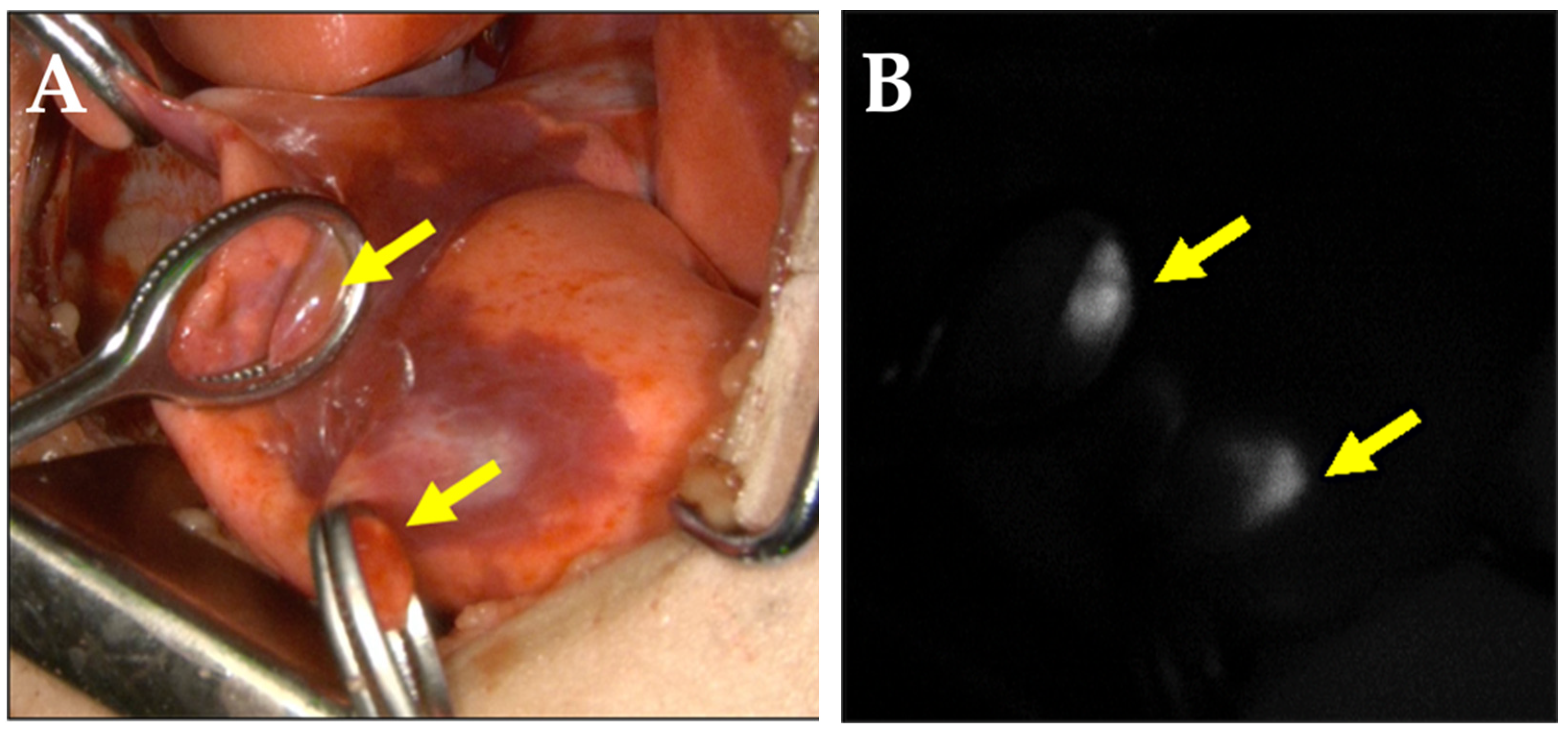
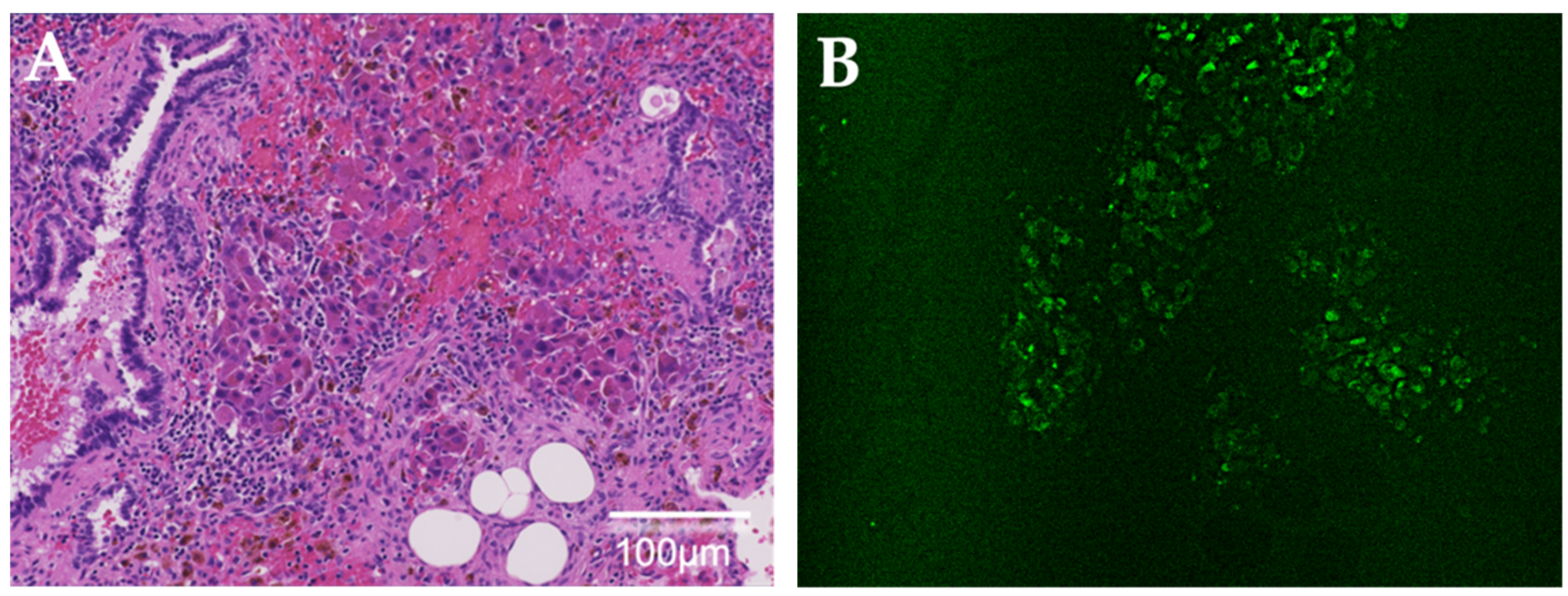
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- von Schweinitz, D. Hepatoblastoma: Recent developments in research and treatment. Semin. Pediatr. Surg. 2012, 21, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Hiyama, E.; Hishiki, T.; Watanabe, K.; Ida, K.; Ueda, Y.; Kurihara, S.; Yano, M.; Hoshino, K.; Yokoi, A.; Takama, Y.; et al. Outcome and Late Complications of Hepatoblastomas Treated Using the Japanese Study Group for Pediatric Liver Tumor 2 Protocol. J. Clin. Oncol. 2020, 38, 2488–2498. [Google Scholar] [CrossRef] [PubMed]
- Hishiki, T.; Watanabe, K.; Ida, K.; Hoshino, K.; Iehara, T.; Aoki, Y.; Kazama, T.; Kihira, K.; Takama, Y.; Taguchi, T.; et al. The role of pulmonary metastasectomy for hepatoblastoma in children with metastasis at diagnosis: Results from the JPLT-2 study. J. Pediatr. Surg. 2017, 52, 2051–2055. [Google Scholar] [CrossRef] [PubMed]
- Zsiros, J.; Brugieres, L.; Brock, P.; Roebuck, D.; Maibach, R.; Zimmermann, A.; Childs, M.; Pariente, D.; Laithier, V.; Otte, J.B.; et al. Dose-dense cisplatin-based chemotherapy and surgery for children with high-risk hepatoblastoma (SIOPEL-4): A prospective, single-arm, feasibility study. Lancet Oncol. 2013, 14, 834–842. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, A.F.; Towbin, A.J.; Krailo, M.D.; Xia, C.; Gao, Y.; McCarville, M.B.; Meyers, R.L.; McGahren, E.D.; Tiao, G.M.; Dunn, S.P.; et al. Characterization of Pulmonary Metastases in Children With Hepatoblastoma Treated on Children’s Oncology Group Protocol AHEP0731 (The Treatment of Children With All Stages of Hepatoblastoma): A Report From the Children’s Oncology Group. J. Clin. Oncol. 2017, 35, 3465–3473. [Google Scholar] [CrossRef] [PubMed]
- Zsiros, J.; Maibach, R.; Shafford, E.; Brugieres, L.; Brock, P.; Czauderna, P.; Roebuck, D.; Childs, M.; Zimmermann, A.; Laithier, V.; et al. Successful treatment of childhood high-risk hepatoblastoma with dose-intensive multiagent chemotherapy and surgery: Final results of the SIOPEL-3HR study. J. Clin. Oncol. 2010, 28, 2584–2590. [Google Scholar] [CrossRef]
- Meyers, R.L.; Katzenstein, H.M.; Krailo, M.; McGahren, E.D., 3rd; Malogolowkin, M.H. Surgical resection of pulmonary metastatic lesions in children with hepatoblastoma. J. Pediatr. Surg. 2007, 42, 2050–2056. [Google Scholar] [CrossRef]
- Angelico, R.; Grimaldi, C.; Gazia, C.; Saffioti, M.C.; Manzia, T.M.; Castellano, A.; Spada, M. How Do Synchronous Lung Metastases Influence the Surgical Management of Children with Hepatoblastoma? An Update and Systematic Review of the Literature. Cancers 2019, 11, 1693. [Google Scholar] [CrossRef] [Green Version]
- Chu, X.P.; Chen, Z.H.; Lin, S.M.; Tang, W.F.; Zhang, J.T.; Lai, Y.M.; Fu, R.; Qiu, Z.B.; Lin, J.T.; Nie, Q.; et al. Precise resection of multiple pulmonary nodules using a three-dimensional reconstruction model: A case report. Thorac. Cancer 2021, 12, 970–973. [Google Scholar] [CrossRef]
- Wu, W.; Wu, Y.; Shen, G.; Zhang, G. Preoperative virtual simulation for synchronous multiple primary lung cancers using three-dimensional computed tomography lung reconstruction: A case report. J. Cardiothorac. Surg. 2021, 16, 10. [Google Scholar] [CrossRef]
- Akiba, T. Utility of three-dimensional computed tomography in general thoracic surgery. Gen. Thorac. Cardiovasc. Surg. 2013, 61, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Akiba, T.; Morikawa, T.; Ohki, T. Thoracoscopic lung segmentectomy simulated by a tailor-made virtual lung: Computed bronchography and angiography. Thorac. Cardiovasc. Surg. 2013, 61, 151–153. [Google Scholar] [PubMed]
- Kitagawa, N.; Shinkai, M.; Mochizuki, K.; Usui, H.; Miyagi, H.; Nakamura, K.; Tanaka, M.; Tanaka, Y.; Kusano, M.; Ohtsubo, S. Navigation using indocyanine green fluorescence imaging for hepatoblastoma pulmonary metastases surgery. Pediatr. Surg. Int. 2015, 31, 407–411. [Google Scholar] [CrossRef]
- Yamamichi, T.; Oue, T.; Yonekura, T.; Owari, M.; Nakahata, K.; Umeda, S.; Nara, K.; Ueno, T.; Uehara, S.; Usui, N. Clinical application of indocyanine green (ICG) fluorescent imaging of hepatoblastoma. J. Pediatr. Surg. 2015, 50, 833–836. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.J.; Namgoong, J.M.; Kwon, H.H.; Kwon, Y.J.; Kim, D.Y.; Kim, S.C. The Advantages of Indocyanine Green Fluorescence Imaging in Detecting and Treating Pediatric Hepatoblastoma: A Preliminary Experience. Front. Pediatr. 2021, 9, 635394. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Ohno, M.; Fujino, A.; Kanamori, Y.; Irie, R.; Yoshioka, T.; Miyazaki, O.; Uchida, H.; Fukuda, A.; Sakamoto, S.; et al. Fluorescence-Guided Surgery for Hepatoblastoma with Indocyanine Green. Cancers 2019, 11, 1215. [Google Scholar] [CrossRef] [Green Version]
- Souzaki, R.; Kawakubo, N.; Matsuura, T.; Yoshimaru, K.; Koga, Y.; Takemoto, J.; Shibui, Y.; Kohashi, K.; Hayashida, M.; Oda, Y.; et al. Navigation surgery using indocyanine green fluorescent imaging for hepatoblastoma patients. Pediatr. Surg. Int. 2019, 35, 551–557. [Google Scholar] [CrossRef]
- Ishizawa, T.; Fukushima, N.; Shibahara, J.; Masuda, K.; Tamura, S.; Aoki, T.; Hasegawa, K.; Beck, Y.; Fukayama, M.; Kokudo, N. Real-time identification of liver cancers by using indocyanine green fluorescent imaging. Cancer 2009, 11, 2491–2504. [Google Scholar] [CrossRef]
- Kitagawa, N.; Shinkai, M.; Mochizuki, K.; Usui, H.; Yagi, Y.; Yukihiro, T.; Ikkei, O.; Akio, K.; Mio, T.; Tanaka, Y. Examination of Performance of Detection Device in ICG Fluorescence Method: Comparison of Handheld Type and Endoscopic Type. Jpn. J. Pediatric Hematol. Oncol. 2021, 58, 292. [Google Scholar]
- Hiyama, E. Fluorescence Image-Guided Navigation Surgery Using Indocyanine Green for Hepatoblastoma. Children 2021, 8, 1015. [Google Scholar] [CrossRef]
- Speich, R.; Saesseli, B.; Hoffmann, U.; Neftel, K.A.; Reichen, J. Anaphylactoid reactions after indocyanine-green administration. Ann. Intern. Med. 1988, 109, 345–346. [Google Scholar] [CrossRef] [PubMed]
- Kudo, H.; Ishizawa, T.; Tani, K.; Harada, N.; Ichida, A.; Shimizu, A.; Kaneko, J.; Aoki, T.; Sakamoto, Y.; Sugawara, Y.; et al. Visualization of subcapsular hepatic malignancy by indocyanine-green fluorescence imaging during laparoscopic hepatectomy. Surg. Endosc. 2014, 2, 2504–2508. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Ma, S.; Yan, T.; Song, J.; Wang, K.; He, W.; Bai, J. Computed Tomography Guided Hook-wire Precise Localization and Minimally Invasive Resection of Pulmonary Nodules. Zhongguo Fei Ai Za Zhi 2015, 18, 680–685. [Google Scholar] [PubMed]
- Yamamichi, T.; Nishikawa, M.; Takayama, K.; Takase, K.; Kim, K.; Umeda, S.; Tayama, A.; Tsukada, R.; Nomura, M.; Okuyama, H.; et al. Computed tomography-guided marking using a dye-staining method for preoperative localization of tiny pulmonary lesions in children. Pediatr. Surg. Int. 2021, 37, 1265–1272. [Google Scholar] [CrossRef]
- Mochizuki, C.; Nakamura, J.; Nakamura, M. Development of Non-Porous Silica Nanoparticles towards Cancer Photo-Theranostics. Biomedicines 2021, 9, 73. [Google Scholar] [CrossRef]
- Imamura, T.; Saitou, T.; Kawakami, R. In vivo optical imaging of cancer cell function and tumor microenvironment. Cancer Sci. 2018, 109, 912–918. [Google Scholar] [CrossRef]
- He, X.; Li, L.; Fang, Y.; Shi, W.; Li, X.; Ma, H. In vivo imaging of leucine aminopeptidase activity in drug-induced liver injury and liver cancer via a near-infrared fluorescent probe. Chem. Sci. 2017, 8, 3479–3483. [Google Scholar] [CrossRef] [Green Version]
- Tam, J.; Pilozzi, A.; Mahmood, U.; Huang, X. Simultaneous Monitoring of Multi-Enzyme Activity and Concentration in Tumor Using a Triply Labeled Fluorescent In Vivo Imaging Probe. Int. J. Mol. Sci. 2020, 21, 3068. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICG Fluorescent Imaging | Histological Examination | |
|---|---|---|
| Tumor | Non-Tumor | |
| Positive | 52 | 22 |
| Negative | 1 | 22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komatsu, S.; Terui, K.; Nakata, M.; Shibata, R.; Oita, S.; Kawaguchi, Y.; Yoshizawa, H.; Hirokawa, T.; Nakatani, E.; Hishiki, T. Combined Use of Three-Dimensional Construction and Indocyanine Green-Fluorescent Imaging for Resection of Multiple Lung Metastases in Hepatoblastoma. Children 2022, 9, 376. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030376
Komatsu S, Terui K, Nakata M, Shibata R, Oita S, Kawaguchi Y, Yoshizawa H, Hirokawa T, Nakatani E, Hishiki T. Combined Use of Three-Dimensional Construction and Indocyanine Green-Fluorescent Imaging for Resection of Multiple Lung Metastases in Hepatoblastoma. Children. 2022; 9(3):376. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030376
Chicago/Turabian StyleKomatsu, Shugo, Keita Terui, Mitsuyuki Nakata, Ryohei Shibata, Satoru Oita, Yunosuke Kawaguchi, Hiroko Yoshizawa, Tomoya Hirokawa, Erika Nakatani, and Tomoro Hishiki. 2022. "Combined Use of Three-Dimensional Construction and Indocyanine Green-Fluorescent Imaging for Resection of Multiple Lung Metastases in Hepatoblastoma" Children 9, no. 3: 376. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030376