
Differential Diagnosis of Cyclic Vomiting and Periodic Headaches in a Child with Ventriculoperitoneal Shunt: Case Report of Chronic Shunt Overdrainage

 ,
, 

Abstract
:1. Introduction
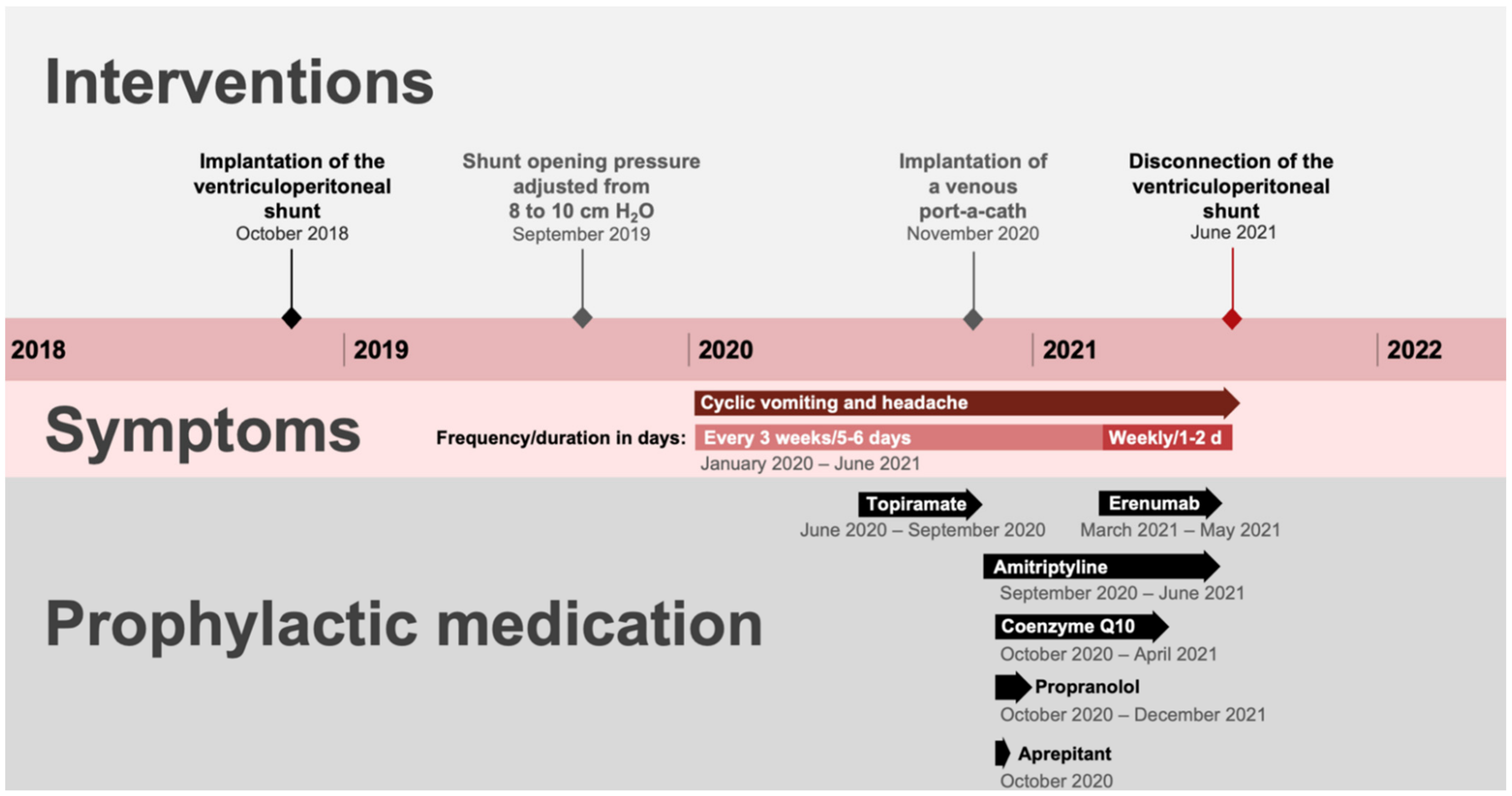
2. Case Report
2.1. Patient Information
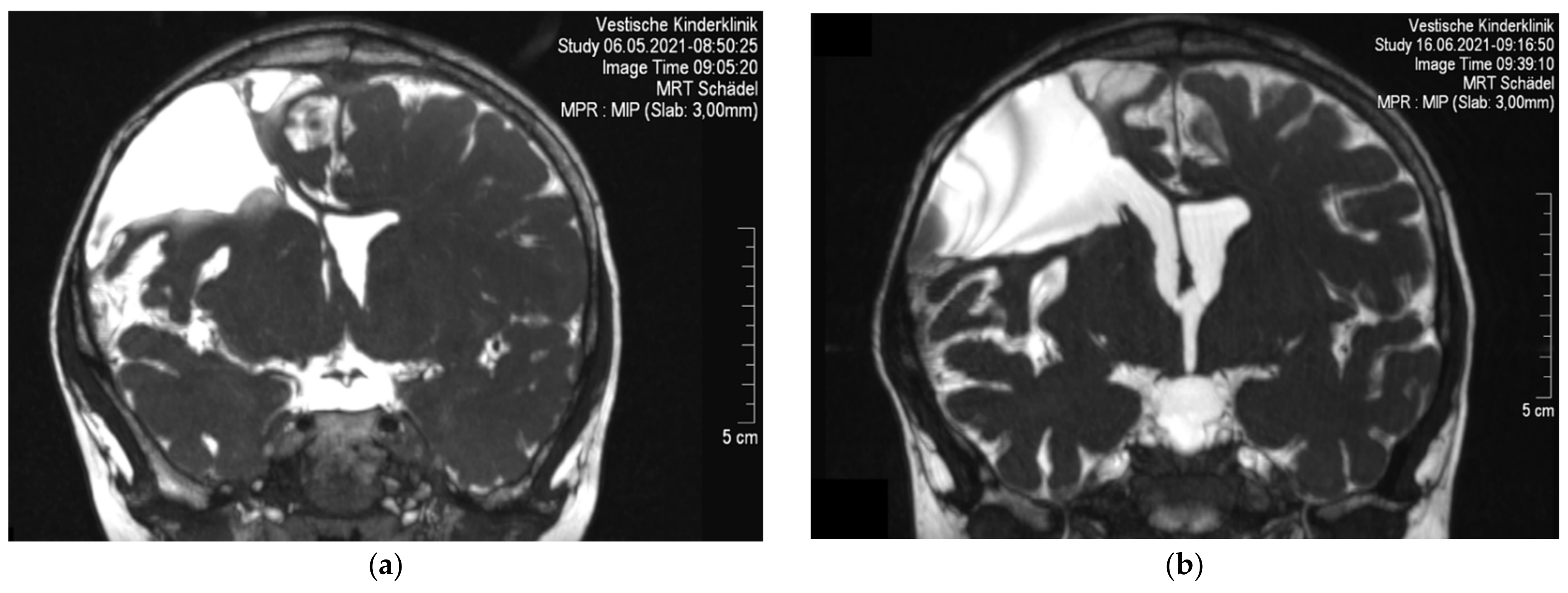
2.2. Symptoms and Clinical Findings
2.3. Therapeutic Intervention
2.4. Follow-Up and Outcome
3. Discussion
3.1. Overdrainage Syndrome
3.2. Pharmacological Treatment of CVS
3.3. Clinical Course
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, B.U.K.; Lefevre, F.; Chelimsky, G.G.; Boles, R.G.; Nelson, S.P.; Lewis, D.W.; Linder, S.L.; Issenman, R.M.; Rudolph, C.D.; North American Society for Pediatric Gastroenterology. North American Society for Pediatric Gastroenterology, Hepatology, and North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition Consensus Statement on the Diagnosis and Management of Cyclic Vomiting Syndrome. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 379–393. [Google Scholar] [CrossRef] [PubMed]
- Hyams, J.S.; Lorenzo, C.D.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Childhood Functional Gastrointestinal Disorders: Child/Adolescent. Gastroenterology 2016, 150, 1456–1468.e2. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, S.; Venkatesan, T. Novel Treatments for Cyclic Vomiting Syndrome: Beyond Ondansetron and Amitriptyline. Curr. Treat. Options Gastroenterol. 2016, 14, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Li, B.U.K. Managing Cyclic Vomiting Syndrome in Children: Beyond the Guidelines. Eur. J. Pediatr. 2018, 177, 1435–1442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raucci, U.; Borrelli, O.; Nardo, G.D.; Tambucci, R.; Pavone, P.; Salvatore, S.; Baldassarre, M.E.; Cordelli, D.M.; Falsaperla, R.; Felici, E.; et al. Cyclic Vomiting Syndrome in Children. Front. Neurol. 2020, 11, 583425. [Google Scholar] [CrossRef] [PubMed]
- Kovacic, K.; Sood, M.; Venkatesan, T. Cyclic Vomiting Syndrome in Children and Adults: What Is New in 2018? Curr. Gastroenterol. Rep. 2018, 20, 46. [Google Scholar] [CrossRef]
- Hasler, W.L.; Levinthal, D.J.; Tarbell, S.E.; Adams, K.A.; Li, B.U.K.; Issenman, R.M.; Sarosiek, I.; Jaradeh, S.S.; Sharaf, R.N.; Sultan, S.; et al. Cyclic Vomiting Syndrome: Pathophysiology, Comorbidities, and Future Research Directions. Neurogastroenterol. Motil. 2019, 31, e13607. [Google Scholar] [CrossRef]
- Yu, E.S.; Yasodara Priyadharsini, S.S.; Venkatesan, T. Migraine, Cyclic Vomiting Syndrome, and Other Gastrointestinal Disorders. Curr. Treat. Options Gastroenterol. 2018, 16, 511–527. [Google Scholar] [CrossRef]
- Schulman, M.L.; Mangel, S.L. Cyclic Vomiting Syndrome in a Medically Complex Patient: A Case Report. J. Pediatr. Health Care 2019, 33, 711–717. [Google Scholar] [CrossRef]
- Rekate, H.L. Shunt-Related Headaches: The Slit Ventricle Syndromes. Child’s Nerv. Syst. 2008, 24, 423–430. [Google Scholar] [CrossRef]
- Rekate, H.L. Slit Ventricle Syndrome. Diagnosis and Management. In Pediatric Hydrocephalus; Cinalli, G., Maxner, W.J., Sainte-Rose, C., Eds.; Springer: Berlin/Heidelberg, Germany, 2004; pp. 335–349. [Google Scholar]
- Ros, B.; Iglesias, S.; Linares, J.; Cerro, L.; Casado, J.; Arráez, M.A. Shunt Overdrainage: Reappraisal of the Syndrome and Proposal for an Integrative Model. J. Clin. Med. 2021, 10, 3620. [Google Scholar] [CrossRef]
- Riley, D.S.; Barber, M.S.; Kienle, G.S.; Aronson, J.K.; von Schoen-Angerer, T.; Tugwell, P.; Kiene, H.; Helfand, M.; Altman, D.G.; Sox, H.; et al. CARE Guidelines for Case Reports: Explanation and Elaboration Document. J. Clin. Epidemiol. 2017, 89, 218–235. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd ed. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Szperka, C.L.; VanderPluym, J.; Orr, S.L.; Oakley, C.B.; Qubty, W.; Patniyot, I.; Lagman-Bartolome, A.M.; Morris, C.; Gautreaux, J.; Victorio, M.C.; et al. Recommendations on the Use of Anti-CGRP Monoclonal Antibodies in Children and Adolescents. Headache J. Head Face Pain 2018, 58, 1658–1669. [Google Scholar] [CrossRef] [PubMed]
- Sainz, L.V.; Hockel, K.; Schuhmann, M.U. Chronic Overdrainage Syndrome: Pathophysiological Insights Based on ICP Analysis: A Case-Based Review. Child’s Nerv. Syst. 2018, 34, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Albright, A.L.; Tyler-Kabara, E. Slit-Ventricle Syndrome Secondary to Shunt-Induced Suture Ossification. Neurosurgery 2001, 48, 764. [Google Scholar] [CrossRef]
- Hanak, B.W.; Bonow, R.H.; Harris, C.A.; Browd, S.R. Cerebrospinal Fluid Shunting Complications in Children. Pediatr. Neurosurg. 2017, 52, 381–400. [Google Scholar] [CrossRef]
- Ros, B.; Iglesias, S.; Martín, Á.; Carrasco, A.; Ibáñez, G.; Arráez, M.A. Shunt Overdrainage Syndrome: Review of the Literature. Neurosurg. Rev. 2018, 41, 969–981. [Google Scholar] [CrossRef]
- Iglesias, S.; Ros, B.; Ibáñez, G.; Delgado, A.; Ros, Á.; Arráez, M.Á. Shunt Independence in Paediatric Hydrocephalus: Our 16-Year Experience and Review. Child’s Nerv. Syst. 2019, 35, 1547–1555. [Google Scholar] [CrossRef]
- Kraemer, M.R.; Sandoval-Garcia, C.; Bragg, T.; Iskandar, B.J. Shunt-Dependent Hydrocephalus: Management Style among Members of the American Society of Pediatric Neurosurgeons. J. Neurosurg. Pediatr. 2017, 20, 216–224. [Google Scholar] [CrossRef]
- Kraemer, M.R.; Koueik, J.; Rebsamen, S.; Hsu, D.A.; Salamat, M.S.; Luo, S.; Saleh, S.; Bragg, T.M.; Iskandar, B.J. Overdrainage-Related Ependymal Bands: A Postulated Cause of Proximal Shunt Obstruction. J. Neurosurg. Pediatr. 2018, 22, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Keyser, V.D.; Woods, D.D. Fixation Errors: Failures to Revise Situation Assessment in Dynamic and Risky Systems. In Systems Reliability Assessment: ISPRA Courses (on Reliability and Risk Analysis); Colombo, A.G., de Bustamante, A.S., Eds.; Springer: Dordrecht, The Netherlands, 1990; pp. 231–251. ISBN 978-94-009-0649-5. [Google Scholar]
- Coggon, D.; Martyn, C.; Palmer, K.T.; Evanoff, B. Assessing Case Definitions in the Absence of a Diagnostic Gold Standard. Int. J. Epidemiol. 2005, 34, 949–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Association of Paediatric Palliative Medicine Master Formulary 5th Edition. Available online: https://www.appm.org.uk/_webedit/uploaded-files/All%20Files/Event%20Resources/2020%20APPM%20Master%20Formulary%202020%20protected.pdf (accessed on 15 March 2022).
- Maasumi, K.; Michael, R.L.; Rapoport, A.M. CGRP and Migraine: The Role of Blocking Calcitonin Gene-Related Peptide Ligand and Receptor in the Management of Migraine. Drugs 2018, 78, 913–928. [Google Scholar] [CrossRef] [PubMed]
- Greene, K.A.; Gentile, C.P.; Szperka, C.L.; Yonker, M.; Gelfand, A.A.; Grimes, B.; Irwin, S.L. Calcitonin Gene–Related Peptide Monoclonal Antibody Use for the Preventive Treatment of Refractory Headache Disorders in Adolescents. Pediatr. Neurol. 2021, 114, 62–67. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| NASPGHAN [1] | Rome IV [2] | ICH-D-3 [11] |
|---|---|---|
| All the criteria must be met: 1. At least five attacks in any interval or a minimum of three attacks during a 6-month period; 2. Episodic attacks of intense nausea and vomiting lasting from 1 h to 10 days and occurring at least 1 week apart; 3. Stereotypical pattern and symptoms in the individual patient; 4. Vomiting during attacks occurs at least 4 times/hour for at least 1 h; 5. Return to baseline health between episodes; 6. Not attributed to another disorder. | Children and Adolescents Must include all of the following: 1. The occurrence of 2 or more periods of intense, unremitting nausea and paroxysmal vomiting, lasting hours to days within a 6-month period; 2. Episodes are stereotypical in each patient; 3. Episodes are separated by weeks to months with return to baseline health between episodes; 4. After appropriate medical evaluation, the symptoms cannot be attributed to another condition. Neonates and toddlers Must include all of the following: 1. Two or more periods of unremitting paroxysmal vomiting with or without retching, lasting hours to days within a 6-month period; 2. Episodes are stereotypical in each patient; 3. Episodes are separated by weeks to months with return to baseline health between episodes of vomiting. | A. At least five attacks of intense nausea and vomiting, fulfilling criteria B and C. B. Stereotypical in the individual patient and recurring with predictable periodicity. C. All of the following: 1. Nausea and vomiting occur at least four times per hour; 2. Attacks last ≥1 h and up to 10 days; 3. Attacks occur ≥1 week apart. D. Complete freedom from symptoms between attacks. E. Not attributed to another disorder (in particular, history and physical examination do not show signs of gastrointestinal disease). |
| Prophylactic Medication | Abortive Medication |
|---|---|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mauritz, M.D.; Hasan, C.; Schreiber, L.; Wegener-Panzer, A.; Barth, S.; Zernikow, B. Differential Diagnosis of Cyclic Vomiting and Periodic Headaches in a Child with Ventriculoperitoneal Shunt: Case Report of Chronic Shunt Overdrainage. Children 2022, 9, 432. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030432
Mauritz MD, Hasan C, Schreiber L, Wegener-Panzer A, Barth S, Zernikow B. Differential Diagnosis of Cyclic Vomiting and Periodic Headaches in a Child with Ventriculoperitoneal Shunt: Case Report of Chronic Shunt Overdrainage. Children. 2022; 9(3):432. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030432
Chicago/Turabian StyleMauritz, Maximilian David, Carola Hasan, Lutz Schreiber, Andreas Wegener-Panzer, Sylvia Barth, and Boris Zernikow. 2022. "Differential Diagnosis of Cyclic Vomiting and Periodic Headaches in a Child with Ventriculoperitoneal Shunt: Case Report of Chronic Shunt Overdrainage" Children 9, no. 3: 432. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030432